
Abstract
Background:
The benefit of levothyroxine treatment of subclinical hypothyroidism (SCH) is subject to debate. This study compared treatment satisfaction between older adults with SCH using levothyroxine or placebo.
Methods:
We analyzed pooled individual participant data from two randomized, double-blind, placebo-controlled trials investigating the effects of levothyroxine treatment in older adults with SCH. Community-dwelling participants aged ≥65 years, with SCH (persistent thyrotropin levels 4.60–19.99 mIU/L for >3 months and normal free T4 level), were included. Intervention dose titration until thyrotropin levels normalized, with a mock dose adjustment of placebo. Treatment satisfaction was determined during the final study visit using the Treatment Satisfaction Questionnaire for Medication (TSQM), encompassing perceived effectiveness, side effects, convenience, and global satisfaction, along with the participants’ desire to continue study medication after the trial.
Results:
We included 536 participants. At baseline, the median (interquartile range [IQR]) age was 74.9 (69.7–81.4) years, and 292 (55%) were women. The median (IQR) thyrotropin levels were 5.80 (5.10–7.00) mIU/L at baseline in both groups; at final visit, 4.97 (3.90–6.35) mIU/L in the placebo and 3.24 (2.49–4.41) mIU/L in the levothyroxine group. After treatment, the groups did not differ significantly in global satisfaction (mean difference [CI] −1.1 [−4.5 to 2.1], p = 0.48), nor in any other domain of treatment satisfaction. These results held true regardless of baseline thyrotropin levels or symptom burden. No major differences were found in the numbers of participants who wished to continue medication after the trial (levothyroxine 35% vs. placebo 27%), did not wish to continue (levothyroxine 27% vs. placebo 30%), or did not know (levothyroxine 37% vs. placebo 42%) (p = 0.14). In a subpopulation with high symptom burden from hypothyroid symptoms at baseline, those using levothyroxine more often desired to continue the medication after the trial than those using placebo (mean difference [CI]: −21.1% [−35.6% to −6.5%]).
Conclusion:
These pooled data from two RCTs showed no major differences in treatment satisfaction between older adults receiving levothyroxine or placebo. This finding has important implications for decision-making regarding initiating levothyroxine treatment for SCH. Our findings generally support refraining from routinely prescribing levothyroxine in older adults with SCH.
Introduction
Subclinical hypothyroidism (SCH) is a common condition defined by an elevated level of thyrotropin and a free T4 level within the normal reference range. Its prevalence is more frequent in women and increases with advancing age, varying from 5–20% in adults older than 60 years. 1 SCH is often asymptomatic or accompanied by nonspecific symptoms 2 and around 90% of all individuals with SCH have mildly elevated thyrotropin levels < 10 mIU/L. 3,4 Progression from subclinical to overt hypothyroidism (defined by both elevated thyrotropin and reduced free T4 levels) has been reported to occur in 1.9–12.7% of adults older than 55 years with an elevated thyrotropin level < 10 mIU/L (mean follow-up of 12–38 months). 5 –7 Whereas the need for thyroid hormone replacement therapy with levothyroxine is evident for overt hypothyroidism, controversy exists for SCH, in particular for older adults with a thyrotropin level < 10 mIU/L. 8 Nevertheless, levothyroxine is most frequently prescribed and initiated in older adults (50–70 years), 9 while the observed rise in prescriptions in recent decades 10,11 is likely attributed to an increase in treatment of SCH. 12
When considering levothyroxine treatment in individuals with SCH, it has been recommended to base the decision on both the physician’s judgment of the present evidence and the patient’s preference. 13 Randomized controlled trials (RCTs) have shown that levothyroxine treatment does not improve thyroid-related symptoms, quality of life, symptoms of depression, or cognitive function in older adults with SCH. 14 –17 However, patient preferences regarding treatment of SCH are at present unknown. In general, studies have shown that patients’ health-related and treatment-related decisions can be affected by their perceptions of care, a patient-reported outcome described as patient satisfaction. 18,19 Understanding treatment satisfaction and patients’ preferences regarding (dis)continuation of levothyroxine treatment in an RCT may provide valuable insights into treatment-related decision-making and may reveal patient perspectives that have not been captured by frequently used formal endpoint measurements such as thyroid-related quality of life.
