
Abstract
Background:
Hypothyroidism is common, however, aspects of its treatment remain controversial. Our survey aimed at documenting treatment choices of European thyroid specialists and exploring how patients' persistent symptoms, clinician demographics, and geo-economic factors relate to treatment choices.
Methods:
Seventeen thousand two hundred forty-seven thyroid specialists from 28 countries were invited to participate in an online questionnaire survey. The survey included respondent demographic data and treatment choices for hypothyroid patients with persistent symptoms. Geo-economic data for each country were included in the analyses.
Results:
The response rate was 32.9% (6058 respondents out of 17,247 invitees). Levothyroxine (LT4) was the initial treatment preferred by the majority (98.3%). Persistent symptoms despite normal serum thyrotropin (TSH) while receiving LT4 treatment were reported to affect up to 10.0% of patients by 75.4% of respondents, while 28.4% reported an increasing such trend in the past 5 years. The principal explanations offered for patients' persistent symptoms were psychosocial factors (77.1%), comorbidities (69.2%), and unrealistic patient expectations (61.0%). Combination treatment with LT4+liothyronine (LT3) was chosen by 40.0% of respondents for patients who complained of persistent symptoms despite a normal TSH. This option was selected more frequently by female thyroid specialists, with high-volume practice, working in countries with high gross national income per capita.
Conclusions:
The perception of patients' dissatisfaction reported by physicians seems lower than that described by hypothyroid patients in previous surveys. LT4+LT3 treatment is used frequently by thyroid specialists in Europe for persistent hypothyroid-like symptoms even if they generally attribute such symptoms to nonendocrine causes and despite the evidence of nonsuperiority of the combined over the LT4 therapy. Pressure by dissatisfied patients on their physicians for LT3-containing treatments is a likely explanation. The association of the therapeutic choices with the clinician demographic characteristics and geo-economic factors in Europe is a novel information and requires further investigation.
Introduction
Primary hypothyroidism is a common condition with a prevalence of 0.6–12.0% in women and 1.3–4.0% in men. 1 This wide range has been attributed to differences in age, sex, ethnic origin, iodine status, smoking behavior, 1,2 and variations in reference intervals for serum thyrotropin (TSH). The most common etiology in iodine-sufficient areas is autoimmune thyroid disease. 1
Hypothyroidism usually implies lifelong therapy and surveillance aiming at preventing the somatic and psychiatric morbidity and mortality associated with both under- and overtreatment. 3 –5 Thyroid hormone (TH) replacement therapy, using levothyroxine (LT4), is considered the standard of care and is recommended as the treatment of choice by professional organizations. 6,7
The management of patients with hypothyroidism can be challenging. Optimal absorption of LT4 tablets requires fasting and abstention from food and drink for at least 30 minutes after ingestion. 8 In addition, several medications and comorbidities may influence the bioavailability of LT4. 8 To overcome these difficulties, formulations containing predissolved LT4 have become available in some countries. 8 However, their high cost and limited evidence for increased bioavailability and improved quality of life (QoL) are limitations. 8
About 15% of hypothyroid individuals complain of persistent symptoms despite achieving biochemical euthyroidism on LT4. 9,10 Evidence from several randomized controlled trials (RCTs) indicates nonsuperiority of treatment with combination LT4+liothyronine (LT3) or desiccated thyroid extract (DTE) compared with LT4. 11 While the long-term safety of LT4 is well established, that of combination LT4+LT3 and DTE remains unknown. 11
THESIS (“Treatment of Hypothyroidism in Europe by Specialists: An International Survey”) is a survey of European thyroid specialists. Given the plurality of health care systems and socioeconomic diversity, yet overarching historical, ethnic, and administrative and regulatory similarities among European countries, THESIS was driven by a perceived need to explore national as well as broader geo-economic factors that may be relevant in the delivery of care to hypothyroid patients. This necessitated making the data generated by THESIS available to both national health care professionals (through the medium of national publications) 12 –31 and exploring pan-European trends for a wider readership.
The study was exploratory and the aims were (1) to document treatment choices and how they related to the presence of comorbidities and patients' well-being, (2) to explore correlations between respondent demographics and geo-economic factors with treatment choices, and (3) to define the perceived frequency and etiology of persistent symptoms, using aggregate data from all 28 participating countries.
Materials and Methods
Institutional review board waiver statement
The noninterventional nature of the survey and the fact that data were anonymized rendered the study exempt from institutional review board approval, as granted by the Danish Ethics Committee.
Design
THESIS was a questionnaire survey of thyroid specialists in 28 countries. The project aimed at European countries fulfilling three requirements: (1) a population exceeding 4 million, (2) an established national endocrine and/or thyroid professional organization, and (3) a national medical journal. Norway was the only invited nation that declined participation. Israel was included due to its cultural connections with Europe.
