
Abstract
Background:
It has been reported that intracytoplasmic sperm injection (ICSI) may be the preferred fertilization method for women with thyroid autoimmunity (TAI) seeking assisted reproduction. We compared the reproductive outcomes of women with TAI who were treated with ICSI compared with in vitro fertilization (IVF).
Methods:
In this retrospective cohort study, we included women with infertility who were referred to the Reproductive Centre of Peking University Third Hospital for their first IVF/ICSI and embryo transfer (ET) treatment cycle from January 2019 to February 2021. In total, 2171 and 743 women with TAI underwent IVF and ICSI, respectively, while 8702 and 2668 women without TAI underwent IVF and ICSI, respectively. We examined the cumulative live birth rate (primary outcome) from the initiated stimulative cycle as well as the secondary outcomes of fertilization rate, rates of clinical pregnancy, and live birth after the first ET cycle. We compared the reproductive outcomes of women treated with IVF and ICSI according to TAI status. Multivariable logistic regression analyses were performed to adjust for relevant confounders.
Results:
Women who underwent ICSI had significantly higher fertilization rates than those who underwent IVF (median [interquartile range]: 0.6 [0.5–0.8] in the TAI-positive and IVF group vs. 0.7 [0.5–0.8] in the TAI-positive and ICSI group vs. 0.6 [0.5–0.8] the TAI-negative and IVF group vs. 0.7 [0.5–0.8] in the TAI-negative and ICSI group, p < 0.001). However, the rates of cumulative live births, clinical pregnancies, and live births were significantly lower among women with TAI who underwent ICSI than those who underwent IVF (cumulative live birth: 51.8% vs. 47%, adjusted odds ratio [aOR]: 0.80 [confidence interval, CI: 0.67–0.97]; clinical pregnancy: 43.0% vs. 38.8%, aOR: 0.81 [CI: 0.67–0.97]; live birth: 36.2% vs. 32.4%, aOR: 0.81 [CI: 0.66–0.98]).
Conclusion:
We observed that the use of ICSI in women with TAI was not associated with better assisted reproductive outcomes compared with IVF. Further prospective clinical trials are needed to confirm our findings.
Introduction
Thyroid autoimmunity (TAI) is the most common autoimmune disorder among women of childbearing age, which is characterized by the presence of thyroid antibodies, including thyroid peroxidase antibody (TPOAb) and thyroglobulin antibody (TgAb). The prevalence of thyroid antibodies is significantly higher in women with infertility. 1 –3 Moreover, infertile women with TAI may be prone to adverse assisted reproductive outcomes, including fewer good-quality embryos, increased spontaneous miscarriage rates, and decreased live birth rates, even when thyroid function is normal. 4 –6
The mechanism by which TAI affects female reproduction remains unclear. TAI may negatively impact follicle growth and development. Several studies have reported an association between TAI and ovarian reserve. A higher prevalence of thyroid antibodies in women with diminished ovarian reserves has been reported. 7,8 Women with TAI reportedly have a significantly higher risk of premature ovarian insufficiency. 9 Several studies suggest activation of an immune response in the ovarian microenvironment of women with TAI. Monteleone et al. reported the presence of thyroid antibodies in follicular fluid obtained from patients with TAI and detected the expression of thyroid peroxidase in human granulosa cells using immunocytochemistry, indicating that thyroid antibody-mediated cytotoxicity may be activated against follicles. 10 We previously reported significantly elevated levels of proinflammatory cytokines and chemokines in the follicular fluid of patients with TAI, suggesting an immune imbalance in the follicular microenvironment of patients with TAI, which may have detrimental effects on the oocytes and zona pellucida. 11
In vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI) are used to achieve fertilization during assisted reproduction. Although initially used for severe male factor infertility, ICSI has been increasingly used for other causes of infertility. 12 Based on studies demonstrating an abnormal follicular microenvironment in women with TAI, ICSI was suggested to overcome the impeding effect of thyroid antibodies in the follicular fluid and improve fertilization and pregnancy outcomes. 13 However, this suggestion stems primarily from hypotheses. Studies evaluating whether ICSI improves assisted reproductive outcomes in women with TAI were limited. 10,14 Therefore, we conducted this large-scale retrospective cohort study to investigate the impact of different fertilization protocols on assisted reproductive outcomes and investigate the value of ICSI in women with TAI.
