
Abstract
Background:
Desiccated thyroid extract (DTE) is no longer recommended for the treatment of hypothyroidism but is still in use. This review aimed to summarize the available literature on treatment with DTE in adult patients with hypothyroidism.
Methods:
The search was conducted up until January 6, 2024, in six electronic databases. Two reviewers independently screened all the search results. The retrieved studies compared DTE treatment with levothyroxine or combination therapy with liothyronine and levothyroxine. The primary outcome was quality of life (QoL), and the secondary outcomes included symptoms, treatment preference, adverse effects, thyroid hormone levels, thyroid autoantibodies, cardiovascular measures, and gene polymorphisms in deiodinase enzymes.
Results:
In the qualitative synthesis, we included nine nonrandomized studies of interventions (NRSIs), two randomized clinical trials (RCTs), and three case reports. The overall quality of evidence was moderate to very low for the various outcomes. The RCTs found no difference between treatments regarding QoL and symptom score assessments. In the NRSIs, symptom and QoL assessments were in favor of DTE. The included studies indicated that DTE may cause an increase in heart rate, lower body weight, and lower high-density lipoprotein compared with other treatment regimens, but results were conflicting.
Conclusions:
Most studies of DTE treatment are hampered by an inferior design, and data on long-term effects and side effects are lacking. Two RCTs could not demonstrate any difference in QoL or symptom scores when comparing DTE with other thyroid hormone substitutions. Future trials of DTE in patients with hypothyroidism should be based on adequate study designs, validated measures of QoL, patients with reduced QoL, and the assessment of biomarkers reflecting long-term adverse effects.
Introduction
Desiccated thyroid extract (DTE), derived from the porcine or bovine thyroid gland, was the standard therapy for hypothyroidism until the mid-1970s, 1 but is no longer recommended by guidelines worldwide. 2 The primary concern of DTE is the high content of triiodothyronine (T3), compared with the human thyroid, which potentially leads to transient thyrotoxicosis. This may harm bone tissue and the cardiovascular system. 3 –7 A possible association between a high T3 level and breast cancer has also been described, but the evidence is conflicting. 8 –10
Even though levothyroxine (LT4) was introduced in 1949, it took some time before it became the first choice of therapy for hypothyroidism. 11 Despite a normal thyrotropin (TSH) level on LT4 treatment, 10–15% of the patients have impaired quality of life (QoL) when compared with the background population. 12 –14 It is debated whether this is caused by insufficient amounts of T3 in the tissues due to an inadequate conversion of thyroxine (T4) by deiodinases. 15
Despite concerns about drugs containing T3, many patients request DTE treatment, incited by ongoing debates on social media. 16 Even though there has been renewed interest in DTE, only 0–5% of the European endocrinologists prescribe DTE to their patients. 17 –22 Still, there are exceptions, as 17% of Swedish and 13% of Irish endocrinologists are more prone to prescribe DTE. 23,24 In this systematic review, we aimed to summarize the possible benefits and adverse effects of DTE treatment.
Materials and Methods
The study protocol, developed in line with the PRISMA-P statement, 25 was registered in the International Prospective Register of Systematic Reviews (PROSPERO), and was published on July 5, 2020 (ID: CRD42020185456). 26
Eligibility criteria
We wanted to identify available literature concerning the association between treatment with DTE in patients with hypothyroidism of age ≥18 years and various outcomes of interest. The primary outcome was the overall QoL, self-rated or assessed by a questionnaire instrument. Secondary outcomes were cognitive function, anthropometric measures, level of fatigue, thyroid hormone levels, adverse effects or events, patient preference for treatment, surrogate markers (e.g., biomarkers of bone metabolism and the cardiovascular system), interactions with gene polymorphisms, or any other relevant outcome reported in the related studies. The comparator was other thyroid hormone substitutions, placebo, or no treatment.
The TSH radioimmunoassay was developed in the early 1970s. Until then, various methods were used to diagnose hypothyroidism, including evaluation of symptoms, serum protein–bound iodine levels, and basal metabolic rate. 27 These methods are much less reliable than the assessment of TSH for diagnosing and monitoring patients with hypothyroidism. 27,28 Therefore, an additional eligibility criterion was added during the screening process, in that studies had to employ TSH in the clinical management of the patients. This led to the exclusion of 24 studies/case reports conducted >50 years ago (Supplementary Data S2: categorized as “Wrong method for diagnosis” in reason for exclusion). 27
Search
The search was conducted up until January 6, 2024, by the first author K.R.R. in the electronic databases CINAHL (EBSCO), Scopus, “Cochrane central register of controlled trials” (CENTRAL), and “Cochrane Database of Systematic Reviews” (CDSR) via Cochrane library, Embase Classic + Embase via Ovid, MEDLINE, and Epub Ahead of Print and In-Process, and other nonindexed citations via Ovid, without time restrictions. The search strategy was developed in collaboration with a research librarian at the University Library of Southern Denmark. We used medical subject headings (MeSH), CINAHL subject headings, Embase subject headings (Emtree), and text words related to our eligibility criteria. The complete search strategy is compiled in Supplementary Data S1.
Reference lists of reviews, guidelines, and meta-analyses found in the full-text screening were hand-searched for relevant references. A citation search from the included studies was conducted in Scopus. OpenGrey.eu and Clinicaltrials.gov were searched for unpublished literature.
