
Abstract
Background:
Although childhood exposure to radioactive iodine-131 (I-131) is an established risk factor for thyroid cancer, evidence for an association with thyroid nodules is less clear. The objective of this study is to evaluate the association between childhood I-131 exposure and prevalence of ultrasound-detected thyroid nodules overall and by nodule histology/cytology (neoplastic/suspicious/non-neoplastic), size (<10 mm/≥10 mm), and number (single/multiple).
Methods:
This is a cross-sectional study of radiation dose (mean = 0.53 gray, range: 0.0003–31 gray) and screen-detected thyroid nodules conducted in 1998–2000 (median population age 21.5 years) in a cohort of 13,243 residents of Ukraine who were under 18 years at the time of the Chornobyl accident on April 26, 1986. Excess odds ratios per gray (excess odds ratio [EOR]/Gy) and confidence intervals (CIs) were estimated using logistic regression.
Results:
Among 13,078 eligible individuals, we identified 358 (2.7%) with at least one thyroid nodule. Significantly increased dose–response associations were found for all nodules and nodule groups with doses <5 Gy except individuals with non-neoplastic nodules. Among individuals with doses <5 Gy, the EOR/Gy for neoplastic nodules (5.35; CI: 2.19–15.5) was significantly higher than for non-neoplastic nodules (0.24; CI: 0.07–0.74), but the EOR/Gy did not vary by nodule size or number.
Conclusions:
Childhood exposure to I-131 is associated with an increased risk of thyroid nodules detected 12–14 years following exposure, and the risk for neoplastic nodules is higher than for non-neoplastic nodules. Analyses of incident thyroid nodules may help clarify dose–response patterns by nodule characteristics and provide insights into thyroid nodule etiology.
Introduction
Unlike thyroid cancer, thyroid nodules are fairly common. 1 Prevalence of thyroid nodules depends on the age and sex composition of the population under study and on the method of detection, ranging from 2% to 6% using palpation, 19% to 35% using ultrasound, and up to 65% at autopsy. 2 A strong association between history of thyroid nodules and thyroid cancer has been found in nonirradiated individuals. 2,3 Ionizing radiation exposure during childhood is one of the strongest established risk factors for thyroid cancer 4 and has been associated with thyroid nodules. 5 However, the relationship between exposure to internal radioactive iodine 131 (I-131) and the development of thyroid nodules is not well characterized. 4
Studies of individuals exposed to radioactive I-131 from the 1986 accident at the Chornobyl nuclear power plant during childhood have reported an approximately linear dose–response relationship between I-131 dose and thyroid cancer with statistically significant excess relative risk per Gray (ERR/Gy) varying between 2 and 8. 6 –9 A pooled analysis of studies of individuals exposed to medical or atomic bomb radiation at age <20 years found that the estimated ERR/Gy was 5.5, among the highest radiation risks for any solid cancer. 10 Relative risk estimates with internal I-131 exposure appear to be statistically compatible with those found for external radiation exposure of children. Radiation-related risks of follicular adenoma have also been reported. 11,12
In a cross-sectional study that relied on measurement-based I-131 doses and standardized thyroid screening of adolescents and young adults from Belarus, we found a strong association with I-131 dose from the Chornobyl accident for neoplastic nodules and large (≥10 mm) non-neoplastic thyroid nodules with estimated excess odds ratio (EOR) per Gy of 3.8 and 1.6, respectively. 13 The objective of this study is to evaluate the association between I-131 dose and prevalence of thyroid nodules detected at first screening examination in a cohort from Ukraine.
Methods
Study population and thyroid screening
Details of the study methods have been published previously. 14 Briefly, the cohort includes 13,243 individuals less than 18 years at the time of the accident on April 26, 1986, who resided in three highly contaminated northern Ukrainian oblasts, and had direct thyroid radioactivity measurements taken in May–June 1986 (Supplementary Fig. S1). Between 1998 and 2008, individuals in the cohort underwent four standardized thyroid screening examinations. The first examination conducted between April 1998 and December 2000 was used to ascertain prevalence of thyroid nodules in this cross-sectional study. Institutional review boards of participating organizations in Ukraine and the United States approved this study. Informed consent forms were signed by all participants or their legal guardians.
