
Abstract
Background:
Orthotopic heart transplantation (HTx) is a long-term surgical therapeutic approach for patients with end-stage heart failure. The objective of the present study was to uncover associations between altered thyroid hormone (TH) status and adverse outcomes after HTx.
Methods:
In this prospective, single-center cohort study, 283 patients underwent HTx between 2013 and 2020 at the Heart and Vascular Center of Semmelweis University in Hungary. We measured serum free triiodothyronine (fT3), free thyroxine (fT4), and thyrotropin (TSH) pre- and postoperatively. TaqMan qPCR was used to measure type 2 deiodinase and type 3 deiodinase mRNA (Dio2 and Dio3, respectively) levels from the diseased heart bioptates. To assess the local TH action of the heart, mRNA levels of Hcn2 and Myh7 were measured in a subgroup of patients receiving extracorporeal membrane oxygenation (ECMO) postoperatively. Groups were compared using nonparametric tests. Cox regression analysis and logistic regression test were used to investigate the outcomes. The connection between serum TH parameters and cardiac gene expressions was assessed using linear regression.
Results:
Serum TSH (p = 0.009), fT3 (p < 0.001), and fT4 (p < 0.001) levels were lower after HTx than preoperatively. Levothyroxine (LT4) administered to donors was associated with better survival after 30 days (p = 0.049). LT4 replacement given to recipients after HTx was associated with better survival after 30 days (p = 0.018), 1 year (p = 0.002), and 2 years (p = 0.001). Dio3 mRNA level was significantly increased in patients who were treated with ECMO (p = 0.026), left ventricular assist device (LVAD) (p = 0.008), and biventricular assist device (BiVAD) (p = 0.013) preoperatively, and ECMO (p = 0.042) postoperatively, compared with those who did not require any type of mechanical circulatory support (MCS). We found no significant difference in the expression of the Hcn2 and Myh7 marker genes between patients on postoperative ECMO and those without MCS, and neither did they correlate with serum hormone levels (p = 0.519 and p = 0.056, respectively).
Conclusions:
We conclude that TH status plays an important role in HTx patients, and monitoring of TH status in the perioperative period may contribute to improved treatment outcomes. Our findings require independent confirmation in a randomized controlled clinical trial.
Introduction
Orthotopic heart transplantation (HTx) still stands as one of the gold standards and final therapeutic approaches for end-stage heart failure (HF). 1 Despite the constantly improving perioperative management of HTx, donor shortages remain one of the most important limitations of transplantation. 1 Enhancement of organ allocation strategies is needed.
Nonthyroidal illness syndrome (NTIS) or euthyroid sick syndrome are widely known terms for thyroid hormone (TH) alterations during critical care that is usually hallmarked by low serum levels of free triiodothyronine (fT3) and low or normal serum levels of free thyroxine (fT4) accompanied by an impaired response of the hypothalamic–pituitary–thyroid (HPT) axis represented by low or normal serum levels of thyrotropin (TSH). 2 The association between adverse outcomes after heart surgeries and postoperatively recorded NTIS is well documented in the literature. 3,4 Notably, the magnitude of changes in thyroid functions usually corresponds with the severity and criticality of NTIS and increases the probability of adverse outcomes of the patients’ critical condition. 5
The exact pathophysiological mechanisms underlying NTIS are still poorly understood. It was suggested that the acute and the chronic phases of NTIS are adaptive and maladaptive, respectively. 6 Importantly, TH economy is subjected to a complex regulation that involves both central components exerted by the HPT axis and local, tissue-specific mechanisms; essentially, both systems are affected by NTIS. 7,8 Recent data suggest that while different forms of the syndrome uniformly result in decreased HPT output, the local regulatory system of TH action is variably involved in different forms of NTIS. 9 TH activation and inactivation represent the critical component of local regulation of TH economy. Type 2 deiodinase (D2) is the main activator of TH and the main source of fT3 under nonhyperthyroid conditions, while type 3 deiodinase (D3) is responsible for inactivating TH. 7,10 Notably, NTIS has been shown to impact both the deiodinase tissues specifically. 9,11
To expand access for transplantable hearts, the United Network for Organ Sharing (UNOS) has recommended standard administration of TH replacement with levothyroxine (LT4) as a part of the donor management protocol. 12 Although supported by several studies, 4,13 this approach was independently associated with adverse outcomes. 14 While LT4 replacement for donors remains controversial, it might mitigate the severity of NTIS after HTx for recipients. 15,16
Our primary objective was to evaluate the potential benefits of TH replacement therapy on short- and long-term mortality rate following HTx. A secondary objective was to explore for any associations between both central and local parameters of TH economy, mechanical circulatory support (MCS) device implantation, and acute allograft rejection (as two of the most prevalent complications in the perioperative period after HTx). We also assessed the mRNA levels of the TH activating and inactivating D2 and D3 enzymes (Dio2 and Dio3, respectively)from the diseased heart specimens, to explore their potential role in the pathomechanism.
Materials and Methods
Design and setting
This prospective, single-center cohort study was performed on patients who underwent HTx at the Heart and Vascular Center of Semmelweis University, Budapest, Hungary, and provided written informed consent. The present study was approved by the Regional Ethics Committee of Semmelweis University in Budapest [ETT TUKEB 7891/2012/EKU (119/PI/12.) and IV/10161-1/2020/EKU]. Written informed consent was obtained from every patient.
