
Abstract
Background:
International guidelines recommend targeted screening to identify gestational thyroid dysfunction. However, currently used risk factors have questionable discriminative ability. We quantified the risk for thyroid function test abnormalities for a subset of risk factors currently used in international guidelines.
Methods:
We included prospective cohort studies with data on gestational maternal thyroid function and potential risk factors (maternal age, body mass index [BMI], parity, smoking status, pregnancy through in vitro fertilization, twin pregnancy, gestational age, maternal education, and thyroid peroxidase antibody [TPOAb] or thyroglobulin antibody [TgAb] positivity). Exclusion criteria were pre-existing thyroid disease and use of thyroid interfering medication. We analyzed individual participant data using mixed-effects regression models. Primary outcomes were overt and subclinical hypothyroidism and a treatment indication (defined as overt hypothyroidism, subclinical hypothyroidism with thyrotropin >10 mU/L, or subclinical hypothyroidism with TPOAb positivity).
Results:
The study population comprised 65,559 participants in 25 cohorts. The screening rate in cohorts using risk factors currently recommended (age >30 years, parity ≥2, BMI ≥40) was 58%, with a detection rate for overt and subclinical hypothyroidism of 59%. The absolute risk for overt or subclinical hypothyroidism varied <2% over the full range of age and BMI and for any parity. Receiver operating characteristic curves, fitted using maternal age, BMI, smoking status, parity, and gestational age at blood sampling as explanatory variables, yielded areas under the curve ranging from 0.58 to 0.63 for the primary outcomes. TPOAbs/TgAbs positivity was associated with overt hypothyroidism (approximate risk for antibody negativity 0.1%, isolated TgAb positivity 2.4%, isolated TPOAb positivity 3.8%, combined antibody positivity 7.0%; p < 0.001), subclinical hypothyroidism (risk for antibody negativity 2.2%, isolated TgAb positivity 8.1%, isolated TPOAb positivity 14.2%, combined antibody positivity 20.0%; p < 0.001) and a treatment indication (risk for antibody negativity 0.2%, isolated TgAb positivity 2.2%, isolated TPOAb positivity 3.0%, and combined antibody positivity 5.1%; p < 0.001). Twin pregnancy was associated with a higher risk of overt hyperthyroidism (5.6% vs. 0.7%; p < 0.001).
Conclusions:
The risk factors assessed in this study had poor predictive ability for detecting thyroid function test abnormalities, questioning their clinical usability for targeted screening. As expected, TPOAb positivity (used as a benchmark) was a relevant risk factor for (subclinical) hypothyroidism. These results provide insights into different risk factors for gestational thyroid dysfunction.
Introduction
Thyroid hormones regulate the increased metabolic demand during pregnancy as well as fetal growth and development. 1 It is ubiquitously recognized that maternal gestational overt hypothyroidism requires levothyroxine treatment due to a high risk of adverse pregnancy outcomes. 2 –4 Milder forms of gestational thyroid function test abnormalities such as subclinical hypothyroidism and isolated hypothyroxinemia are much more prevalent 5 and have also been associated with a higher risk of adverse pregnancy outcomes, including pregnancy loss, 6 placental abruption, 7 pre-eclampsia, 8,9 gestational diabetes, 10,11 small for gestational age, 12,13 preterm birth 11,14,15 and adverse effects on offspring neurodevelopment. 16,17
Nonetheless, for milder forms of gestational thyroid function test abnormalities the absolute risk differences for adverse pregnancy outcomes are small, and randomized controlled trials yielded mixed results on the effect of levothyroxine treatment on pregnancy outcomes and offspring neurodevelopment. 18 –23 Consequently, many international guidelines recommend a targeted screening in high-risk women for the detection of gestational thyroid dysfunction rather than universal screening. 2,3,24
For the targeted screening approach, it is recommended to use both major established risk factors for hypothyroidism such as thyroid antibody positivity (when known), history of head or neck radiation and amiodarone or lithium use, as well as more common characteristics such as age above 30 years, body mass index [BMI] above 40 kg/m2, or multiple prior pregnancies. 2 Other factors such as smoking status and maternal education have also been associated with thyroid function test abnormalities in the past but are not currently included in any guidelines. 25
However, altogether these risk factors poorly distinguish women at high risk of gestational thyroid disease. Their combined use has been associated with the screening of 55–78% of women, while detection rates vary from 75% to 85% for women with overt hypothyroidism and 54–60% for women with subclinical hypothyroidism. 26 –28
The suboptimal differentiating potential of current risk factors can at least partially be attributed to the characteristics of the studies from which these were derived, since in those studies (1) risk factors were identified in nonpregnant populations, (2) risk factors were identified for thyrotropin (TSH) and free thyroxine (fT4) concentrations, rather than more clinically relevant thyroid dysfunction states, and (3) there was considerable between-study heterogeneity in methods and populations hampering the generalization of results to guidelines. 2,3,24
To provide more homogeneous results that are better suitable for incorporation into clinical guidelines, we performed an individual participant data meta-analysis to study risk factors for thyroid dysfunction in pregnancy. As a benchmark, we additionally studied the association of thyroid antibody positivity with different thyroid dysfunction states in pregnancy.
Methods
This study was conducted within the Consortium on Thyroid and Pregnancy (https://www.consortiumthyroidpregnancy.org), an international research collaboration that aims to study gestational thyroid (dys)function, physiology, determinants, and clinical risk profiles. There was no indication for additional approval of the Institutional Review Board, as all cohort studies included have obtained approval separately already by local review boards.
For this study, we followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Individual Patient Data guidelines and preregistered our study protocol (PROSPERO CRD42023422290; Supplementary Appendix S1). Cohorts included in the consortium were identified through a rolling systematic literature review, as described previously, 14 or were included after responding to our public invitations. 29 –32
Included in this study were prospective population-based cohort studies without selection criteria related to health status, with data available on potential risk factors and TSH, fT4, thyroid peroxidase antibody (TPOAb) and/or thyroglobulin antibody (TgAb) status during pregnancy. Quality of the studies and risk of bias were assessed using the Newcastle-Ottawa scale. 33 Exclusion criteria were pre-existing thyroid disease and medication usage affecting thyroid function test results. We analyzed multiple gestation pregnancies and pregnancy achieved through in vitro fertilization techniques (IVF) as a separate risk factor, but in analyses of other risk factors these women were excluded.
