
Abstract
Background:
Hypothyroidism is a common endocrine condition and chronic thyroid hormone deficiency is associated with adverse effects across multiple organ systems. In compensated hypothyroidism, however, patients remain clinically stable due to gradual physiological adaptation. In contrast, the clinical syndrome of decompensated hypothyroidism referred to as myxedema coma (MC) is an endocrine emergency with high risk of mortality. Because of its rarity, there are currently limited data regarding MC. This study analyzes the clinical features and hospital outcomes of MC compared with hypothyroid patients without MC (nonMChypo) in national United States hospital data.
Methods:
A retrospective analysis of the National Inpatient Sample, a public database of inpatient admissions to nonfederal hospitals in the United States, 2016–2018, including adult patients with primary diagnosis of MC (International Classification of Diseases 10th Revision [ICD-10]: E03.5) or nonMChypo (E03.0–E03.9, E89.0). Patient demographics, relevant clinical features, mortality, length of stay (LOS), and hospital costs were compared.
Results:
Of 18,635 patients hospitalized for hypothyroidism, 2495 (13.4%) had a diagnosis of MC. Sex distribution and race/ethnicity were similar between patients with MC and nonMChypo, whereas MC was associated with older patient age (p = 0.02), public insurance (p = 0.01), and unhoused status (p = 0.04). More admissions with MC occurred in winter compared with other seasons (p = 0.01). The overall mortality rate for MC was 6.8% versus 0.7% for nonMChypo (p < 0.001), and MC was independently associated with in-hospital mortality after adjusted regression analysis (adjusted odds ratio = 9.92 [CI 5.69–17.28], p < 0.001). Mean LOS ± standard error was 9.64 ± 0.73 days for MC versus 4.62 ± 0.12 days for nonMChypo (p < 0.001), and total hospital cost for MC was $21,768 ± $1759 versus $8941 ± $276 for nonMChypo (p = 0.07). In linear regression analyses, MC was an independent predictor of both increased LOS and total hospital cost.
Conclusions:
In summary, MC remains a clinically significant diagnosis in the modern era, independently associated with high mortality and health care costs. This continued burden demonstrates a need for further efforts to prevent, identify, and optimize treatment for patients with MC.
Introduction
Hypothyroidism is a common endocrine disease resulting from insufficient thyroid hormone that can have deleterious effects across multiple organ systems, affecting thermoregulation, cardiac chronicity and contractility, respiratory drive, and cognition. 1,2 Untreated, these effects of hypothyroidism can impair the body's ability to respond to episodes of physiological stress, such as infection, myocardial infarction, or trauma. 1 In compensated hypothyroidism (CH), patients remain clinically stable due to gradual physiological adaptation. By contrast, the clinical syndrome of severe long-standing hypothyroidism with physiological decompensation referred to as myxedema coma (MC), or myxedema crisis, is an endocrine emergency with high risk of mortality.
Hallmark clinical signs that distinguish the physiological decompensation of MC from usual or CH include altered mentation, hypothermia, and hemodynamic instability. 1 Importantly, this decompensated form of severe hypothyroidism carries a marked mortality risk, estimated at 26–52% in modern era studies. 3 –6 Furthermore, in contrast to CH that can be treated with gradual thyroid hormone replacement, MC requires the rapid initiation of hormone therapy and intensive supportive care measures to prevent adverse clinical outcomes. 7
Given the rarity of MC, direct comparisons in the literature between MC and severe, but CH have been limited. These prior reports, comprising several small, single-center studies, 3,4,8 one multicenter study, 6 and one analysis of 149 patients from Japan's national inpatient database, 5 suggest higher morbidity and mortality in MC, but do not yet provide a full picture of the current burden of disease, patient clinical features, and hospital outcomes.
Therefore, we utilized the Agency for Healthcare Research and Quality's Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS) database to construct the largest MC sample to date. We evaluated how demographic and clinical characteristics were associated with patient mortality and hospitalization costs in MC and compared them with a cohort of patients with patients hospitalized for hypothyroidism without MC in the United States.
Methods
We performed a retrospective analysis examining hospital discharge data for patients with a primary diagnosis of hypothyroidism with or without MC from the NIS. The NIS is a large publicly available all-payer inpatient health care database in the United States that approximates a 20% stratified sample of all discharges from nonfederal U.S. hospitals. The NIS is drawn from all states participating in HCUP, covering more than 97% of the U.S. population.