Therefore, this study aimed to compare patient satisfaction for treatment between older adults with SCH using either levothyroxine or placebo. Patient satisfaction for treatment was operationalized in this study as (1) effectiveness, side effects, convenience, and global satisfaction of the trial medication and (2) the participants’ desire for continuation of medication after the trial.
Materials and Methods
Design
This study constitutes a preplanned secondary study pooling individual participant data from two randomized, double-blind and placebo-controlled parallel-group trials. The primary focus of these trials was to investigate the effects of levothyroxine treatment in community-dwelling older adults aged ≥ 65 years and diagnosed with SCH. The trials, TRUST (Thyroid hormone Replacement for Untreated older adults with Subclinical hypothyroidism—a randomized placebo-controlled Trial) 15,20 and IEMO 80+ (the Institute for Evidence-Based Medicine in Old Age 80-plus thyroid trial), 16,21 were designed and executed as parallel studies, using identical study protocols. The TRUST study was registered at ClinicalTrials.gov (NCT01660126) and the IEMO80+ study at the Netherlands Trial Register (NL3641; formerly NTR3851). Both clinical trials were approved by the local institutional review boards (IRB) before data collection (see Table S1 in the Supplementary Appendix for IRB study numbers). Written informed consent was obtained from all participants. The trial was performed in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice guidelines.
Baseline Characteristics of the Participants
Includes myocardial infarction, angina, stroke, transient ischemic attack, heart failure, peripheral vascular disease, revascularization, atrial fibrillation, and/or hypertension.
Range, 0–30; 29–30 indicates no cognitive impairment; 25–28, mild cognitive impairment; 19–24, moderate cognitive impairment; <19, cognitive impairment.
The number of digits coded within 90 seconds; higher scores indicated better executive cognitive function.
Higher scores indicate better muscle strength; mean for women aged 75 years, 21.4 kg; mean for men aged 75 years, 35.6 kg.
Range, 0–20; 20 indicates fully independent in activities of daily living and mobility; 15–19, moderately to fully independent; 10–14, needing help but capable of own activities; 5–9, severely dependent, 0–4, totally dependent.
Range, 0–14, higher scores indicate better performance in instrumental activities of daily living.
IQR, interquartile range; nr, number; SD, standard deviation.
Study population
In summary, community-dwelling older adults with persisting SCH were recruited from sites in Ireland, the Netherlands, Switzerland, and the United Kingdom between April 2013 and May 2015. Persisting SCH was defined as having a thyrotropin level 4.60–19.99 mIU/L and a free T4 level within the reference range, measured on at least two occasions between 3 months and 3 years apart. Patient satisfaction questionnaires for treatment were implemented at all sites, except the United Kingdom (n = 150). Therefore, data from randomized participants from Ireland, the Netherlands, and Switzerland were used for this analysis.
Data collection
Participants were assigned randomly in a 1:1 ratio to be administered either levothyroxine or placebo. The levothyroxine groups commenced with a daily dosage of 50 µg (or 25 µg for individuals with a body weight < 50 kg or a history of coronary heart disease), while the placebo group started with an equivalent placebo. The levothyroxine dose was incremented by 25 µg at intervals of 6–8 weeks, aiming to achieve a thyrotropin level within the reference range (0.4–4.6 mIU/L). In the placebo group, an identical schedule was used for mock titration. The final dose was defined as the dose received at the final visit or the last dose received before withdrawal. Participants were followed up for a minimum of 12 months and a maximum of 36 months between April 2013 and May 2018, during which the final visit was scheduled.
