
Abstract
Background:
Subclinical hypothyroidism, defined by elevated thyrotropin (TSH) and normal free thyroxine levels, is associated with adverse pregnancy outcomes, including preterm birth, pre-eclampsia, and small for gestational age. Despite the uncertainty regarding the effectiveness of levothyroxine (LT4) treatment on pregnancy outcomes in subclinical hypothyroidism, LT4 is widely administered with a pre-treatment threshold TSH level of 2.5 mU/L. The aim of this study is to investigate the efficacy of periconceptional LT4 treatment for subclinical hypothyroidism, including TSH levels >2.5 mU/L, and identify the characteristics of subclinical hypothyroidism that can benefit from LT4 treatment.
Methods:
We conducted a systematic review and meta-analysis of randomized controlled trials from inception to February 2023. We analyzed the pooled effects of LT4 on subclinical hypothyroidism before and during pregnancy. The main outcomes before pregnancy were live birth, pregnancy, and miscarriage. The main outcomes during pregnancy were live birth, miscarriage, and preterm birth. We conducted subgroup analyses to compare the effects of LT4 on subclinical hypothyroidism with TSH levels of 2.5–4.0 and >4.0 mU/L.
Results:
Of the 888 studies identified, 27 full-text articles were screened for eligibility. Five studies on pre-conception treatment with 768 participants and eight studies on treatment during early pregnancy with 2622 participants were analyzed. One of the two studies on pre-conception treatment in subclinical hypothyroidism with TSH >4.0 mU/L had high risk of bias and the other was composed of 64 participants. Pre-conception LT4 treatment had no significant effect in improving rates of live births and pregnancies, or reducing miscarriages (risk ratio [RR], 95% confidence interval): 1.41 (0.84–2.36), 1.73 (0.88–3.39), and 0.46 (0.11–2.00), respectively. LT4 treatment during pregnancy was not significantly associated with higher rates of live births (RR 1.03, 0.98–1.09) nor decreased miscarriage rates (RR 1.01, 0.66–1.53). The effect of LT4 treatment on preterm birth during pregnancy was significantly different depending on the TSH values (p = 0.04); a positive effect was shown in the subclinical hypothyroidism subgroup with TSH >4.0 mU/L (RR 0.47, 0.20–1.10), while no significant effect was observed in the subgroup with TSH 2.5–4.0 mU/L (RR 1.35, 0.79–2.31).
Conclusions:
Pre-conceptional LT4 treatment for subclinical hypothyroidism does not improve fertility or decrease the incidence of miscarriages. However, further well-designed studies are needed for pre-conceptional treatment, especially in TSH >4.0 mU/L. LT4 treatment during pregnancy had a positive effect on preterm birth; nevertheless, this was only applicable to subclinical hypothyroidism with TSH >4.0 mU/L.
Introduction
Subclinical hypothyroidism, defined by elevated thyrotropin (TSH) concentrations with normal free thyroxine (fT4) concentrations, is prevalent among women of reproductive age. Subclinical hypothyroidism is associated with multiple adverse pregnancy outcomes, including pregnancy loss, preterm birth, and preeclampsia. 1 –3 Subclinical hypothyroidism negatively affects the outcomes of artificial reproductive technologies (ART) proportional to the increase in TSH levels; hence, the American Thyroid Association guidelines recommends levothyroxine (LT4) supplementation to achieve TSH levels <2.5 mU/L. 4
In real world clinical settings, considering the potential risk of TSH level elevation, LT4 is also prescribed to euthyroid women with TSH levels of 2.5–4.0 mU/L before or during pregnancy; 5,6 however, the beneficial effects in periconceptional subclinical hypothyroidism remain controversial. For thyroid peroxidase antibody (TPOAb)-positive euthyroid women, the limited effectiveness of LT4 has been demonstrated in multiple randomized controlled trials (RCTs). 7 –9 Hence, a systematic review of the literature to clarify the patient groups potentially benefiting from LT4 treatment in pregnancy is needed.
Several systematic reviews and meta-analyses have investigated the effects of LT4 on pregnancy outcomes. 10 –13 However, it is difficult to interpret the efficacy of LT4 in women with subclinical hypothyroidism because of the following limitations: most analyses are composed of studies with heterogeneous levels of evidence, including RCTs and observational studies; the participants in the studies are not limited to those with subclinical hypothyroidism but include those with euthyroidism (TSH levels <2.5 mU/L) or overt hypothyroidism; and the LT4 intervention was not necessarily initiated from early pregnancy.
Therefore, to overcome these limitations, we analyzed only RCTs and strictly extracted the outcomes of subclinical hypothyroidism in the studies that initiated LT4 treatment before or in early pregnancy. We assessed the effect of LT4 before and during pregnancy on subclinical hypothyroidism, including cases with TSH levels >2.5 mU/L, which is the population in which there are questions about the potential treatment benefit.
