
Abstract
Background:
The COVID-19 pandemic's impact on thyroid function is a growing concern. Previous studies have produced inconclusive results, and there is a lack of comprehensive research into the long-term risks of thyroid dysfunction following COVID-19 infection.
Methods:
In this retrospective cohort study, we used data from the TriNetX international database, which includes electronic health records from a broad, diverse patient population. We compared patients with COVID-19 (cases) to those without (controls), matching for age, sex, race, and comorbidities using propensity score matching. The primary outcome was the diagnosis of thyroid dysfunction (thyrotoxicosis or hypothyroidism) within a 12-month period, analyzed using hazard ratios (HRs) and Kaplan–Meier curves, and stratified by age and sex.
Results:
Initially, the study included 1,379,311 COVID-19 patients and 6,896,814 non-COVID-19 patients from the TriNetX database. After matching, the cohorts were comparable in demographics and baseline characteristics. This study consistently demonstrated a significant increase in the risk of thyroid dysfunction, including thyrotoxicosis and hypothyroidism, among COVID-19 patients compared to non-COVID-19 patients. In the short term (3 months postexposure), the COVID-19 group exhibited a HR of 2.07 (95% confidence interval [CI] 2.01–2.12) for thyroid dysfunction, which included both thyrotoxicosis (HR 2.10, CI 1.92–2.29) and hypothyroidism (HR 2.08, CI 2.01–2.13). This heightened risk persisted over the long term (up to 12 months), with HRs indicating an ∼2.01-fold increased risk for overall thyroid dysfunction, a 1.8-fold increased risk for thyrotoxicosis, and a 2.04-fold increased risk for hypothyroidism. Subgroup analysis, stratified by age and sex, revealed a notably higher risk of thyroid dysfunction in patients aged 65 and above (HR 2.18, CI 2.11–2.25), compared to those in the under-65 age group (HR 1.97, CI 1.91–2.03). Both male and female patients were associated with an elevated risk, with females showing a slightly higher association with thyroid dysfunction (HR 2.12, CI 2.06–2.16) compared to males (HR 1.76, CI 1.69–1.82).
Conclusions:
COVID-19 infection was associated with an increased risk of thyroid dysfunction, including thyrotoxicosis and hypothyroidism, regardless of age or sex, during a 12-month follow-up period. Further research is required to validate these findings.
Introduction
COVID-19
There remains a significant knowledge gap concerning the long-term risks of thyroid dysfunction following COVID-19 infection. In the first month postinfection, it is hypothesized that thyroid dysfunction may result from direct viral effects on thyroid tissues or neurohormonal changes triggered by the systemic response to the infection. 19,20 However, the implications of COVID-19 on thyroid function appear to extend beyond this initial period. After one month, the role of autoimmune reactions becomes increasingly significant. Notably, several case reports and studies have documented occurrences of Graves' disease following COVID-19 infection, with onset times ranging from two weeks to two months. 13 –16 These findings, primarily based on case reports with small sample sizes and limited follow-up durations, limit their generalizability and long-term relevance. Similarly, occurrences of Hashimoto's thyroiditis have been reported, 17,18 suggesting a broader spectrum of thyroid-related autoimmune responses triggered by COVID-19.
To address these complexities, our study aims to systematically evaluate the risk of thyroid dysfunction over a one-year period following COVID-19, utilizing data from the Trinetx community-based large database. This longitudinal approach will assist in distinguishing the early effects directly attributable to the infection from the later autoimmune phenomena, thereby providing a comprehensive understanding of the temporal dynamics of thyroid dysfunction post-COVID-19. By utilizing the large-scale data available in the Trinetx database, our research intends to overcome the limitations of prior studies, such as small sample sizes and brief observation periods. This comprehensive approach allows for a more robust and detailed understanding of the trajectory of thyroid function following COVID-19.