Study selection
All records from the search were assessed and organized as references in the open-access software program Mendeley Desktop (version 1.19.8, Mendeley Ltd., London, United Kingdom). Duplicates were removed, and the remaining references were imported to the Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia; Available at www.covidence.org). Covidence removed additional duplicates and was used independently by two authors (K.R.R. and C.B.L.) for the title and abstract screening according to the eligibility criteria. The full text of potentially eligible references was retrieved, and both authors read and evaluated the articles. Any disagreement was discussed and solved by consensus with the contribution from author S.J.B., who had the deciding vote.
Randomized controlled trials (RCTs), prospective or retrospective observational studies (cohort and case–control), cross-sectional or longitudinal studies, case reports, and case series were all included. Qualitative, quantitative, and mixed-methods research were included. Nonoriginal studies, including editorials, letters to the editor, textbook chapters, and guidelines, were excluded. Only publications in English were included. The authors of conference abstracts were requested a full report, which was included if it met the eligibility criteria. The conference abstract was excluded if a full study report was not accessible or the author did not respond.
Data collection
For all included studies, characteristics (e.g., year of publication, sample size, study design, setting, intervention, outcome, and conflict of interest), demographic data of the participants (e.g., age, sex, and etiology of hypothyroidism), and results were extracted and compiled in tables. Data extraction was done twice by the first author. Results are presented as numbers and percentages for categorical data and mean with standard deviations or median with range for continuous data, as appropriate. Some results are presented narratively.
Quality assessment
The risk of bias for each study was evaluated by two authors (K.R.R. and C.B.L.). Judgment between the authors was cross-checked, and a consensus was reached if there were any disagreements.
The methodological quality of each nonrandomized study of intervention (NRSI) was assessed using the risk-of-bias assessment tool “Risk Of Bias In Non-randomized Studies of Interventions” (ROBINS-I). 29 The risk-of-bias assessment tool revised Cochrane risk-of-bias tool for randomized trials (RoB 2.0) was used for RCTs. 30 The authors were contacted if a study protocol or statistical analysis plan was unavailable. The overall quality of evidence was assessed using the “Grading of Recommendation, Assessment, Development, and Evaluation” (GRADE) approach. 31
Meta-analysis
A meta-analysis of the included RCTs was conducted using the inverse-variance approach with fixed effects. Statistical heterogeneity was evaluated with visual inspection of the forest plots, chi-square tests, and I 2-statistics. The meta-analyses were performed using Stata software (V17.0; StataCorp, College Station, TX, USA). Because fewer than ten studies complied with the inclusion criteria for each outcome, we did not conduct a funnel plot to assess small-study effects.
Results
Literature search
Figure 1 illustrates the literature search and study selection process. The full-text screening led to the exclusion of 146 articles (Supplementary Data S2). In total, fourteen articles met the inclusion criteria, here among two RCTs, nine NRSIs, and three case reports. 32 –45
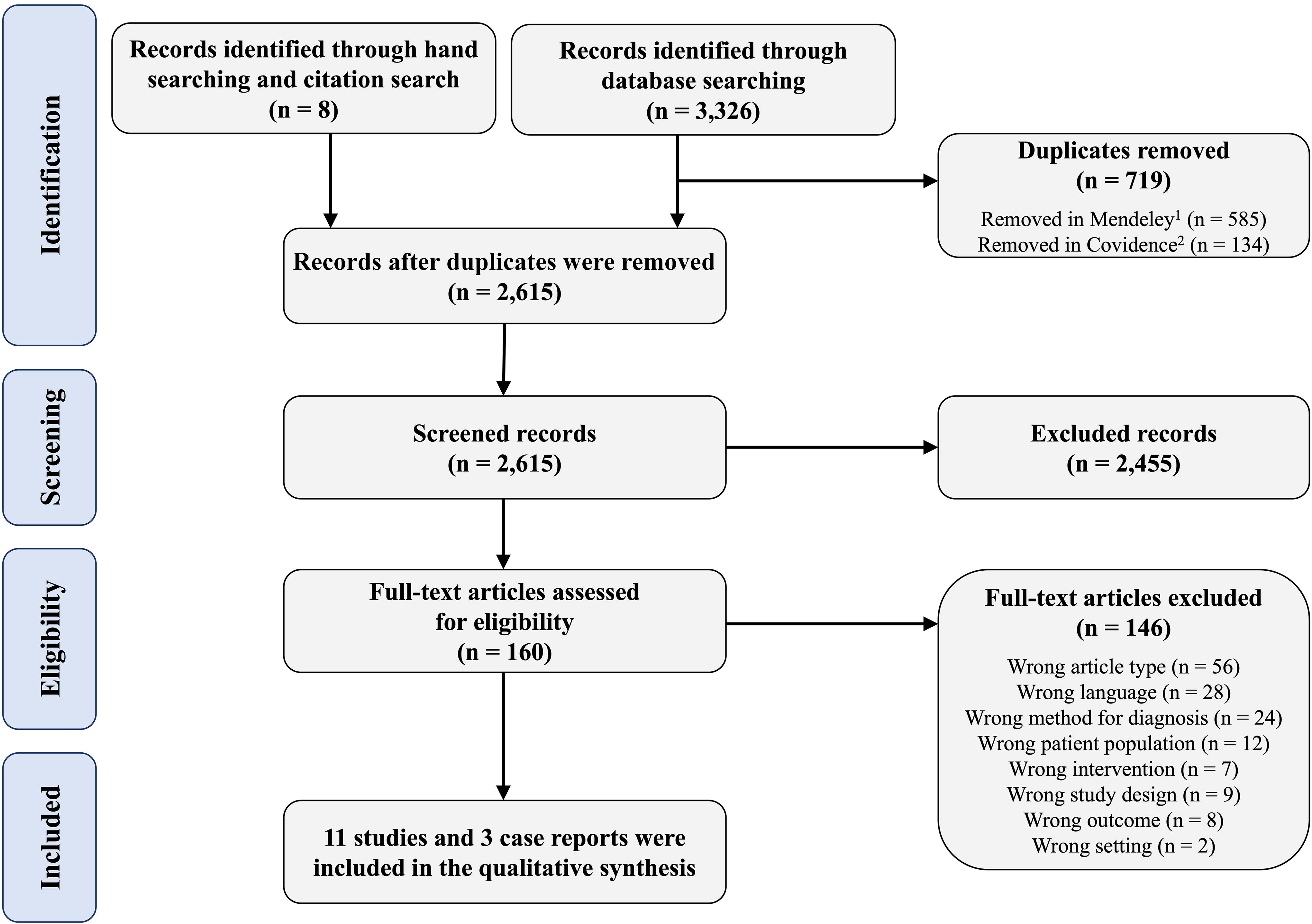
PRISMA flow diagram illustrating the search and screening process for the review “potential risks and benefits of desiccated thyroid extract for the treatment of hypothyroidism: A systematic review.” 1Mendeley Desktop (version 1.19.4, Mendeley Ltd., London, United Kingdom). 2Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia).