Materials and Methods
This systematic review was performed based on the principles outlined in the Meta-Analysis of Observational Studies in Epidemiology guidelines 14 and the Cochrane Handbook for Systematic Reviews for Intervention. The study protocol was registered in advance in PROSPERO (CRD42023399795).
The PICO question was as follows: Population (P): women with subclinical hypothyroidism who were planning to become or being pregnant. Intervention (I): LT4 treatment before pregnancy and/or started in early pregnancy (at least within 20 weeks of pregnancy). Comparator (C): placebo or no treatment. Outcome (O): the main outcomes of preconception LT4 treatment were live births, pregnancies, and miscarriages. The main outcomes of LT4 treatment during early pregnancy were live births, miscarriages, and preterm births. Secondary outcomes included hypertensive disorders of pregnancy, preeclampsia, gestational diabetes mellitus, caesarean section, placental abruption, neonatal admission, birth weight, small-for-gestational age, and neurodevelopmental outcomes.
Study design (inclusion criterion): RCTs were included. Case reports, case series, and observational studies were excluded.
Definition of subclinical hypothyroidism
Subclinical hypothyroidism was defined as a normal fT4 level with an elevated TSH level. In the present study, the lower limit of the reference range of TSH was defined as 2.5 mU/L both before and during pregnancy. Considering the physiological fluctuations of TSH in early pregnancy, 15 a normal fT4 and a TSH level of 2.5–4.0 mU/L are usually categorized as subclinical hypothyroidism during pregnancy, but as euthyroid before pregnancy. However, we defined pre-conceptional TSH levels >2.5 mU/L as subclinical hypothyroidism to investigate the efficacy of LT4 in line with actual clinical practice. 4,16
Search strategy
We searched the PubMed, Cochrane Central Register of Controlled Trials, Embase, ClinicalTrials.gov, and WHO International Clinical Trials Registry Platform from inception to February 21, 2023. We updated the search on January 19, 2024. The search words included terms for “subclinical hypothyroidism,” “pregnancy,” or “levothyroxine.” The details of the search strategy for each database are presented in Supplementary Table S1.
Study selection
Two reviewers (A.S. and H.S.) independently screened the titles and abstracts generated from the search results. Disagreements were resolved through a discussion between the two reviewers or a consultation with senior reviewers, if necessary. We contacted the authors for additional information, the extracted outcomes limited to subclinical hypothyroidism.
Data extraction
One reviewer (A.S.) extracted the data, and the other two reviewers (S.K. and M.I.) checked the extracted data independently. The extracted data included the following: first author's name, year of publication, country of study, study population, number of participants (the randomized number and the number of subclinical hypothyroidism patients included), the cut-off TSH level for subclinical hypothyroidism, baseline characteristics (TPOAb positivity, ART, and TSH levels at randomization), details of intervention methods (timing of LT4 treatment initiation, LT4 initial dose and subsequent dose adjustment, and TSH levels after LT4 treatment), and outcomes. Live births, one of the main outcomes, were estimated using the number of participants, miscarriages, and stillbirths in cases where the exact number of live births was not shown in the original study.
Risk of bias
Two reviewers (A.S. and H.S.) independently assessed the risk of bias across the seven domains using the Cochrane Collaboration risk-of-bias tool. 17 The risk of bias in each domain was classified as low, high, or unclear. Disagreements were resolved through a discussion between the two reviewers or a consultation with senior reviewers (E.O. and N.A.), if necessary.
Statistical analysis
All meta-analyses were performed using the RevMan 5.4 (Cochrane Collaboration, Oxford, UK). The pooled effect size was described as risk ratio (RR) with 95% confidence intervals (CIs) for dichotomous outcomes and mean difference and 95% CIs for continuous outcomes. Heterogeneity was assessed using the chi squared (I 2 ) test.
We revised the protocol to use the random effect model regardless of the heterogeneity. The level of statistical significance was set as p < 0.05. Outcomes with p-values <0.1 were considered positive or negative effects. We performed subgroup analyses by dividing the included studies into those where subclinical hypothyroidism was defined by TSH levels of 2.5–4.0 and >4.0 mU/L, respectively. If necessary, studies that did not have a TSH cut-off value of 4.0 mU/L were allocated depending on the upper limit of the reference range. Sensitivity analyses were performed to exclude studies with a high risk of bias.
Results
Study selection and characteristics
A flowchart of the search and selection process for eligible studies is presented in Supplementary Figure S1. The search identified 888 records after excluding 266 duplicates. After screening titles and abstracts, 27 records were identified as potentially relevant. We assessed the full-text articles for these 27 studies and contacted the authors for additional information if necessary. In the studies with women who were euthyroid, only the studies presenting the outcomes for TSH levels >2.5 mU/L separated from the outcomes for TSH levels <2.5 mU/L were included.