Each entry represents one hospital discharge and includes 40 associated diagnosis and 25 associated procedure International Classification of Diseases 10th Revision (ICD-10) codes. The database includes data on patient and hospital demographics, mortality, length of stay (LOS), and charges. It does not include clinical information such as laboratory data.
We used data from 2016 to 2018 as 2016 was the first year that the ICD-10 code for MC was used in the database. We included patients 18 years of age or older, nonelective admissions, and with a principal diagnosis of hypothyroidism for their hospitalization. Patients were then subcategorized based on ICD-10 coding as either having MC using ICD-10 code E03.5, or hypothyroidism without MC (nonMChypo) using ICD-10 codes E03.0–E03.3, E03.8, E03.9, and E89.0. The principal diagnosis was defined as the first listed diagnosis for a hospital discharge that was responsible for “occasioning the admission” of the patient. 9
To generate national estimates, we used survey analysis techniques to account for the stratification, weighting, and clustering of the NIS database. 9 Since patients diagnosed with MC would universally have an inpatient hospital admission, we calculated the annual incidence of MC by dividing the estimated number of MC hospital discharges in 2016–2018 by the number of individuals in the general population of the United States in the corresponding years. 10 This calculation was based on the HCUP Methods Series Document, 11 which describes the ability to determine the incidence of disorders, such as MC, that are likely to have a relatively acute period of onset and are likely to result in a hospital admission.
Preselected diagnoses across organ systems potentially relevant to hypothyroidism and MC were included for analysis. To assess comorbid medical conditions that could impact the occurrence of MC and/or the prognosis, Charlson comorbidity index (CCI) was calculated with a modified algorithm using ICD-10 coding. 12,13 The outcomes of interest included demographics, clinical characteristics, LOS, hospital mortality, and hospital costs. Patients with a principal inpatient diagnosis of MC were compared with patients with a principal diagnosis of nonMChypo.
Continuous variables are reported as mean with standard error (SE) and design-adjusted F-tests were used to compare continuous variables between the two groups. Categorical variables are shown as numbers with percentage and design-adjusted chi-squared tests for independence were used for comparisons between groups. Mortality was calculated for both groups and compared with a design-adjusted F-test. Independent predictors of mortality were determined by calculating odds ratios (OR) using univariable logistic regressions. Variables with p < 0.1 were included in a multivariable logistic regression to calculate an adjusted odds ratio (aOR) for independent predictors of mortality.
Mean LOS and mean cost were calculated for both groups and compared with T-test. Mean cost was calculated by adjusting total charges using the NIS-provided cost-to-charge ratio supplement. Predictors of LOS and total cost were determined by multivariable linear regressions. All statistical analyses were performed using STATA (Version 18.0; StataCorp LLC, College Station, TX). A p-value of <0.05 was considered statistically significant. This study has exempt status by the governing Institutional Review Board.
Results
From 2016 to 2018, there were 18,635 hospital discharges in the United States for patients 18 years of age or older with a primary diagnosis of hypothyroidism, after exclusion of elective admissions (Fig. 1). Of these, 2495 (13.4%) were identified as MC, while 16,140 (86.6%) were considered nonMChypo (Supplementary Table S1). The most common codes used in the nonMChypo group were unspecified hypothyroidism (12,295 [76.2%]) and postprocedural hypothyroidism (2360 [14.6%]). Using the population of the United States by corresponding year from the U.S. Census Bureau, the estimated incidence of hospitalization for MC was 2.56 cases per 1 million U.S. persons per year from 2016 to 2018. Thus, MC remains a rare but important endocrine diagnosis in the United States.