Population and sampling
Classification of end-stage HF was categorized as per the ACC/AHA guidelines, 17 while functional classification was defined as per the New York Heart Association (NYHA) classification. 18 We included patients between 18 and 80 years who underwent heart transplant at the Heart and Vascular Center of Semmelweis University and the Department of Anesthesiology and Intensive Therapy of Semmelweis University, Budapest, Hungary, between February 2013 and November 2020. Exclusion criteria were pregnancy, exposure to iodine-containing contrast material, lack of written informed consent, and missing relevant data.
Donor management
Oversight of organ donation in Hungary falls under the purview of the National Blood Transfusion Service. The protocols governing donor management draw upon international standards. The determination of brain death was made by a team of experts in accordance with the accepted medical standards. Following the confirmation of brain death, the National Blood Transfusion Service collaborates with the Eurotransplant International Foundation to orchestrate the subsequent steps crucial for a successful transplant.
At the time of the determination of brain death, LT4 was administered as a part of a decision made by a team of experts. One hundred micrograms of LT4 was administered enterally every 24 hours during donor management. Once T4 therapy was initiated, it was administered regularly until explantation. Conditions that led to brain death are detailed in Supplementary Table S1.
Data collection
Preoperative, intraoperative, and postoperative data were collected, as detailed in Supplementary Methods.
Anonymously coded data were entered and systematized into our database management system.
Procedure and thyroid assays
Serum concentrations of TSH, fT3, and fT4 were measured as described. 19 The definitions of overt hypothyroidism, subclinical hypothyroidism, overt hyperthyroidism, and subclinical hyperthyroidism are as follows: overt hypothyroidism (TSH > 5.0 μU/ml and fT4 < 9 pmol/l), subclinical hypothyroidism (TSH > 5 μU/ml and fT4: 9.0–23.0 pmol/l), overt hyperthyroidism (TSH < 0.1 μU/ml and fT4 > 23.0 pmol/l), and subclinical hyperthyroidism (TSH < 0.1 μU/ml and fT4: 9.0–23.0 pmol/l).
Details are reported in Supplementary Methods.
Sample collection, RNA isolation, and gene expression
Well-characterized, deidentified human myocardial left ventricular (LV) samples from end-stage HF patients were collected during HTx from the diseased hearts immediately after explantation as provided in Supplementary Methods. qPCR was performed as previously described 9 and detailed in Supplementary Table S2.
Outcomes
Our primary outcome was long-term mortality, specifically defined as mortality within 2 years. Secondary outcomes included short-term and midterm mortality, assessed at 30 days and 1 year, respectively. Mortality rates were last assessed on June 6, 2023.
Acute allograft rejection after HTx was defined as an adverse event that requires enhanced immunosuppression with an International Society of Heart and Lung Transplantation (ISHLT) grade ≥ 2R endomyocardial biopsy result or hemodynamic compromise with noncellular reactions. 20,21 According to institutional protocols, echocardiography and endomyocardial biopsy were performed weekly in the first month after HTx was performed as well as after 3, 6, 9, and 12 months as a part of routine surveillance for allograft function.
The decision to implant an MCS device was always made by a team of experts, including a cardiac surgeon, a cardiologist, and a cardiac anesthesiologist, based on international protocols and guidelines.
Statistical analyses
Kolmogorov–Smirnov and Shapiro–Wilk statistical tests were applied to assess normality in the case of continuous data. Data with a normal distribution are presented herein as means and standard deviations (SD), while data with a non-normal distribution are presented as medians and interquartile ranges. Categorical data are presented as quantities (n) and percentages (%). Chi-square and Fisher’s exact tests were used to analyze categorical variables, while nonparametric tests were applied to assess continuous data.
Kaplan–Meier curves with log-rank tests were used to compare survival distributions. Univariate Cox regression analyses were performed to assess primary factors related to survival. Clinically and statistically relevant risk factors with a significance level of p < 0.20 in the univariate analysis were included in the multivariable model. Backward elimination was applied to produce mortality prediction models.
The association of all plausible factors (age, sex, LT4 replacement therapy) with 30-day rejection rate was evaluated via logistic regression models. Thyroid-associated variables with a significance level of p < 0.20 in the univariate model were entered into the final multivariable analysis. The multivariable logistic regression model was adjusted for age, sex, and T4 administration status. The Hosmer–Lemeshow goodness-of-fit test was applied for the final model. Harrell’s C-index (area under the receiver operating curve) was calculated to test the appropriateness of inclusion. R 2 using the Nagelkerke method was calculated also for logistic regression and Cox models to quantify the variation accountable to the investigated parameters. To account for multiple testing, the Bonferroni method was applied to adjust the p value. A p value < 0.017 was considered statistically significant. Pearson correlation was used to quantify the strength and direction of the linear relationship between serum thyroid parameters and thyroid marker genes.
All statistical tests were two-sided, and a significance level of p < 0.05 was considered statistically significant. Patients with missing data, such as thyroid parameters, were excluded from the study. IBM SPSS Statistics software (IBM Corp. Released 2021. IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp) was used to conduct statistical analyses. All statistical analyses were conducted by Dr. Pál Maurovich-Horváth, PhD, MPH, who is a professional statistician.
Results
Participants
A total of 387 patients’ data were evaluated for eligibility for the present study and 283 were included in the final analysis. A total of 104 patients were excluded due to missing thyroid values (Fig. 1).