Study outcomes
Patient satisfaction for treatment was determined first by assessment of the Treatment Satisfaction Questionnaire for Medication (TSQM v.II). The TSQM is an 11-item, general, and nonspecific medication satisfaction questionnaire that has been developed and validated for chronic diseases and outpatient settings. The TSQM comprises the following domains: effectiveness, side effects, convenience, and global satisfaction. 22 All items are scored on a 5- or 7-point Likert scale except one item for the presence of side effects, which is binary (i.e., yes or no). The scores for each domain are derived by summing the TSQM items. Subsequently, the composite score is transformed into a value ranging from 0 to 100. Higher scores signify greater satisfaction, greater perceived effectiveness, less burden associated with side effects, or enhanced convenience. Participants experiencing no side effects automatically attain the maximum score for the respective domain (i.e., 100). Side effects were further assessed using an additional open question. Second, patient satisfaction was determined by assessing the participants’ desire to continue the medication after the trial (closed question: yes/no). The TSQM and other questions were translated to the local language of the study sites and were filled in at the final visit, before disclosure of the actual treatment allocation. All research personnel remained blinded to the participants’ answers until after the trial.
To characterize the study population, the following parameters were analyzed at baseline: independent living, medical history, concomitant medication, Mini-Mental State Examination scores, letter-digit coding test, handgrip strength, body mass index, Barthel index, instrumental activities of daily living score, thyroid function, and thyroid-related quality of life (as assessed by using the Hypothyroid Symptoms score [4 items] and Tiredness score [7 items] from the ThyPRO-39 questionnaire, each on a scale from 0–100, with higher scores indicating more symptoms/tiredness). 23
Data analysis
Participants were included in the statistical analysis if they had data available for at least the TSQM v.II domain “global satisfaction” (representing overall satisfaction with the trial medication), or the question assessing the participant’s desire to continue the medication after the trial. Baseline characteristics are presented as mean (standard deviation [SD]) or median (interquartile range [IQR]) depending on data distribution.
For all participants, the following parameters were determined per treatment arm: mean or median TSQM compound scores for each domain, the number of participants experiencing side effects, the number of participants expressing the desire to continue treatment medication post-trial, including confidence intervals (CIs). Furthermore, reported side effects were described and counted. Independent t-tests, Mann–Whitney U tests, or chi-square tests were performed to analyze between-group differences using IBM SPSS Statistics for Windows, Version 29.0 (Armonk, NY: IBM Corp.); CIs of differences were included. Furthermore, additional analyses were performed to determine whether the thyrotropin level at baseline, symptom burden at baseline, or sex influenced the outcomes of treatment satisfaction. Subgroups of baseline thyrotropin levels included <7.00 mIU/L and ≥7.00 mIU/L to match cutoff values in applicable guidelines. Participants with high or low symptom burden were identified using the primary outcome parameters from the TRUST, Hypothyroid Symptoms, and Tiredness scores from the ThyPRO-39. 23 High symptom burden was defined as a baseline score for Hypothyroid Symptoms >30 or Tiredness score >40. 24 Independent t-tests, Mann–Whitney U tests, or chi-square tests were performed to analyze differences in patient satisfaction per treatment arm by comparing the following: groups with high or low symptom burden, baseline thyrotropin subgroups, and women versus men. p-Values < 0.05 were considered statistically significant.
Results
In the pooled trials of TRUST and IEMO 80+, a total of 692 participants from Ireland, the Netherlands, and Switzerland were included (346 randomized to levothyroxine and 346 to placebo). Data for treatment satisfaction were available for 276 (80%) participants in the levothyroxine group and for 260 (75%) participants in the placebo group (Fig. 1).