Study characteristics
The detailed characteristics of the included studies and baseline descriptions of the study participants are compiled in Tables 1 and 2, respectively. In six studies, DTE was compared with LT4 monotherapy, 32,34,35,43 –45 while one study compared DTE with either LT4 monotherapy or no treatment. 36 The remaining studies (case reports not considered) compared three treatment regimens, that is, DTE, LT4 monotherapy, and LT4 and liothyronine (LT3) combination therapy. 33,37 –39 Most studies used Armour thyroid tablets, one study used both Armour and ERFA, and one study used Thyranon (Table 2). 32 –36,38,43,45 Three studies did not describe the type of DTE used, besides that it was “prescribed” DTE (Table 2). 37,39,44
Study Characteristics
89 participants were LT4 treated and 832 were untreated at baseline, of whom 40 and 278, respectively, had follow-up.
35 patients were offered DTE, of whom 4 refused and 3 discontinued DTE.
78 were enrolled, 70 completed the study.
Medication was adjusted after six weeks aiming at TSH in the range of 0.5–3.0 μIU/L; hereafter patients continued the medication for an additional 12 weeks.
435 DTE treated and 435 LT4 treated.
Seven received DTE and 6 received LT4.
5106 received LT4, 252 received DTE, and 79 received LT4/LT3 combination therapy.
450 undergoing LT4 treatment were screened, 154 were switched to DTE because of failure to achieve clinical euthyroidism. Four patients were excluded from the TSH, TT4, and TT3 analyses due to post-thyroid cancer therapy or suppressive treatment for thyroid nodular disease.
90 were enrolled, 75 completed the study.
100 patients included initially, 60 patients received DTE (3 were excluded), and 40 received LT4/LT3 combination therapy (3 were excluded); 51 patients receiving DTE completed the cross-sectional study with SF-20.
BDI, beck depression inventory; BMI, body mass index; DTE, desiccated thyroid extract; EuroQoL EQ-5D-5L, european quality of life 5 dimension 5-level; EQ-VAS, european quality of life visual analog scale; fT3, free triiodothyronine; fT4, free thyroxine; GHQ-12, general health questionnaire; IQR, interquartile range; LT3, liothyronine; LT4, levothyroxine; NI, no information; SF-20, medical outcomes study short form-20 questionnaire; TgAb, thyroglobulin antibodies; ThyPRO-39, thyroid-related patient-reported outcome; TPOAb, thyroid peroxidase antibody; TSH, thyrotropin; TSQ-36, thyroid symptom questionnaire; TT4, total T4; TT3, total T3; T4, thyroxine; T3, triiodothyronine; WMS-IV, wechsler memory scale fourth version.
Baseline Demographic Characteristics of the Participants and Thyroid Supplement Dose in the Included Nonrandomized and Randomized Clinical Trials
Participants were divided into group 1 (receiving LT4 at baseline), 40 patients, and group 2 (untreated at baseline), 278 patients; in all, 318 patients received DTE (content: 23 µg triiodothyronine, 100 µg thyroxine).
Twelve patients had subtotal thyroidectomy due to thyrotoxicosis, nontoxic goiter, or AIT, and three had a total thyroidectomy due to thyroid cancer.
Four patients had unknown etiology, one had Schmidt’s syndrome, and three had congenital hypothyroidism.
Total thyroidectomy due to toxic goiter.
Two patients were taking DTE at inclusion (75 and 100 mg/day, respectively).
DTE content: 65 mg provides 38 µg/day thyroxine and 9 µg/day triiodothyronine.
The DTE and LT4 groups were matched on age, sex, and ethnicity.
Exclusion criteria: previous radioiodine therapy, panhypopituitarism, pregnancy, previous thyroid cancer, Graves’ disease, autoimmune thyroiditis, and prescription of more than one thyroid supplement.
No information about number of patients in each treatment category.
Content of T4:T3 ratio is 4:1.
AIT, autoimmune thyroiditis; DTE, desiccated thyroid extract; LT4, levothyroxine; LT3, liothyronine; n, number; NI, no information; RAI, radioactive iodine; SD, standard deviation.