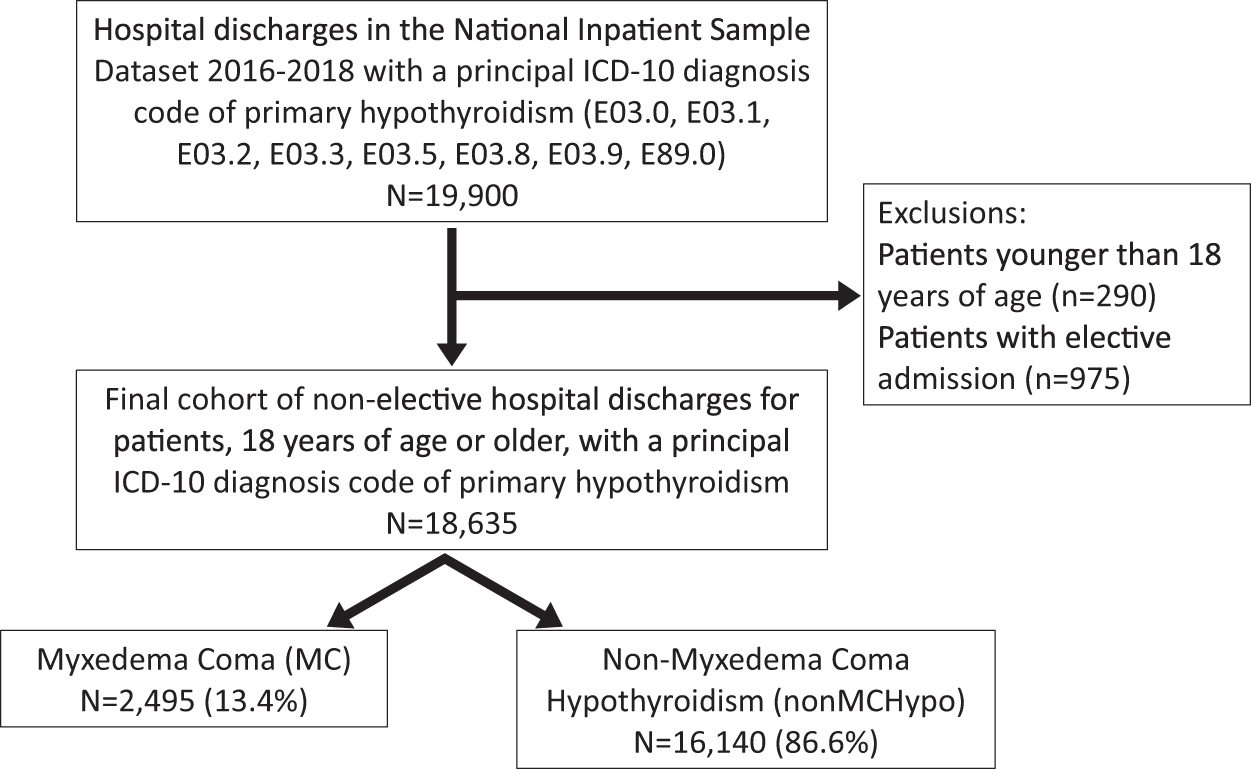
Participant flowchart diagram.
The population demographics for hospitalizations for MC and nonMChypo are shown in Table 1. Patients hospitalized with MC were slightly older, with a mean age ± SE of 66.13 ± 0.72 years compared with 63.41 ± 0.32 years for patients with nonMChypo (p < 0.001). A trend was observed toward a lower proportion of MC hospitalizations for patients with Hispanic and other race/ethnicity that did not reach statistical significance (p = 0.08).
Population Description for Patients Admitted for Hypothyroidism in the National Inpatient Sample Stratified by Myxedema Coma Diagnosis
SE, standard error.
More MC patients had Medicare insurance (63.2% vs. 56.5%, p = 0.01). MC was associated with higher CCI (p < 0.001, Table 1), with an index of ≥3 in 42.9% of MC hospitalizations versus 31.8% of nonMChypo hospitalizations. Overall, more U.S. admissions for MC occurred in the winter season compared with fall, summer, or spring (30.3% of admissions for hypothyroidism compared with 21.0–25.1% in other seasons, p = 0.02, Supplementary Table S2).
To investigate further the role of temperature variability in precipitating MC hospitalizations, data were stratified by region (Supplementary Table S3). A greater percentage of MC hospitalizations occurred in the winter for the Midwest (36.7%) and Northeast (40.2%) compared with the West (28.7%) and South (23.4%) regions (p = 0.02), consistent with colder seasonal temperatures in the former. No other statistically significant differences were found in demographic variables. In summary, patients with MC were older, more likely to have Medicare insurance, and most often presented in the winter season compared with nonMChypo.
Associated diagnoses and acute care utilization
Additional ICD-10 codes during each hospitalization were analyzed to assess diagnoses and acute hospital care interventions for patients with MC compared with nonMChypo (Table 2). MC diagnosis was associated with higher rates of vital sign abnormalities (e.g., hypothermia, bradycardia, and hypotension), metabolic abnormalities, and signs of multiorgan failure (e.g., altered mental status, heart failure, respiratory failure, renal failure, and hepatic failure). The percentage of patients with cardiac tamponade, constipation, and medication noncompliance were not associated with MC compared with nonMChypo.