The study design and questionnaire development have been described in detail elsewhere. 32 Briefly, the questionnaire was developed in English. It was initially tested in a pilot study 12 and then revised to reach its final form. National leads used the original English version or translations performed by a bilingual clinician and validated by a senior bilingual clinician. The target population consisted of thyroid specialists who were members of their respective national endocrine and/or thyroid professional organizations and treated patients with hypothyroidism. Thus, their background besides endocrinology also extended to other specialties involved in the management of hypothyroid patients in Europe (such as nuclear medicine and internal medicine).
Project oversight was provided by a Steering Committee (L.H., E.V.N., E.P., P.P., R.A., and R.N.).
The questionnaire
The questionnaire contained 8 questions about respondents' demographic characteristics and 23 questions on the use of TH in different clinical settings. In addition, it enquired about respondents' perceptions of the cause of patients' persistent symptoms and how the prevalence of such complaints had changed over time (Supplementary Table S1). The responses were collected anonymously on secure online platforms that blocked repeat submissions from the same IP (Internet Protocol) address; those collected by e-mail (Belarus and Bulgaria) were anonymized before entering responses into the database.
Analysis
Data handling is shown in Supplementary Figure S1. Responses were considered valid for inclusion in the analysis when all the demographic questions were completed.
For evaluation of regional differences, the participating countries were grouped into geographic areas according to the United Nations Department of Economic and Social Affairs Statistics Division classification. 33 Namely, Western Europe includes Austria, Belgium, France, Germany, the Netherlands, and Switzerland; Northern Europe includes Denmark, Finland, Ireland, Sweden, and the United Kingdom; Southern Europe includes Croatia, Greece, Italy, Portugal, Serbia, and Spain; Eastern Europe includes Belarus, Bulgaria, Czechia, Hungary, Poland, Romania, Russia, Slovakia, and Ukraine; Western Asia includes Israel and Turkey.
Data about gross national income per capita (GNIPC) corresponding to the time period that the survey was conducted were retrieved from the World Bank 34 and grouped into middle income (Belarus, Bulgaria, Romania, Russia, Serbia, Turkey, and Ukraine) and high income (all the others; World Bank List of Economies). 35
Statistics
R packages were used for the statistical analyses. Frequencies/percentages (for categorical) and means and standard deviations (for quantitative variables) were used. The survey data were not weighted. The level of statistical significance was fixed at p < 0.05. Association between qualitative variables was tested using chi-square tests and Cramer's V tests. Linear, multinomial logistic, and ordinal regression were applied as appropriate using R packages statistics and ordinal. Both the p-values and effect size measures are reported and conclusions are guided largely by the latter, in view of the effect size being independent of sample size and p-value, thus allowing statistically significant but practically irrelevant results to be disregarded. 36 Interval variables (e.g., age) were grouped and converted to means using R package actuar. Cramer's V values were interpreted as per Rea and Parker 37 : <0.1 negligible, 0.1–0.2 weak, 0.2–0.4 moderate, 0.4–0.6 relatively strong, and over 0.6 strong association.
The prevalence was calculated using a survey package that estimates variances through the Taylor Series linearization method. 38 The variable selection process was carried out using the backward elimination technique with the help of the “rms” package. 39
Results
The response rate was 32.9% (5695/17,332). Respondent characteristics are shown in Supplementary Table S2. The assessment and management of nonresponse bias were addressed in a previous publication. 32 Briefly, mean age of respondents, proportion of females, survey language (local or English), GNIPC, number of days the survey was accessible, and number of reminders sent were not associated with response rates.
Initial choice of treatment for hypothyroidism
Nearly all respondents (98.3%, 5338/5431) recommended LT4 as the initial treatment for hypothyroid patients. Other options favored by a minority were LT4+LT3 1.2% (66/5431); LT3 monotherapy 0.3% (18/5431); and DTE 0.1% (7/5431) (LT4 vs. other TH regimens; p < 0.0001).
Several parameters (country of residence, region, income group, specialty, and caseload) correlated with the choice of LT4 as the first treatment modality, but these associations were weak or negligible.
The choice of initial treatment did not correlate with respondents' sex, age, years of medical practice, membership of international endocrine societies, GNIPC, or work setting.
Persistence of symptoms of hypothyroidism despite normal serum TSH during LT4 treatment
Most respondents (75.4%, 3283/4353) perceived that the prevalence of persistent hypothyroid-like symptoms despite the achievement of normal serum TSH with LT4 among patients was ≤10% (Table 1). Nearly half of study respondents (42.7%, 1860/4353) estimated this prevalence as ≤5%.
Physician-Reported or Perceived Persistent Symptoms Among Patients Treated with Levothyroxine Despite Achieving Normal Serum Thyrotropin
More than one answer was allowed.
CI, confidence interval; LT4, levothyroxine.
Multivariable analysis showed that respondents from Eastern Europe (odds ratio, OR, 0.44 [confidence interval, CI, 0.37–0.52]), Southern Europe (OR, 0.49 [CI, 0.41–0.59]), and Western Asia (OR, 0.74 [CI, 0.57–0.96]) reported a lower prevalence of persistent symptoms compared with Western and Northern Europe (Fig. 1E). A lower reported frequency of persistent symptoms was also associated with longer clinical experience (years in medical practice) (Fig. 1B) (OR, 0.40 [CI, 0.30–0.52]). In contrast, being an endocrinologist (Fig. 1A) (OR, 1.93 [CI, 1.51–2.48]), working at a university center (Fig. 1C) (OR, 1.26 [CI, 1.11–1.42]), and having a high-volume practice (i.e., >100 patients with hypothyroidism per year) (Fig. 1D) (OR, 1.26 [CI, 1.10–1.44]) were associated with higher estimates of prevalence of persistent symptoms.