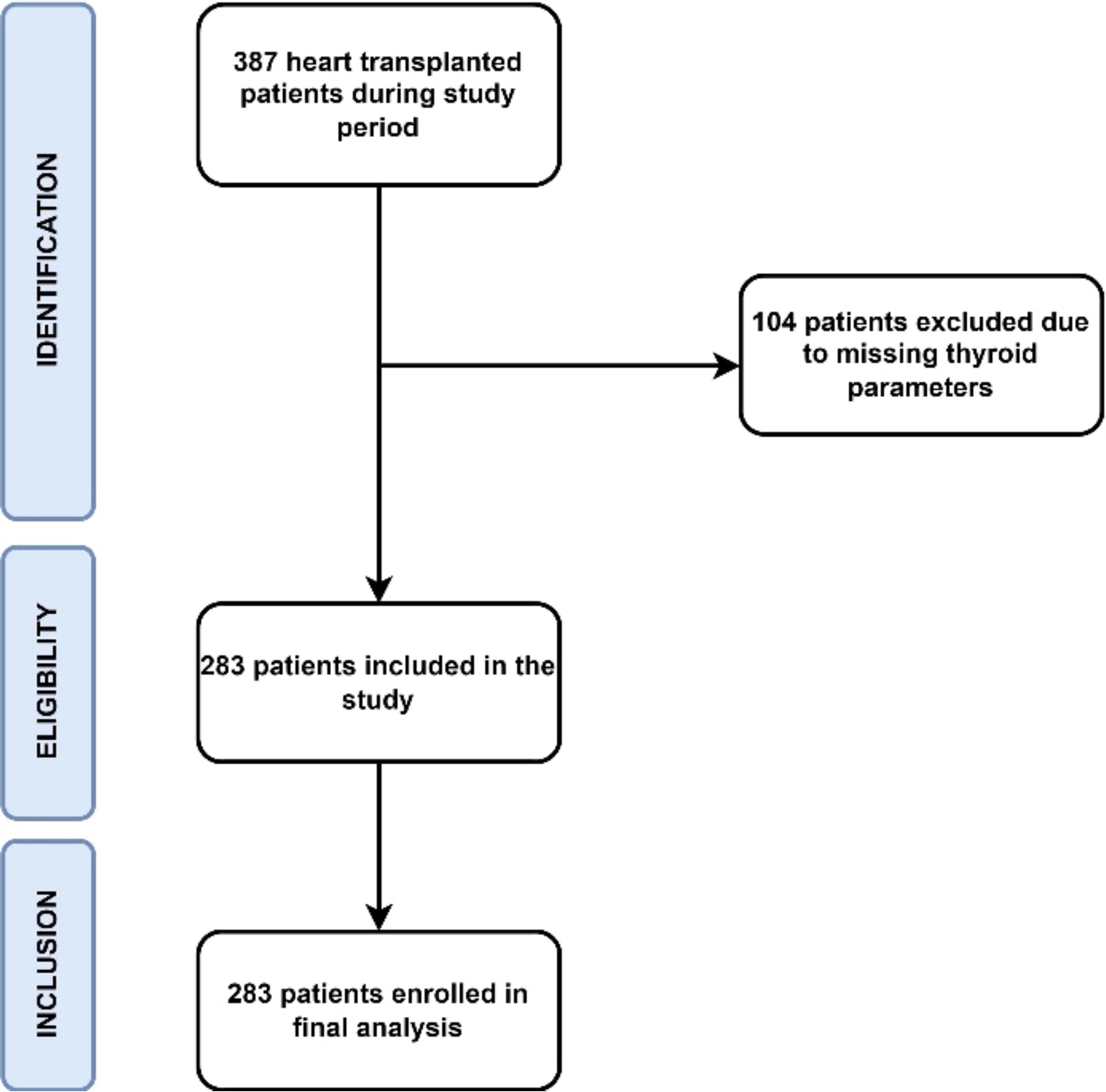
Participant flow diagram.
Descriptive and demographic data
The recipients’ median age was 54 years [interquartile range (IQR) 25–75: 45–59 years], and 71 female patients (25.1%) were included. The donors’ median age was 42 years (IQR 25–75: 32–50 years), of whom 70 were female (24.7%). Dilated cardiomyopathy (n = 187, 66.1%) and ischemic-dilated cardiomyopathy (n = 61, 21.6%) were the most common indications for HTx. The median follow-up time was 57.6 months (IQR 25–75: 29.5–81.7 months). The median Index for Mortality Prediction After Cardiac Transplantation (IMPACT) score was 4 (IQR 25–75: 2–10). All descriptive data are shown in Table 1. Detailed data on adverse effects after HTx are reported in Supplementary Table S3.
Patient Characteristics and Heart Transplantation Details
*The IMPACT score is a numerical measure used to predict the risk of mortality after HTx. The score typically ranges from 0 to 30, higher scores indicating an increased predicted risk of mortality after HTx.
BiVAD, biventricular assist device; BMI, body mass index; COPD, chronic obstructive pulmonary disease; DCM, dilated cardiomyopathy; ECMO, extracorporeal membrane oxygenation; IMPACT, Index for Mortality Prediction After Cardiac Transplantation*; IQR, interquartile range; I-DCM, idiopathic dilated cardiomyopathy; LVAD, left ventricular assist device; NYHA, New York Heart Association; RCM, restrictive cardiomyopathy; RVAD, right ventricular assist device.