Four studies evaluated QoL using various tools. 32,33,35,37 Other outcomes included symptoms of hypothyroidism, symptoms of depression, thyroid function measures, treatment preference, body weight, adverse effects, lipid profile, heart rate, and blood pressure. Gene variants in relation to symptoms and the response to treatment were investigated in one study. 33
Risk of bias
One NRSI was classified with moderate risk of bias with ROBINS-I, four NRSIs were classified with serious risk of bias, and the remaining four with critical risk of bias (Fig. 2, Supplementary Data S3). Overall, the RCTs were classified with some concern due to a missing protocol or an a priori statistical analysis plan (Fig. 2, Supplementary Data S4).
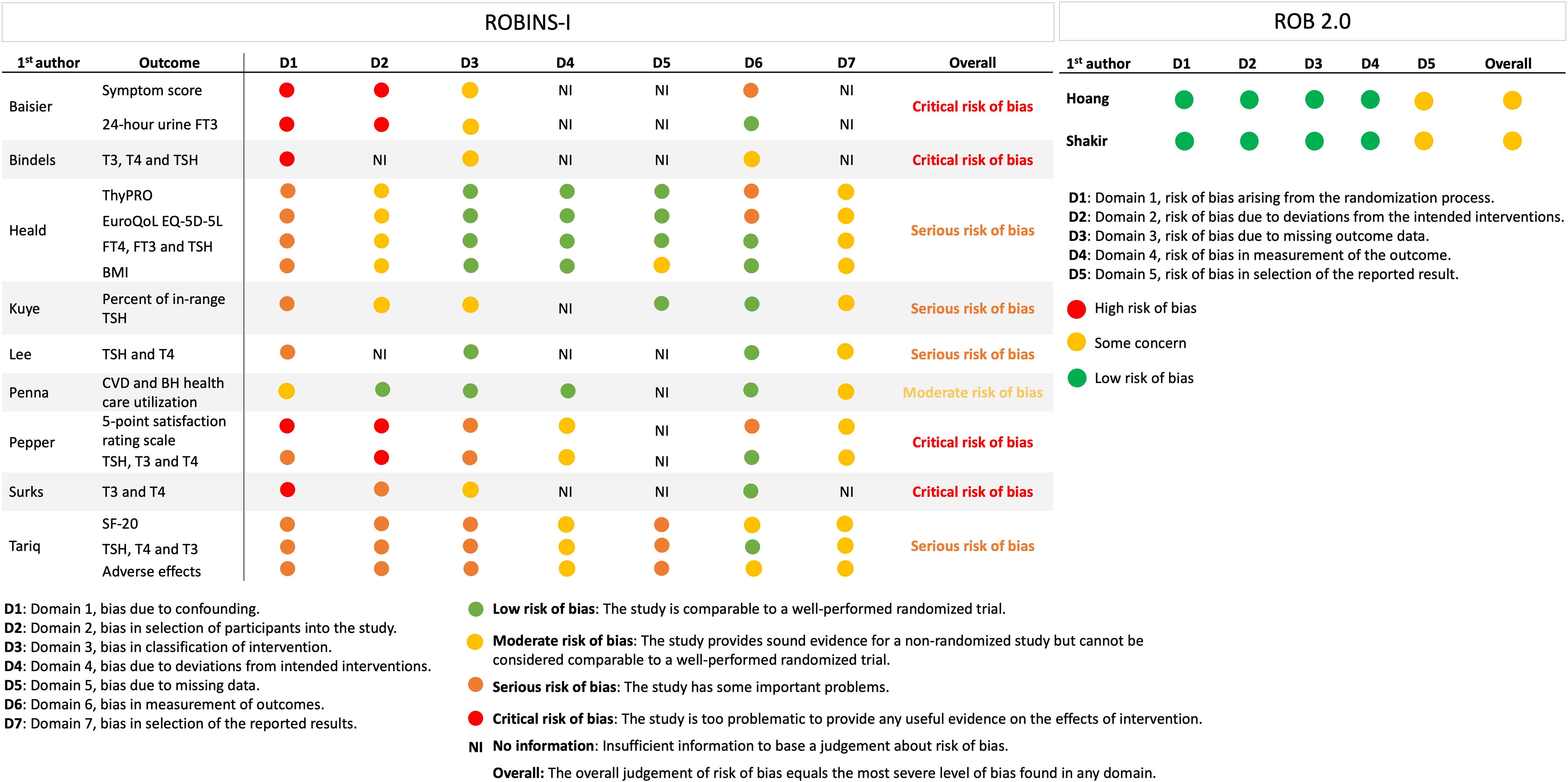
Risk-of-bias assessment in the nonrandomized trials using ROBINS-I (Risk Of Bias In Non-randomized Studies of Interventions) and in the randomized controlled trials using RoB 2.0 (Revised Cochrane risk-of-bias tool for randomized trials). The detailed evaluation with answers to all signaling questions is compiled in Supplementary Data S3 and S4. In RoB 2.0, Domain 5 is judged as “some concerns” in both the randomized controlled trials, as no a priori statistical analysis plan or protocol was available for either study. BH, bone health; BMI, body mass index; CVD, cardiovascular; EuroQoL EQ-5D-5L, European Quality of life 5-dimension 5-level; fT3, free triiodothyronine; fT4, free thyroxine; SF-20, Medical outcomes study short form-20 questionnaire; T3, triiodothyronine; T4, thyroxine; TSH, thyrotropin; ThyPRO, Thyroid-related Patient-Reported Outcome.
Quality of evidence
Including both RCTs and NRSIs in the certainty of evidence assessment, the overall rating was low for the QoL outcome (Supplementary Data S5). Based on the RCTs only, the body of evidence was higher. The certainty of evidence was low also for the secondary outcomes, such as symptom scores and thyroid hormone levels. The certainty of evidence for adverse effects was rated as very low due to the low number of cases and moderate for the cardiovascular surrogate markers.