Methods
Data source
In this retrospective, population-based matched cohort study, we employed the TriNetX analytics platform. TriNetX is a web-based, multi-institutional database encompassing deidentified electronic health records from over 100 million patients across various regional collaborative networks, including the United States, Europe, the Middle East, Africa, Latin America, and the Asia-Pacific region. The dataset comprises essential demographic information, diagnoses (International Classification of Diseases, Tenth Revision, Clinical Modification, ICD-10-CM), procedure codes (International Classification of Diseases, Tenth Revision, Procedure Coding System, ICD-10-PCS; Current Procedural Terminology), medication codes referencing Anatomical Therapeutic Chemical code or RxNorm (normalized medical prescription codes), as well as laboratory measurements (Logical Observation Identifiers Names and Codes).
Ethics statement
This study has been exempted from the requirement for informed consent. It involves a secondary analysis of preexisting data, which does not necessitate intervention or interaction with human subjects. Furthermore, the data have been de-identified in accordance with the standards outlined in Section 164.514(a) of the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. The de-identification process has been verified and certified by a qualified expert, as mandated in Section 164.514(b)(1) of the HIPAA Privacy Rule. Additionally, this study received an exemption waiver from the Institutional Review Board of Chung Shan Medical University Hospital, identified by the reference number CS2-20121.
Study population
Case group (COVID-19 cases)
The case group comprised patients diagnosed with SARS-CoV-2 infection (COVID-19) from January 1, 2020, to December 31, 2021, based on positive COVID-19-specific polymerase chain reaction tests or serological assays (Supplementary Table S1). Their index date was the initial COVID-19 test.
Control group (non-COVID-19)
The control group included patients with COVID-19-like symptoms but tested negative for SARS-CoV-2 within the same timeframe. Their index date was the date of the negative COVID-19 test. Patients with preexisting thyroid disorders or related surgeries were excluded from both the exposure and control groups. This approach ensures a well-matched control group for evaluating the impact of COVID-19 on thyroid function.
Baseline characteristics were obtained from the three months before the index date. Demographic factors encompassed age, sex, and race, while pertinent baseline comorbidities included hypertensive diseases (ICD-10-CM = I10–I16), overweight and obesity (ICD-10-CM = E66), type 2 diabetes mellitus (ICD-10-CM = E11), ischemic heart diseases (ICD-10-CM = I20–I25), cerebrovascular diseases (ICD-10-CM = I60-I69), hyperlipidemia (ICD-10-CM = E78), chronic obstructive pulmonary disease (ICD-10-CM = J44), and chronic kidney disease (ICD-10-CM = N18). Propensity score matching (PSM), facilitated by the built-in functionality of TriNetX, was executed to address baseline characteristic disparities between the two groups. This process established a 1:1 ratio match based on age, sex, race, and comorbidities.
Outcomes
The primary outcome of this study was the diagnosis of composite thyroid dysfunction (ICD-10-CM = E05, E01.8, E02, E03.8, E03.9), which included thyrotoxicosis (ICD-10-CM = E05) or hypothyroidism (ICD-10-CM = E01.8, E02, E03.8, E03.9). The follow-up period for assessing the outcome was defined as 12 months.
We chose to observe the study for 12 months for several reasons. First, this extended duration enabled a comprehensive evaluation of long-term thyroid dysfunction following COVID-19 exposure, capturing delayed or persistent effects. Second, we considered the possibility of autoimmune reactions affecting thyroid function, such as Hashimoto's thyroiditis and Graves' disease, which may develop over time. Lastly, a 12-month observation period was assumed to reduce diagnosis bias associated with conditions like subacute thyroiditis or NTIS, allowing differentiation between transient and longer-term thyroid abnormalities due to COVID-19.
Statistical analysis
All statistical analyses were conducted using the TriNetX platform. Balance of baseline characteristics was assessed through standardized mean differences (SMD), with well-matched variables defined as those with an SMD less than 0.1. Cox proportional hazards regression analysis facilitated the comparison of matched cohorts, with reported hazard ratios (HR) and 95% confidence intervals (CI). Incidence of thyroid dysfunction was calculated using the Kaplan–Meier method, accompanied by a log-rank test. Statistical significance was defined as a two-sided p-value of <0.05.