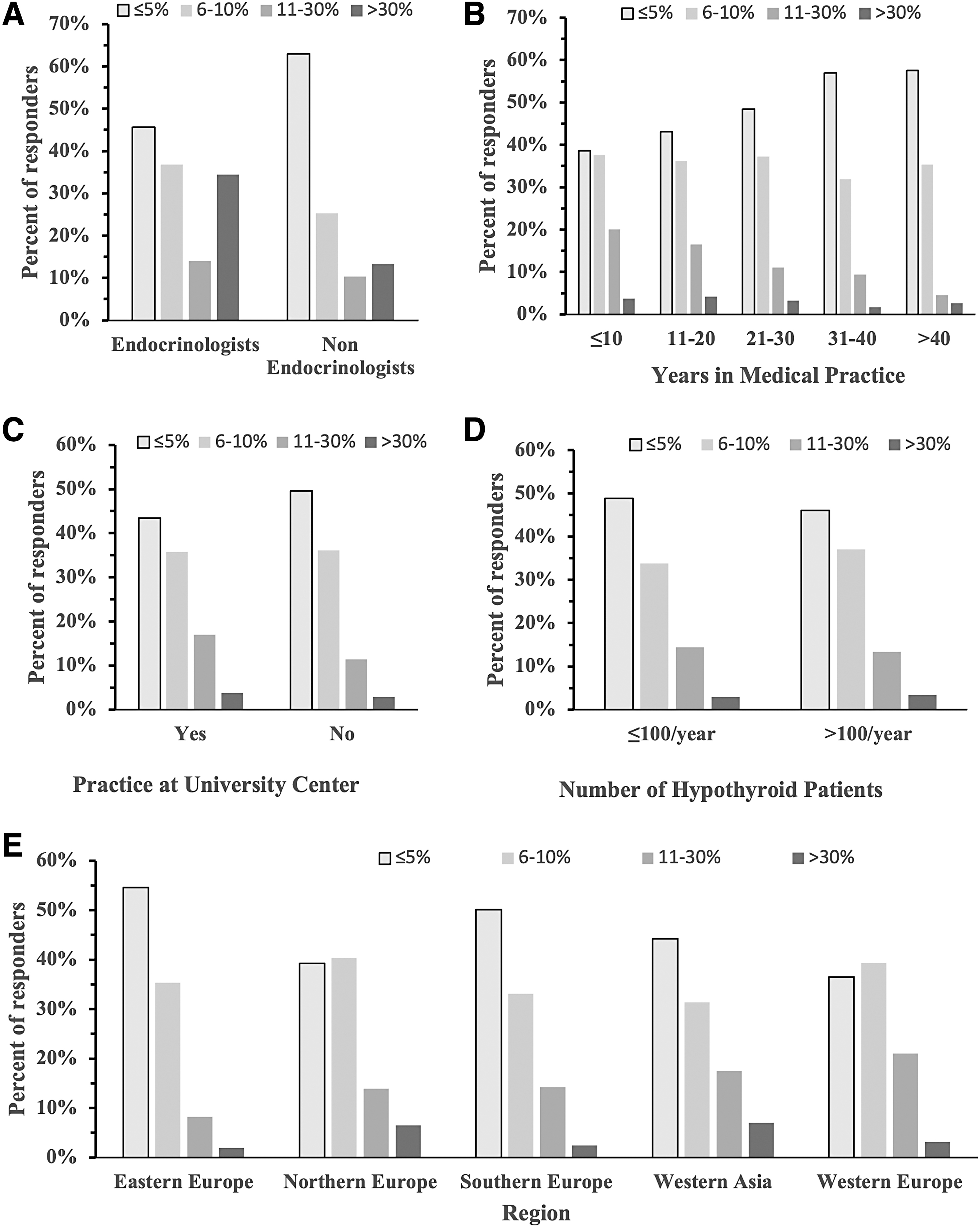
Respondent estimates of the prevalence of persistent symptoms despite normal serum TSH among hypothyroid patients treated with LT4. Multivariable analysis showed significant differences in estimated prevalence by specialty (
Reported trends for persistent symptoms across time
Most respondents perceived either a stable prevalence or an increasing trend of persistent symptoms despite achieving a normal TSH on LT4 among hypothyroid patients over the past 5 years (40.9%, 1777/4345 and 28.4%, 1234/4345, respectively) (Table 1).
Multivariable analysis showed that compared with Western Europeans, Northern Europeans and Western Asian respondents had a higher probability to report an increasing trend, while Eastern Europeans had a higher probability to report a decreasing trend (Table 2 and Supplementary Table S3). An increasing trend was also reported by respondents working in private practice and those with a high-volume practice.