Materials and Methods
Study population and follow-up
Peking University Third Hospital Medical Science Research Ethics Committee approved this retrospective study (approval number: M2023653) and waived the requirement for written informed consent. There were 20,033 women with infertility who were referred to the Reproductive Center of Peking University Third Hospital for their first IVF/ICSI-embryo transfer (ET) treatment cycle between January 2019 and February 2021. Women were excluded if they had no retrieved oocytes; had a history of thyroid surgery, thyroid cancers, hyperthyroidism, and other autoimmune diseases; underwent in vitro maturation or a natural or mini-stimulation protocol; received donor sperm or eggs; used frozen semen or eggs; underwent mixed IVF-ICSI cycles; obtained semen samples by testicular or microsurgical epididymal sperm aspiration; or underwent preimplantation genetic testing. In total,14,284 women were screened, including 10,873 and 3411 who underwent IVF and ICSI fertilization, respectively.
Patients with history of thyroid cancers and hyperthyroidism were excluded from our study based on clinical diagnosis. Patients with overt thyroid dysfunction based on their initial thyroid function test results were also excluded. We assessed thyroid function and measured levels of thyroid antibodies before performing controlled ovarian hyperstimulation (COH). Thyroid function markers, including thyrotropin (TSH) and free thyroxine (fT4) were within normal ranges in both groups. TPOAb and TgAb levels were measured in all patients. Patients with TPOAb and/or TgAb positivity were defined as the TAI group, and those with TPOAb and TgAb negativity were defined as the control group. Baseline characteristics were collected before initiating treatment. This study only included patients who underwent their first COH and oocyte retrieval cycles. Fresh ET cycles and all subsequent frozen-thawed ET cycles from the first stimulative cycles were analyzed. The participants were followed up until December 31, 2021. Follow-up was terminated when a live birth was achieved or when all embryos from the first oocyte retrieval were used.
Assisted reproductive technology procedures
All patients underwent a standardized COH regimen. 15 Oocyte retrieval was performed 34–36 hours after human chorionic gonadotropin (HCG) administration. The retrieved cumulus–oocyte complexes (COCs) were incubated for 2–6 hours before insemination or injection. Fresh ejaculated semen samples were obtained through masturbation on the day of oocyte retrieval and processed through discontinuous density gradient centrifugation. In conventional IVF groups, each oocyte was inseminated using a concentration of 0.1–0.2 × 106 motile sperms per milliliter. In the ICSI groups, the retrieved COCs were stripped using hyaluronidase, and only mature oocytes (metaphase II oocytes) were microinjected. Normal fertilization (the presence of two pronuclei [2PN]) was assessed at ∼16–18 hours after insemination. Embryos were evaluated 67–69 hours after fertilization according to the quality, number, and size of the blastomeres and the amount of anucleate fragmentation. Fresh or frozen-thawed ET was performed according to the patient’s condition. Our standard practice is to transfer fresh embryos whenever available. The freeze-all strategy was initiated in some cases, including patients at risk for ovarian hyperstimulation syndrome, elevated progesterone levels on the HCG trigger day, hydrosalpinx, endometrial factors (endometrial polyps, endometrial cavity fluid, and thin endometrium), systemic diseases (stomach, fever, or cold), and sudden accidents.
Laboratory testing
Blood samples were collected within 6 months before the initiation of COH for thyroid function measurement. Serum TSH, fT4, TPOAb, and TgAb levels were measured using a fully automatic chemiluminescence immunoassay analyzer (Supplementary Table S1 provides assay method and variable coefficient). The reference values were 0.55–4.78 uIU/mL for TSH and 0.89–1.76 ng/dL for fT4. Concentrations above 60 IU/mL were considered positive for TPOAb and TgAb. The levels of basal female hormones, including follicle-stimulating hormone (FSH), luteinizing hormone (LH), and estradiol, were measured using an automatic chemiluminescence immunoassay analyzer (Supplementary Table S1 reports assay method and variable coefficient) during days 2–4 of the unstimulated menstrual cycle. Blood samples for LH, estradiol, and progesterone levels were collected on the trigger day for female hormone testing. Sperm concentration and progressive motility were assessed before COH using computer-assisted semen analysis.