In studies with several types of thyroid abnormalities, we contacted the authors to provide outcomes restricted to subclinical hypothyroidism, excluding overt hypothyroidism, isolated hypothyroxinemia, and euthyroidism. We excluded studies that did not provide specific results for subclinical hypothyroidism. The list of the excluded studies through the full-text review process is presented in Supplementary Table S2. Finally, 768 participants in five reports with pre-conception LT4 treatment 7 –9,18,19 and 2622 participants in eight reports with LT4 treatment during early pregnancy 20 –27 were included. The main characteristics of the included reports are shown in Table 1 (preconception) and Table 2 (during pregnancy).
Characteristics of the Included Reports: Levothyroxine Before Pregnancy
The analyzed number in the meta-analysis, excluding participants with TSH <2.5 mU/L and normal fT4.
Shown as median (IQR) or mean (SD).
Provided information from authors.
fT4 were not evaluated.
ART, assisted reproductive technology; CTRL, control; EU, euthyroidism; IQR, interquartile range; LT4, levothyroxine; RPL, recurrent pregnancy loss; SCH, subclinical hypothyroidism; SD, standard deviation; TPOAb, anti-thyroid peroxidase antibody; TSH, thyrotropin.
Characteristics of the Included Reports: Levothyroxine During Pregnancy
The analyzed number in the meta-analysis, excluding participants with isolated hypothyroxinemia, overt hypothyroidism, and TSH <2.5 mU/L with normal fT4.
Shown as median (IQR) or mean (SD). median (95% CI) in Casey et al. 20
Shown as median (IQR) or mean (SD), range.
Provided information from authors.
BW, body weight; CI, confidence interval; SCH, subclinical hypothyroidism; TPOAb, anti-thyroid peroxidase antibody.
Quality of the included studies
The risk-of-bias assessment is shown in Figure 1. Nine reports had a high risk of blinding participants and personnel owing to the lack of a placebo. 7,19,21 –27 One report was considered to have a high risk of other biases as it had 100% pregnancy outcomes in the intervention arm without any biochemical miscarriages. 18 In six reports, we performed a meta-analysis extracting the participants who were eligible for our study: a TSH level over 2.5 mU/L with normal fT4 levels. 7 –9,22–24
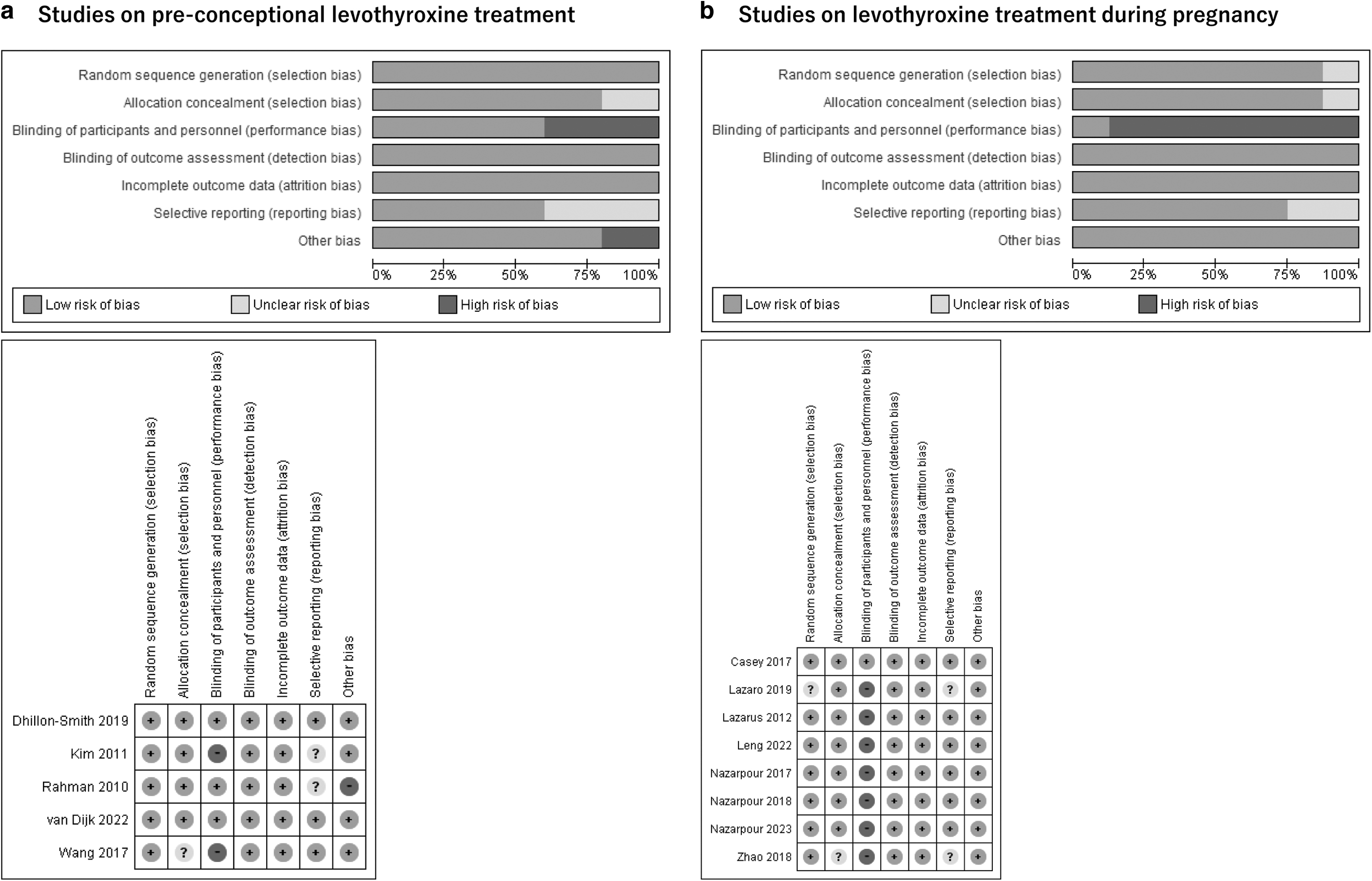
Risk-of-bias assessment and trial quality assessment.