Five-Year Trend in Physician-Reported Persistent Symptoms Despite Achieving a Normal Thyrotropin on Levothyroxine Among Hypothyroid Patients over the Past 5 Years
Statistically significant associations using multivariable analysis, setting “no change occurring in the last 5 years in the prevalence of persistent symptoms” as the reference.
Putative causes of persistent symptoms
Respondents were asked to select one or more options of putative causes for persistent symptoms of hypothyroid patients and to grade the strength of their opinion on a 1–5 Likert scale, where grades 4 and 5 denote agreement and strong agreement, respectively (Table 1). Psychosocial factors, comorbidities, patient unrealistic expectations, chronic fatigue syndrome, and the burden of chronic disease were the most frequent selected explanations (selected by 77.1%, 69.2%, 61.0%, 58.5%, and 53.5%, respectively).
Respondents were also asked to rank each of the putative causes of persistent symptoms in order of importance (from 1; most important, to 8; least important). Overall, psychosocial factors were ranked as most important, and the inability of LT4 to restore normal physiology as least important (3.4 and 5.3, respectively) (Fig. 2).
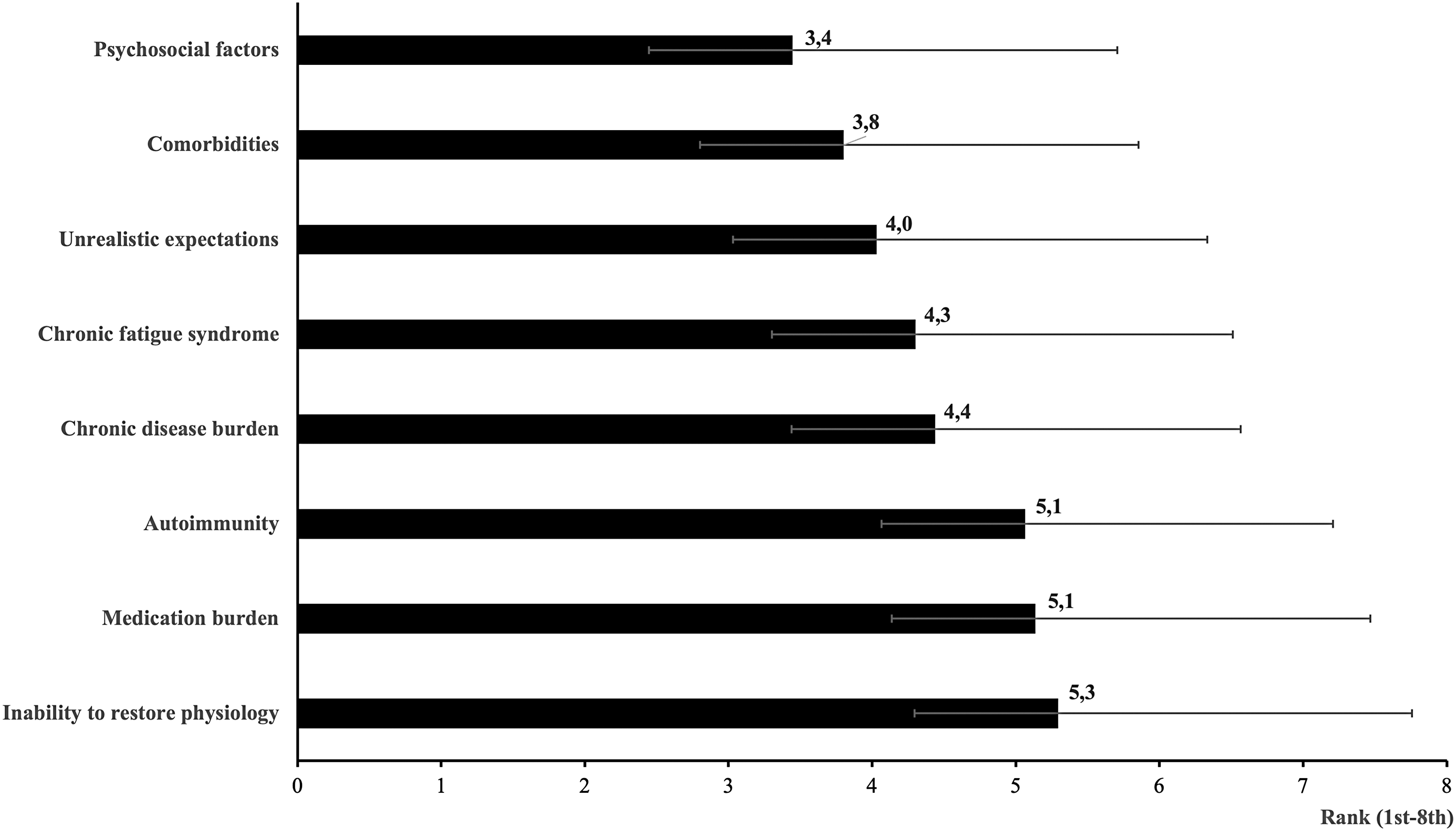
Respondent opinions about causes of persistent symptoms in biochemically euthyroid LT4-treated patients. Respondents were asked to select one or more options among putative causes for the persistence of hypothyroid-like symptoms in biochemically euthyroid patients. Respondents were presented with 8 putative causes of persistent symptoms [listed in the questionnaire in the following order: (1) medication burden, (2) unrealistic expectations, (3) inability (of levothyroxine) to restore normal physiology, (4) psychosocial factors, (5) presence of underlying inflammation due to autoimmunity, (6) comorbidities, (7) chronic fatigue syndrome, (8) the burden of chronic disease]. They were asked to rank them according to their opinion as most likely (score 1) and least likely (score 8) explanation for persistent symptoms. The horizontal axis shows the mean and standard deviation scores in respondents' opinions for the putative causes of persistent symptoms that are aligned along the vertical axis according to ranking from 1 to 8, at the top and bottom, respectively.