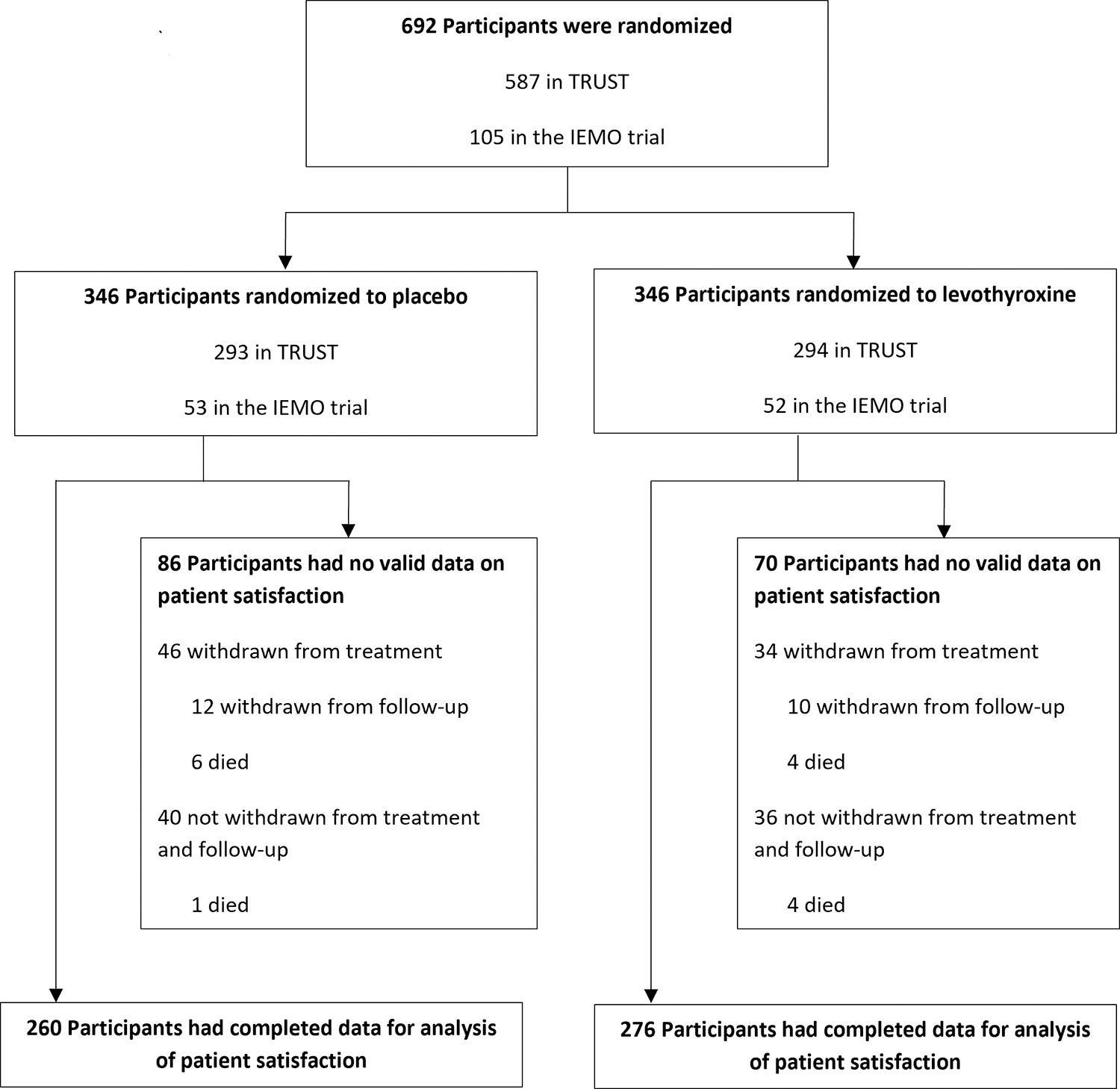
Randomization and participant flow. This flow diagram shows randomization and participant flow in a secondary study investigating patient satisfaction with levothyroxine or placebo treatment in adults aged 60 years and older with subclinical hypothyroidism using pooled data of TRUST and the IEMO 80+ thyroid trial, including the study sites in Ireland, the Netherlands, and Switzerland. IEMO, Institute for Evidence-Based Medicine in Old Age; TRUST, Thyroid hormone Replacement for Untreated older adults with Subclinical hypothyroidism-a randomized placebo-controlled Trial.
At baseline, the median (IQR) age was 74.9 years (69.7–81.4), ∼55% (n/n = 292/536) of participants were women and the median (IQR) thyrotropin level was 5.8 (5.1–7.0) mIU/L in both the placebo and levothyroxine groups (Table 1). At randomization, the median (IQR) hypothyroid symptom scores were similar [12.5 (0.0–25.0) in both the placebo and levothyroxine groups], as were the median (IQR) Tiredness scores [17.8 (10.7–28.5) in the placebo and 17.8 (8.0–35.7) in the levothyroxine group]. At the final visit, the median (IQR) thyrotropin level was 3.24 mIU/L (2.49–4.41) in the levothyroxine group at a mean (SD) final dose of 53.7 µg (17.1) per day compared with 4.97 mIU/L (3.90–6.35) in the placebo group at a mean final placebo dose of 52.3 µg (15.2) per day (mean difference in change between groups [CI]: 1.84 mIU/L [−2.25 to 1.42], p < 0.001]). The median (IQR) treatment duration was 375 (360–715) days for placebo and 422 (357–731) days for levothyroxine. Baseline characteristics were similar between participants who were included in the analysis for treatment satisfaction and those who were excluded (data not shown).