Definition of risk factors
Risk factors assessed in this study were those specified in the 2017 American Thyroid Association (ATA) guidelines for the diagnosis and management of thyroid disease during pregnancy 2 (if available in our data set) or those described in literature. 25,34 –37
Risk factors assessed were maternal age, BMI, smoking status (nonsmoking or quit after pregnancy was known vs. continued smoking), parity (nulliparous, 1, 2, or ≥3 births after 20 weeks of gestation), maternal education level (defined according to the International Standard Classification of Education 38 as low [ISCED 0–2], medium [ISCED 3–4], or high [ISCED 5–8]), gestational age at time of thyroid function testing in weeks, TPOAb and/or TgAb status (cutoff defined per cohort according to assay manufacturer), multiple gestation, pregnancy through IVF and iodine status (sufficient vs. mild-to-moderate-deficiency 39 ).
Iodine status was based on urinary iodine concentration (sufficient 150–250 μg/L, mild-to-moderate deficient 50–150 μg/L), either measured in the cohort or reported by national or international reports on iodine status at the study site and during the time of participants inclusion.
Definition of outcomes
The primary outcomes were a treatment indication or consideration, defined according to the 2017 ATA guidelines 2 and thyroid function test abnormalities (overt and subclinical hypothyroidism, isolated hypothyroxinemia, overt and subclinical hyperthyroidism). Secondary outcomes were continuous thyroid function test measurements (TSH and fT4). Trimester-specific reference intervals used to define thyroid function test abnormalities were defined in a cohort-specific manner based on the 2.5th and 97.5th percentiles in TPOAb negative women.
Overt hypothyroidism was defined as TSH above the 97.5th percentile and fT4 below the 2.5th percentile. Subclinical hypothyroidism was defined as TSH above the 97.5th percentile and an fT4 within the normal range (2.5th–97.5th percentile). Overt hyperthyroidism was defined as TSH below the 2.5th percentile and an fT4 above the 97.5th percentile. Subclinical hyperthyroidism was defined as a TSH below the 2.5th percentile and an fT4 within the normal range. Isolated hypothyroxinemia was defined as an fT4 below the 2.5th percentile and a TSH within the normal range.
We defined the trimesters as <13 weeks, 13–27 weeks, and >27 weeks of gestation. A treatment indication was defined as either overt hypothyroidism, subclinical hypothyroidism with TSH >10 mU/L, or subclinical hypothyroidism with TPOAb positivity. Since TPOAb status is part of the definition of a treatment indication, for the association of TPOAb positivity with a treatment indication we alternatively defined treatment indication as either overt hypothyroidism or TSH >10 mU/L (regardless of TPOAb status) to avoid any self-fulfilling definitions that include the exposure. The association of TPOAb positivity with subclinical hypothyroidism was studied separately.
Treatment indications for hyperthyroidism were outside the scope of this study, since gestational hyperthyroidism is often considered physiological, and we do not have data available to differentiate between gestational transient thyrotoxicosis and Graves' hyperthyroidism. 2
A treatment consideration was defined as a TSH between 2.5 mU/L and the upper reference limit with concomitant TPOAb positivity or subclinical hypothyroidism without TPOAb positivity. 2 No analyses on the association between a treatment consideration and thyroid antibodies were performed, since antibody status is part of the definition of a treatment consideration. For cohorts with repeated measurements, we used the first available sample for each trimester.
Statistical analyses
We used generalized logistic mixed regression models with a random intercept for each cohort to study the association of the exposures with thyroid function test abnormalities (compared with euthyroidism defined as TSH and fT4 between the 2.5th and 97.5th percentile) and a treatment indication or consideration. We calculated cohort-specific TSH and fT4 SD-scores to make values comparable between cohorts/assays while retaining interindividual differences and used linear mixed effect regression models with a random intercept for each cohort to study the association of the exposures with TSH and fT4.
All models were adjusted for maternal age, maternal education level, BMI, smoking, parity, gestational age at blood sampling, and fetal sex. We used multilevel multiple imputation for missing data on covariates creating five imputed data sets for pooled analyses. 40 In case of systematically missing data for an exposure within a cohort, that cohort was excluded from the analysis for that specific exposure. To assess the predictive ability of combined risk factors to discriminate women with thyroid hypofunction from normal subjects, we calculated receiver operating characteristic (ROC) curves.
ROC models were fitted using significant explanatory variables. TPOAb/TgAb status was excluded from the models to be able to assess both the direct predictive effects and indirect predictive effects through thyroid autoimmunity. All statistical analyses were performed using R statistical software 41 version 4.2.1 (packages lme4, mice, micemd, and sjPlot 42 –45 ). More detailed information on statistical analysis and a list of sensitivity analyses can be found in the Supplementary Data S1.
Results
Study population
The final study population comprised 65,559 women from 25 cohorts (Fig. 1), characteristics of whom are shown in Table 1. Of the total study population, the prevalence of thyroid function test abnormalities was 0.4% for overt hypothyroidism, 3.2% for subclinical hypothyroidism, 2.2% for isolated hypothyroxinemia, 1.4% for subclinical hyperthyroidism, and 0.9% for overt hyperthyroidism (Table 1). The prevalence was 1.7% for a treatment indication and 3.2% for a treatment consideration (Supplementary Table S1). Cohort-specific prevalence of thyroid dysfunction, detailed maternal demographics, and information on missing values per cohort are presented in Supplementary Tables S1–S3.

Study flowchart.