Multivariable analysis revealed several significant associations (Table 3).
Multivariable Analysis for Causes of Persisting Hypothyroid Symptoms in Patients with Normal Thyrotropin on Levothyroxine. Options Are Expressed as Odds Ratios [Confidence Interval]
Compared with nonendocrinologists.
Compared with <10-year experience.
Compared with not working in that setting.
Compared with Western Europe.
Compared with females.
Compared with low-volume practice.
Evaluated as a continuous variable per 10,000 US$.
GNIPC, gross national income per capita.
Choices of combination treatment with LT4+LT3 in specific situations as second-line treatment after LT4 monotherapy
A sizeable minority (42.4%, 2184/5146) of respondents stated that they would never consider LT4+LT3 combination treatment. This combination was favored by 39.7% (2041/5146) for patients with persistent symptoms, by 15.7% (807/5146) for a short period in patients recovering from protracted hypothyroidism, and by 1.8% (93/5146) for unexplained weight gain.
Multivariable analysis revealed several associations. Choice of LT4+LT3 combination treatment was positively associated with (1) being an endocrinologist (OR, 1.44 [CI, 1.17–1.76]); (2) having a high-volume practice (OR, 1.39 [CI, 1.23–1.58]); and (3) working in countries with high GNIPC (OR, 1.021 [CI, 1.014–1.027]). Conversely, LT4+LT3 combination treatment was negatively associated with (1) respondent being male (OR, 0.86 [CI, 0.76–0.97]) and (2) working in Western Europe (OR, 0.27 [CI, 0.20–0.36]). In addition, choice of triiodothyronine (T3)-containing medication (LT4+LT3 combination treatment or DTE) was significantly associated with respondents' view that LT4 alone cannot restore normal physiology and inversely associated with the view that patients' unrealistic expectations are the cause of persisting symptoms (Supplementary Fig. S2 and Fig. 3, respectively).
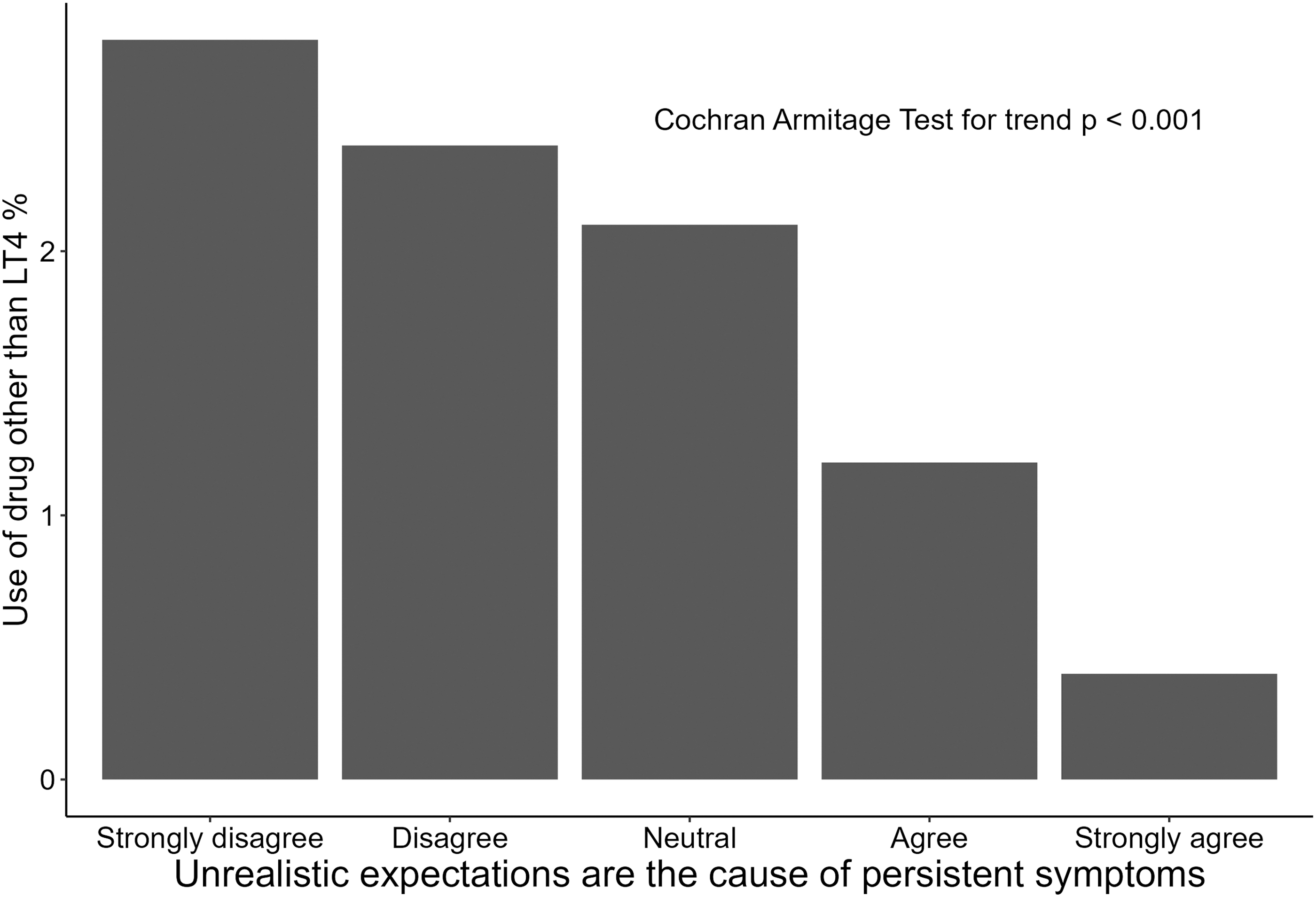
Association between respondents' view of patients' unrealistic expectations and prescription of T3-containing medication. The trend along the 1–5 Likert scale (on the X-axis, from “strongly disagree” to “strongly agree”) for unrealistic expectations as the proposed cause of persistent symptoms was plotted against the use of drug other than LT4 (on the Y-axis) and analyzed by Cochran Armitage test for trend. T3, triiodothyronine.
Local availability and reimbursement of LT3-containing products did not influence respondents' choices (data not shown).
Choices of different LT4 formulations in different clinical scenarios