The study consisted of clinical exams and structured interviews conducted during the same visit. Ultrasonography was performed with a 7.5 MHz ultrasound probe along with palpation of the thyroid. The ultrasonographer recorded detailed information on thyroid size and echostructure, and number and characteristics of thyroid nodules (up to the four largest nodules, if multiple nodules were detected). An independent clinical examination and palpation was conducted by an endocrinologist in all participants. Blood and spot urine samples were collected to measure levels of thyroid hormones and iodine excretion, respectively. Information on medical, smoking, and residential history, demographics, and milk consumption (May and June 1986) were collected through structured interviews. 15 Participants were referred to fine-needle aspiration biopsy (FNAB) if they had a nodule larger than 10 mm, 5–10 mm that was at least partly solid and the nodule had signs suggesting malignancy (i.e., hypoechoic, indistinct borders, calcifications, extension through the thyroid capsule, or suspicious lymphadenopathy), or diffusely abnormal thyroid tissue accompanied by unexplained cervical lymphadenopathy. Based on results of FNAB, individuals were referred to thyroid surgery, and histological diagnoses were established according to WHO classification and independently reviewed by the International Pathology panel of the Chornobyl Tissue Bank. 16 Examiners were unaware of participants’ individual dose estimates.
We sequentially excluded individuals exposed in utero or at age 18 years or older on April 26, 1986 (n = 40), and those individuals without a thyroid dose estimate (n = 7), having diagnosis of thyroid cancer (n = 14) or thyroid surgery prior to first screening examination (n = 33), missing information on ultrasound examination (n = 19), and self-reported history of thyroid hormone intake (n = 35). 6 We also excluded 17 individuals in whom the presence or absence of thyroid nodule on ultrasound could not be determined with certainty. The final analytic sample consisted of 13,078 individuals.
Case definitions
Individuals were considered cases if they had at least one thyroid lesion ≥2 mm on first ultrasound examination conducted 1998–2000. Cases were grouped according to histological/cytological and ultrasound findings, and we refer to these as “case groups.” Individuals with thyroid cancer and/or follicular adenoma detected at first screening and surgically confirmed within three years were neoplastic cases. Individuals who were referred to FNAB following ultrasound examination but did not comply or had a cytological conclusion of inadequate, indeterminate, suspicious for cancer or neoplasia FNAB and did not undergo surgery were considered suspicious cases. Non-neoplastic cases included individuals whose nodules were determined to be benign (excluding follicular adenoma) either through FNAB and/or surgery (n = 148) or had no suspicious characteristics and were not referred to FNAB (n = 30). We also categorized individuals into case groups with single/multiple and large (≥10 mm)/small (<10 mm) nodules based on the largest ultrasound dimension. For individuals with multiple nodules, histological/cytological case designation was determined by the nodule with most suspicious finding.
Dosimetry
Details of the dosimetry methods have been described elsewhere. 17,18 Briefly, the main component of thyroid exposure was internal irradiation from ingestion of I-131, primarily through consumption of contaminated fresh cow’s milk, dairy products, and green leafy vegetables. Thyroid doses were based on: (1) direct measurements of I-131 thyroid activity taken within 2 months of the accident (prior to July 1986); (2) ecological and biokinetic models used to assess the temporal variation of I-131 radioactivity in the thyroid; and (3) personal interview information on individual behavior and dietary habits. An update of the dosimetry system has been recently completed. The main changes include the revision of I-131 thyroid activity measurements in study members, 19 the use of thyroid-mass values specific to the Ukrainian population, 20 and the revision of ground deposition densities of I-131 in Ukraine. 21 In our dose–response analyses, we used the arithmetic mean of the 1,000 dose estimate realizations per individual. Updated doses used in this analysis ranged from 0.0003 to 31 Gy with a mean of 0.53 Gy, median of 0.20 Gy, and 10–90 percentile range of 0.037–1.19 Gy.