Characteristics of the Total Study Population
Descriptive statistics of all included women, denoted as the mean (SD), median (95% range) or count (percentage) as appropriate. Descriptive characteristics per cohort and detailed descriptions of missing data are shown in the Supplementary Data.
Defined according to modified International Standard Classification of Education classification.
A treatment indication was defined according to the 2017 American Thyroid Association guidelines as either overt hypothyroidism, subclinical hypothyroidism with TSH >10 mU/L, or subclinical hypothyroidism with TPOAb positivity. A treatment consideration was defined as a TSH between 2.5 mU/L and the upper reference limit with concomitant TPOAb positivity or subclinical hypothyroidism without TPOAb positivity.
BMI, body mass index; fT4, free thyroxine; IVF, in vitro fertilization; TgAb, thyroglobulin antibodies; TPOAb, thyroperoxidase antibodies; TSH, thyrotropin.
Maternal age
Higher maternal age was associated with a higher risk of subclinical hypothyroidism (absolute risks varied from ∼3.3% to 4.8% for maternal age between 20 and 40 years; Fig. 2), treatment indication (absolute risks varied from ∼1.1% to 2.2% for maternal age between 20 and 40 years; Fig. 2) and treatment consideration (absolute risks varied from ∼4.0% to 5.6% for maternal age between 20 and 40 years; Fig. 2).

Association of maternal age and BMI with the risk of thyroid function test abnormalities. A treatment indication and consideration were defined according to the 2017 American Thyroid Association guidelines. BMI, body mass index.
In addition, higher maternal age was associated with a higher risk of isolated hypothyroxinemia (absolute risks varied from ∼1.2% to 2.8% for maternal age between 20 and 40 years; Supplementary Fig. S1). Sample sizes per analysis and effect estimates for modeled associations are presented in Supplementary Tables S4 and S5.
Maternal BMI
A higher BMI was associated with a higher risk of overt hypothyroidism (absolute risk varied from ∼0.5% to 0.8% for BMI between 20 and 40 kg/m2; Fig. 2) while no association with subclinical hypothyroidism and the risk of a treatment indication or consideration was found (Fig. 2). Moreover, a higher BMI was associated with a higher risk of isolated hypothyroxinemia (absolute risk varied from ∼1.1% to 4.2% for BMI between 20 and 40 kg/m2; Supplementary Fig. S1).
Parity
A higher parity was associated with a lower risk of subclinical hypothyroidism (absolute risk varied from ∼3.9% to 3.2% between nulliparity and parity ≥3; Fig. 3) and treatment consideration (absolute risk varied from ∼4.8% to 3.3% between nulliparity and parity ≥3; Fig. 3). A higher parity was also associated with a higher risk of isolated hypothyroxinemia (absolute risk varied from ∼1.7% to 2.3% between nulliparity and parity ≥3; Supplementary Fig. S2), subclinical hyperthyroidism (absolute risk varied from ∼1.4% to 2.6% between nulliparity and parity ≥3; Supplementary Fig. S2) and overt hyperthyroidism (absolute risk varied from ∼0.7% to 1.2% between nulliparity and parity ≥3; Supplementary Fig. S2).
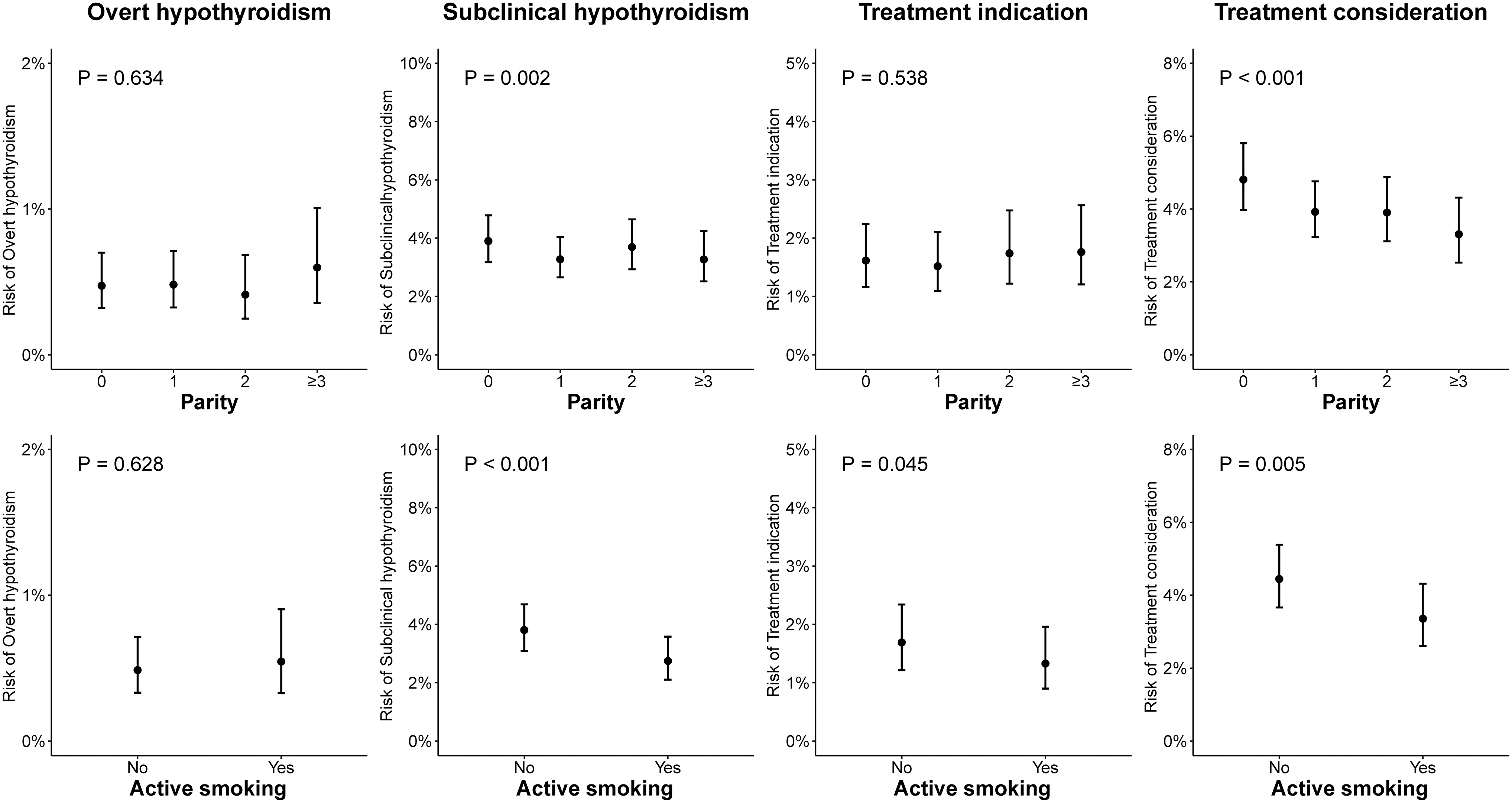
Association of parity and maternal smoking status with thyroid function test abnormalities. A treatment indication and consideration were defined according to the 2017 American Thyroid Association guidelines.