Most respondents preferred LT4 tablets to other LT4 formulations. Only a minority expected advantages when switching from tablets to predissolved LT4 formulations in specific conditions, such as taking potentially interfering drugs (34.3%), presence of gastrointestinal comorbidities (16.7%), or unexplained poor biochemical control of hypothyroidism (20.8%). In contrast, half of the respondents (49.8%) favored switching to predissolved LT4 formulations in patients with poor biochemical control and inability to take LT4 fasted. Preference for predissolved LT4 formulations was higher for all clinical scenarios in respondents from countries where these formulations were available at the time of the survey. In particular, in patients with poor biochemical control and inability to take LT4 fasted, the percentage of respondents who opted for predissolved LT4 formulations was 37.3% and 62.2% according to the lack or availability of such formulations in the respondent's country, respectively (Table 4).
Levothyroxine Formulations Chosen by THESIS Respondents in Specific Clinical Scenarios: N (% [Confidence Interval])
Available on the national market at the time of the survey in Austria, Denmark, Finland, France, Germany, Greece, Hungary, Italy, The Netherlands, Slovakia, Switzerland, and the United Kingdom.
Available on the national market at the time of the survey in Austria, Denmark, Finland, France, Germany, Greece, Italy, The Netherlands, Romania. Slovakia, Sweden, Switzerland, and the United Kingdom.
THESIS, Treatment of Hypothyroidism in Europe by Specialists: An International Survey.
Multivariable analysis revealed several statistically significant associations (Table 5).
Multivariable Analysis for Prescription of Predissolved Levothyroxine Formulations in Comparison with Tablets
Data are expressed as odds ratios [CI].
Compared with nonendocrinologists.
Compared with <10-year experience.
Compared with not working in that setting.
Compared with low-volume practice.
Discussion
Several clinically important trends in the diagnosis and treatment of hypothyroidism have been reported over the past few years. The threshold of TSH at which TH is prescribed has fallen in some European countries and the United States. 40 –43 Consequently, prescriptions for TH have increased 42,44 and in some countries this has been paralleled by an increase of the use of LT4+LT3 combination treatments. 45,46 This trend has occurred despite evidence from several RCTs and meta-analyses showing the nonsuperiority of combination LT4+LT3 treatment compared with LT4 alone, although these studies did not specifically target symptomatic patients. 11 Physician surveys conducted in the United States have shown a shift from rare usage of combination LT4+LT3 treatment in 2013 (0.8%) 47 to use by 18–40% of physicians in 2017. 48 Patient demands were highlighted as a possible reason for this change in practice. 49
A survey conducted by the American Thyroid Association (ATA) in 2017 found that among several physician characteristics, practitioners in North America were more likely to prescribe LT3-containing treatments compared with ATA members practicing elsewhere. 9 Information about choices of treatment for hypothyroidism and the impact of physician characteristics in Europe are lacking, a knowledge gap that was addressed by THESIS.