Statistical analysis
We used binary logistic regression to estimate an excess odds ratio for thyroid nodule prevalence (EOR = OR − 1) in this cross-sectional study. A model of the prevalence probability, P(x, d, z), had the following linear form on the odds scale:
Both attained age (age at screening) and age at exposure (age at accident) were tested for interaction. By contrast, only attained age was used to characterize the background risk since it is biologically meaningful regardless of radiation exposure. We also examined effect modification by sex, urban versus rural residency in 1986, oblast of residence in 1986 (Zhytomyr, Kyiv, or Chernihiv), smoking history, family history of thyroid disease, urinary iodine concentration, and ultrasound-detected thyroid volume.
To examine variation in the effect of I-131 dose according to nodule’s histology/cytology, size, or number, we used the method of Pierce at al. for joint analysis of different outcomes. 23 Missing values were treated as separate categories in analyses, and statistical tests were two sided with a type I error of 0.05. Likelihood maximization 24 and profile likelihood confidence intervals 25 were used for parameter estimation using the GMBO module of EPICURE. 26
Results
Among 13,078 cohort members included, there were 358 (2.7%) individuals with at least one thyroid nodule detected at ultrasound examination. Of these, 65 (18%) were confirmed thyroid carcinoma (n = 44) or follicular adenoma (n = 21), 115 (32%) were suspicious for thyroid neoplasm, and 178 (50%) were non-neoplastic (Table 1). Overall, 256 (72%) individuals had large and 102 (28%) had small nodules. The proportion of neoplastic cases in individuals with large nodules was higher than in individuals with small nodules (22% vs. 9%), whereas the proportion of suspicious cases was lower (29% vs. 39%). Most individuals had a single nodule (n = 295, 82%). The distribution of cases by histology/cytology in individuals with single and multiple nodules was largely comparable.
Distribution of Cases with Any Ultrasound-Detected Thyroid Nodule by Histology/Cytology and Ultrasound Characteristics: Ukrainian-American Cohort, 1998–2000
Neoplastic cases included individuals with thyroid cancer (n = 44) or follicular adenoma (n = 21) histologically confirmed through surgery. Suspicious cases included individuals who were referred to FNAB following ultrasound examination but did not comply or had a cytological conclusion of inadequate, indeterminate, suspicious for cancer or neoplasia, and did not undergo surgery. Non-neoplastic cases included individuals whose nodules were determined to be benign (excluding follicular adenoma) either through FNAB (n = 148) and/or surgery (n = 12 with surgery and FNAB) or were not referred to FNAB (n = 30).
FNAB, fine-needle aspiration biopsy.
Background risk factors
Selected associations with background risk (adjusted for dose so that dose equals zero) of being a case with any thyroid nodule are presented in Table 2. Females had a greater odds of any thyroid nodule than males (OR = 3.82; CI: 3.00–4.90). Odds increased with increasing age at screening, leveling off at older ages. The odds of having any thyroid nodule was also higher for residents of Chernihiv compared with Zhytomyr (OR = 1.43; CI: 1.11–1.86). In addition, nodule odds increased with increasing thyroid volume. Urbanicity, self-reported history of smoking, and urinary iodine concentration were not associated with having a thyroid nodule. A family history of any thyroid disease was associated with a higher odds of having a thyroid nodule (not shown), although after adjustment for thyroid volume, this association was no longer statistically significant.
Background Risk Factors for Being a Case with Any Ultrasound-Detected Thyroid Nodule: Ukrainian-American Cohort, 1998–2000
Adjusted for I-131 dose based on a linear-exponential function, sex, oblast of residence in 1986, age at screening, and thyroid volume in the background (i.e., dose equals zero) unless one of these factors is under investigation.
Self-reported at first screening examination. One individual with unknown smoking status is excluded.
p-Values are based on likelihood ratio tests comparing nested models with and without factor under investigation. Age at screening and thyroid volume are modeled as linear quadratic on log scale trends and urinary iodine concentration as linear on log scale trend.
N, number; OR, odds ratio; CI, confidence interval; yrs, years.
I-131 dose-response
We found a dose–response based on a linear EOR model for each case group (Table 3). However, consistent with downturn or flattening in category-specific EORs at high doses, there was evidence of exponential departure from linearity for all thyroid nodules (LRT p = 0.02; Supplementary Table S1). The nonparametric and modeled dose–responses for all nodules as a group are shown in Figure 1. According to the best-fitting linear-exponential model, the I-131-related nodules EOR/Gy increase up to about 4 Gy, plateauing between 4 and 6 Gy, and slowly decrease thereafter. Below 5 Gy, the dose–responses were consistent with linearity for each case group (not shown).