We excluded euthyroidism with a TSH level <2.5 mU/L, isolated hypothyroxinemia, and overt hypothyroidism. 7 –9,22–24 All these six reports originally had low risk of random sequence generation before the extraction of eligible participants for the present study. However, randomization may not be maintained through the extraction process in our analysis.
Effect of pre-conception LT4 treatment
Data on live births were available in all of the five included studies (Fig. 2a). 7 –9,18,19 LT4 treatment did not improve the live birth rate compared with the controls (RR, 95% CI): 1.41, 0.84–2.36; p = 0.20). A high level of statistical heterogeneity was found on pooling the data from these five studies (p < 0.001, I2 = 82%).
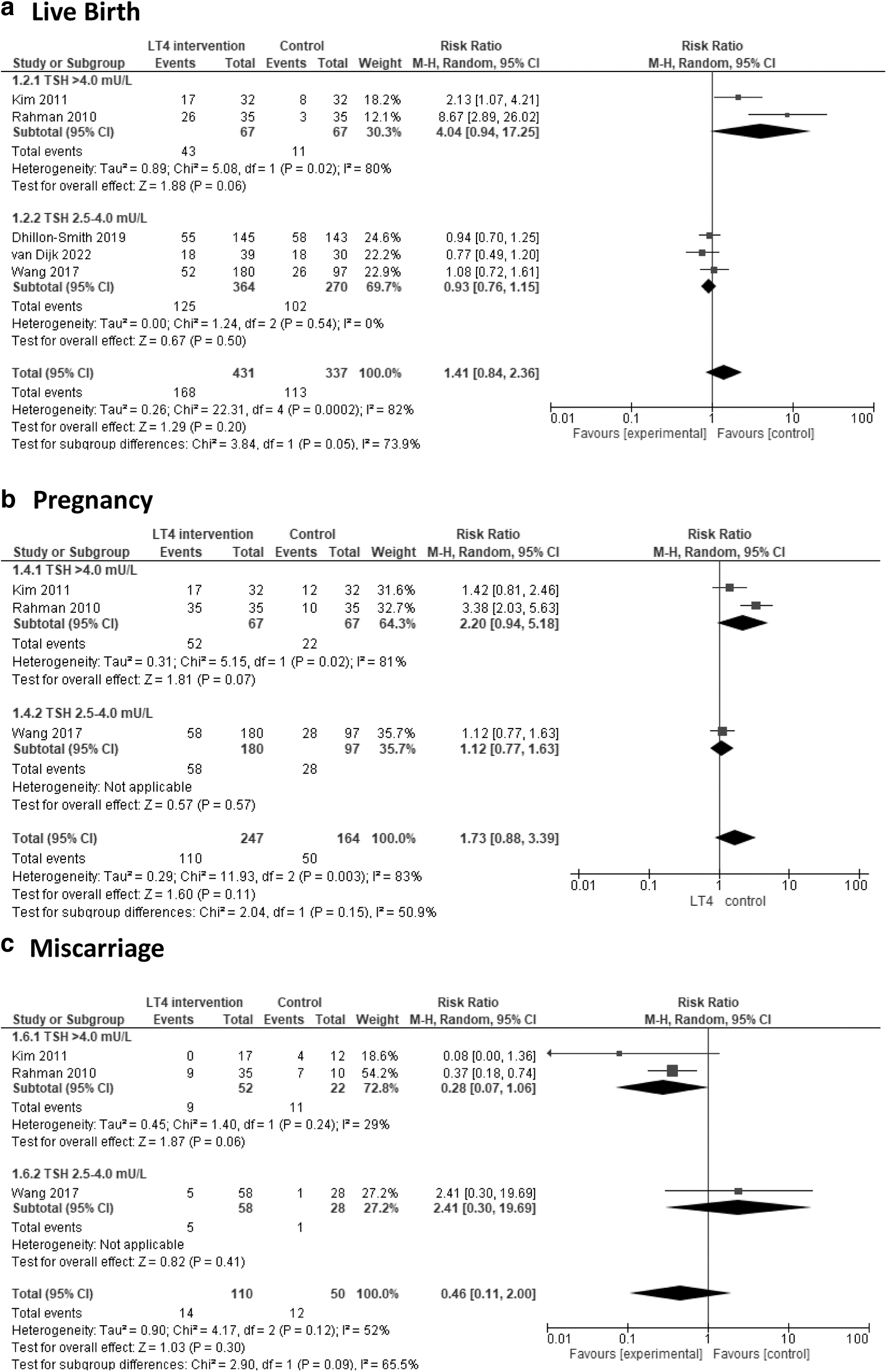
Forest plots presenting the effects of pre-conception LT4 on
Pregnancy rate data were available for three of the included studies (Fig. 2b). 7,18,19 All these three studies were conducted during ART treatment, and the majority of the participants were TPOAb-positive women. LT4 treatment did not improve the pregnancy rate compared with the controls (RR 1.73, 0.88–3.39; p = 0.11). Significantly high heterogeneity existed among the three studies (p = 0.003; I2 = 83%).
Miscarriage data were available for three of the included studies (Fig. 2c). 7,18,19 All these three studies were conducted during ART treatment, and the majority of the participants were TPOAb-positive women. LT4 treatment did not decrease miscarriage rates compared with the controls (RR 0.46, 0.11–2.00; p = 0.30). Moderately high heterogeneity existed among the three studies (p = 0.12, I2 = 52%).
Although tests for subgroup differences showed no significance in all of the three primary outcomes (live birth, I2 = 73.9%, p = 0.05; pregnancy, I2 = 50.9%, p = 0.15; and miscarriage, I2 = 65.5%, p = 0.09, respectively), the potential positive effects for each outcome were more evident in the studies of subclinical hypothyroidism with TSH levels >4.0 mU/L than with TSH levels of 2.5–4.0 mU/L.