Smoking status
Active smoking was associated with a lower risk of subclinical hypothyroidism (∼3.8% vs. 2.6%; Fig. 3), treatment indication (∼1.7% vs. 1.3%; Fig. 3) and treatment consideration (∼4.4% vs. 3.7%; Fig. 3). In addition, active smoking was also associated with a higher risk of isolated hypothyroxinemia (∼1.9% vs. 2.4%; Supplementary Fig. S2) and a lower risk of overt hyperthyroidism (∼0.7% vs. 0.4%; Supplementary Fig. S2).
Pregnancy through IVF or twin pregnancy
There was no association between a pregnancy through IVF and thyroid function test abnormalities (Fig. 4 and Supplementary Fig. S3). No association was identified between a twin pregnancy and overt or subclinical hypothyroidism, or treatment indication or consideration (Fig. 4). A twin pregnancy was associated with a higher risk of isolated hypothyroxinemia (∼2.0% vs. 3.5%; Supplementary Fig. S3), subclinical hyperthyroidism (∼1.2% vs. 3.0%; Supplementary Fig. S3), and overt hyperthyroidism (∼0.5% vs. 5.7%; Supplementary Fig. S3).
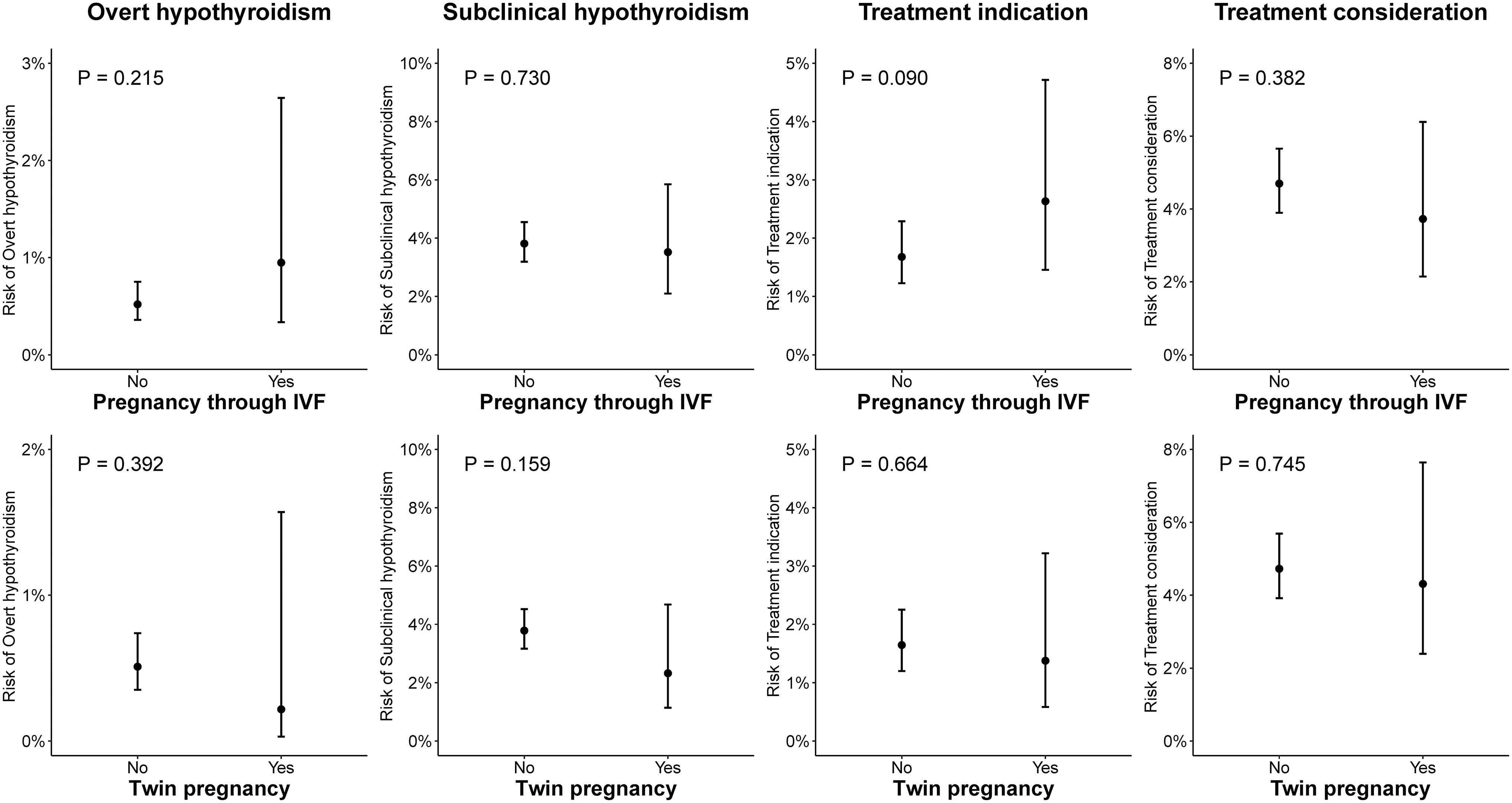
Association of pregnancy through IVF and twin pregnancy with thyroid function test abnormalities. A treatment indication and consideration were defined according to the 2017 American Thyroid Association guidelines. IVF, in vitro fertilization.