Study outcomes
The primary outcome was the cumulative live birth rate, which was defined as the deliveries of one or more living infants in the first and subsequent frozen-thawed cycles. The calculation of the cumulative rate included births from the first transfer cycle and all subsequent frozen-thawed cycles from the initiated stimulative cycles performed before December 2021. The secondary outcomes were fertilization rates, number of good-quality embryos, clinical pregnancy rates, and live birth rates. Normal fertilization was defined as the number of zygotes with 2PN. The denominator of the fertilization rate was the number of inseminated or injected oocytes. The fertilization rate in the IVF group was calculated as the number of zygotes with 2PN divided by the number of retrieved oocytes. The fertilization rate in the ICSI group was calculated as the number of zygotes with 2PN divided by the number of retrieved metaphase II oocytes. Embryos were evaluated on the third day after fertilization. Good-quality embryos were developed from 2PN zygotes and met the following criteria: (1) more than five blastomeres, (2) size difference <20%, and (3) fragmentation <50%. Clinical pregnancy was defined as the presence of at least one gestational sac on ultrasonography. Live birth was defined as the delivery of one or more live infants.
Statistical analyses
Regarding continuous variables, normally distributed parameters were presented as means (standard deviations) and non-normally distributed parameters as medians (interquartile ranges). Analysis of variance was performed to compare the differences among samples with normal distribution and equal variance, and the Kruskal–Wallis H test was conducted for samples without normal distribution or equal variance. For categorical variables, data were presented as the number of cases (percentage) and compared using the chi-square test. For analyzing the pregnancy outcomes after the first ET cycles, a multivariable logistic regression model was conducted to calculate the odds ratios (ORs) with confidence intervals (CIs) after adjusting for covariates including age, body mass index (BMI), type of infertility (primary vs. secondary), cause of infertility (male factor only, female factor only, combined male/female factor, or unexplained infertility), fT4 and TSH levels, COH protocols (ultralong gonadotropin-releasing hormone [GnRH] agonist, long GnRH agonist, or GnRH antagonist protocol), type of transfer (fresh ET vs. frozen-thawed ET), and type of transferred embryos (cleavage-stage embryo vs. blastocyst). In the analysis of cumulative live birth rates, we only included the initial live birth for each patient and live births after the initial one was not considered. A multivariable logistic regression analysis was performed to analyze cumulative live birth rates and calculate the ORs with CIs after adjusting for covariates including age, BMI, type of infertility (primary vs. secondary), cause of infertility (male factor only, female factor only, combined male/female factor, or unexplained infertility), fT4 and TSH levels, COH protocols (ultralong GnRH agonist, long GnRH agonist, or GnRH antagonist protocol), type of transfer (fresh ET vs. frozen-thawed ET), and type of transferred embryos (cleavage-stage embryo vs. blastocyst). All analyses were performed using IBM SPSS Statistics for Windows, version 24 (IBM Corp., Armonk, NY, USA). Statistical significance was defined as a two-sided p-value of <0.05.
Results
Overall, 14,284 women scheduled for their first IVF/ICSI cycles were screened for inclusion. Furthermore, 2171 women with TAI and 8702 women without TAI underwent fertilization via IVF, and 743 women with TAI and 2668 women without TAI underwent fertilization via ICSI. After excluding women with no embryos obtained and women with all embryos frozen (only women who froze all embryos and did not transfer embryos until our follow-up was terminated), 1933 women with TAI in the IVF group, 7773 women without TAI in the IVF group, 670 women with TAI in the ICSI group, and 2668 women without TAI in the ICSI group began their first ET cycle (Fig. 1).