The subgroup with TSH levels of 2.5–4.0 mU/L in the analyses on pregnancy and miscarriage is composed of a single study, 7 as we could not obtain data specifically focused on a TSH above 2.5 mU/L in the other two studies. 8,9
In the sensitivity analysis to exclude the study with high risk in other biases, 18 the effect on live birth was significantly different between the subgroups with TSH levels of 2.5–4.0 and >4.0 mU/L (I 2 = 80.5%, p = 0.02). In the subgroup with TSH levels of >4.0 mU/L, consisting of a single study, 19 LT4 treatment significantly improved the live birth rate compared with the controls (RR 2.13, 1.07–4.21; p = 0.03). On the other hand, in the subgroup with TSH levels of 2.5–4.0 mU/L, LT4 treatment did not improve the live birth rate compared with the controls (RR 0.93, 0.76–1.15; p = 0.50) with low risk of heterogeneity (I 2 = 0%, p = 0.54). LT4 treatment did not improve the pregnancy rate and decrease miscarriage rates compared with the controls (RR 1.20, 0.88–1.64; p = 0.24, and RR 0.50, 0.02–14.59; p = 0.69, respectively). Tests for subgroup differences showed no significance in pregnancy and miscarriage (I 2 = 0%, p = 0.49; and I2 = 72.1%, p = 0.06). These results of the sensitivity analyses are shown in Supplementary Figure S2.
Effect of LT4 treatment during pregnancy
Data on live births were available for six of the included studies (Fig. 3a). The pooled estimates suggested that LT4 treatment had no significant effect on live birth rate compared with the controls (RR 1.03, 0.98–1.09; p = 0.23). Significantly high heterogeneity existed among the six studies (p < 0.001; I2 = 87%). Among four of the six studies, we performed subgroup analysis to compare the effects in subclinical hypothyroidism with TSH levels of 2.5–4.0 and >4.0 mU/L (Fig. 3b). The two subgroups showed no significant difference (I 2 = 0%, p = 0.58).