At the final visit, participants from the levothyroxine and placebo groups did not differ with respect to treatment satisfaction as measured by the TSQM domains: effectiveness, side effects, convenience, and global satisfaction (Table 2). In the levothyroxine group, 11.0% [CI: 7.2–14.7] of participants reported experiencing side effects versus 8.5% [CI: 5.0–11.8] in the placebo group (mean difference [CI]: −2.5 [−7.5 to 2.5], p = 0.32). A variety of side effects concerning many organ systems were reported, including headache, fatigue, mood change, cognitive problems, perspiration, palpitations, gastrointestinal complaints, skin problems, dry eyes, and muscle ache. In both treatment groups, similar rates of complaints were observed except for gastrointestinal problems, which were reported more often in the levothyroxine group (n = 7 vs. n = 1 in the placebo group).
Outcome Parameters of Patient Satisfaction Regarding Treatment with Levothyroxine or Placebo in Older Adults
Range, 0–100; score derived from a 7-point Likert scale ranging from extremely dissatisfied to extremely satisfied; higher scores indicate more satisfaction regarding the effectiveness of levothyroxine.
Range, 0–100; score derived from a 5-point Likert scale ranging from extremely bothersome to not at all bothersome; higher values indicate less bothersome side effects from levothyroxine.
Range, 0–100; score derived from a 5-point Likert scale ranging from extremely difficult to extremely easy; higher scores indicate more convenience regarding levothyroxine usage.
Range, 0–100; score derived from a 5-point Likert scale ranging from not at all confident to extremely confident; higher scores indicate more global satisfaction with levothyroxine usage.
CI, confidence interval; IQR, interquartile range; TSQM, Treatment Satisfaction Questionnaire for Medication.
When participants were asked at the final visit whether they would like to continue the treatment after the trial, no major differences were found between both treatment groups (Fig. 2): 35.4% [CI: 29.7–41.1] in the levothyroxine group wished to continue treatment versus 27.4% [CI: 21.9–32.8] in the placebo group (mean difference [CI]: −8.0 [−15.8 to −0.1]), 30.1% [CI: 24.5–35.7] in the placebo group did not wish to continue treatment versus 27.3% [CI: 22.0–32.6] in the levothyroxine group (mean difference [CI]: 2.8 [−4.8 to 10.5]), and 37.3% [CI: 31.5–43.0] in the levothyroxine versus 42.5% [CI: 36.4–48.4] in the placebo group did not know (mean difference [CI]: 5.2 [−3.1 to 13.5]; p = 0.14). When comparing the TSQM scores from participants who wished to continue the study medication after the trial, we found no relevant differences between both treatment groups (mean [SD] scores for effectiveness: 63.6 [19.3] in the levothyroxine and 62.1 [17.7] in the placebo group, mean difference [CI]: −1.5 [−7.9 to 4.8], p = 0.63; for convenience: 77.0 [14.3] in the levothyroxine and 73.8 [14.1] in the placebo group, mean difference [CI]: −3.2 [−7.6 to 1.2], p = 0.15; and for global satisfaction 68.6 [16.7] in the levothyroxine and 67.7 [14.1] in the placebo group, mean difference [CI]: −0.9 [−5.9 to 4.1], p = 0.72; median scores [IQR] for side effects in both groups 100 [100–100], p = 0.04). Likewise, no differences between both treatment groups were found for the TSQM scores when comparing participants who did not wish to continue the study medication after the trial, or who did not know (all p values > 0.10).