Thirty-five patients (12.4%) were diagnosed with overt hypothyroidism, while 6 patients (2.1%) were diagnosed with subclinical hypothyroidism, and 19 patients (6.7%) were diagnosed with hyperthyroidism before HTx. Of the donors, 107 patients (37.8%) were given LT4 replacement during donor management. Thirty-two recipients (11.3%) took LT4 supplementation preoperatively, whereas 55 patients (19.4%) received LT4 replacement postoperatively. Seventy-eight patients (27.6%) were on amiodarone treatment. The patient characteristics are shown in Table 2.
Thyroid-Related Characteristics of Patients
fT3, free triiodothyronine; fT4, free thyroxine; IQR, interquartile range; postop, postoperative; preop, preoperative; TSH, thyrotropin.
Changes in TH levels
In the perioperative period after HTx, significant decreases were observed in the levels of serum TSH, fT3, and fT4. The serum TSH level declined significantly from a median value of 1.45 μU/mL (IQR 25–75: 0.80-3.81 μU/mL) preoperatively to a median value of 1.30 μU/mL (IQR 25–75: 0.39-2.92 μU/mL) postoperatively (p = 0.009). The serum fT3 level was reduced from 3.12 pmol/l (IQR 25–75: 2.49-3.79 pmol/l) preoperatively to a median of 2.38 pmol/l (IQR 25–75: 2.03-2.98 pmol/l) postoperatively (p < 0.001). The serum fT4 level exhibited a significant decrease from a median of 14.14 pmol/l (IQR 25–75: 11.63-15.96 pmol/l) preoperatively to a median of 11.81 pmol/l (IQR 25–75: 10.81-14.11 pmol/l) postoperatively (p < 0.001). These results are shown in Table 2. Recipients on LT4 replacement had significantly lower TSH levels after the administration of T4 (3.78 μU/ml vs. 1.96 μU/ml; p < 0.001). There was no significant difference in pre- and postoperative fT3 levels in patients who received LT4 (2.84 pmol/l vs. 2.42 pmol/l; p = 0.152).
Thyroid function and mortality
During the postoperative period of HTx, 42 patients (14.8%, n/n = 42/283) died within 30 days, 64 patients (22.6%, n/n = 64/283) died within 1 year, and 67 patients (23.7%, n/n = 67/283) died within 2 years. Kaplan–Meier curves show better survival with LT4 treatment in 30 days and in 2 years’ time, as shown in Figure 2. Univariate Cox regression models showed significantly better survival for the postoperative 30-day period in cases where donors received LT4 replacement (p = 0.049). Postoperatively administered LT4 replacement therapy was associated with better survival in the first 30 days, 1 year, and 2 years (p = 0.019, p = 0.004, and p = 0.003, respectively). After adjustment of the multivariable model