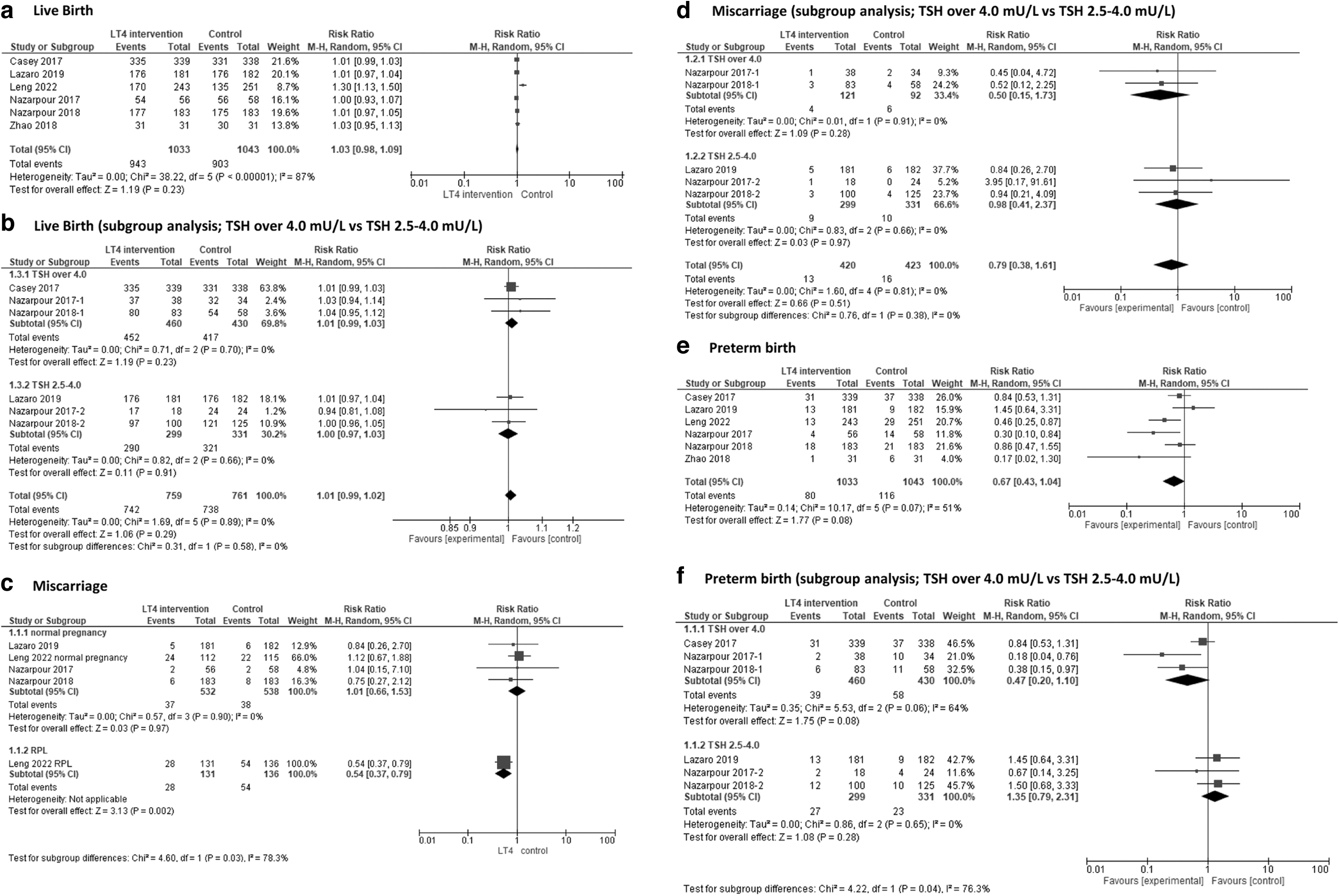
Forest plots presenting the overall effects of LT4 during early pregnancy and subgroup analysis to compare the effects between TSH levels over 4.0 mU/L and TSH levels between 2.5 and 4.0 mU/L on
Miscarriage data were available for five of the included studies (Fig. 3c). We performed subgroup analysis to divide the five studies into two subgroups (I 2 = 78.3%, p = 0.03): women with and without recurrent pregnancy loss. Miscarriage rates among women with recurrent pregnancy loss were significantly decreased by LT4 treatment (RR 0.54, 0.37–0.79; p = 0.002), while the recurrent pregnancy loss subgroup was composed of a single study with 267 participants. However, miscarriage rates were not decreased among women without recurrent pregnancy loss (RR 1.01, 0.66–1.53; p = 0.97). Among three of the four studies without recurrent pregnancy loss, we performed subgroup analysis to compare the effects of LT4 treatment in subclinical hypothyroidism with TSH levels of 2.5–4.0 and >4.0 mU/L (Fig. 3d). There was no significant difference between the two subgroups (I 2 = 0%, p = 0.38).
Data on preterm births were available for six of the included studies (Fig. 3e). The pooled estimates suggested that LT4 treatment showed a positive effect in decreasing the incidence of preterm birth, compared with the case for the controls, without statistical significance (RR 0.67, 0.43–1.04; p = 0.08). Moderately high heterogeneity existed among the six studies (p = 0.07, I2 = 51%).