Results
Figure 1 illustrates the inclusion and flow chart of patients in this study. Initially, 104 million individuals were included from the TriNetX database. Patients exposed to COVID-19 were designated as cases, while those without exposure served as controls, resulting in 1,585,802 COVID-19 cases and 7,997,366 non-COVID-19 cases. To ensure data reliability, individuals previously diagnosed with thyroid diseases or who had undergone thyroid operations before the index date were excluded. This refinement yielded a cohort of 1,379,311 COVID-19 cases and 6,896,814 non-COVID-19 cases. Finally, PSM based on age, sex, race, and comorbidities was applied, establishing equal cohorts of cases and controls.
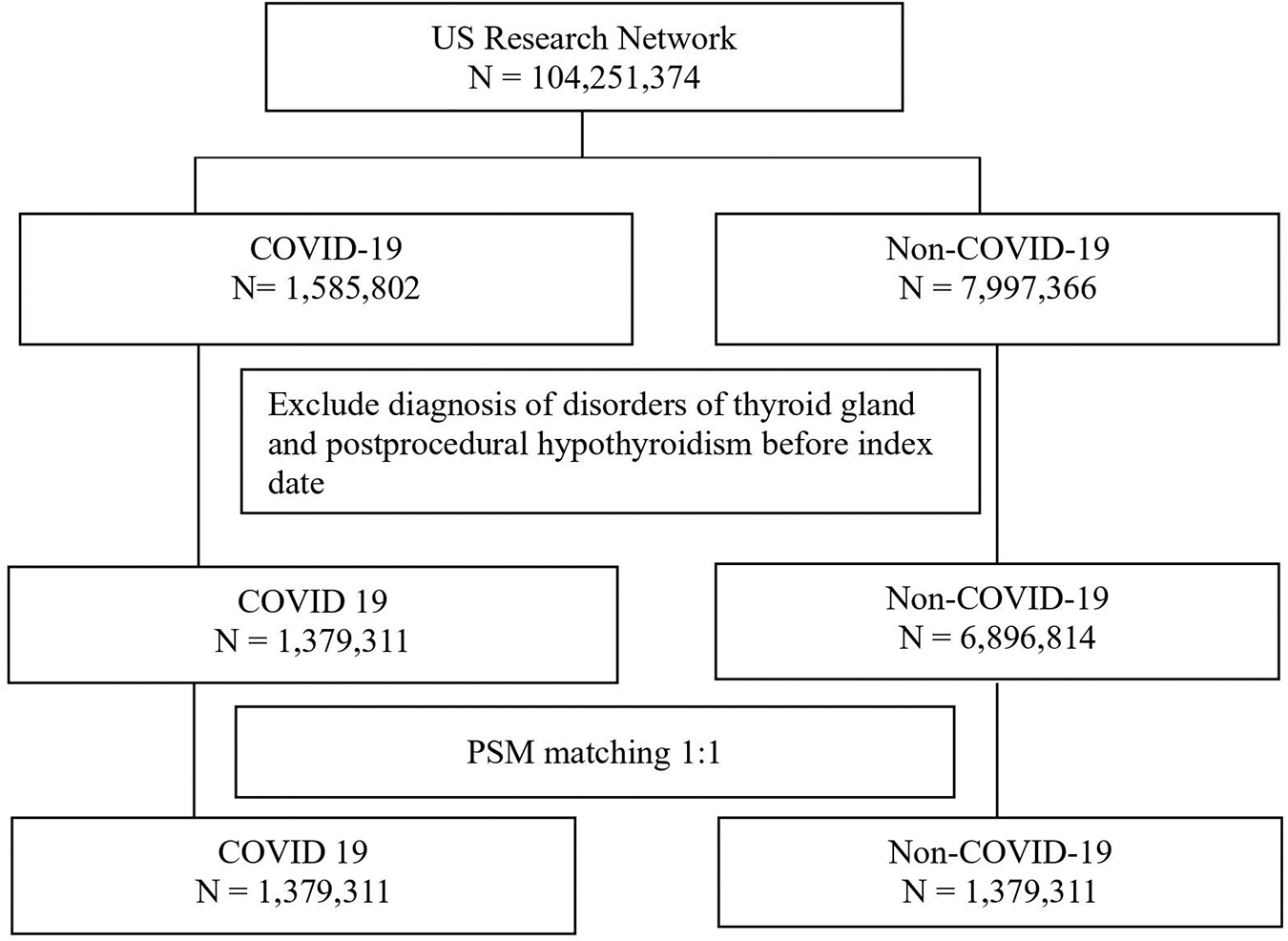
Participant flow diagram.