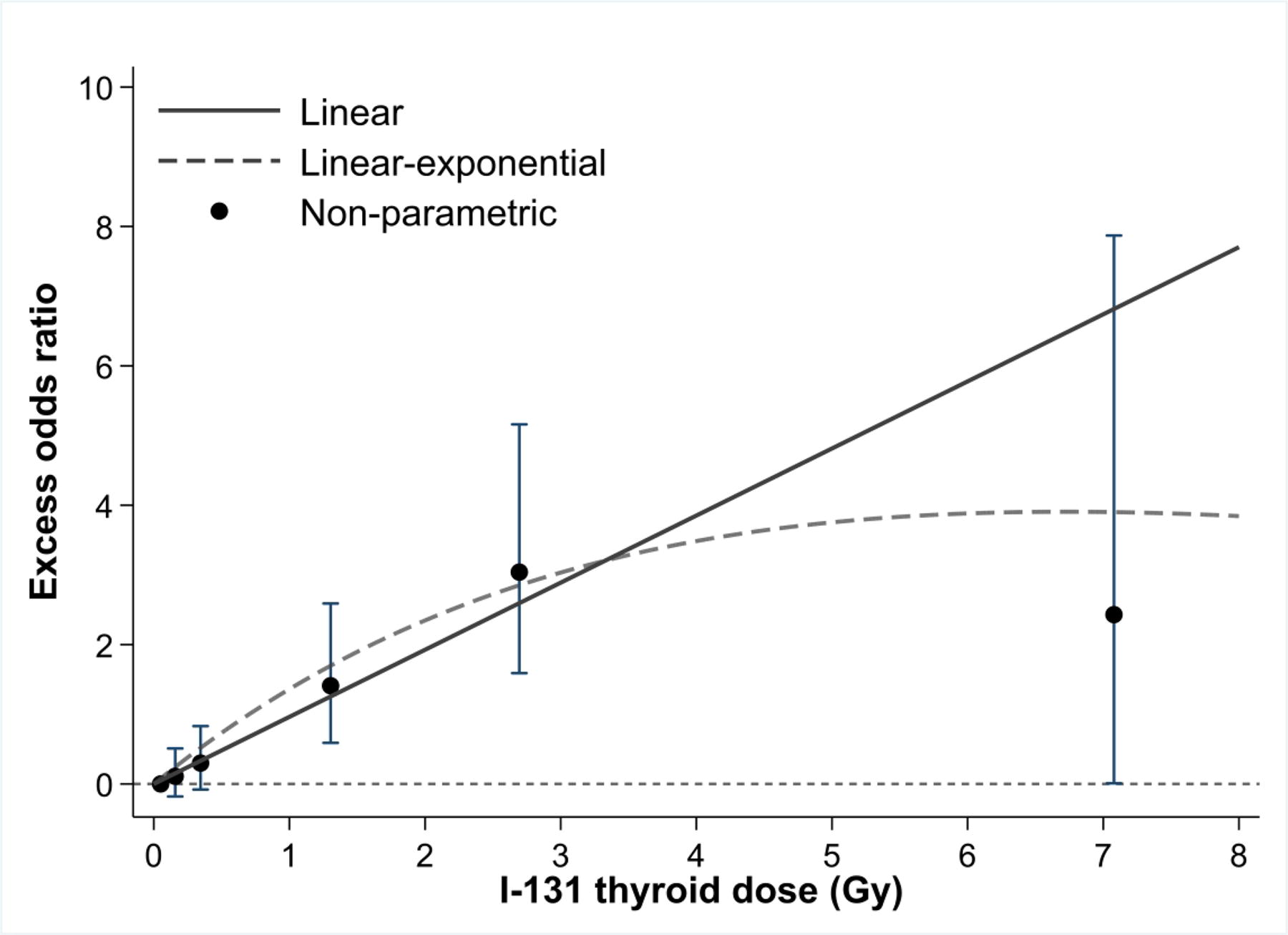
I-131 dose–response for all thyroid nodules over the full dose range: Ukrainian-American cohort, 1998–2000. Excess odds ratios are adjusted for sex, age at screening, oblast of residence in 1986, and thyroid volume. The solid and dashed lines represent fitted excess odds ratios based on linear and linear-exponential models, respectively. Circles and error bars represent non-parametric category-specific excess odds ratios and confidence intervals for the mean I-131 dose per category.