Thyroid autoimmunity
TPOAb positivity was associated with a higher risk of overt hypothyroidism (∼0.2% vs. 4.2%; Fig. 5), subclinical hypothyroidism (∼2.2% vs. 17.6%; Fig. 5), and treatment indication (∼0.2% vs. 3.9%, with treatment indication alternatively defined as either overt hypothyroidism or TSH >10 to avoid that the exposure is part of the outcome; Fig. 5). Moreover, TPOAb positivity was associated with a higher risk of isolated hypothyroxinemia and overt hyperthyroidism (approximate absolute risk differences <1%; Supplementary Fig. S4).

Association of thyroid autoimmunity with thyroid function test abnormalities. A treatment indication and consideration were defined according to the 2017 American Thyroid Association guidelines. Analyses with TPOAb and TgAb were performed in a subset with data on both autoantibodies. *Since TPOAb positivity is part of the definition of a treatment indication, treatment indication was alternatively defined as either overt hypothyroidism or TSH >10 mU/L. TgAb, thyroglobulin antibodies; TPOAb, thyroperoxidase antibodies.
Considering both TPOAb and TgAb, any thyroid autoimmunity was associated with a higher risk of overt hypothyroidism (approximate risk for women negative for TPOAbs and TgAbs 0.1%, isolated TgAb positivity 2.4%, isolated TPOAb positivity 3.8%, and TPOAb and TgAb positivity 7.0%; Fig. 5), subclinical hypothyroidism (approximate risk for women negative for TPOAbs and TgAbs 2.2%, isolated TgAb positivity 8.1%, isolated TPOAb positivity 14.2%, and TPOAb and TgAb positivity 20.0%; Fig. 5), and a treatment indication (absolute risk for TPOAb and TgAb negative women 0.2%, isolated TPOAb positivity 3.0%, isolated TgAb positivity 2.2%, and TPOAb and TgAb positivity 5.1%; Fig. 5).
In addition, any thyroid autoimmunity was associated with a higher risk of isolated hypothyroxinemia, overt and subclinical hyperthyroidism (approximate absolute risk differences <1%; Supplementary Fig. S4).
ROC curves, screening, and detection rates
To assess the predictive effect of combined significant risk factors, ROC curves were calculated using maternal age, BMI, smoking status, parity, and gestational age at blood sampling as explanatory variables. Associated areas under the curve (AUC) were 0.63 [95% confidence interval (CI) 0.60–0.67] for overt hypothyroidism and 0.58 [CI 0.57–0.60] for subclinical hypothyroidism. The AUCs for a treatment indication and consideration were 0.63 [CI 0.62–0.65] and 0.58 [CI 0.57–0.60], respectively (Fig. 6). The screening rate in all cohorts combined using risk factors currently recommended (maternal age >30 years, parity ≥2, and BMI ≥40) was 58%, with a detection rate for overt and subclinical hypothyroidism of 59%.
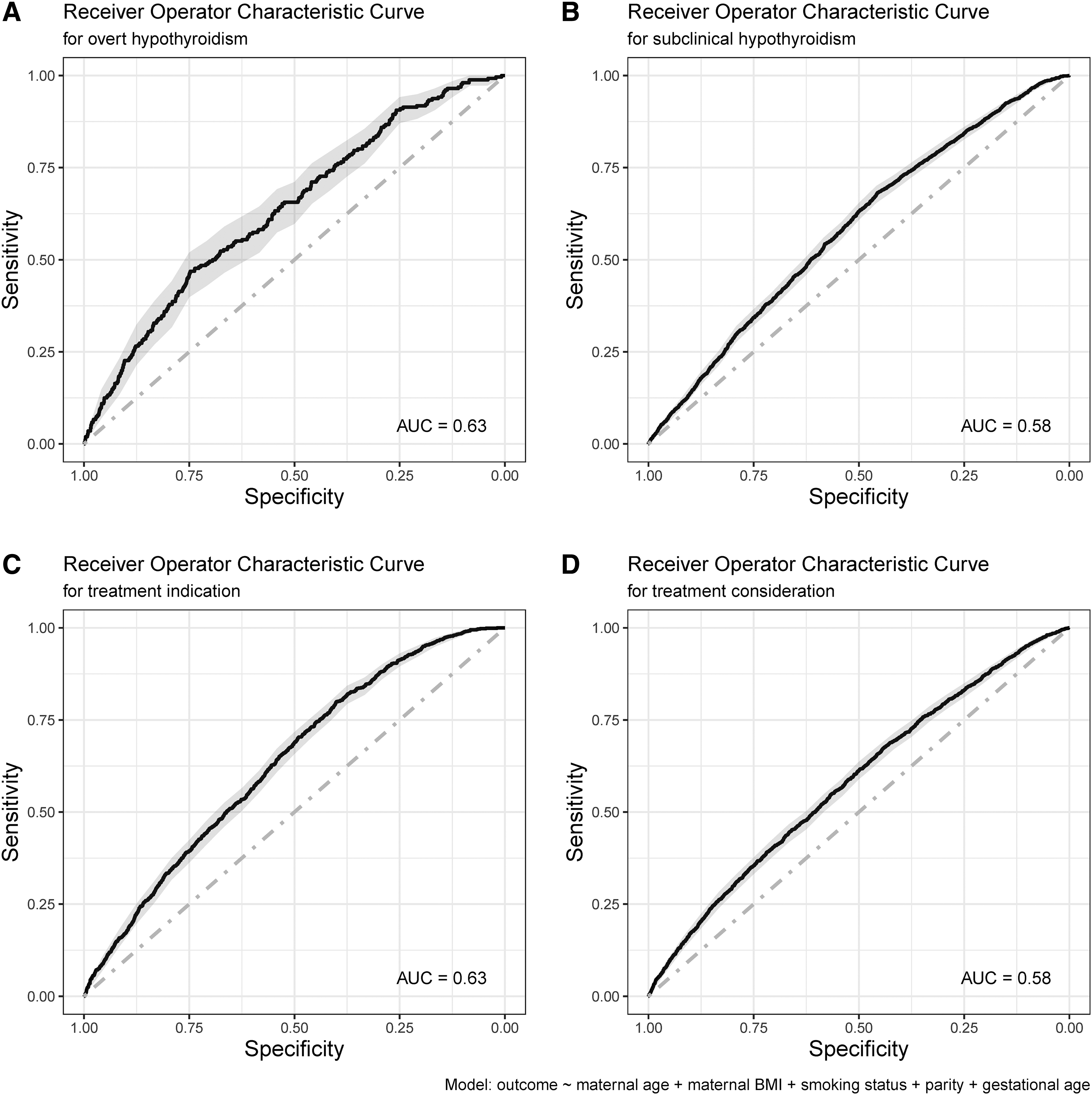
Receiver operating characteristic curves. Visualization of discriminatory ability of significant explanatory variables; maternal age, BMI, smoking status, parity, and gestational age at blood sampling. TPOAb/TgAb status were not included in the models to be able to assess both the direct predictive effects and indirect predictive effects through thyroid autoimmunity. A treatment indication and consideration are defined according to the 2017 American Thyroid Association guidelines.