Quality of life
In the two RCTs, QoL was evaluated with the General Health Questionnaire (GHQ-12), and no difference could be detected between the treatment regimens (Table 3). 32,33 In a fixed-effects meta-analysis, the overall Hedges’ g of GHQ-12 was −0.014 (95% CI: −0.37, 0.09; p = 0.23) when comparing DTE with LT4 treatment (Supplementary Data S6). The heterogeneity was estimated to be low (I 2 = 0%).
Summary Table of the Associations Between Treatment with Desiccated Thyroid Extract and Quality of Life, General Health, and Symptom Scores
Evaluates eight symptoms with a score from 0 to 2; 0 is no symptoms and 2 is full presence of symptoms.
Five dimensions of health: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Five levels can be chosen within each health dimension: no problems to extreme problems.
Utility scores: representing a preference-weighted measure of patients’ health evaluation from the EQ-5D-5L dimensions, a lower score signifies poorer perceived health.
EQ-VAS scale: self-rated score, 100 is “the best imaginable health state” and 0 represents “the worst imaginable health state.”
hyPRO-39 questionnaire, self-administered and measures QoL within 39 items (scores of 0–100); increasing scores indicate decreasing QoL.
Self-developed TSQ: 12 questions, higher scores indicate more symptoms.
BDI: self-rating scale of 21 items, scores of ≤10 indicate normal mood variation, scores of ≥11 indicate symptoms of depression, and scores of >20 reflect clinical depression.
WMS-IV includes Auditory Memory Index (AMI), Visual Memory Index (VMI), Visual Working Memory Index (VWMI), Immediate Memory Index (IMI), and Delayed Memory Index (DMI).
SF-20 is available at https://www.rand.org/health-care/surveys_tools/mos/20-item-short-form/survey-instrument.html. SF-20 was not tested in patients receiving LT4, and there is no preintervention data for comparison.
BDI: beck depression inventory; DTE, desiccated thyroid extract; EuroQoL EQ-5D-5L, european quality of life 5-dimension 5-level; EQ-VAS, european quality of life visual analog scale; GHQ-12, general health quality of life questionnaire; LT4, levothyroxine; n, number; ns, nonsignificant; QoL, quality of life; SF-20, medical outcomes study short form-20 questionnaire; ThyPRO, thyroid-related patient-reported outcome; TSQ-36, thyroid symptom questionnaire; WMS-IV: wechsler memory scale fourth version.
In consecutive case series, Heald et al. evaluated QoL with both the Thyroid-related Patient-Reported Outcome (ThyPRO-39) and the European Quality of Life 5-Dimension 5-Level questionnaire (EuroQoL EQ-5D-5L). 35 Both tools showed an improvement in QoL from baseline (treatment with LT4) to six months after initiating DTE (Table 3). For ThyPRO-39, all domains and the composite score improved significantly on DTE treatment. The same pattern was seen in the EuroQoL EQ-5D-5L questionnaire (Table 3). 35
Tariq et al. evaluated QoL with the Short Form-20 questionnaire (SF-20) (Table 3). 37 Most patients (92%) indicated that their self-health was excellent, very good, or good after initiating DTE compared with LT4. In addition, most of the participants (92.7%) claimed to have improved QoL after a switch of treatment to DTE. 37
Symptom score
In the study by Baisier et al., a self-developed hypothyroid symptom score tool was applied. 36 Patients unresponsive to LT4 or being treatment-naïve were all treated with DTE. The study did not compare the symptom score before and after treatment with DTE, but, nevertheless, the authors concluded that the mean symptom score declined in both groups following DTE treatment (Table 3). The primary outcome of the study by Tariq et al. was clinical signs and symptoms of hypothyroidism following DTE treatment, but these results were, for unknown reasons, not reported in the article. 37
In the two-armed RCT by Hoang et al., symptoms were evaluated with TSQ-36 (Thyroid-Symptom Questionnaire), and there were no differences between DTE and LT4 monotherapy. 32 The three-armed RCT by Shakir et al. also used TSQ-36 and found no difference in symptoms between DTE, LT4, and LT4/LT3 (Table 3). 33 In addition, the Beck Depression Inventory (BDI) and Wechsler Memory Scale (WMS) were evaluated in these two RCTs, without finding any difference between treatments (Table 3). In fixed-effects meta-analyses of TSQ-36, BDI, and Wechsler’s memory indices, there were no differences comparing DTE and LT4 treatment (Supplementary Data S6), and the heterogeneity was low in all outcomes (I 2 = 0%).
Thyroid hormone levels
Three studies found no difference in TSH between DTE and other treatment regimens, 34,43,45 two studies found a significantly higher TSH, 32,33 and one found a significantly lower TSH on DTE compared with LT4 treatment (Table 4). 44 One study found DTE superior to LT4 in maintaining plasma TSH within the reference range. 37
Association Between the Treatment of Hypothyroidism with Desiccated Thyroid Extract and Thyroid Hormone Levels
No statistical methods used to compare groups.
TSH reference range: <4.0 mIU/L (lower detection limit was 0.6 mIU/L, i.e., the method could not distinguish between euthyroidism and thyrotoxicosis). T3 reference range: 1.5–3.1 nmol/L. T4 reference range: 80–180 nmol/L.
TSH reference range: 0.35–5.50 mIU/L. fT3 reference range: 3.5–6.5 pmol/L. fT4 reference range: 8.3–30.0 pmol/L.