Excess Odds Ratios and Confidence Intervals of Being a Subject with Any Ultrasound-Detected Thyroid Nodule by Categories of I-131 Thyroid Dose for Different Case Groups: Ukrainian-American Cohort, 1998–2000
Excess odds ratios are adjusted for sex, oblast of residence in 1986, age at screening, and thyroid volume in the background.
1 degree of freedom test for linear trend with I-131 dose.
EOR, excess odds ratio.
Among individuals with doses < 5 Gy, for cases with any nodule, the EOR/Gy = 1.11 (CI: 0.65–1.77) (Table 4). We found heterogeneity in dose–response slopes by nodule histology/cytology, with the EOR/Gy = 5.35 (CI: 2.19–15.5) for neoplastic and 0.24 (CI: −0.07 to 0.74) for non-neoplastic cases for the pairwise comparison of slopes for neoplastic versus non-neoplastic (p < 0.001, degree of freedom = 1). We found no heterogeneity in dose–response slopes by size (p = 0.28) or number of nodules (p > 0.50). The EOR/Gy = 0.95 (CI: 0.50–1.64) for ≥10 mm, 1.73 (CI: 0.63,3.97) for <10 mm nodules and 1.05 (CI: 0.58–1.74) for single and 1.49 (CI: 0.36,4.54) for multiple nodules. The nonparametric and fitted linear dose response models below 5 Gy are shown in Supplementary Figure S2 for different case groups.
The Excess Odds Ratios per Gy and Confidence Intervals of Being a Subject with Any Ultrasound-Detected Nodule for Case Groups Defined by Nodule’s Characteristics and Thyroid Doses Less than 5 Gy: Ukrainian-American Cohort, 1998–2000
Excess odds ratio per Gy is estimated based on a simple linear model with adjustment for sex, age at screening, oblast of residence in 1986, and thyroid volume in the background.
Tests of heterogeneity of linear trends: 1 degree of freedom test comparing neoplastic versus non-neoplastic.
For all cases with thyroid nodules, there was no significant variation in the radiation dose response by sex, age at accident, age at screening, oblast of residence in 1986, urban/rural residence, thyroid volume, or urinary iodine (Supplementary Table S2).
Discussion
In this study of Ukrainian residents exposed in childhood or adolescence to radioactive I-131 from the Chornobyl accident, we found a strong association between thyroid dose and prevalence of any thyroid nodule detected at first screening. The dose–response was consistent with linearity below 5 Gy although, at high doses, there was evidence of a downturn in the EOR/Gy. An elevated EOR/Gy was found for all case groups in the full dose range. However, there was heterogeneity in risk by histology/cytology, with risk highest for neoplastic and lowest for non-neoplastic nodules, but not by nodule size or number.