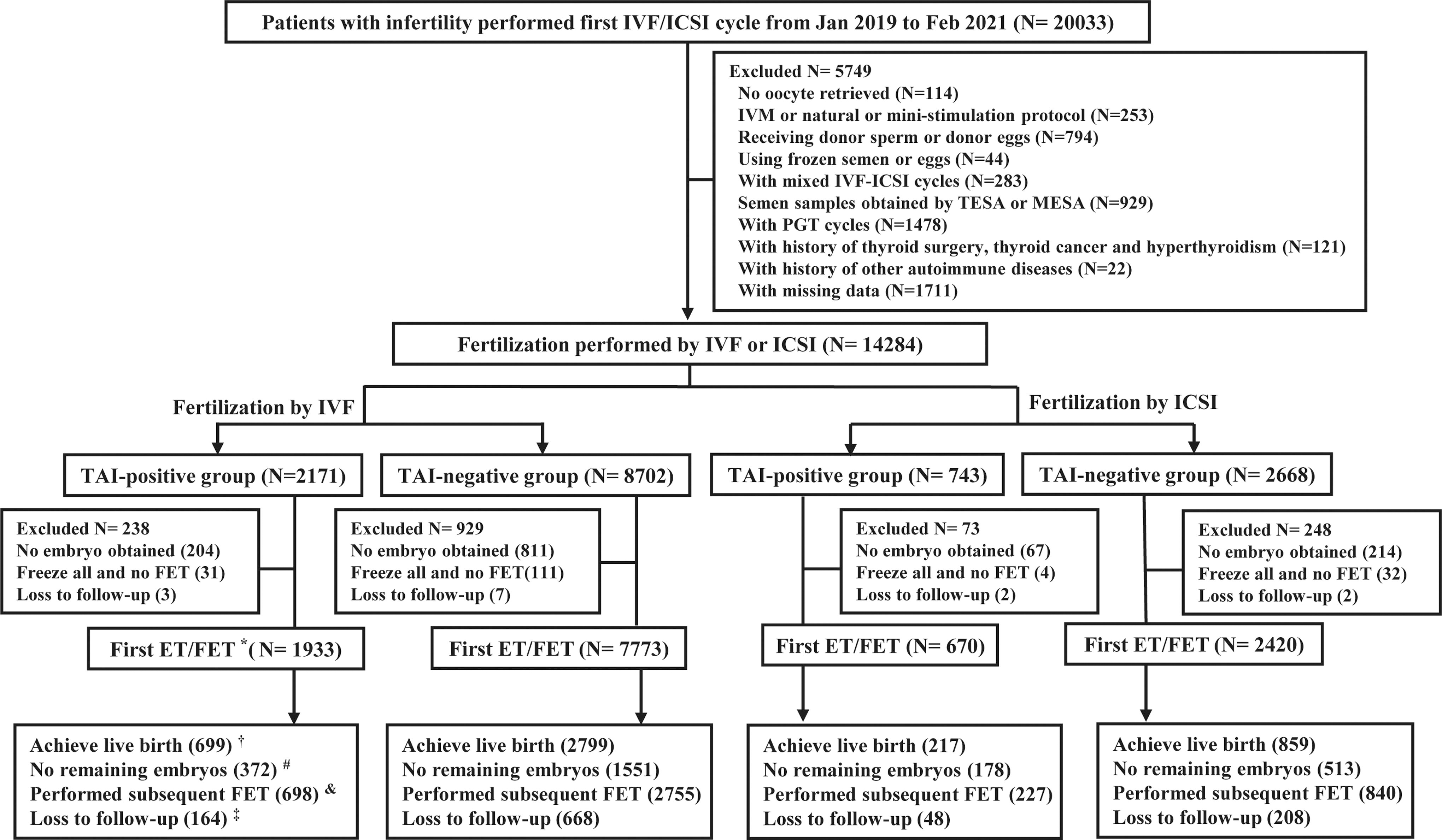
Flowchart of the study cohort and follow-up procedures. ET, embryo transfer; FET, frozen-thawed embryo transfer; ICSI, intracytoplasmic sperm injection; IVF, in vitro fertilization; MESA, microsurgical epididymal sperm aspiration; PGT, preimplantation genetic testing; TAI, thyroid autoimmunity; TESA, testicular sperm aspiration. *Includes patients with their first fresh embryo transfer and those who underwent the freeze-all strategy and their first frozen-thawed embryo transfer.
The baseline characteristics of the patients are presented in Table 1. Age, but not BMI, was significantly different among the four groups. The incidence of primary infertility was significantly higher in the ICSI group than in the IVF group in both TAI-positive and TAI-negative women. Regarding couples with a known cause of infertility, the proportion of male infertility factors was significantly higher in the ICSI group (53.3% in TAI-positive group and 54.8% in TAI-negative group) than in the IVF group (21.7% in TAI-positive group and 19% in TAI-negative group) (p < 0.001). Basal hormone levels were measured before treatment, and no significant difference was observed among the four groups in terms of FSH levels (p = 0.807). However, the levels of LH (p < 0.001) and estradiol were significantly different among the four groups (p = 0.003). A significant difference in thyroid function was also observed among the four groups. TSH levels were significantly higher in women with TAI (median [interquartile range]: 2.1 [1.5–3.0] in the IVF group and 2.2 [1.4–3.1] in ICSI group) than in those without TAI (median [interquartile range]: 2.0 [1.4–2.7] in the IVF group and 2.0 [1.5–2.8] in the ICSI group) (p < 0.001). Sperm concentration and motility were significantly lower in the ICSI group than in the IVF group (p < 0.001), which may be associated with a higher proportion of couples with male infertility in the ICSI group.