TSH reference range: 0.27–4.20 mIU/L. TT3 reference range: 60–181 ng/dL. TT4 reference range: 4.5–12 µg/dL. fT4 reference range: 0.89–1.76 ng/dL.
TSH reference range: 0.32–5.5 mIU/L.
No reference range is specified in the article.
TSH reference range: 0.4–4.0 mIU/L. Reference range was not specified for T4 and T3.
p-value reports the results of a linear mixed-effects model evaluation of the fixed effect of the three treatment regimes, using participants as a random effect. TSH reference range: 0.27–4.20 mIU/L. TT3 reference range: 60–181 ng/dL. TT4 reference range: 4.5–12 µg/dL. fT4 reference range: 0.89–1.76 ng/dL. T4:T3 ratio reference range: 22.7–150.
DTE was administered to three patients: two received 120 mg DTE, and one received 60 mg DTE. Serum was obtained at intervals of 1–2 hours throughout the day. No p-values are given.
Mean TSH, fT3, and fT4 values are presented during DTE and LT4 therapy but without comparing regimens. TSH reference range: 0.35–5.5 mIU/L. Patients with an abnormally low TSH had previous thyroid cancer. Thyroid status was measured in 60 patients receiving LT4 and 57 receiving DTE.
DTE, desiccated thyroid extract; fT3, free triiodothyronine; fT4, free thyroxine; LT4, levothyroxine; TT4, total thyroxine; TT3, total triiodothyronine.
In the study by Baisier et al., 24-hour urine excretion of T3 was higher during DTE treatment compared with LT4 or no treatment. 36 Likewise, several studies found higher serum/plasma T3 levels on DTE treatment compared with LT4. 32 –34,45 In the study by Tariq et al., DTE was better than LT4 in maintaining fT3 within the reference range, in line with the finding for TSH. 37 Finally, Surks et al. investigated, in three patients, changes in plasma T3 after ingestion of DTE; in two participants, plasma T3 increased by 100%, while one patient showed no change. 38
Plasma T4 (measured as free T4, total T4, or free T4 index) was lower on DTE than on LT4 treatment in all studies evaluating thyroid function measures (Table 4). Surks et al. demonstrated that plasma T4 was stable throughout 24 hours on DTE treatment. 38 Furthermore, in the study by Tariq et al., plasma T4 was within target to the same extent when comparing DTE and LT4 treatment. 37
Lee et al. found small fluctuations in plasma levels of thyroid peroxidase and thyroglobulin antibodies when treated with DTE or LT4, but without any difference between the two treatment regimens. 43 No other studies included data on thyroid autoantibodies.
Cardiovascular markers and anthropometric measures
The effect on lipids was evaluated only in the two RCTs, with slightly different results. 32,33 In the two-armed RCT, high-density lipoprotein (HDL) was significantly lower in DTE-treated patients compared with those receiving LT4 (Table 5), while Shakir et al. found no difference. 32,33 In both RCTs, low-density lipoprotein (LDL), total cholesterol, and triglyceride levels were unaffected by the type of treatment (Table 5). 32,33 In a fixed-effects meta-analysis comparing DTE with LT4, the overall Hedges’ g of triglyceride was −0.02 (95% CI: −0.25, 0.21; p = 0.84), for LDL −0.08 (95% CI: −0.31, 0.15; p = 0.48), for total cholesterol −0.05 (95% CI: −0.28, 0.18; p = 0.65), and for HDL −0.05 (95% CI: −0.28, 0.18; p = 0.69) (Supplementary Data S6). The heterogeneity was low in all outcomes (I 2 = 0%) (Supplementary Data S6).
Association Between Treating Hypothyroidism with Desiccated Thyroid Extract and Body Mass Index, Body Weight, Lipid Profile, Heart Rate, and Blood Pressure
In 17 participants, BMI was measured when initiating DTE and at their last follow-up visit.
Converted from pounds to kilograms (kg).
Normal range > 40 mg/dL.
BMI, body mass index; DTE, desiccated thyroid extract; HDL, high-density lipoprotein; LDL, low-density lipoprotein; LT4, levothyroxine; LT3, liothyronine; min, minute.
Regarding body weight, neither Heald et al. nor Pepper et al. found any difference in mean body mass index before and after treatment with DTE (Table 5). 35,45 The two RCTs showed divergent results, as Hoang et al. found a significant decrease of 1.3 kg (p < 0.0001) in body weight during treatment with DTE, compared with LT4, while Shakir et al. found neutral effects (Table 5). 32,33 In a fixed-effects meta-analysis, there was no difference in body weight when comparing DTE with LT4 (p = 0.67), and the heterogeneity was low (I 2 = 0%) (Supplementary Data S6).