Additional results and sensitivity analyses
Gestational age at blood sampling and maternal education
Higher gestational age at blood sampling was associated with a lower risk of overt hypothyroidism (absolute risks varied from ∼0.9% to 0.1% between week 6 and 36; Supplementary Fig. S5). Gestational age was also nonlinearly associated with all other states of thyroid dysfunction, with higher risks of overt hyperthyroidism (Supplementary Fig. S5) and treatment indication at week 10–12 and a lower risk of subclinical hypothyroidism and a treatment consideration between week 10 and 12 (Supplementary Fig. S6). Maternal education was associated with subclinical hypothyroidism, isolated hypothyroxinemia, and overt hyperthyroidism (approximate absolute risk differences <1%; Supplementary Fig. S5).
TPOAb sensitivity analyses and adjustments
The association of maternal age with subclinical hypothyroidism was no longer statistically significant after adjusting for TPOAb status (p = 0.30; Supplementary Fig. S7). Adjustment for TPOAb positivity did not change any other associations (Supplementary Figs. S7–S10). Associations between risk factors and TSH/fT4 were in line with analyses on thyroid dysfunction states and are presented in Supplementary Figures S11 and S12.
The association of TSH SD-scores with gestational age at blood sampling significantly differed according to TPOAb status (Supplementary Fig. S13). TPOAb positivity was associated with a positive increase of TSH SD-scores between week 10 and 15 of gestation, while the absence of TPOAb positivity was associated with a decrease of TSH SD-scores during this period. For TPOAb positive women fT4 SD-scores were lower, especially in early pregnancy (Supplementary Fig. S13).
Risk of thyroid dysfunction per combination of risk factors
We stratified the incidence of outcomes per risk factor and per combination of risk factors in Supplementary Tables S6–S12. The absolute risks varied from 0.5% to 0.8% for overt hypothyroidism and from 3.4% to 4.6% for subclinical hypothyroidism in the presence of single or double risk factors (Supplementary Tables S6 and S7). The absolute risks varied from 1.7% to 2.3% for a treatment indication and from 3.7% to 4.1% for a treatment consideration (Supplementary Tables S8 and S9).
The risks for isolated hypothyroxinemia varied from 2.1% to 15.9% in the presence of single or double risk factors and was especially high in women with both a high BMI and age >35 years (absolute risks varying from 9.2% to 11.6%) and for women with a high BMI and parity ≥3 (absolute risks varying from 10.2% to 15.9%; Supplementary Table S10). Sensitivity analyses showed no interaction effect between maternal age and BMI (p = 0.70) and between BMI and parity (p = 0.36).
Thyroid autoantibody positivity per thyroid dysfunction state
Thyroid autoantibody positivity per thyroid dysfunction state is presented in Supplementary Table S13. Of all women classified as overt hypothyroidism, 80.1% were positive for TPOAb and/or TgAb. Out of all women classified as subclinical hypothyroidism, 44.2% were positive for TPOAb and/or TgAb (Supplementary Table S13).
Iodine status
No difference in the mean prevalence of a thyroid function abnormalities was found between cohorts with a mild-to-moderate iodine-deficient status and cohorts with a sufficient iodine status (Supplementary Table S14). Iodine status and trimester-specific reference intervals per cohort can be found in Supplementary Tables S15 and S16.
Discussion
Identifying and quantifying risk factors for gestational thyroid function test abnormalities may improve targeted screening strategies. In this study, we show that higher maternal age, higher BMI, nulliparity, and nonsmoking status are associated with a higher risk of gestational thyroid dysfunction or thyroid function test abnormalities for which treatment is indicated or should be considered. However, the absolute difference in the risk of thyroid dysfunction for these risk factors was limited, questioning their added benefit for targeted screening.
We studied TPOAb positivity as a benchmark for clinically meaningful risk, and also provide data on TgAb positivity, showing that isolated TgAb positivity is a risk factor for overt and subclinical hypothyroidism as well as for a treatment indication, but not to the same extent as TPOAb positivity.