Baseline Patient Characteristics
The p-value refers to the comparison among four groups.
*In TAI-positive IVF vs. ICSI, p < 0.05.
**In TAI-negative IVF vs. ICSI, p < 0.05.
Cause of infertility is the most important indication for couples who undergo IVF/ICSI treatment.
Testing for basal FSH, LH, and estradiol was performed between day 2 and day 4 of the menstrual cycle.
Statistically analyzed using the analysis of variance.
Statistically analyzed using the chi-square test.
Statistically analyzed using the Kruskal–Wallis H test.
BMI, body mass index; FSH, follicle-stimulating hormone; fT4, free thyroxine; ICSI, intracytoplasmic sperm injection; IQR, interquartile range; IVF, in vitro fertilization; LH, luteinizing hormone; SD, standard deviation; TAI, thyroid autoimmunity; TSH, thyrotropin.
As presented in Table 2, the protocols for COH differed significantly among the four groups. Regardless of TAI status, the ICSI group demonstrated a significantly higher number of retrieved oocytes (median [interquartile range]: 10.0 [6.0–16.0] in the TAI-positive and IVF group vs. 12.0 [8.0–17.0] in the TAI-positive and ICSI group vs. 10.0 [6.0–16.0] in the TAI-negative and IVF group vs. 12.0 [8.0–17.0] in the TAI-negative and ICSI group, p < 0.001) and fertilization rates per inseminated or injected oocyte (median [interquartile range]: 0.6 [0.5–0.8] in the TAI-positive and IVF group vs. 0.7 [0.5–0.8] in the TAI-positive and ICSI group vs. 0.6 [0.5–0.8] in the TAI-negative and IVF group vs. 0.7 [0.5–0.8] in the TAI-negative and ICSI group, p < 0.001) than the IVF group. However, the number of good-quality embryos did not significantly differ among the four groups (median [interquartile range]: 4.0 [2.0–7.0] in the TAI-positive and IVF group vs. 4.0 [2.0–7.0] in the TAI-positive and ICSI group vs. 4.0 [2.0–7.0] in the TAI-negative and IVF group vs. 4.0 [2.0–7.0] in the TAI-negative and ICSI group, p = 0.893) (Table 2).
Details of Protocols for Controlled Ovarian Hyperstimulation and Data on In vitro Fertilization and First Embryo Transfer Cycle
The p-value refers to the comparison among four groups.
*In TAI-positive IVF vs. ICSI, p < 0.05.
**In TAI-negative IVF vs. ICSI, p < 0.05.
Normal fertilization was defined as the number of zygotes with two pronuclei. The denominator of the fertilization rate was the number of inseminated or injected oocytes. The fertilization rate in the IVF group was calculated as the number of zygotes with 2PN divided by the number of retrieved oocytes. The fertilization rate in the ICSI group was calculated as the number of zygotes with 2PN divided by the number of retrieved metaphase II oocytes.
Embryos were evaluated on the third day after fertilization. Good-quality embryos were developed from 2PN zygotes and met the following criteria: (1) more than five blastomeres, (2) size difference <20%, and (3) fragmentation <50%.
Statistically analyzed using the analysis of variance.
Statistically analyzed using the chi-square test.
Statistically analyzed using the Kruskal–Wallis H test.
2PN, two pronuclei; COH, controlled ovarian hyperstimulation; E2, estradiol; GnRH, gonadotropin-releasing hormone; P, progesterone.