Table 1 in the study provides an overview of baseline characteristics before and after matching. Initially, significant demographic disparities, including age, sex, race, and comorbidities, were noted between the groups. Following PSM, adjusted to a 1:1 ratio, the cohort included 1,379,311 patients per group. SMD values below 0.1 indicated similar distributions in age, sex, race, and comorbidities. The average age was 39.7 years, and 52.4% were females, predominantly White (59.3%) and Black (19.8%). Key comorbidities such as hypertension, obesity, and type 2 diabetes were matched, enabling robust comparisons.
Demographic Characteristics of Patients with COVID-19 and Controls Non-COVID-19
COPD, chronic obstructive pulmonary disease; COVID-19, coronavirus disease 2019; PSM, propensity score matching; SMD, standardized mean difference.
Table 2 demonstrates that COVID-19 patients consistently have a higher risk of thyroid dysfunction, including thyrotoxicosis and hypothyroidism, compared to non-COVID-19 patients. In the short term (3 months) following COVID-19 exposure, the study recorded the following events: Thyroid dysfunction with 16,702 cases, thyrotoxicosis with 1545 cases, and hypothyroidism with 15,471 cases. However, it's important to note that the sum of thyrotoxicosis and hypothyroidism cases (1545 + 15,471 = 16,016) is not equal to the total number of thyroid dysfunction cases (16,702). The reason for this discrepancy lies in the definition of thyroid dysfunction as a composite endpoint that includes both thyrotoxicosis and hypothyroidism. Therefore, some patients may have experienced thyroid dysfunction characterized by a combination of thyrotoxicosis and hypothyroidism or may have developed both conditions sequentially.
Hazard Ratios of the Association with Thyroid Dysfunction According to Prior History of COVID-19 Infection
CI, 95% confidence interval; HR, hazard ratio.
Nevertheless, the risk of overall thyroid dysfunction at 3, 6, 9, and 12 months postexposure is ∼2.07, 2.13, 2.09, and 2.01 times higher, respectively. Similarly, the risks for thyrotoxicosis are 2.10, 2.01, 1.91, and 1.80 times higher, while for hypothyroidism, they are 2.08, 2.15, 2.12, and 2.04 times higher. This indicates a significant risk increase not only in the short term (within 3 months) but also in the long term (up to 12 months).
Supplementary Table S2 details the short-term effects of COVID-19 on thyroid function. Initially, in the 0–2 week period, the HRs (HR) for thyroid dysfunction, thyrotoxicosis, and hypothyroidism are 1.31 (CI 1.26–1.36), 1.48 (CI 1.28–1.70), and 1.30 (CI 1.25–1.35), respectively. These ratios rise notably in the 2–4 week interval, reaching 3.01 (CI 2.83–3.18) for thyroid dysfunction, 2.55 (CI 2.13–3.04) for thyrotoxicosis, and 3.08 (CI 2.90–3.27) for hypothyroidism. The HRs consistently indicate an elevated risk for these conditions during the 4–12 week follow-up.
Figure 2 in the study, consisting of Figure 2A–F, utilizes Kaplan–Meier curves to illustrate the patterns of thyroid dysfunction following COVID-19 exposure. These curves assess different durations: Figure 2A–C analyze the short-term effects (3 months postexposure), while Figure 2D–F examine the long-term effects (12 months postexposure). Figure 2A and D concentrate on overall thyroid dysfunction. Figure 2B and E focus on thyrotoxicosis. Figure 2C and F investigate hypothyroidism. This representation provides insights into both immediate and extended risks of thyroid dysfunction post-COVID-19.