In the RCT by Shakir et al., patients had an increased heart rate when treated with DTE, compared with LT4 and LT4/LT3 (p = 0.04). 33 In contrast, the heart rate was unaffected by type of treatment in the other RCT by Hoang et al. (Table 5, Supplementary Data S6). 32 None of the RCTs found any association between blood pressure and treatment regimen, and the meta-analysis showed no difference comparing DTE with LT4 treatment (Table 5, Supplementary Data S6). 32,33
Adverse events
Adverse effect was an outcome in the study by Tariq et al. 37 One patient discontinued DTE due to mild hyperthyroid symptoms. No participants were hospitalized for adverse events or arrhythmias, but 6.7% of the patients (whether treated with DTE or LT4/LT3) complained of palpitations. All these individuals had a plasma TSH level <0.35 μIU/L. In the study by Penna et al., 39 fewer patients treated with DTE (2.8%) or LT4/LT3 (5.8%), compared with LT4 (7.7%), had outpatient visits associated with cardiovascular or bone disease (p = 0.023), but the difference was insignificant when adjusted for sociodemographic and clinical covariates. There was no difference in emergency or hospital visits. 39
Five other articles reported adverse effects but not as a prespecified outcome. 32,33,35,43,45 In the study by Heald et al., two participants discontinued DTE due to palpitations but without abnormalities on ECG. 35 In the study by Pepper et al., three patients on DTE had complaints of itchiness of the eyelids, scalp hair loss, and palpitations, respectively. 45 Lee et al., Shakir et al., and Hoang et al. did not observe any adverse events among their participants. 32,33,43
The three included case reports also described adverse effects due to over-the-counter bovine thyroid supplementations or high-dose DTE treatment, respectively (Table S1). 40 –42 These adverse effects were all due to iatrogenic thyrotoxicosis and included atrial fibrillation, weight loss, tachycardia, and myocardial infarction (Table S1). 40 –42
Treatment preference
In the RCT by Hoang et al., 34 patients (48.6%) preferred DTE, 13 (18.6%) preferred LT4, and 23 (32.9%) had no preference. 32 Preference for DTE over LT4 was statistically significant (p = 0.002). In the RCT by Shakir et al., no difference was found in preference among the three treatment regimens, that is, DTE, LT4, and LT4/LT3. 33
In the unblinded study by Pepper et al., a five-point satisfaction rating scale (SRS) was used to evaluate treatment preference between LT4 and DTE. The scale ranged from 5 points (“DTE definitely superior to LT4”) to 1 point (“DTE definitely worse than LT4”). 45 Of the 154 DTE-treated patients, 117 patients (78%) indicated an SRS score >3 (responders), while 33 patients (22%) indicated a score ≤3 (nonresponders) (p < 0.001). 45
Gene polymorphism
The participants in the study by Shakir et al. were examined for DIO2 polymorphism, that is, the Ala92-DIO2 and Thr92-DIO2 variants. 33 Of 75 participants, 41 were heterozygotes, while 9 and 25 individuals were monozygotic for the Ala92-DIO2 and Thr92-DIO2 variants, respectively. The authors found no difference in the evaluated outcomes, that is, GHQ-12, TSQ-36, BDI, and WMS-IV, when the gene variants were considered. 33
Discussion
In this systematic review, there was a dearth of high-quality studies. We chose to include all types of studies, realizing that the published reports on DTE treatment in hypothyroid adults were limited. Despite this broad search strategy, only 11 studies and 3 case reports were included, here among two blinded RCTs. These latter two trials were generally well-conducted, only judged with some concerns due to the lack of an a priori statistical plan.
Different doses of DTE, nonstandardized treatment regimens, various DTE preparations and brands, and patient selection are all factors that complicate comparison across studies. It is reported that a DTE dose of 80 mg on average should restore clinical and biochemical euthyroidism. 47 However, the participants received DTE doses in the range of 200–233 mg in one NRSI, while only 30 mg DTE per day was given in another study. 36,37 These huge differences may reflect that some patients were over- or undertreated, respectively, or that the participants’ thyroid functional reserve differed between studies. In fact, information on the proportion of subclinical and overt hypothyroid patients is not provided in virtually any of the studies.
Quality-of-life and symptom scores
In the two RCTs, no difference in QoL or symptom scores was found by comparing a DTE regimen with either LT4 or LT4/LT3 combination therapy. 32,33 On the contrary, in the NRSIs by Heald et al. and Tariq et al., QoL as well as symptom scores improved significantly when patients were switched from LT4 monotherapy to DTE because of persistent symptoms. 35,37 The discrepancy in outcome between the RCTs and the NRSIs is most likely caused by the nonblinded design of the latter studies. Indeed, patients with hypothyroidism are highly susceptible to the placebo effect, as demonstrated in the recent RCT of the effect of selenium supplementation. 49
Various tools for assessment of QoL were used, which makes comparison across studies difficult. The GHQ-12, used in both RCTs, has been extensively validated in different settings, but not in thyroid patients, to the best of our knowledge. 46,50 The same reservation goes for SF-20 used by Tariq et al. 37,48 The ThyPRO, used by Heald et al., has been developed and validated specifically for patients with benign thyroid disease, and this tool seems the obvious choice for estimating the QoL in future studies of this patient group. 35,51,52
Thyroid hormone levels
Since T3 has a short half-life, multiple daily dosing is required to restore a near-normal diurnal serum profile of T3. In most studies included in the present review, the patients were given DTE only once daily. Nevertheless, serum T3 in patients treated with DTE largely remained within the normal range, even though at a higher level when compared with LT4 monotherapy. The levels of TSH also remained within the normal range but were more fluctuating during DTE therapy. Kuye et al. showed no difference between DTE and LT4 treatment in TSH values within range over a three-year period. 44 In contrast to other studies, Kuye et al. adjusted for a range of potential confounders. However, for unknown reasons, patients with Hashimoto’s thyroiditis were excluded in that study. 44
Adverse effects
Long-term studies of patients treated with DTE are lacking. Regarding short-term adverse effects, DTE—compared with treatment with LT4—seems to carry a higher risk of cardiac events and symptoms of thyrotoxicosis. However, the overall level of evidence was judged as very low in line with other outcomes of this review. It is most likely that the majority of adverse effects seen with DTE therapy are caused by iatrogenic thyrotoxicosis, which also is the perception among physicians and patients. 53,54 However, transient iatrogenic and supraphysiological levels of T3 during DTE treatment may raise concern. Guidelines advocate for the normalization of TSH serum levels, as TSH outside the normal range is associated with increased risk of cardiac events and mortality. 3 A similar recommendation does not exist for T3, even though increased levels of T3 have been linked to cancer development and cardiovascular events. 3,6,8 Importantly, as serum T3 shows diurnal variations in patients on LT3 treatment, T3 levels that periodically exceed the upper reference limit may remain undetected by the conventional biochemical monitoring. 55 Therefore, blood sampling for measurement of serum T3 should be standardized to be clinically useful. The same applies to future long-term studies of patients treated with DTE.