for thyroid status (hypothyroidism, hyperthyroidism, LT4 replacement treatment, amiodarone treatment, and Dio mRNA levels), in addition to the IMPACT score (p < 0.001), postoperatively administered LT4 was associated with greater survival at the 30-day survival (p = 0.018) (Supplementary Table S4). A multivariable Cox regression analysis showed a statistically significant association between postoperatively administered LT4 and 1-year survival (p = 0.002) (Supplementary Table S5). LT4 treatment initiated in the postoperative period was associated with significantly better survival at 2 years (p = 0.001) (Table 3, Fig. 3).

Kaplan–Meier curves for 30-day
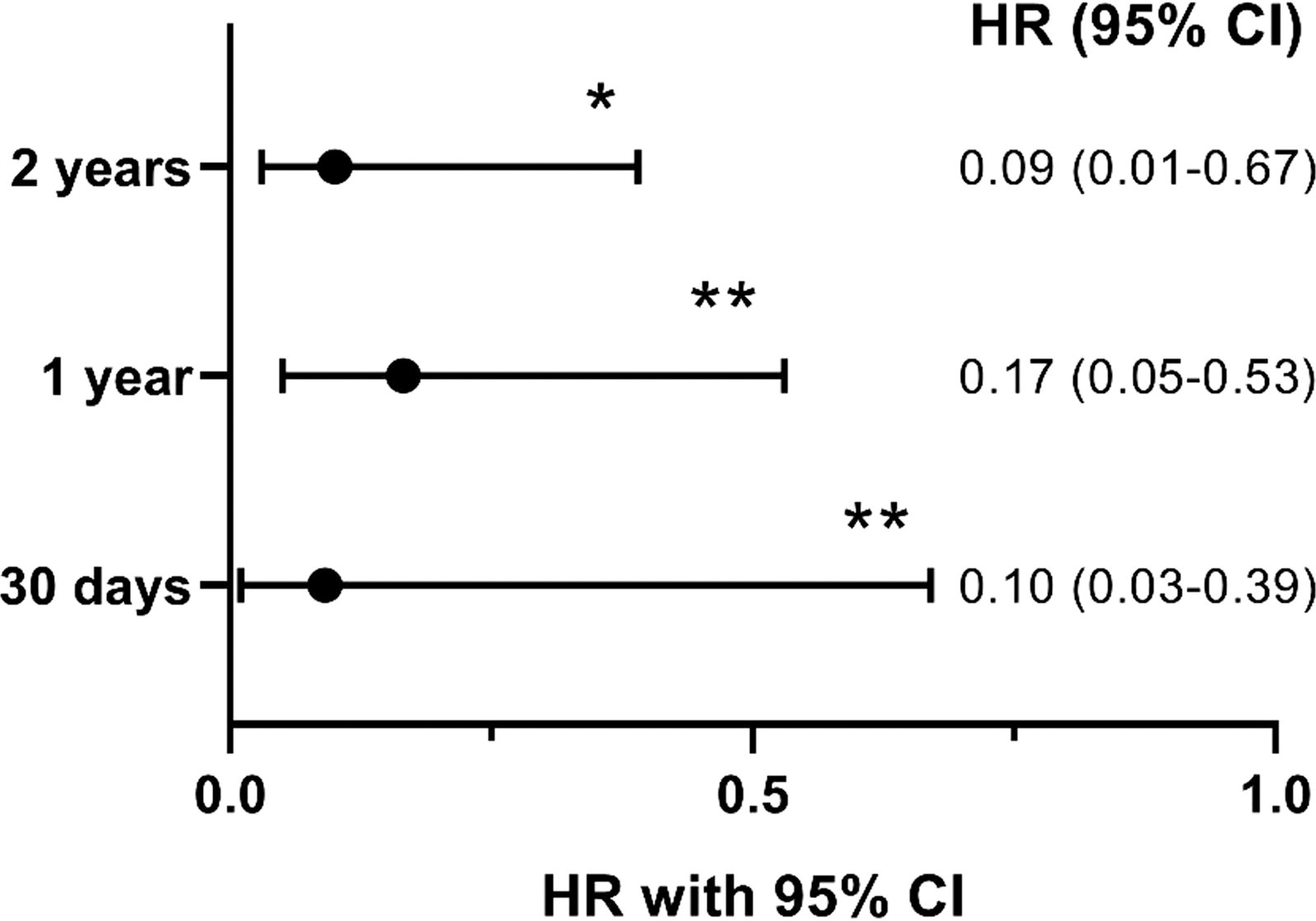
The association of postoperatively administered thyroxine and mortality assessed in multivariable Cox regression models at different time points. CI: confidence interval, HR: hazard ratio, *: p < 0.02, **: p < 0.002.
Univariate Analyses and a Multivariable Cox Regression Model Examining Associations with 2-Year Mortality After Heart Transplantation
A total of 275 patients were included in the multivariable analysis, Harrell’s C- index = 0.83, Nagelkerke R 2 = 0.39.
CI, confidence interval; Dio2, type 2 deiodinase mRNA; Dio3, type 3 deiodinase mRNA; IMPACT, Index for mortality prediction after cardiac transplantation. 22
Thyroid function and MCS
Preoperatively, 68 patients (24.0%) required extracorporeal membrane oxygenation (ECMO), 49 patients (17.3%) were treated with left ventricular assist device (LVAD), 41 patients (14.5%) required right ventricular assist device (RVAD), and 21 patients (7.4%) were treated with biventricular assist device (BiVAD) as a part of bridge to transplant solution. Furthermore, 69 patients (24.4%) required ECMO postoperatively. DIO2 and DIO3 expression levels were analyzed among the patients who required any type of MCS (Fig. 4.). There was no statistically significant difference in DIO2 expression between patients requiring MCS and patients who did not. However, a statistically significant difference was observed in DIO3 mRNA levels among these patient groups (p = 0.022). Preoperatively, DIO3 mRNA was significantly increased among those patients who were treated with ECMO compared with those who were not (n/n = 68/283, p = 0.026). Patients with preoperative LVAD implantation had significantly higher Dio3 expression than those patients who did not (n/n = 49/283, p = 0.008). Patients with BiVAD insertion had significantly higher DIO3 expression than those patients who did not require BiVAD implantation (n/n = 21/283, p = 0.013). Dio3 mRNA levels in patients with postoperative ECMO treatment were significantly elevated compared with those who were not treated with ECMO (n/n = 69/283, p = 0.042). In the case of RVAD insertion, a statistically significant difference was not observed regarding Dio3 expression (n/n = 41/283, p = 0.834).