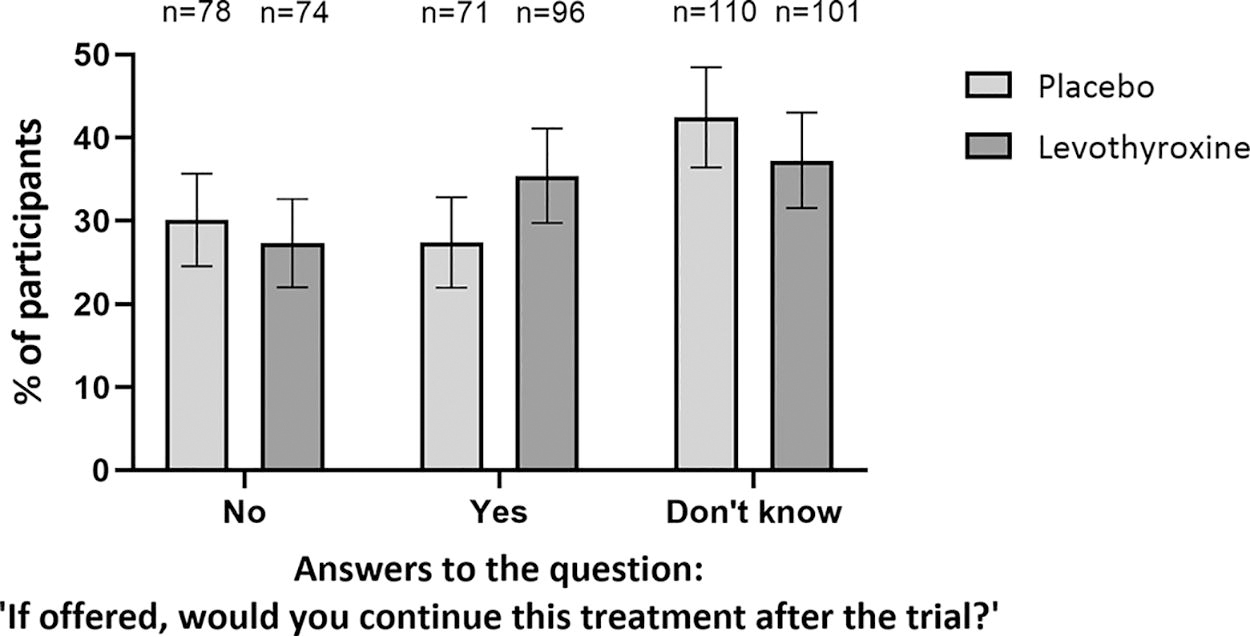
The wish of participants receiving placebo or levothyroxine to continue the medication after the trial. Shown are the percentage of participants from the placebo and the levothyroxine group, who responded to the question, “If offered, would you continue this treatment after the trial?” with “No,” “Yes,” or “Don’t know.” Error bars depict confidence intervals. Between-group differences were analyzed using chi-square (p = 0.14).
Subgroup analysis for low versus high thyrotropin levels at baseline with a cutoff point of 7.00 mIU/L showed no significant differences in treatment satisfaction between the levothyroxine and the placebo groups (Table 3). Subgroup analyses for participants with high or low symptom burden at baseline did not show significant differences between the levothyroxine and placebo groups for any of the treatment satisfaction domains of the TSQM (Table 4). Within participants with a high symptom burden, those in the levothyroxine group more often wished to continue the medication after the trial than those in the placebo group (34.3% vs. 13.2% for a high burden of hypothyroid symptoms (mean difference [CI]: −21.1% [−35.6% to −6.5%]); 37.3 vs. 15.6% for a high burden of tiredness (mean difference [CI]: −21.6% [−39.9% to −3.3%]) (Table 4). Subgroup analysis of women versus men did not reveal any differences between both treatment groups with respect to treatment satisfaction (Table S2 in the Supplementary Appendix).
Patient Satisfaction Regarding Treatment with Levothyroxine or Placebo in Older Adults Stratified by Thyrotropin Levels at Baseline
Range, 0–100; score derived from a 7-point Likert scale ranging from extremely dissatisfied to extremely satisfied; higher scores indicate more satisfaction regarding the effectiveness of levothyroxine.