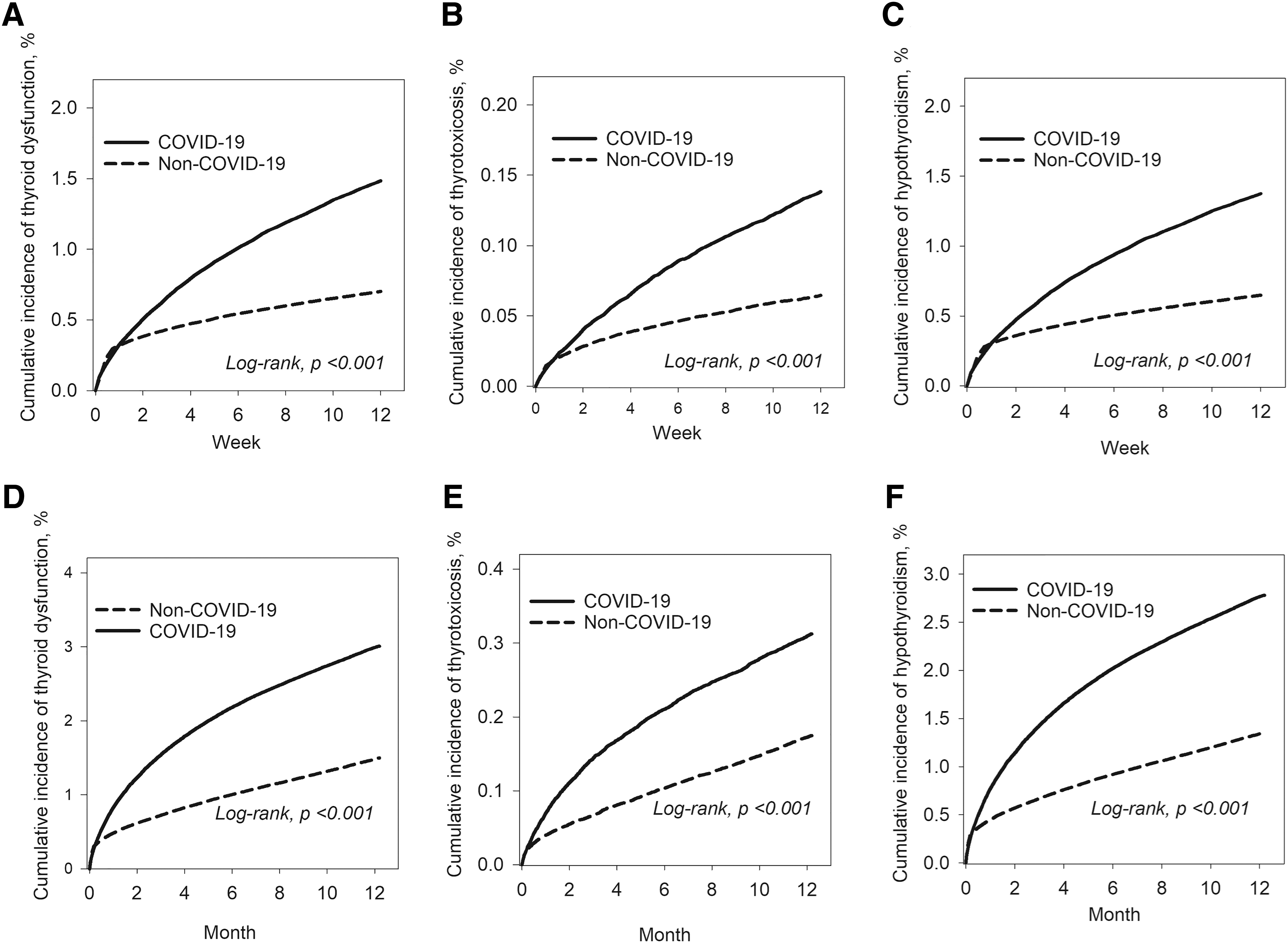
Kaplan–Meier curves examining the patterns of thyroid dysfunction following COVID-19 exposure.
The Kaplan–Meier curves demonstrate an elevated risk of thyroid dysfunction following COVID exposure, quantified by HRs at different time intervals. Two weeks postexposure, the HR is 3.01 (CI 2.83–3.18), indicating a significant divergence in risk trends that begins early and persists throughout the study period. At 3 months postexposure, the HR for thyroid dysfunction is 2.07 (CI 2.01–2.12), and it remains elevated at 12 months postexposure with a HR of 2.01 (CI 1.96–2.04). These values consistently indicate an increased risk of thyroid dysfunction both in the short-term and in the long-term following COVID exposure.