We performed a subgroup analysis with four of the six analyzed studies to compare the effects of LT4 treatment in subclinical hypothyroidism with TSH levels of 2.5–4.0 and >4.0 mU/L (Fig. 3f). There was significant difference between the two subgroups (I 2 = 76.3%, p = 0.04). Although LT4 treatment showed positive effect to decrease the incidence of preterm birth in the TSH >4.0 mU/L subgroup (RR 0.47, 0.20–1.10; p = 0.06), no effect was observed on preterm birth in the TSH 2.5–4.0 mU/L subgroup (RR 1.35, 0.79–2.31; p = 0.28).
Other pregnancy outcomes were analyzed, including: hypertensive disorders of pregnancy, preeclampsia, gestational diabetes mellitus, caesarean section, placental abruption, neonatal admission, small for gestational age, neonatal birth weight, and neurodevelopmental outcomes in childhood (intelligence quotient). No significant effect of LT4 treatment was observed for any of these outcomes (Supplementary Fig. S3).
Nazarpour et al., 26 in a follow-up study of Nazarpour et al., 24,25 investigated neurodevelopmental outcomes at the age of 3 years using the Ages and Stages Questionnaires to show no significant effect of LT4 in four of the five domains (communication, gross motor, fine motor, problem-solving, and social-personal domains), excluding gross motor.
Discussion
To the best of our knowledge, our study is the first to exclusively focus on RCTs and to perform subgroup analyses focused on pregnant patients with subclinical hypothyroidism, including the subgroups of TSH levels of 2.5–4.0 and >4.0 mU/L.
Previous meta-analyses included studies of variable quality levels of evidence and variable eligibility of participants; euthyroidism with TPOAb positivity, subclinical hypothyroidism, and overt hypothyroidism. 10,11,13,28 –31 Hence, there have been discrepancies in the results, and the subgroups that can derive the most benefit from LT4 treatment remain unclear, that is, the TSH cutoff values, TPOAb positivity, the number of previous pregnancies lost, and the regimen of LT4 treatment.
However, there has been a marked increase in periconceptional LT4 prescriptions and the threshold for initiating LT4 treatment has declined over the past decade. 5,6,32
Although statistical significance was not observed in any subgroup analyses involving pre-conceptional LT4, the most benefit was observed in the subgroup where subclinical hypothyroidism was defined by TSH levels of >4.0 mU/L (live birth: RR 4.04, 0.94–17.25; p = 0.06, pregnancy: RR 2.20, 0.94–5.18; p = 0.07, miscarriage: RR 0.28, 0.07–1.06; p = 0.06).
The three high-quality RCTs among TPOAb positive women who have experienced infertility or pregnancy loss showed consistent result that pre-conception LT4 did not improve live births in subclinical hypothyroidism with TSH levels between 2.5 to 4.0 mU/L (p = 0.50, I 2 = 0%). 7 –9 However, further studies are needed for TSH levels of >4.0 mU/L, considering the small sample size and the fact that one of the two studies, Rahman 2010, was subject to a high risk in other bias. 18 Based on the current evidence, we believe that the target population for pre-conception LT4 treatment should be narrowed down to those with subclinical hypothyroidism with TSH levels of >4.0 mU/L.
In the present analysis of LT4 administration during pregnancy, no effects on live births or miscarriages were observed. While the critical period for miscarriage is the early phase within the first trimester of pregnancy, 33 LT4 treatment was initiated at almost the end of the first trimester in many of the included studies. Thus, the present analysis of LT4 treatment during pregnancy might be inappropriate for assessing the effect on miscarriages and live births.
Alcazar Lazaro et al. 21 and Leng et al. 23 did not show significantly decreased incidence rates of miscarriages with LT4 treatment, although LT4 was initiated within the first trimester. The limited impact of LT4 on miscarriage might be because the estimated risk of subclinical hypothyroidism may not be as important as the other risk factors for early pregnancy loss, including maternal age, diabetes mellitus, and obesity.
Leng et al. showed a significant effect of LT4 in preventing miscarriage in subclinical hypothyroidism patients with recurrent pregnancy loss. 23 Two observational studies investigated the effect of LT4 on recurrent pregnancy loss in subclinical hypothyroidism patients and found no significant effects. 34,35 No other RCTs have primarily investigated the effects of LT4 in women with recurrent pregnancy loss. Van Dijk et al. 9 and the subgroup analysis by Dhillon-Smith et al. 8 showed no significant effect of LT4 in preventing miscarriage in TPOAb-positive euthyroid participants with recurrent pregnancy loss. Although not statistically significant, van Dijk et al. showed a tendency of reduced pregnancy loss rates in the LT4 group compared with that in the placebo group (23% and 33%, respectively). 9 Further studies are needed to clarify whether recurrent pregnancy loss is treatable with LT4 in subclinical hypothyroidism.