Range, 0–100; score derived from a 5-point Likert scale ranging from extremely difficult to extremely easy; higher scores indicate more convenience regarding levothyroxine usage.
Range, 0–100; score derived from a 5-point Likert scale ranging from not at all confident to extremely confident; higher scores indicate more global satisfaction with levothyroxine usage.
Range, 0–100; score derived from a 5-point Likert scale ranging from extremely bothersome to not at all bothersome; higher values indicate less bothersome side effects from levothyroxine.
CI, confidence interval; IQR, interquartile range; SD, standard deviation; TSQM, Treatment Satisfaction Questionnaire for Medication.
Patient Satisfaction Regarding Treatment with Levothyroxine or Placebo in Older Adults Stratified by High vs. Low Symptom Burden for (A) Hypothyroid Symptoms and for (B) Tiredness Symptoms at Baseline
Range, 0–100; higher scores indicate more symptoms. The mean scores in the general population are 14 for hypothyroid symptoms and 35 for tiredness.
Range, 0–100; score derived from a 7-point Likert scale ranging from extremely dissatisfied to extremely satisfied; higher scores indicate more satisfaction regarding the effectiveness of levothyroxine.
Range, 0–100; score derived from a 5-point Likert scale ranging from extremely difficult to extremely easy; higher scores indicate more convenience regarding levothyroxine usage.
Range, 0–100; score derived from a 5-point Likert scale ranging from not at all confident to extremely confident; higher scores indicate more global satisfaction with levothyroxine usage.
Range, 0–100; score derived from a 5-point Likert scale ranging from extremely bothersome to not at all bothersome; higher values indicate less bothersome side effects from levothyroxine.
CI, confidence interval; IQR, interquartile range; ThyPRO, Thyroid-Related Quality of Life Patient-Reported Outcome; TSQM, Treatment Satisfaction Questionnaire for Medication.
Discussion
In this analysis of pooled data from two RCTs of community-dwelling adults aged 65 and older with SCH, patient satisfaction for treatment did not differ between those treated with levothyroxine or placebo with respect to perceived effectiveness, convenience, side effects, and global satisfaction. This was also true for participants with high or low symptom burden based on hypothyroid symptoms or tiredness, and for different thyrotropin levels at baseline. In addition, the participants’ desire for continuation of the study medication after the trial did not differ between both treatment groups, except for a subgroup of participants with high symptom burden using levothyroxine who more often wished to continue the study medication than those in the placebo group.
Assessment of treatment satisfaction for levothyroxine as a means to judge the efficacy of therapy, adds to other patient-reported outcome measures (PROMs) that are used to determine the success of therapy. Particularly, treatment satisfaction has been demonstrated to be sensitive to drug therapy-induced changes in various conditions. 25 –28 To the best of our knowledge, this is the largest RCT in which patient satisfaction for hormone replacement therapy in SCH was investigated. To date, we have found only one study that examined satisfaction with levothyroxine treatment in subjects with SCH. Razvi et al. conducted a randomized, double-blind, placebo-controlled crossover trial to investigate the effects of 12 weeks of levothyroxine treatment on cardiovascular risk profile and patient-reported outcomes in community-dwelling adults with SCH. 29 In line with our results, although in the short term, they found no significant effect of levothyroxine therapy on treatment satisfaction, which was measured using the 7-item Underactive Thyroid Treatment Satisfaction Questionnaire (ThyTSQ) (no quantitative outcomes shown). Likewise, these results were independent of baseline thyrotropin values.
Previous analyses from the TRUST and IEMO-80+ RCTs have shown no beneficial effect of levothyroxine treatment in older adults with SCH when investigating a broad range of clinical parameters, including thyroid-related quality of life, executive cognitive function, blood pressure, body mass index, 15,16 physical or mental fatiguability, 30 depressive symptoms, 17 muscle function, 31 bone health, 32,33 hemoglobin level, 34 carotid atherosclerosis, 35 systolic and diastolic heart function, 36 and risk of cardiovascular outcomes. 37 The present results, demonstrating no major effect of levothyroxine on treatment satisfaction in older adults with SCH, extend these findings. Only a subgroup of participants with high symptom burden from hypothyroid symptoms using levothyroxine more often desired to continue the medication after the trial when compared with placebo. This might point to some positive effect that these subjects are experiencing but has not been measured yet. However, caution should be exercised in interpreting these results. The numbers were small and given the precision of the estimate this could be a chance finding. Overall, the combination of outcomes does not support routine levothyroxine treatment of SCH in adults aged 65 years and older.