Our study explored associations between therapeutic choices with clinician demographic characteristics and geo-economic factors, by combining data from national surveys.
In our study, the overall valid response rate of 32.9% was comparable with the response rates achieved by European physician surveys related to topics focusing on benign thyroid disease. 50,51 Physician characteristics (sex distribution) and response/nonresponse bias were small. 32 Moreover, the response rates recorded in THESIS are likely to be underestimated, as the membership of national endocrine and thyroid professional organizations includes basic researchers and individuals not clinically active in thyroid disease management, and who are not the target of the present survey. 32 Therefore, the respondents are likely to be representative of the current clinical practice in Europe and to include national opinion leaders who influence primary care in their respective countries.
Initial choice of treatment for hypothyroidism
LT4 monotherapy is currently recommended as first-line treatment by international guidelines. 6,11 Indeed, the vast majority of respondents considered LT4 as the first line of treatment, while a very small minority (1.7%) chose T3-containing treatments. In contrast, studies from North America show a much greater tendency for physician preference for T3-containing treatments as the initial choice for hypothyroidism. 48,49 This markedly different approach may be related to socioeconomic and cultural factors, as well as easier access to T3 or T3-containing preparations, resulting in a greater demand from patients for such treatments and possibly by a lower physicians' adherence to professional guideline recommendations. 49 Notably, our study shows consensus for LT4 as the initial choice of treatment across thyroid specialist demographics and geo-economic factors in Europe.
Persistent symptoms
A sizeable minority of hypothyroid patients who achieve biochemical euthyroidism on LT4 therapy complain of the persistence of symptoms consistent with hypothyroidism. 9,10 Seventy-five percent of respondents estimated that the persistence of hypothyroid-like symptoms occurs in <10% of their patients. This prevalence is lower than in the surveys performed among hypothyroid patients that reported dissatisfaction in up to 15% of the subjects treated with LT4. 9,52 This perception was less prevalent among respondents from Eastern Europe, Southern Europe, and Western Asia, nonendocrinologists, and respondents not working in university centers. 53
Several explanations for persistent symptoms have been proposed. 10 The potential for low T3 levels in the brain or an impact of LT4/LT3 ratio in hypothyroid patients treated with LT4 is the most commonly offered, but a not yet confirmed explanation for the persistence of symptoms consistent with hypothyroidism. 54 In our study, psychosocial factors were the most frequent explanation provided; this correlated with respondents being endocrinologists. The “inability of LT4 to restore normal physiology” hypothesis was preferred by a minority of respondents, mostly nonendocrinologists from Southern Europe or Western Asia. That hypothesis, however, has not been confirmed by interventional studies using LT3 treatment. 11 Importantly, chronic diseases that require daily medication may affect patients' QoL negatively. 55 Thus, some hypothyroid patients who complain of impaired well-being may do so despite restoration of euthyroidism.
Therefore, the majority view, attributing the persistence of hypothyroid-like symptoms to psychosocial factors, appears to be in keeping with the currently available evidence. The overall prevalence of persistent symptoms among hypothyroid patients was reported to be stable over time; however, respondents from countries with high GNIPC reported an increasing trend, while respondents from low GNIPC regions reported a decreasing trend.
Combination treatment with LT4+LT3 and use of DTE
Thyroid specialists frequently face patients with persistent symptoms 10 who often ascribe their poor QoL to lower than optimal free triiodothyronine (fT3) levels while on LT4 monotherapy 11 and often request combination treatment containing LT3. This is an area that attracts controversy. 11,56
The THESIS respondents' approach to LT3-containing treatments is in accordance with present evidence. Nearly all respondents stated that they would not use LT4+LT3 combination as initial treatment, and only 40% would consider this therapy for persistent symptoms. Why this attitude was more frequent among respondents who work in private practice, who are female, and who live in countries with higher GNIPC is unclear. It is of interest that somatization has recently been shown to be very prevalent among hypothyroid patients; they tended to attribute all symptoms to hypothyroidism, which in turn may drive them to seek LT4+LT3 combination through the private sector, particularly in rich countries. 57
At variance with reports from the United States, 58 DTE was nearly never recommended by THESIS respondents. This may reflect the fact that DTE is not as accessible in Europe as in the United States, while LT4 brands and formulations are, as well as concerns about overtreatment, unphysiological fluctuations in T3 levels, and variable potency 59 ; these perceptions are consistent with available evidence and recommendations by professional guidelines. 60
Use of the different LT4 formulations
While LT4 tablets are the initial formulation of choice for hypothyroidism in Europe, the use of predissolved formulations was considered favorable in specific clinical conditions. The preference for predissolved LT4 formulation by THESIS respondents in patients with malabsorption was consistent with the limited evidence for better absorption than LT4 tablets. 8 A sizeable percentage of respondents also considered predissolved LT4 formulation for patients who have difficulty adhering to the requirement for taking LT4 tablets fasted and waiting for a minimum of 30 minutes before breakfast. 61,62 Notably, the switch from LT4 tablets to different formulations in case of unexplained poor control of hypothyroidism was reported more frequently by the young physicians and by those who work in private practice.