International guidelines recommend using targeted screening approaches to identify gestational thyroid dysfunction. Although we reached statistical significance to show that maternal age, BMI, parity, and smoking status are risk factors for gestational thyroid dysfunction, the small absolute risk differences implicate that there is no clinically meaningful difference that could improve screening efforts. 46 This is supported by the ROC curves and the corresponding AUCs (ranging from 0.58 to 0.63; Fig. 6). Pragmatically, omitting the use of these highly prevalent risk factors from a targeted screening algorithm would result in less women screened.
In this study, at least one of the three studied risk factors (maternal age >30 years, parity ≥2, or BMI ≥40) was present in 58% of all women, while the detection rate for overt and subclinical hypothyroidism was only 59%. These rates are comparable with previous studies. 26 –28 These data aid the general discussion on the harms and benefits of (targeted) screening. On one hand, omitting these risk factors from a targeted screening approach could result in reduced benefits by lower detection of gestational hypothyroidism. On the other hand, it would result in reduced harms due to both a lower detection of mild thyroid function test abnormalities (for which it remains unknown if levothyroxine treatment is warranted) and less overdiagnosis and/or overtreatment. The results of this study do not aid policy makers in recommending for or against universal or targeted screening. Instead, the results of this study suggest the reconsideration of risk factors for targeted screening and stimulate identification of more relevant risk factors.
Currently, known TPOAb positivity has been included in both obstetric and endocrinology guidelines as an indication for gestational screening for thyroid dysfunction, while no consensus has been reached on known TgAb positivity. 2,3,24 As expected, TPOAb positivity was associated with a meaningful higher risk of (subclinical) hypothyroidism (Fig. 5). Vice versa, out of all women with overt hypothyroidism 68.1% was positive for TPOAbs and 35.0% of women with subclinical hypothyroidism were TPOAb positive (Supplementary Table S13).
It was previously shown that in pregnancy, both TPOAb-positivity and TPOAbs on a continuous scale are independently associated with TSH and fT4 concentrations. 47 TgAb positivity and concentration, respectively, were also independently associated with higher TSH concentrations but the association between TgAbs and TSH and fT4 concentrations were no longer significant after adjusting for TPOAbs. 47 Based on this study, there seems little added value of adding TgAb positivity on top of known TPOAb positivity as an indication for thyroid function testing in pregnancy since the vast majority of women with TgAb positivity were also TPOAb positive (Supplementary Table S13).
Moreover, only 2.2% of women with isolated TgAb positivity had a treatment indication according to the 2017 ATA guidelines (data not shown). 2 Our results do support current recommendations that in case of (known pre-existing) TPOAb positivity, for instance as assessed during a fertility program, additional testing for gestational thyroid function should be performed. In the odd case that there is known pre-existing TgAb positivity but an unknown TPOAb status, the large overlap between positivity for both antibodies would be an argument in favor of also testing gestational thyroid function in these cases.
The results of this study also provide a physiological perspective. A higher maternal age was associated with a higher risk of overt and subclinical hypothyroidism, but this was primarily mediated through TPOAb positivity, which is in line with population-based studies and fits with the cumulative risk of thyroid autoimmunity during aging. 48,49 We also found that a higher BMI was associated with higher TSH and lower fT4 concentrations, which adds to mixed results published so far. 50 –52 Multiple hypotheses have been postulated for the potential bidirectional association of thyroid function tests with BMI and obesity, including a role for leptin, which indirectly stimulates TSH secretion and altered deiodinase expression and activity in obese individuals leading to changes in thyroid function tests, suggesting an effect of BMI on thyroid function. Other hypothesis includes a decreased energy expenditure in individuals with relatively low fT4 concentrations possibly leading to weight gain, suggesting an effect of thyroid function on BMI. 53,54
Another noteworthy result is the association of increasing parity with a lower risk for subclinical hypothyroidism and a treatment consideration, which seems primarily driven by lower TSH values in women with higher parity (Supplementary Figs. S11 and S12). It could be hypothesized that changes in either TPOAb or human chorionic gonadotropin (hCG) are responsible for these findings, but results were consistent after adjusting for TPOAb in our study and previous research on the association between parity and hCG demonstrated lower hCG concentrations with increasing parity. 55,56 The recommendation by the 2017 ATA guidelines to screen women with parity ≥2 was based on a postpartum cohort, which could explain this discrepancy. 2
Interestingly, smoking was associated with lower fT4 serum concentrations, a lower risk of subclinical hypothyroidism, and a higher risk of isolated hypothyroxinemia. These results are in line with other population-based studies that found lower fT4 concentrations in smoking individuals, lower thyroid autoimmunity, and a lower risk of hypothyroidism, although results are heterogeneous. 37,57,58 And while a protective effect of smoking may be suggested here, it is unlikely that such an effect would persist if clinical endpoints would be taken into account. 59 Moreover, smoking in pregnancy has previously been associated with an increased risk of other forms of thyroid dysfunction such as Graves' disease and postpartum thyroiditis. 36,60
Another relevant result is that twin pregnancy was associated with overt and subclinical hyperthyroidism. In subgroup analyses, this association was only present during early pregnancy (8–14 weeks), which is in line with the results of a recent Chinese study 61 and coincides with the hCG peak at the end of the first trimester that is more prominent in multiple pregnancies. 62,63 To what extent the higher risk of hyperthyroidism in twin pregnancies also translates to the risks of pregnancy complications remains to be elucidated.
In this study, we were able to assess the association of multiple risk factors with thyroid function test abnormalities in a homogenous way using a unique set of prospective cohorts worldwide. Owing to data availability, we were not able to study all known or potentially relevant risk factors. For instance, a family or personal history of thyroid disease and other autoimmune disorders are potentially relevant risk factors to take into account in practice, but these could not be assessed in this study. We were not able to assess the impact of iodine status within a population due to lack of data.
Because of the fixed percentiles used to define reference limits, the prevalence of thyroid dysfunction cannot differ much between populations. As a result, upstream factors such as the effect of iodine deficiency could be masked in our study and results should be interpreted with care. Another relevant pitfall in individual participant data meta-analyses such as this study is the overinterpretation of statistically significant results. We should caution in promptly interpreting the clinical relevance of statistically significant results, which we aimed to communicate in this discussion.