Associated Diagnoses in Hospitalized Patients with Myxedema Coma or Non-Myxedema Coma Hypothyroidism
Table 3 shows the use of supportive measures for acute care during hospitalization for patients with MC and nonMChypo. Diagnosis of MC compared with nonMChypo was associated with a higher rate of noninvasive ventilation (5.4% vs. 1.7%, p < 0.001), intubation (17.4% vs. 0.8%, p < 0.001), hemodialysis (6.6% vs. 2.4%, p < 0.001), vasopressor use (2.8% vs. 0.1%, p < 0.001), cardiac-assist device use (0.2% vs. 0.0%, p = 0.01), as well as a trend toward higher use of cardiac pacing (0.4% vs. 0.1%, p = 0.08).
Adjunctive and Acute Supportive Care in Patients Hospitalized for Hypothyroidism, Stratified by Myxedema Coma Diagnosis
Thus, these data show that patients with MC require significantly higher levels of care and medical intervention, particularly around cardiopulmonary support, during hospitalizations compared with those with nonMChypo. In summary, MC was strongly associated with signs of hemodynamic decompensation and end-organ dysfunction.
Mortality
The estimated in-hospital mortality was 6.8% for patients hospitalized with MC compared with 0.7% for patients hospitalized with CH (p < 0.001). In a univariate analysis of all patients with a primary diagnosis of hypothyroidism (Table 4), MC was strongly associated with higher mortality compared with nonMChypo (OR = 10.19 [confidence interval, CI 5.96–17.43], p < 0.001). Other factors associated with higher mortality (Table 4) were age greater than 65 years compared with age 18–40 years (p = 0.02), Medicaid compared with Medicare insurance type (p = 0.03), Midwest region (p = 0.02), or West region (p = 0.04) compared with the Northeast, presentation in the fall (p = 0.02), winter (p = 0.04), or spring (p = 0.04) compared with summer, and CCI greater than zero (p = 0.01 for all comparisons).
Predictors of Mortality in Patients Hospitalized for Hypothyroidism in the National Inpatient Sample
The multivariable logistic regression showed that a diagnosis of MC remained independently associated with in-hospital mortality compared with nonMChypo (aOR = 9.92 [CI 5.69–17.28], p < 0.001). Midwest region (OR = 3.02 [CI 1.06–8.58], p = 0.04), fall (OR = 4.23 [CI 1.56–11.47], p = 0.01), or spring season, and CCI compared with zero (ORCCI=1 = 6.23 [1.89–20.50], p = 0.01; ORCCI=2 = 3.61 [0.99–13.25], p = 0.05; ORCCI ≥3 = 3.40 [1.04–11.10], p = 0.04) also were significant in multivariable analysis (Table 4).
To further investigate predictors of mortality in MC, univariable and multivariable regression analyses were performed specifically in only patients with a primary diagnosis of MC (Table 5). Demographic variables that were independently predictive of mortality in patients with MC included age greater than 65 years old compared with 18–40 years old (OR = 8.17 [CI 1.48–45.24], p = 0.02) and large hospital size (OR = 3.01 [CI 1.08–8.40], p = 0.04).
Predictors of Mortality in Patients Hospitalized for Myxedema Coma in the National Inpatient Sample
Similar to the overall study population, CCI was an independent predictor of mortality in MC (ORCCI=1 = 25.12 [5.84–108.10], p < 0.001; ORCCI ≥3 = 6.15 [1.41–26.75], p = 0.02). Individual clinical variables independently predictive of mortality were cardiogenic shock (OR = 13.49 [CI 2.87–64.41], p = 0.01), cardiac arrest (OR = 8.94 [1.08–74.10], p = 0.04), acute renal failure (OR = 3.52 [1.34–9.21], p = 0.01), and septicemia (OR = 4.29 [1.07–17.23], p = 0.04).