Table 3 of the study presents a detailed subgroup analysis, assessing the risk of thyroid dysfunction in COVID-19 patients over 12 months, categorized by age and sex. Increased risks are observed across all subgroups, with a notably higher risk in those aged 65 and above years old (HR 2.18, CI 2.11–2.55 for thyroid dysfunction) compared to the under 65 group (HR 1.97, CI 1.91–2.01). Both male and female patients exhibit elevated risk, with females displaying a slightly higher tendency toward thyroid dysfunction (HR 2.12, CI 2.06–2.16) than males (HR 1.76, CI 1.69–1.82).
Subgroup Analyses According to Age and Sex
Discussion
To date, this study is the largest and most extended investigation into the risk of thyroid dysfunction following COVID-19 exposure. Our findings reveal a statistically significant associations in increased risk, with HRs of 2.07 in the short term (0–3 months), 2.13 at 6 months, 2.09 at 9 months, and 2.01 in the long term (up to 12 months). These results underscore the enduring impact of COVID-19 on thyroid health, emphasizing sustained risks over an extended period. Notably, this heightened observed risk persists uniformly across different age groups and sexes, implying a universal impact of COVID-19 on thyroid dysfunction, including both thyrotoxicosis and hypothyroidism.
The association between thyroid dysfunction and COVID-19 has yielded mixed results in previous case reports and studies. Some investigations have explored the possibility of direct viral impact on the thyroid or the induction of cytokine responses that subsequently affect the thyroid or pituitary glands. 19–20 Specifically, studies conducted by Brancatella, 8 Muller, 11 and Lania 12 have reported an increased risk of thyrotoxicosis, which often presented as subacute thyroiditis, among individuals with COVID-19. Furthermore, the occurrence of subacute thyroiditis has been found in the research of Brancatella, 8 Ippolito, 9 and Asfuroglu. 10 Additionally, Chen conducted research on NTIS in the context of COVID-19. 6 Conversely, the study by Khoo et al. presents an alternative perspective, suggesting that the risk of thyroid dysfunction in COVID-19 patients may be minimal and negligible. 21
This study noted that the majority of COVID-19 patients had normal thyroid function upon hospital admission. 21 It's crucial to recognize that these case reports or studies have inherent limitations, primarily due to their small sample sizes and short follow-up duration. Furthermore, thyroid function tests were typically conducted within three days of hospital admission, which may not capture the full spectrum of thyroid-related outcomes that could develop in COVID-19 patients over time.
In the mid- to long-term duration, our findings suggest that the risk of thyroid dysfunction following exposure to COVID-19 is not solely attributable to direct thyroid insults or transient effects but may involve an influence on the immune response, potentially leading to autoimmune processes such as Graves' disease and Hashimoto's thyroiditis.
Several case reports, including patients from different countries and age groups, have provided insights into the potential impact of COVID-19 on thyroid health. 13 –18 These studies have reported cases of Graves' disease reactivation, new-onset cases, and rapid development of the condition following COVID-19 exposure. Salat et al. documented Graves' disease reactivation in a 60-year-old male patient 1 month after COVID-19 infection and in a 53-year-old female patient 2 months after COVID-19 infection. 16 Jimenez reported reactivation in two female patients (ages 45 and 61). 14 Additionally, Harris described a 21-year-old female patient who developed new-onset Graves' disease just 16 days after COVID-19 exposure. 15 Notably, Montebello from Malta also reported a 22-year-old individual with Graves' disease emerging 2 months after COVID-19 infection. 13
In addition, Tee et al. 17 from Singapore reported a 45-year-old male who developed Hashimoto's thyroiditis after 7 days of COVID-19 infection, while Dixit et al. 18 from the United States reported a 69-year-old female who developed Hashimoto's thyroiditis within 1 day of COVID-19 infection. Notably, when examining the existing literature, it becomes evident that the risk of hypothyroidism, as opposed to thyrotoxicosis, is relatively rare in COVID-19 cases. However, an intriguing divergence emerges when we consider our study's findings. Unlike the prevailing pattern in the literature, our research suggests that the risk of hypothyroidism after COVID-19 exposure is not less significant than that of thyrotoxicosis. This unexpected result prompts us to explore possible reasons behind this discrepancy. Further investigation is warranted to elucidate the mechanisms contributing to this distinctive observation and its implications for understanding thyroid dysfunction in the context of COVID-19.