Logistic regression analysis was performed to adjust for covariates associated with pregnancy outcomes, including age, BMI, type of infertility (primary vs. secondary), cause of infertility (male factor only, female factor only, combined male/female factor, or unexplained infertility), thyroid function, COH protocols (ultralong GnRH agonist, long GnRH agonist, or GnRH antagonist protocol), type of transfer (fresh vs. frozen-thawed ET), and type of transferred embryos (cleavage-stage embryo vs. blastocyst). Women who were TAI-positive and fertilized with IVF were defined as the reference group. Clinical pregnancy and live birth rates after the first ET from the initial cycle did not significantly differ in the IVF and ICSI groups among patients without TAI (clinical pregnancy: 42.7% and 41.5%, adjusted OR: 0.96 and 0.89 [CI: 0.87–1.07 and 0.78–1.01], compared with the reference group; live birth: 36% and 35.5%, OR: 0.96 and 0.91 [CI: 0.87–1.07 and 0.80–1.04], compared with reference) (Table 3). However, the clinical pregnancy and live birth rates were significantly lower in the ICSI group than in the IVF group in patients with TAI (clinical pregnancy: 43% vs. 38.8%, adjusted OR: 0.81 [CI:0.67–0.97]; live birth: 36.2% vs. 32.4%, adjusted OR: 0.81 [CI: 0.66–0.98]) (Table 3).
Pregnancy Outcomes After the First Embryo Transfer Cycle in Different Groups
The multivariable model was adjusted for age, body mass index, type of infertility (primary vs. secondary), cause of infertility (male factor only, female factor only, combined male/female factor, or unexplained infertility), fT4 and TSH levels, COH protocol (ultralong GnRH agonist, long GnRH agonist, or GnRH antagonist protocol), type of transfer (fresh ET vs. frozen-thawed ET), and type of transferred embryos (cleavage-stage embryo vs. blastocyst).
Clinical pregnancy was defined as the presence of at least one gestational sac in the uterus identified by ultrasonography 35 days after ET.
Live birth was defined as the delivery of at least one live infant.
CI, confidence interval; ET, embryo transfer; OR, odds ratio.
In the TAI-negative group, 7773 women who underwent IVF performed 11,706 ET cycles, whereas 2420 women who underwent ICSI performed 3597 ET cycles, resulting in 4076 (52.4%) cumulative live births and 1240 (51.2%) cumulative live births, respectively. In the TAI-positive group, 1933 women who underwent IVF performed 2912 ET cycles, resulting in 1001 cumulative live births (51.8%), while 670 women who underwent ICSI performed 988 ET cycles, resulting in 315 live births (47%). As illustrated in Figure 2, women who were TAI-positive and underwent ICSI exhibited lower cumulative live birth rates than those in the other groups (Fig. 2). Logistic regression analysis was performed, adjusting for age, BMI, type of infertility (primary vs. secondary), cause of infertility (male factor only, female factor only, combined male/female factor, or unexplained infertility), fT4 and TSH levels, COH protocols (ultralong GnRH agonist, long GnRH agonist or GnRH antagonist protocol), type of transfer (fresh ET vs. frozen-thawed ET), and type of transferred embryos (cleavage-stage embryo vs. blastocyst), and we analyzed the differences among the four groups (where women who were TAI-positive and fertilized by IVF were defined as the reference group). No significant difference in the cumulative live birth rates was observed among women without TAI, regardless of whether they underwent IVF or ICSI (adjusted OR: 0.99 and 0.93 [CI: 0.89–1.10 and 0.82–1.06], compared with reference group) (Table 4). However, among women in the TAI-positive group, the cumulative live birth rates in the ICSI group were significantly lower than those in the IVF group (adjusted OR: 0.80 [CI: 0.67–0.97]) (Table 4).

Observed cumulative live birth rates among the different groups.
Comparison of Cumulative Live Birth Rates Among the Different Groups
The multivariable model was adjusted for age, body mass index, type of infertility (primary vs. secondary), cause of infertility (male factor only, female factor only, combined male/female factor or unexplained infertility), fT4 and TSH levels, COH protocol (ultralong GnRH agonist, long GnRH agonist, or GnRH antagonist protocol), type of transfer (fresh ET vs. frozen-thawed ET), and type of transferred embryos (cleavage-stage embryo vs. blastocyst).
CLBR was defined as the delivery of one or more living infants in the first and subsequent frozen-thawed cycles. The cumulative live birth rate was calculated as the number of cumulative live births divided by the number of COH cycles.
CLBR, cumulative live birth rates.