In conclusion, the risk factors assessed in our study were associated with inadequate predictive ability to discriminate women with gestational thyroid dysfunction from euthyroid women, questioning their value in targeted screening. Thyroid antibodies, especially TPOAbs, were associated with a more relevant risk profile for overt and subclinical hypothyroidism, supporting the current recommendations on routine gestational screening in women with known thyroid autoimmunity.
Taken together, the results of this study provide new insights into different risk factors for gestational thyroid dysfunction, which can be considered in the development of clinical guidelines and in medical practice and invite further research to identify risk factors for gestational thyroid dysfunction that would be more effective in targeted screening approaches.
Footnotes
Acknowledgments
The authors would like to gratefully acknowledge all participants, general practitioners, hospitals, and midwives for their important contribution to the establishment of the cohorts and the resulting works.
Authors' Contributions
Conceptualization by A.D., J.A.J.O., T.I.M.K., and Y.L. Data curation and analysis by A.D., J.A.J.O., and Y.L. Cohort establishment and/or management by A.L.-B., A.I., A.P., A.F.-S., A.H., A.A., A.H., B.V., C.De., D.M.C., E.S., E.N.G., E.N.P., E.O., F.-B.T., F.G., F.V., G.A., G.E.P., I.R.-G., J.P.W. J.M.D.-S., J.B., J.Y., K.G.P., K.H., K.H.N., L.B., L.Che., L.Cha., L.M., L.S.-M., M.A.C.B., M.Va., M.R., M.Vr., M.E.D., M.K., M.G., P.N.T., P.V.P., R.K., R.P.P., S.I., S.M.N., S.B., S.J.B., T.G.M.V., T.M., U.F.-R., V.J.M.P., and X.L. Writing original report by A.D., J.A.J.O. (lead), and Y.L. Feedback on proposal, results and/or article by A.L.-B., A.I., A.P., A.F.-S., A.H., A.A., A.H., B.V., C.De., D.M.C., E.S., E.N.G., E.N.P., E.O., F.-B.T., F.G., F.V., G.A., G.E.P., I.R.-G., J.P.W., J.M.D.-S., J.B., J.Y., K.G.P., K.H., K.H.N., L.B., L.Che., L.Chat., L.M., L.S.-M., M.A.C.B., M.Va., M.R., M.Vr., M.E.D., M.K., M.G., P.N.T., P.V.P., R.K., R.P.P., S.I., S.M.N., S.B., S.J.B., T.G.M.V., T.M., U.F.-R., V.J.M.P., X.L., T.I.M.K., C.T.N., C.Do., W.E.V., E.K.A., G.B., H.G., J.L.E., K.B., ![]() ., L.F.M.-W., R.D.-S., S.M., S.Y.L., and Z.S. Supervision and oversight by T.I.M.K. and A.D.
., L.F.M.-W., R.D.-S., S.M., S.Y.L., and Z.S. Supervision and oversight by T.I.M.K. and A.D.
Disclaimer
The individuals involved in setting up the call for proposal and the funding were not involved in the design, data collection, analyses, writing, or review of this study.
Author Disclosure Statement
P.N.T. declares personal consulting fees from Immunovant and leadership roles in the Society for Endocrinology and British Thyroid Association. E.O. reports grants from the National Institutes of Health. E.N.G. received speaker's fees and payment for expert testimony from Merck and consulting fees from Brunel Rus. T.G.M.V. reports grants from the Netherlands Organization for Health Research and Development. E.K.A. reports consultancy with Roche Diagnostics. L. Chaker received travel support by Pfizer. S.M.N. has received consultancy, speakers' fees, or travel support from Access Fertility, Beckman Coulter, Ferring Pharmaceuticals, Merck, Modern Fertility, Roche Diagnostics, and The Fertility Partnership. S.M.N. also reports payments for medical–legal work and investment in The Fertility Partnership. T.I.M.K. reports lectureship fees from Berlin-Chemie, Goodlife Healthcare, Institut Biochimique SA, Merck, and Quidel. U.F.R.'s research salary was sponsored by an unrestricted grant from Kirsten and Freddy Johansen's Fund and reports lecture fee from Merck, Darmstadt. S.B.'s research salary was sponsored by the Capital Region of Denmark's Research Foundation and the Novo Nordisk Foundation (ID 0077221). S.B. received a lecture fee from Merck and Novo Nordisk. M.G. was funded by a Miguel Servet II fellowship (CPII18/00018) awarded by the Spanish Institute of Health Carlos III. J.M.D.-S. is funded by Generalitat Valenciana–Regional Ministry of Education, Research, Culture and Sport under the Talented Researcher Support Programme–Plan GenT (CIDEGENT/2019/064). S.Y.L. is supported in part by grants from the National Institute of Health (5K23ES028736) received honorarium for lecture from the National Dairy Council. K.G.P. received lecture fees from the Berlin-Chemie AG and Merck company. L.B. is supported in part by an MSK Core grant (P30 CA008748). E.N.P. reports honoraria for speaking at Merck China Symposium and for speaking on behalf of the National Dairy Council. E.N.P. is Management Council Member for the Iodine Global Network. All other authors declare no competing interests.
Funding Information
This study was co-funded by a grant of the American Thyroid Association (Request for Proposals [Competitive Grant Program]: Examining Risks Factors of Thyroid Dysfunction in Pregnancy). This study was also funded by the Netherlands Organization for Scientific Research (grant 401.16.020) and additional local funding from participating cohorts.
Supplementary Material
Supplementary Data S1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Figure S8
Supplementary Figure S9
Supplementary Figure S10
Supplementary Figure S11
Supplementary Figure S12
Supplementary Figure S13
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
Supplementary Table S10
Supplementary Table S11
Supplementary Table S12
Supplementary Table S13
Supplementary Table S14
Supplementary Table S15
Supplementary Table S16
Supplementary Appendix SA1