LOS and costs
The mean LOS ± SE for patients hospitalized with MC was 9.64 ± 0.73 days compared with 4.62 ± 0.12 days for patients hospitalized with nonMChypo (p < 0.001), suggesting a near doubling of in-hospital time in MC. In a multivariable linear regression, diagnosis of MC (p < 0.001), age 40–65 (p < 0.001), large hospital size (p = 0.01), and CCI (p = 0.01 for 1, p = 0.01 for 2, p < 0.001 for ≥3) were associated with increased LOS (Table 6). Hispanic race (p = 0.01), private insurance (p = 0.01), and Midwest hospital region (p = 0.01) were associated with decreased LOS.
Predictors of Length of Stay for Hospitalizations with Primary Diagnosis of Hypothyroidism
Longer hospitalization LOS and greater need for supportive interventions would suggest that MC is associated with more costly care. Indeed, the mean total hospitalization cost for MC was $21,768 ± $1759 compared with $8941 ± $276 for hospitalizations for nonMChypo (p = 0.07). In a multivariable linear regression model evaluating all patients with hypothyroidism (MC or nonMChypo) for factors associated with total hospital cost (Table 7), we found that increased total cost was positively associated with MC (p < 0.001), age between 40 and 65 years old (p = 0.01), Black racial designation (p = 0.02), large hospital size (p = 0.03), and all CCI categories greater than zero (p < 0.001).
Predictors of Total Hospital Cost for Hospitalizations with Primary Diagnosis of Hypothyroidism
Medication nonadherence (p = 0.02) and Midwest (p < 0.001) or South (p < 0.001) regional location were associated with decreased total cost. In summary, individuals hospitalized for MC, compared with those hospitalized for nonMChypo, required longer and more costly hospital care that related to their hypothyroidism diagnosis.
Discussion
MC represents a rare decompensated physiological state typically occurring in severe hypothyroidism when there is a precipitating illness or physiological stress. 1,14 The rarity of this diagnosis is a substantial barrier to robust analyses due to small sample sizes of clinical data, which may have been observed over long periods of time and evolving standards of medical care. This study is the first analysis of MC using a large sample from national hospitalization data in the United States, and investigates its frequency, associated diagnoses, and hospital outcomes. Most notably, these results show that MC remains associated with higher in-hospital mortality, hospital LOS, and higher hospital costs compared with hospitalizations for hypothyroidism without MC in modern U.S. hospitals.
Using the U.S. NIS data from 2016 to 2018, the estimated incidence of MC was 2.56 cases per 1 million U.S. persons per year. This is similar to the incidence found in the national inpatient database study from Japan, which estimated an incidence of 1.08 cases per 1 million Japanese persons per year in 2012. 5 Hospitalization for MC accounted for 13.5% of all hospitalizations with a primary discharge diagnosis of hypothyroidism in the NIS from 2016 to 2018.
Although this could be viewed as a substantial proportion, patients infrequently require hospitalization for a primary diagnosis of hypothyroidism and, therefore, we postulate that when hospitalization is required, patients more commonly have severe hypothyroidism and higher likelihood of MC. Furthermore, a smaller single-center study 8 corroborates our data where they showed a similar rate of 14% of MC in a group of patients admitted from the emergency department with newly diagnosed primary overt hypothyroidism.
Patients with MC were more likely to be female, above age 65 years, and Caucasian, which is similar to our findings in the nonMChypo population. These data also indicated an association between MC diagnosis and insurance type, with a higher percentage of MC patients with Medicare compared with private insurer, likely related to the older age of these patients compared with patients without MC. Numerous diagnoses suggesting worse clinical severity were more common in patients with MC, such as cardiac, respiratory, hepatic, and renal conditions (Table 2).
However, because temporal relationships between hospital discharge diagnoses are not available, it is not possible to determine if these were precipitants of MC or conditions that occurred during hospitalization. With respect to variables associated with hospitalization for MC, seasonal variation was of particular interest since previous opinions have suggested increased presentations during colder weather. 3 –5,8 The findings of this study provide data from the United States to support this clinical observation. MC was relatively more frequent in the winter. Furthermore, the increase in admissions during the winter was most pronounced in the Northeast and Midwest, where winter temperatures are lower, compared with the South or West.
We identified that MC had an estimated in-hospital mortality of 6.8% (compared with only 0.7% for nonMCHypo) and an adjusted hazard ratio for mortality of 9.92 ([CI 5.69–17.28], p < 0.001) in multivariable analysis (Table 4). This mortality rate is lower than previous reports. A study of 149 patients with MC between 2010 and 2013 from a national inpatient database in Japan reported an in-hospital mortality of 29.5%. 5 A multicenter study of French intensive care units from 2000 to 2017 found a mortality rate of 26% among 82 patients with MC. 6 A number of potential explanations may account for the difference between these data and our findings.