Strengths of the study
The large number of respondents, the participation of nearly all the eligible European countries with endorsement of their corresponding endocrine/thyroid professional organizations, and the acceptable response rate, compared with other published surveys, 11 offer unique insight into the current medical management of hypothyroidism in Europe. Respondents were representative of the spectrum of thyroid specialists who manage hypothyroid patients in Europe.
Limitations
The focus of the present study was on the use of TH, and therefore, no distinction was made between subclinical and overt hypothyroidism. Therapeutic approaches to central hypothyroidism, as well as the treatment of pregnant women or women who are planning pregnancy, were not addressed in the survey. We consider the virtual patient scenario and the ongoing corona virus disease-19 (COVID-19) pandemic as limitations. The exclusion of primary care physicians may limit generalizability, although practices in primary care usually reflect the guidance and advice of national experts and specialists.
Conclusions
This study has identified associations between European thyroid specialists' willingness to use an LT4+LT3 treatment and clinician demographic and national geo-economic factors. We highlight an apparent contradiction: the majority opinion (nearly 80%) of European thyroid specialists is that persistence of symptoms is largely due to psychosocial causes, while nearly half (40%) opt for LT4+LT3 therapy for such patients, when the evidence does not support this strategy. The implication of our findings in the clinical management of patients with hypothyroidism who experience persistent symptoms is that there is a need to explore nonpharmacological interventions such as cognitive behavior therapy. The finding that most of these hypothyroid-like symptoms are considered nonthyroidal by endocrinologists and yet so many endocrinologists resort to thyroid remedies as a solution is paradoxical and intriguing and merits further in-depth studies.
Ethics Guidelines
Ethical approval was not required. Authors confirm that all of the research meets ethics guidelines, including adherence to the legal requirements of the country where the study was performed.
Informed Consent
A signed informed consent was not required from participants in this anonymous and voluntary questionnaire survey.
Footnotes
Acknowledgments
We gratefully thank the leadership of the 28 countries' Endocrine Societies, Chagit Adler Cohen (Israel), Jacob Stampe Frølich (Denmark), Miguel Melo (Portugal), and Elena Yurenya (Belarus), as well as all the members generously answering the questionnaire. Some results were previously presented at the European Thyroid Association Meetings in Dublin, Ireland, in 2022 and in Milan, Italy, in 2023, at the European Congress of Endocrinology online in 2021, as well as at different national meetings in the last 3 years.
Authors' Contributions
Conceptualization, methodology, project administration, and supervision: L.H., E.P., E.V.N., and P.P. (equal). Data curation, visualization, and writing of the original draft: R.A. Formal analysis and visualization: M.Z. Writing and review and editing: R.A., M.Z., L.H., E.P., E.V.N., R.N., and P.P. (equal). Data collection, validation, and review and editing: E.A., M.A., G.A., T.B., B.N.B., E.B., Mik.B., A.M.B., Mih.B., C.B., M.-C.B., J.Ć., J.J.D., H.D., V.F., B.C.T.F., E.F., D.F.-S., J.C.G., T.H., J.J., P.A.K.,
Author Disclosure Statement
All support for the present article (e.g., funding, provision of study materials, medical writing, article processing charges): during the period when data were collected from the Danish endocrinologists, K.R.R. received her salary from a grant from the Danish Medicines Agency.
Grants or contracts from any entity: D.F.-S. from German Research Foundation (CRC/Transregio 296 LOCOTACT);
Consulting fees: E.V.N., L.H., and P.P. from IBSA; E.P. from IBSA and Terumo; T.B. from Merck KGaA; J.C.G. from IBSA and Abbott; L.H. from Horizon;
Payment or honoraria for lectures, presentations, speakers' bureau, article writing, or educational events: P.P. from IBSA; A.M.B. from Berlin-Chemie Menarini and Merck; T.B. from Berlin-Chemie Menarini, Ipsen, Merck KGaA, and Roche Diagnostics; J.C.G. from IBSA and Abbott. L.H. from IBSA, Berlin-Chemie, and Merck;
Support for attending meetings and/or travel: R.A. from IBSA; P.P. from IBSA; E.P. from IBSA; T.B. from Berlin-Chemie Menarini; H.D. from German Society for Endocrinology; J.C.G. from IBSA and Abbott; L.H. from IBSA, Berlin-Chemie, and Merck;
Participation on a Data Safety Monitoring Board or Advisory Board: E.P., E.V.N., L.H., and P.P. were members of the IBSA scientific board; D.F.-S. for IBSA;
Leadership or fiduciary role in other board, society, committee, or advocacy groups, paid or unpaid: A.M.B. from the Bulgarian Society for Endocrinology (no payment); D.F.-S. for AWMF-German Thyroid cancer guideline (including diagnosis and therapy of thyroid nodules);
Other financial or nonfinancial interests: C.M. received publication fees from IBSA for another publication.
All other authors have no conflict of interest.
Funding Information
This research did not receive any financial support.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Figure S1
Supplementary Figure S2