Treatment preference
According to an online survey, patients treated with DTE claimed higher treatment satisfaction compared with other treatment regimens. 56 Such a result is without a doubt under the major influence from selection bias. Significantly more patients preferred DTE to LT4 in the RCT by Hoang et al., 32 but the preference for DTE was not significant compared with patients who indicated “no preference.” In the RCT by Shakir et al., no preference was found overall, but when dividing the participants according to severity of symptoms on LT4 treatment, the most symptomatic participants seemed to prefer DTE or LT4/LT3. 33,57 Several theories have been proposed as to why some patients prefer DTE to LT4. Involved factors may include enhanced well-being from transient thyrotoxicosis, or postulated positive effects of other ingredients in DTE, for example, 3,5-diiodothyronine and calcitonin. 58
DIO2 gene polymorphisms
The presence of the Thr92Ala gene variant in the DIO2 gene may result in reduced conversion of T4 into T3 in athyreotic patients on LT4, potentially leading to reduced levels of T3 in certain tissues, such as the brain. 59 Indeed, previous studies have indicated that individuals with the Thr92Ala gene variant are those who benefit most from the LT4/LT3 combination therapy. 60,61 Only one study investigated whether improvement in QoL depended on the presence of this gene variant, but no such association was demonstrated. 33
Strengths and limitations
We used a systematic approach and did a comprehensive literature search in several databases. The quality assessment of the included studies was done with appropriate tools. We judged some older studies outdated and unsuitable for the present review due to unreliable methods for diagnostics and monitoring. In addition, before 1985, the amount of thyroid hormone in DTE was estimated by measuring the iodine content, with the result that tablets across batches had various potency, and some were even devoid of any active ingredient. 47,62 Nevertheless, some of the studies we decided to exclude have been well cited in the past and made up the cornerstones in previous evidence supporting the use of DTE.
Future perspectives
There is an ongoing debate about the mechanisms behind the persistent symptoms in some patients on LT4, and how these individuals should be treated and managed. 12,56 In future studies, preferably in the setting of RCTs, the focus should be on patients with persistent symptoms, low circulating T3 levels, or those with specific DIO2 gene variants. Likewise, the assessment tools for estimating QoL should be well-validated and disease-specific.
Considering the short half-life of T3, future studies should aim to administer DTE at least twice daily to achieve more physiological T3 levels. Due to the potentially negative impact of the high T3 content, it is of crucial importance that future studies of DTE treatment include long-term follow-up of patients to disclose any slow-onset adverse effects. At least, surrogate biomarkers that reflect unintended effects on other organs should be measured.
Until more solid evidence is provided, the management of patients with hypothyroidism with persistent symptoms remains challenging, as some people may rely more on web-based information than on their caretaking physician. 54,56 This increases the risk of overtreatment due to self-adjusted treatment, and over-the-counter thyroid preparations. 16,40 To address this problem, education and information of patients should be encouraged, and the development and validation of different self-management tools and point-of-care devices are also likely to prove very helpful.
Conclusions
This review of DTE treatment in patients with hypothyroidism comprised 14 previous studies, the majority of which suffered from a poor study design. Accordingly, the quality of current evidence on effects and adverse effects of DTE treatment is low. Several studies indicated that patients with persistent symptoms show improvements when treated with DTE, compared with LT4 monotherapy, but the conclusions are hampered by the lack of a control group, and the positive results most likely reflect a placebo effect. Two well-designed blinded RCTs, comparing DTE with LT4 and/or LT4/LT3 combination therapy, were unable to demonstrate any convincing differences in QoL or symptom scores between the treatment regimens.
Footnotes
Acknowledgments
Research librarian Mette B. Eriksen at the University Library of Southern Denmark is acknowledged for her help in developing the search strategy. Librarians at the University Library of Southern Denmark are acknowledged for providing the full text of several screened articles. The Centre for Evidence Based Medicine Odense (CEBMO) is acknowledged for helping with protocol writing and providing guidance on risk-of-bias assessments.
Authors’ Contributions
K.R.R. contributed to the conceptualization, data curation, formal analysis, funding acquisition, investigation (screening of references and risk-of-bias assessment), project administration, software, validation, visualization, and writing (original draft, review & editing). C.B.L. contributed to the investigation (screening of references and risk-of-bias assessment) and writing (review & editing). S.T.B. contributed to conceptualization, funding acquisition, project administration, resources, supervision, validation, and writing (review & editing).
Author Disclosure Statement
K.R.R., C.B.L., and S.J.B. declare no conflicts of interest.
Funding Information
K.R.R. is enrolled as a Ph.D. student at the University of Southern Denmark and has received research grants from the Danish Medicines Agency, the Region of Southern Denmark (Grant number: 20/14658), and a grant from the “Board of Chief Physicians at Odense University Hospital” (Grant number: A4641). C.B.L. is enrolled as a Ph.D. student at the University of Southern Denmark and has received institutional research grants from the University of Southern Denmark and the Region of Southern Denmark.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4
Supplementary Data S5
Supplementary Data S6