LT4 treatment was shown to reduce the incidence of preterm births during pregnancy. Notably, this effect was observed only in the subgroup with TSH levels >4.0 mU/L, but not in the subgroup with TSH levels of 2.5–4.0 mU/L. The subgroup with TSH levels of 2.5–4.0 mU/L mainly comprised TPOAb-negative women. In an independent-patient-data meta-analysis by the Consortium on Thyroid and Pregnancy, the association between subclinical hypothyroidism and preterm birth was no longer apparent after additional adjustment for TPOAb positivity. Further studies investigating the association between TPOAb positivity and TSH levels are needed to identify the optimal TSH target for LT4 treatment to prevent preterm birth.
In the present study, no significant negative effects of LT4 on adverse pregnancy outcomes were observed. In the retrospective cohort study, Maraka et al. reported a higher risk of preterm birth, preeclampsia, and gestational diabetes mellitus in the LT4 group than in the control group. 36 The follow-up study of the Controlled Antenatal Thyroid Screening Study 20 for children around the age of 9 of the mothers with suboptimal gestational thyroid function showed increased risk of attention deficit hyperactivity disorder symptoms and behavioral difficulties in the overtreated group compared with the untreated group. 37
Recent independent patient data meta-analyses have shown that high-to-normal fT4 levels within the reference range, which are compatible with LT4 treatment, are associated with an increased risk of lower neonatal birthweight. 38 Moreover, the low-to-normal TSH levels within the reference range were shown to be associated with an increased risk of preeclampsia. 3 These findings indicate that LT4 overtreatment, even within the normal range, may lead to potential harm.
Yang et al. showed a U-shaped association between pre-conception TSH levels and adverse pregnancy outcomes, including preterm birth and small for gestational age, in a large-scale population-based cohort study, indicating that the optimal target ranges of TSH and fT4 might be quite narrow. 39 Two of the studies on pre-conceptional LT4 8,9 and four of the studies on LT4 during pregnancy 23 –27 had no dose adjustment after treatment initiation, raising concerns about overtreatment. The effects of LT4 might have been underestimated due to the potential overtreatment. Reconsidering the possibility of overtreatment and verifying the optimal target for LT4 treatment is necessary.
Since the early 2010s, several guidelines have recommended LT4 treatment before 40 or during pregnancy 4,16,40 at a TSH threshold of 2.5 mU/L, despite a lack of sufficient evidence. However, over the past half decade, multiple RCTs have been conducted to determine the appropriate treatment targets. The results of the present study suggest there is a need to reconsider the TSH threshold for LT4 treatment both before and during pregnancy.
The main strength of our study is the strict definition of subclinical hypothyroidism and the subgroup analysis based on TSH values. We exclusively analyzed RCTs and extracted the results of eligible participants, excluding those with isolated hypothyroxinemia, overt hypothyroidism, or euthyroidism with TSH levels <2.5 mU/L. A limitation of our study is the lack of important data, including those for TPOAb positivity and TSH values after LT4 treatment.
In conclusion, in this systematic review and meta-analysis, pre-conception LT4 treatment had no effects on live births, pregnancies, or miscarriages in subclinical hypothyroidism with TSH levels of 2.5 to 4.0 mU/L. Evidence investigating the effects of LT4 treatment for subclinical hypothyroidism with TSH levels >4.0 mU/L is still insufficient. In secondary analyses, we found that LT4 treatment in early pregnancy has the potential to reduce preterm birth rates, but this benefit was observed only among individuals with TSH levels >4.0 mU/L. Further well-designed clinical trials are needed to determine the beneficial effects of LT4 treatment, stratifying for both the TSH and TPOAb levels.
Footnotes
Acknowledgments
The authors thank Prof. Fahimeh Ramezani Tehrani for sending additional data for this study on Nazarpour 2017 and 2018. The data enabled us to perform a detailed subgroup analysis. This study was conducted in collaboration with members of the committee of the Japan Thyroid Association (JTA) to investigate the diagnosis and treatment of subclinical thyroid dysfunction during pregnancy. The authors also thank Dr. Akira Hisinuma, chair of the JTA, and Dr. Masanobu Yamada, chair of the committee. They thank Cochrane Japan (
Authors' Contributions
A.S.: Study selection and assessment (lead), formal analysis (lead), writing–original draft (lead), and review and editing (equal). N.A.: Conceptualization (lead), writing–review and editing (equal). H.S.: Study selection and assessment (supporting), methodology (equal), formal analysis (supporting), and review and editing (equal). E.O.: Methodology (lead), review and editing (equal). M.I., A.Y., S.K., M.K., K.H., Y.H., A.Y., H.N., S.K., M.K.-K., A.I., and T.S.: Conceptualization (supporting), review and editing (equal).
Author Disclosure Statement
N.A., H.N., and A.Y. received speaking fees from ASKA Pharmaceutical Co., Ltd. The other authors have nothing to declare.
Funding Information
This study was supported by a grant from the Children and Families Agency (Grant No.: 23DA0201). The funder had no role in the study. N.A. received the funding. The other authors do not receive any funding to support this study.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2