It is possible that the ICD-10 code was used for patients with less severe hypothyroidism in the NIS data set. However, it is unlikely that the newer ICD-10 code specific for MC would be broadly misapplied since MC was significantly associated with diagnoses of hypothermia and altered mentation, consistent with clinical diagnostic criteria. 1,15 Patients with MC also were more likely to have metabolic abnormalities, multiorgan failure, and treatment with intubation, vasopressors, and hemodialysis, confirming the expected greater severity compared with patients with nonMCHypo. We hypothesize that one explanation for the lower mortality observed in this analysis may relate to improved acute hospital and intensive care unit level care in the more recent time period of our data compared with previous studies.
In addition, oral levothyroxine replacement was frequently used for patients reported in previous studies, 4 –6 whereas it is likely that intravenous levothyroxine predominated under United States recommendations during this time. 7 This also may be a factor in MC mortality, although observational retrospective studies have suggested equivalent outcomes. 16,17 Future studies using individual patient-level data to identify treatments associated with improved outcomes in patients with MC are warranted.
The analysis to elucidate predictors of mortality in patients with MC revealed several independently associated variables (Table 5), of which more advanced age (>65 years old), presence of comorbidities, and diagnoses related to organ failure were the most significant findings. The significant association between cardiogenic shock, cardiac arrest, and acute renal failure are not unexpected as markers of severe illness. A diagnosis of septicemia also was found to be a significant independent predictor. Unlike end-organ dysfunction, septicemia could more likely be a precipitant of MC rather than a consequence of it. Thus it may be an important predictor of mortality to consider in the presentation of MC, although this speculation requires further confirmation.
These are the first data to address total cost for MC hospitalization in the United States and showed a strong trend toward substantially greater mean total cost of $21,768 ± $1759 compared with $8941 ± $276 for patients hospitalized with nonMChypo (p = 0.07). The mean LOS for patients hospitalized with MC of 9.64 ± 0.73 days was significantly longer than 4.62 ± 0.12 days observed in patients with nonMChypo (p < 0.001). Taken together, these data highlight the current burden of MC patient care on U.S. hospitals.
There are limitations of this study to acknowledge. Although the data captured in the NIS are retrospective and uncontrolled, they still represent current real-world patient care for U.S. hospital admissions. The diagnosis of MC and other diagnoses are based on ICD-10 codes used during clinical care and are dependent on their accurate use. In this study, there were some patients with MC that did not have canonical symptoms such as altered mentation or hypothermia, and some patients without MC who did have such associated diagnoses, raising some question as to the validity of these diagnoses.
In addition, diagnosing MC relies on identifying a clinical syndrome for which there is no gold standard, and the criteria may not be consistent across providers. Greater adoption of standardized criteria, such as the quantitative scoring systems recently proposed, 15 may increase the consistency of MC diagnosed with clinical databases such as the NIS. Nevertheless, the study provides a broad national analysis with the diagnosis code as currently utilized in the United States.
The NIS database provides valuable information to understand incidence, and demographic and clinical characteristics of the rare disease in the United States and has been used in other landmark studies in the thyroid field. 18 –20 However, these data do not contain detailed clinical, laboratory, or treatment information, including the route and dose of thyroid hormone therapy, to further assess how these variables might be associated with diagnosis and outcomes. The NIS does not contain information to link potential multiple admissions over time from the same patient and thus the statistical analysis assumes each admission is considered an independent instance of MC.
In conclusion, the incidence of MC in the United States between 2016 and 2018 was 2.56 cases per 1 million U.S. persons per year, with a mortality rate of 6.8%. In addition, the diagnosis of MC was associated with higher mortality, longer hospital LOS, and greater hospital costs compared with those hospitalized for hypothyroidism without MC, which highlights the need for ongoing efforts to prevent, identify, and optimize treatment for this disease.
Footnotes
Authors' Contributions
Conceptualization, methodology, software, formal analysis, investigation, and writing—original draft by D.H.C. Conceptualization, validation, and writing—review and editing by C.R.H. Methodology, software, and writing—review and editing by P.C. Conceptualization and writing—review and editing by M.Z. Conceptualization, methodology, writing—review and editing, and supervision by T.E.A.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3