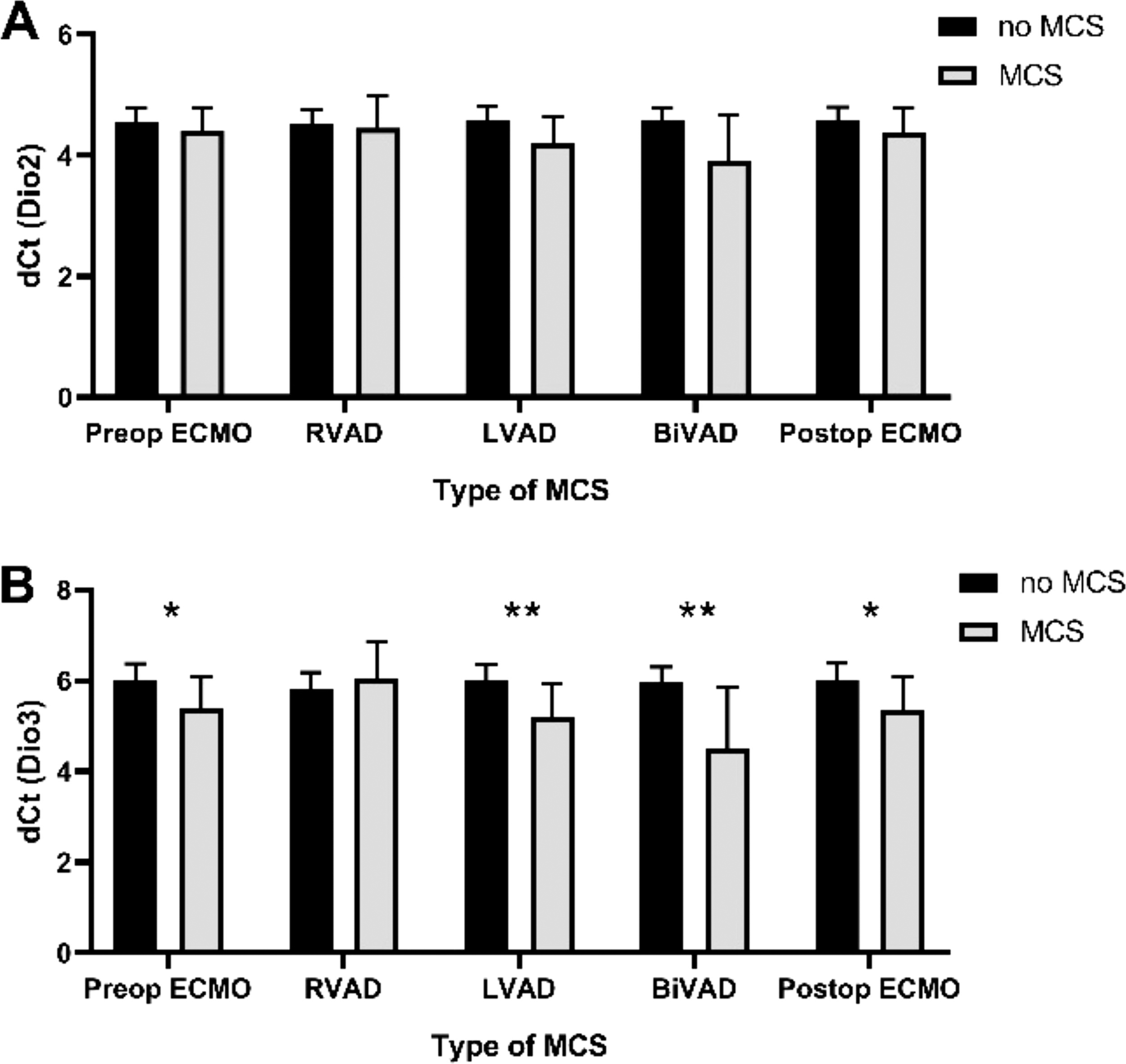
Deiodinase enzyme type 2
To evaluate local TH action in the heart, we also assessed the expression of the Hcn2 gene, positively regulated by TH, and the Myh7 gene, which is negatively regulated by TH. Hcn2 and Myh7 mRNA levels were measured in a subpopulation of 52 participants selected from those not requiring any MCS and cases where postoperative ECMO was applied. We found no significant difference in the expression of either marker gene between the on-ECMO and off-ECMO groups (Hcn2: 1.55 vs. 1.76, p = 0.519; Myh7:−11.26 vs.−11.15, p = 0.056, respectively). Neither marker showed a significant linear correlation with preoperative or postoperative serum hormone levels (Supplementary Table S6). Weak linear correlations were found between Hcn2 versus Dio2 (R 2 = 0.30, p = 0.001), and between Myh7 versus Dio3 (R 2=0.19, p = 0.002) (Supplementary Fig. S1).
Thyroid function and graft survival
Exploratory univariate logistic regression analyses were applied to assess possible associations between thyroid-related factors and 30-day acute allograft rejection (Table 4 and Supplementary Table S7). Moreover, the Hosmer–Lemeshow goodness-of-fit test had a nonsignificant p value of 0.807, indicating that our final multivariable regression model suitably fits the data presented. The final model was adjusted for age, female sex, T4 administration for donors, and LT4 replacement for recipients pre- and postoperatively. Final multivariable logistic regression analysis demonstrated a significant association between Dio2 expression and acute allograft rejection after HTx (odds ratio: 0.667; confidence interval: 0.517-1.861; p = 0.002). DIO3 expression was not associated with rejection after HTx (p = 0.344) (Hosmer–Lemeshow goodness-of-fit test p = 0.807).
Multivariable Logistic Regression Model Examining Potential Associations with Possible 30-Day Acute Allograft Rejection (ISHLT Grade ≥ 2R) After Heart Transplantation
A total of 271 patients were included in the multivariable analysis, Harrell’s C- index = 0.69, Nagelkerke R 2 = 0.21.
Dio2, type 2 deiodinase mRNA; ISHLT, International Society for Heart and Lung Transplantation.