Our study supports the evidence of increased risk of thyroid nodules following childhood exposure to I-131, an important public health issue related to environmental releases from nuclear weapons production, testing, and accidents. 4 An important comparison for the current study findings is the examination of thyroid nodule prevalence in Belarus. 13 The two studies have similar designs, methods of dose estimation and follow-up, and demographic characteristics. In the restricted dose range (<5 Gy), the estimated EOR/Gy for prevalence of having any ultrasound detected nodule in the two studies was comparable; the EOR/Gy in this Ukrainian cohort was 1.11 (CI: 0.65,1.77), although in the Belarusian cohort it was 0.70 (CI: 0.33–1.18) scaled for participants age 5 at the time of the accident. 13 The pattern of I-131 risk for the neoplastic and non-neoplastic case groups was also consistent; the EOR/Gy for neoplastic nodules was higher than for non-neoplastic nodules, i.e., 5.35 (CI: 2.19–15.5) versus 0.24 (CI: −0.07 to 0.74) in Ukraine and 3.82 (CI: 0.87–15.52) versus 0.32 (CI: < −0.03 to 0.70) in Belarus. 13 Higher radiation risks for malignant than benign thyroid nodules were also suggested in a thyroid screening study of atomic bomb survivors exposed <10 years of age to external radiation at a high dose rate, but the difference was not tested statistically; the overall risk estimates, and those broken down by malignant/benign are broadly comparable with our own, with an overall EOR/Gy = 1.65 (CI: 0.89–2.64). 5
We find the accumulating evidence of heterogeneity in dose–response by thyroid nodule histology/cytology intriguing. This could imply that, for a given dose and age/time since exposure, radiation is more effective in the induction of neoplastic than non-neoplastic thyroid lesions or that etiology of these lesions is divergent. Interestingly, in a recent genomic study of papillary thyroid cancers (PTC) and adenomatoid nodules, investigators found that the two lesions had few overlapping mutations and different phylogenetic trees suggesting independent development of PTC and benign nodules in unexposed individuals. 27 A radiation-related genomic profile characterization of papillary thyroid carcinoma after the Chornobyl accident provides evidence that ionizing radiation-induced DNA double-strand breaks represent an early carcinogenic event. 28 There is little information on molecular characteristics of benign thyroid nodules in irradiated children.
Despite the similarity of EORs for case groups with different nodule categories in Ukraine and Belarus, there were several notable differences. The prevalence of cases with small (<10 mm) thyroid nodules was substantially lower in the present study in Ukraine than in Belarus (0.8% vs. 5.3%), and the pattern of EORs by nodule size was opposite. In Ukraine, the EOR/Gy for small nodules was higher than for large nodules (1.73 vs. 0.95) although not significantly so; in Belarus, the EOR/Gy for small nodules was lower than for large nodules (0.27 vs. 2.12), with the difference being highly significant particularly for non-neoplastic nodules. 13 The reasons for this are unclear, but might include a more pronounced level of iodine deficiency in Ukraine or some other unknown factor. Previously, we reported that the median concentration of urinary iodine assessed at first screening was 41.7 µg/L in Ukraine 29 and 65.3 µg/L in Belarus, 30 being consistent with moderate and mild levels of iodine deficiency according to the WHO criteria. 31 Although the degree of endemic iodine deficiency has been associated with higher frequency of diffuse goiter 32 and increased iodine intake has been associated with a reduction in thyroid nodule size, 33,34 there is insufficient understanding of how iodine deficiency at the time or following I-131 exposure may affect induction and/or growth of radiation-related nodules.
The apparent lack of age at exposure effect in Ukraine (i.e., increased radiation risks with younger ages at exposure) contrasts with findings in Belarus and atomic bomb survivors. 5,13 This could be because of lower statistical power, chance, or the importance of some unmeasured modifier operating around the time of the accident.
Our study has several important strengths. We have individual I-131 thyroid dose estimates calculated from direct radioactivity measurements taken within 2 months after the accident. All participants underwent a standardized screening examination, including referral for FNAB and thyroid surgery conducted without knowledge of doses by clinical staff. The rate of compliance with FNAB (75%) and surgery (80%) was high. 6,7 Thyroid cancer and follicular adenoma diagnoses were confirmed through an independent international pathology review. 11,35,36
A limitation is that only 41% of those selected for tracing and recruitment became part of the cohort (Supplementary Fig. S1). However, we do not think that this introduced a selection bias as distributions of measured thyroid radioactivity were similar in participants and nonparticipants. 14 A second limitation is a lack of individual data on intake of stable iodine in 1986. However, we used oblast of residence at the time of accident as a surrogate measure of iodine intake in our analyses. In addition, we used thyroid volume and urinary iodine concentration measured during the first screening examination (12–14 years after the accident), but these reflect individual iodine status prior to screening. A third limitation is the cross-sectional design of the study and, therefore, inferences about causation and temporal patterns of risk should be drawn cautiously. Finally, the impact of uncertainties in dose estimates was not considered, though a study of thyroid cancer in this population did not find a meaningful difference in EORs/Gy after accounting for uncertanty. 37 This may be due in part to the fact that associated dose errors were modest. 17 Although we conducted a number of statistical tests, we did not correct for multiple testing as our main findings (i.e., the positive dose–response, its variation by nodule histology/cytology) were based on reasonable prior evidence.