This study has certain strengths. To our knowledge, this is the first RCT to investigate patient treatment satisfaction with levothyroxine for SCH in older adults. We used the TSQM, a psychometrically sound and valid measure of the major dimensions of patient satisfaction with medication, 22 which has been shown to be sensitive to treatment-induced changes. 25 –28 As an additional measure, we asked participants whether they wished to continue the study medication after the trial. In our opinion, the treatment period of 1 year provided sufficient time for possible benefits concerning treatment satisfaction to become apparent. This is supported by results from the TSQM validation study showing that individuals on medication for <2 months reported significantly lower treatment satisfaction (for effectiveness and side effects) than those on medication for a longer period. 38 Another strength is that the participants’ perceptions were studied within the context of a blinded RCT. This is important since patient reported outcomes such as quality of life and treatment preference may not consistently align with thyrotropin levels. 39
There are also limitations to this study. First, it could be argued that low symptom scores at trial entry may have limited the possibility of detecting an effect on treatment satisfaction with levothyroxine. However, when comparing participants with high symptom burden from hypothyroid symptoms or tiredness, we did not observe more clinical benefits, 24 as well as no difference in treatment satisfaction between the levothyroxine and placebo groups as measured by the TSQM. Second, we cannot exclude the possibility that patient satisfaction for levothyroxine treatment would significantly differ from placebo under more intensive treatment leading to lower thyrotropin levels within the reference range. It must be noted though that Razvi et al. did not find a significant difference in treatment satisfaction using a higher dose of levothyroxine (100 ug) that resulted in a low mean level of thyrotropin (0.5 mIU/L) compared with placebo. 29 Finally, it could be argued that many of our subjects may have been euthyroid if age-adjusted thyrotropin reference values had been used. However, in clinical practice, medical laboratories have not yet implemented these. To date, many older adults are still diagnosed with SCH based on a single reference interval for all ages and receive thyroid hormone replacement therapy. Therefore, our findings remain relevant. At present, levothyroxine stands as one of the most commonly prescribed drugs globally 10,40 and is most frequently prescribed and initiated in older adults (50–70 years). 9 Despite a low prevalence (0.1–1.9%) and a consistent incidence of overt hypothyroidism, prescriptions have increased substantially over the past decades (2.3–3.5%). 10,11 This rise is likely attributed to increased SCH treatment. 12 In the United States, a study found that the majority (65.7%) of individuals starting levothyroxine were diagnosed with SCH. 41 Furthermore, studies have indicated a decline in thyrotropin levels at the onset of treatment. 42,43 This trend is concerning as it may increase the risk of ineffective treatment. These developments stress the relevance of studies investigating the treatment efficacy of SCH and emphasize the necessity to optimize related diagnostics.
This analysis of pooled data from two RCTs shows no major differences in patient satisfaction for treatment with either levothyroxine or placebo in older adults with SCH. This finding has important implications for the process of decision-making concerning the initiation of treatment for SCH and further supports refraining from prescribing thyroxin treatment in older adults with SCH.
Footnotes
Authors’ Contributions
Conceptualization: all authors. Data curation: all authors. Formal analysis: J.R., R.D.P., R.K.E.P., and J.G. Funding acquisition: S.M., J.G., P.K., and N.R. Investigation: all authors. Methodology: all authors. Project administration: R.D.P., S.M., J.G., P.K., and N.R. Supervision: S.M., J.G., P.K., and N.R. Validation: N/A. Writing: J.R., R.K.E.P., and J.G. Writing—review and editing: all authors. All of the authors provided final approval of the version of the article to be published and agreed to be accountable for all aspects of the work.
Author Disclosure Statement
J.R. reported receiving a grant from the Netherlands Organization for Health Research and Development (
Funding Information
A research grant from the
Supplementary Material
Supplementary Appendix