Discussion
In this prospective, single-center cohort study, we conducted in-depth analyses, examining associations between thyroid status and survival as well as other possible adverse outcomes. Serum TSH, fT3, and fT4 levels were significantly decreased compared with preoperative levels. LT4 replacement administered to donors was associated with better survival at 30 days. Moreover, LT4 replacement in recipients after HTx was associated with better survival at 1 year and 2 years. These results support the findings of published data of other groups. 23 –26 The present knowledge on local TH action pre- and postoperation in the heart of HTx patients is highly limited. To gain insight into the local cardiac TH action of HTx patients, we measured mRNA expression of the two crucial TH metabolizing enzymes, Dio2 and Dio3, to study the general strategy of the heart for D2- and D3-mediated TH activation and inactivation, respectively. 27 Preoperative Dio2 and Dio3 mRNA levels were measured from intraoperative myocardial LV samples of the diseased hearts where Dio2 was not associated with any type of MCS device application. However, Dio3 mRNA was significantly increased in patients treated with LVAD, BiVAD, and ECMO pre- and postoperatively compared with those patients who did not require MCS. This would fall in line with the earlier observations, that D3 activity is elevated during hypoxia in the right ventricle of rats, which in turn decreases local T3 availability. 28
The impact of hypoxia on the expression of Dio3 in cells expressing this gene has been previously reported. 29 Importantly, Dio3 is positively regulated by T3, and its protein product serves as a critical regulator of intracellular T3, influencing local TH action. 7 It was revealed that hypoxia triggers the upregulation of Dio3 through a pathway dependent on hypoxia-inducible factor (HIF). 28 An increase in both D3 activity and mRNA levels was noted not only in response to hypoxia but also in the presence of hypoxia mimetics that enhance HIF-1 levels, as Dio3 may be a direct transcriptional target of HIF-1. 28,30 Furthermore, it was shown that endogenous D3 activity leads to a reduction in T3-dependent oxygen consumption in neuronal and hepatocyte cell lines, suggesting that hypoxia-induced D3 may play a role in lowering the metabolic rate in hypoxic tissues. 28
In light of this finding, we hypothesized that certain patients developed local hypoxia that increased the likelihood for requiring MCS despite the compensatory mechanisms of decreased T3 availability. We suspected that a higher Dio3 expression and consequently lower TH availability might indicate the severity of HF, influencing recovery and subsequent circulatory support.
To investigate this hypothesis, we attempted to assess local TH action in a subsample of our participants. Hcn2 is known to be positively regulated, while Myh7 is negatively regulated by TH action 31 and weak linear correlation was present between Myh7 and Dio3. However, we did not find evidence that MCS would affect the expression of these markers. In addition, the two markers showed no correlations with serum parameters and with each other. This suggests that either circulating TH levels are poorly reflected, or that our markers are less representative of cardiac TH action in these patients. However, it is important to note that endogenous markers are not only regulated by TH action, but also by various other mechanisms, including certain medications. 32 –34 Therefore, conclusions from these markers should be drawn with caution. Despite this, it is likely that changes in Dio3 expression are reflected with an attenuated effect on cardiac TH action in these patients and the heart may be attempting to maintain stable local T3 availability, possibly as a compensatory mechanism for NTIS.
Interestingly, Dio2 expression was found to be independently associated with acute allograft rejection after HTx. This would indicate that enhanced cardiac TH activation can be translated to increased local T3 availability. It is quite puzzling how increased T3 availability in patients suffering from NTIS would be disadvantageous. However, such a conclusion is difficult to make based on mRNA levels since the D2 enzyme is subjected to robust posttranslational regulation. 7 While a weak linear correlation was found between Hcn2 and Dio2 expression, we cannot exclude that the observed increase in Dio2 expression is only partially translated into actual T3 generation, but direct measurements of D2 activity and tissue TH status were impaired by the limited size of available tissue samples.
Cardiac surgical procedures usually result in a major stress response in the human body that might manifest in NTIS, which is common in several critical illnesses, and most of the affected patients require intensive care. 35,36 During extended NTIS with sufficient nutritional support, various tissue reactions may be seen as adaptations to the reduced availability of THs. These adaptations include heightened expression of monocarboxylate transporters, increased activity of D2, and enhanced receptivity at the receptor level. 23 Importantly, such changes are tissue-specific and include both enhancement of D2-mediated TH activation and suppression of D3-mediated inactivation. 11 Recently, it has been shown that changes in central and peripheral deiodination and consequently tissue TH action can also vary between different forms of NTIS in mice. 9,37 All these aspects of NTIS emphasize measuring local TH action tissue specifically.
Our results provide a novel insight into the tissue-specific characteristics of cardiac TH economy after HTx, a perspective that has been lacking thus far from human studies. To combat the adverse effects of NTIS, LT4 replacement therapy can be considered. This therapy is involved thoroughly in managing hemodynamically unstable potential organ donors, as it revitalizes suboptimal donor hearts, improves recipient myocardial aerobic metabolism, reduces the need for ionotropic and vasopressor agents, and prevents cardiovascular collapse. 38,39 Further studies revealed that LT4 replacement after brain death may increase the procurement rates and might enhance the salvage of potentially transplantable organs. 24 Moreover, attention was called to the administration of LT4 replacement before the declaration of brain death might be considered in potential organ donors. 40 A recent study enrolling more than 23,000 heart transplanted recipients with the use of the International Society of Heart and Lung Transplantation (ISHLT) registry underlined the independent association between donor T4 administration and elevated risk for early graft loss—defined as death or transplantation. 14 Another study from the same author concluded on the negative impact of donor T4 therapy, as it is independently connected to an increased risk of primary graft dysfunction via the withdrawal effect. 41 A recent multicenter trial found no benefit in intravenously administered T4 for hemodynamically unstable potential heart donors with respect to the number of hearts transplanted. 26 In addition, they observed more cases of tachycardia and severe hypertension in the T4 group that might be in association with the higher dose of T4 administered according to their protocol. On the contrary, graft survival at 30 days was slightly higher at the T4 group than in the saline group that may coincide with our results. 26 Reliable data are still missing on recipient TH usage; however, a retrospective study highlighted the association between decreased mortality and LT4 replacement therapy given to both donors and recipients. 42 A recent rodent study has shown that hypothyroidism before a cardiac event and hyperthyroidism after the event might be the optimal conditions. 43 At present, it is a matter of discussion whether LT4 replacement therapy is beneficial or harmful in the perioperative period of HTx and further studies will be required to be conclusive. However, our data show that both pre- and postoperative T4 supplementation is beneficial for survival. In conclusion, we found that the central parameters of TH economy, including TSH, fT3, and fT4, decreased after HTx compared with the preoperative levels, indicating the development of NTIS. LT4 replacement therapy for both donors and recipients might be beneficial in the postoperative period of HTx, as we found this to be associated with better survival. Dio3 mRNA levels were affected by the insertion of different types of MCS devices. In addition, a higher Dio2 expression in the heart that could be reduced by LT4 replacement is associated with acute allograft rejection, which is one of the most frequent complications after HTx.