To follow-up on our findings, it will be important to evaluate incidence of thyroid nodules detected during subsequent screening examinations in Ukraine. This will provide an improved understanding of age and time patterns of nodule incidence in relation to radiation exposure and role of iodine deficiency in growth dynamic of thyroid nodules. Pooling Ukrainian and Belarusian data will facilitate direct comparison of radiation-related risks and modifying patterns using the same models and accounting for relevant confounders. In addition, studies of genomic alterations in benign and malignant thyroid lesions in relation to I-131 dose will provide insights for improving our understanding of radiation effects.
In conclusion, the results of the current study in Ukraine add to the evidence that childhood exposure to I-131 is associated with an increased risk of having any thyroid nodule detected 12–14 years following exposure and that the I-131 risk for neoplastic nodules is higher than for non-neoplastic nodules. Future analyses of incidence data from subsequent screening cycles in Ukraine and pooling data with Belarus will improve characterization of I-131 risk by nodule groups and provide additional insights into thyroid nodule etiology.
Footnotes
Acknowledgments
Preliminary results related to this manuscript have been submitted as part of a master’s Thesis by Eric Grimm at the University of Colorado Anschutz Medical Campus (2015) and presented by Elizabeth Cahoon as a Highlighted Oral at the American Thyroid Association Annual Meeting (Washington D.C., September 27–October 1, 2023).
Authors’ Contributions
E.K.C.: Writing original draft (equal); review and editing (lead); conceived analysis (equal); conducted analysis (equal); methodology (equal); conceptualization (equal). E.G.: Writing original draft (equal); review and editing (supportive); conducted analysis (equal); conceptualization (supporting). K.M.: Review and editing (supportive); conceptualization (supporting). J.Z.M.: Review and editing (supporting); conducted analysis (equal); methodology (equal); conceptualization (supporting). R.Z.: Conducted analysis (equal); review and editing (supporting). V.D.: Review and editing (supporting). M.H.: Review and editing (supporting). M.P.L.: Conceived analysis (supporting); review and editing (supporting). K.O.P.: Review and editing (supporting). T.I.B.: Collected data (equal); review and editing (supporting). E.S.: Collected data (equal); review and editing (supporting). V.M.S.: Collected data (equal); review and editing (supporting). G.T.: Collected data (equal); review and editing (supporting). G.Z.: Collected data (equal); review and editing (supporting). I.P.P.: Collected data (equal); review and editing (supporting). S.V.M.: Collected data (equal); review and editing (supporting). M.C.: Collected data (equal); review and editing (supporting). L.B.Z.: Review and editing (supporting). R.M.: Review and editing (supporting). P.O’K.: Review and editing (supporting). M.D.T.: Collected data (equal); conceptualization (equal); review and editing (supporting). A.V.B.: Conceptualization (equal); conceived analysis (equal); conducted analysis (equal); writing original draft (equal); review and editing (supporting).
Author Disclosure Statement
E.K.C., E.G., K.M., J.Z.M., R.Z., V.D., M.H., M.P.L., K.O.P., T.I.B., E.S., V.M.S., G.T., G.Z., I.P.P., S.V.M., M.C., L.B.Z., R.M., P.O’K., M.D.T., A.V.B: No conflicts to disclose. No actual or potential competing financial funding to declare.
Funding Information
E.K.C., E.G., K.M., J.Z.M., R.Z., V.D., M.H., M.P.L., K.O.P., T.I.B., E.S., V.M.S., G.T., G.Z., I.P.P., S.V.M., M.C., L.B.Z., R.M., P.O’K., M.D.T., A.V.B.: This research was supported by the Intramural Research Program, Division of Cancer Epidemiology and Genetics, National Cancer Institute, National Institutes of Health, U.S. Department of Health and Human Services through the contract HHSN261201800762P between the National Cancer Institute, National Institutes of Health (USA), and the Science and Technology Center in Ukraine (STCU).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2