In subgroup analyses, we observed that patients with COVID-19 consistently exhibit a higher risk of thyroid dysfunction, thyrotoxicosis, or hypothyroidism across all age groups and both sexes compared to those without COVID-19. Further subgroup analysis based on age reveals distinct patterns. In a secondary analysis, age of 65 years and older was associated with higher risk of thyroid dysfunction, thyrotoxicosis, or hypothyroidism compared to younger ages. This suggests that age may be a significant factor influencing the association between COVID-19 and thyroid dysfunction. Analysis by sex indicates that both females and males with COVID-19 have elevated HRs for thyroid dysfunction, thyrotoxicosis, or hypothyroidism compared to their non-COVID-19 counterparts. However, HRs are generally higher in females. Health care providers should be cognizant of the increased risk of thyroid dysfunction in patients with COVID-19, especially in specific subgroups. This awareness may impact diagnostic and monitoring strategies for thyroid function in COVID-19 patients.
Our study comes with several strengths and limitations. The strengths of this study are, first, the utilization of a large and multinational representative sample size. The use of the TriNetX analytics platform, encompassing electronic health records from over 100 million patients globally, provides a substantial dataset, allowing for more robust analyses. Second, we used real-world data, reflecting the conditions and variability encountered in actual health care settings. This aspect enhances the ecological validity of the findings, making them more applicable to real-life scenarios. Third, we employed a longitudinal analysis with a 12-month follow-up period, providing a temporal dimension to the relationship between COVID-19 and thyroid dysfunction. This longitudinal approach contributes valuable insights into the duration and persistence of thyroid-related outcomes following COVID-19 exposure.
Nevertheless, our study also has several important limitations. First, it does not account for the NTIS, which can manifest in a significant number of patients with acute infectious processes, including COVID-19 infection. Additionally, our study lacks data on the severity of COVID-19, including parameters such as hospital stay, admission to the intensive care unit, and the specific treatments administered (e.g., glucocorticoids or radiological contrast media agents). These factors can be critical in understanding the relationship between the extent of viral infection and the subsequent risk of thyroid dysfunction.
Furthermore, the retrospective design of our study relies on the quality and consistency of electronic health record data, which may vary across different health care systems. Nevertheless, detailed clinical information, such as thyroid hormone levels or thyroid antibodies, is not available. The use of diagnostic codes to define thyroid dysfunction, while common in large-scale studies, may oversimplify the multifaceted nature of thyroid-related outcomes. Despite our efforts to control for confounding factors, observational studies inherently encounter challenges in establishing causal relationships.
In conclusion, while our study provides valuable insights into the association of an increased risk of thyroid dysfunction, including both thyrotoxicosis and hypothyroidism, following COVID-19 infection across diverse age and sex groups, it is evident that additional research is essential. The need to validate these associations, explore potential confounding factors, and determine whether this risk represents a transient or chronic phenomenon cannot be overstated. To establish causation and develop effective preventive and management strategies, long-term studies and clinical trials are crucial. Our findings underscore the critical importance of clinical monitoring for patients recovering from COVID-19. Health care providers should be aware of the potential increased risk of future thyroid dysfunction in patients who have had COVID-19 infection.
Footnotes
Acknowledgment
Special thanks for Jing-Yang Huang and all study team for their dedication and support in this study.
Authors' Contributions
L.-A.H.: Conceptualization, writing—original draft. S.-C.L.: Conceptualization, methodology. Y.-S.Y.: Methodology, data analysis. C.-N.H.: Resources, supervision, data analysis. C.-C.W.: Investigation, review and editing. Y.-H.W.: Data curation, investigation, software, visualization, data analysis. E.K.: Resources, data analysis, supervision, writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from the Chung Shan Medical University Hospital (CSH-2019-C-018).
Supplementary Material
Supplementary Table S1
Supplementary Table S2