Limitations
Our study was conducted as a nonrandomized, observational single-center study, and this was not a preregistered clinical trial. The study did not have an independent Data Safety Monitoring Committee and there were no criteria to stop the study early in the event of observations of benefit or harm, but the protocol was approved by the local research ethics board. The lack of randomization increases the risk of potential bias in interpreting the benefit of treatment effects, although we tried to address this by accounting for relevant confounders in respective multivariable analyses. Another source of bias is that we excluded patients with missing data and some of the analyses were performed only in a subgroup of patients, potentially contributing to some selection bias. Bioptate samples for assessing gene expression were available as cDNA samples and the size of the bioptates did not allow the determination of deiodinase enzyme activity. We acknowledge that the activity of the D2 enzyme does not necessarily strictly follow Dio2 mRNA levels due to the complex regulation of the enzyme. However, Dio3 mRNA levels correlate with enzyme activity relatively well and can be better interpreted directly. 7,44
Conclusions
Our findings suggest that monitoring of TH status in the perioperative period of HTx might contribute to appropriate LT4 treatment, fewer complications, and better survival in the short and long term. Further studies detailing local TH action in the heart are needed to confirm the importance of assessing the local characteristics of cardiac TH action and whether it is worthwhile to implement these evaluations into the clinical routine. Our findings regarding the treatment benefits of LT4 need to be confirmed in a randomized controlled clinical trial.
Footnotes
Acknowledgments
The authors acknowledge all patients who were willing to participate in the recent study and the medical staff of the Heart and Vascular Centre of Semmelweis University, who helped the authors in conducting the present research. The authors would also like to express gratitude to Dr. Pál Maurovich-Horváth for providing invaluable assistance with the statistical methods.
Data Availability Statement
All the data sets generated and analyzed during the present study are not publicly available but are available from the corresponding authors on reasonable request.
Authors’ Contributions
Balázs Szécsi: conceptualization, methodology, validation, formal analysis, investigation, and writing—original draft preparation. Richárd Sinkó: conceptualization, methodology, validation, and writing—review and editing. Alexandra Vereb: conceptualization, methodology, formal analysis, and investigation. Dmitry Khochanskiy: conceptualization, methodology, validation, and investigation. Kálmán Benke: conceptualization, methodology, validation, and writing—review and editing. Tamás Radovits: conceptualization, methodology, validation, resources, and writing—review and editing. Bálint Lakatos: conceptualization, methodology, validation, and investigation. Andrea Kőszegi: conceptualization, methodology, validation, and investigation. Eszter Losoncz: methodology, formal analysis, and investigation. Szilvia Kugler: conceptualization, methodology, formal analysis, and investigation. Márk Szabó: conceptualization, methodology, formal analysis, and investigation. Béla Merkely: methodology, validation, resources, and writing—review and editing. Andrea Székely: conceptualization, methodology, validation, formal analysis, investigation, resources, and writing—review and editing. Balázs Gereben: conceptualization, methodology, validation, and writing—review and editing.
Author Disclosure Statement
Balázs Szécsi, Richárd Sinkó, Alexandra Vereb, Dmitry Khochanskiy, Kálmán Benke, Tamás Radovits, Bálint Lakatos, Andrea Kőszegi, Eszter Losoncz, Szilvia Kugler, Márk Szabó, and Balázs Gereben have nothing to disclose. Andrea Székely received lecture fees from Baxter GmbH and General Electric HealthCare Hungary. Béla Merkely arranged institutional grants to the Heart and Vascular Center of Semmelweis University from Abbott, Astra Zeneca, Biotronik, Boehringer Ingelheim, Boston Scientific, Bristol-Myers Squibb, CSL Behring, Daiichi Sankyo, DUKE Clinical Institute, Eli Lilly, Medtronic, Novartis, Terumo, and VIFOR Pharma. Béla Merkely received lecture fees from Baxter GmbH, General Electric HealthCare Hungary, Abbott, Astra Zeneca, Biotronik, Boehringer Ingelheim, CSL Behring, Daiichi Sankyo, DUKE Clinical Institute, Medtronic, and Novartis.
Funding Information
Projects no. RRF-2.3.1–21-2022-00003 and RRF-2.3.1–21-2022-00011 have been implemented with the support provided by the European Union. TKP2021-EGA-23 and TKP2021-NVA-15 have been implemented with the support provided by the Ministry of Innovation and Technology of Hungary from the National Research, Development and Innovation Fund, financed under the TKP2021-EGA and the TKP2021-NVA funding schemes, respectively. NKFIH-1277-2/2020 project was financed by the Thematic Excellence Programme (2020-4.1.1.-TKP2020) of the Ministry for Innovation and Technology in Hungary, within the framework of the Bioimaging Thematic Programme of the Semmelweis University. This project was supported by a grant from the National Research, Development and Innovation Office (NKFIH) of Hungary (K134939 to TR).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Figure S1