Subgroup analysis was performed to investigate the difference in pregnancy outcomes based on causes of infertility. There was no significant difference in the rates of clinical pregnancy and live birth after the first ET cycle between women fertilized by ICSI and those fertilized by IVF in the TAI-positive group among different subgroups after adjusting for age, BMI, type of infertility (primary vs. secondary), fT4 and TSH levels, COH protocols (ultralong GnRH agonist, long GnRH agonist, or GnRH antagonist protocol), type of transfer (fresh ET vs. frozen-thawed ET), and type of transferred embryos (cleavage-stage embryo vs. blastocyst) (Supplementary Fig. S1). However, among women, owing to unexplained fertility, a significantly higher cumulative live birth rates were observed in TAI-positive women fertilized by ICSI compared with those fertilized by IVF (cumulative live birth rates: 62.5% vs. 45.5%, adjusted OR: 2.34 [CI: 1.05–5.21]) (Supplementary Fig. S2). We also performed subgroup analysis based on different types of thyroid antibodies. Women who were co-positive for TgAb and TPOAb and fertilized with IVF were defined as the reference group. As shown in Supplementary Figure S3, there was no significant difference in the rates of clinical pregnancy (p > 0.05 for all groups) and live birth rate (p > 0.05 for all groups) among different groups after adjusting for relevant covariates. However, a significantly lower cumulative live birth rate was detected in women who were isolated-positive for TPOAb and fertilized by ICSI after adjusting for relevant covariates (p = 0.045) (Supplementary Fig. S4).
Discussion
In this study, we observed significantly lower rates of cumulative live births, clinical pregnancies, and live births after the first ET and from initiated stimulative cycles using ICSI compared with IVF among women with TAI, even after adjusting for relevant covariates.
Over the past two decades, ICSI has been widely used to overcome fertilization failure and obtain high-grade embryos; however, its benefits remain controversial. In our study, irrespective of TAI status, we observed significantly higher numbers of retrieved oocyte and fertilization rates in the ICSI group than in the IVF group, which may be associated with different infertility factors between the groups. The number of participants with male factor infertility was higher in the ICSI group than in the IVF group; thus, women in the ICSI group were prone to have better ovarian reserve and ovarian response. However, the numbers of good-quality embryos were similar among the four groups. Our results are consistent with those of a recent randomized controlled trial conducted by Dang et al., 16 which investigated the differences in assisted reproductive outcomes between IVF and ICSI in couples with non-male factor infertility; they reported a higher fertilization rate in the ICSI group than in the IVF group. Similar to the results of our study, the number of good-quality embryos was similar in the ICSI and IVF groups.
Some discrepancies in the fertilization rate exist among studies on ICSI and IVF. Bhattacharya et al. reported a higher fertilization rate in the IVF group than in the ICSI group. 17 However, a meta-analysis of seven studies found no significant difference in the fertilization rate between the IVF and the ICSI groups. 18 This controversial conclusion may have resulted from different calculation modes. We defined the fertilization rate as the number of zygotes with 2PN divided by the number of oocytes inseminated or injected. However, the denominator of the fertilization rate in some studies was replaced by the number of oocytes retrieved. Despite the discrepancies in fertilization rates, the number of good-quality embryos was similar between the IVF and the ICSI groups in most studies. 16,17,19
The embryo quality assessment is based on morphological features, including cell number, size, and fragmentation. However, pregnancy outcomes, including live birth and cumulative live birth, are more accurate markers that reflect the developmental potential of the obtained embryos. Several studies have focused on whether the increased use of ICSI can improve pregnancy outcomes in patients with non-male factor infertility. Two retrospective cohort studies reported similar live birth and cumulative live birth rates between the IVF and ICSI groups in couples with non-male factor infertility. 20,21 One retrospective study of 745 women aged 40–43 years found no significant differences in pregnancy outcomes between the IVF and ICSI groups. 19 Another retrospective study of women with tubal ligation observed a significantly lower live birth rate in the ICSI group than in the IVF group. 22 One prospective randomized trial of 60 women with unexplained infertility found no significant difference between the two groups. 23 A recent large-scale randomized controlled trial randomly assigned 1064 couples with non-male factors to the IVF or ICSI groups. The two groups had similar pregnancy outcomes, including clinical pregnancy and live birth rates. 16
Studies evaluating the difference in assisted reproductive outcomes between IVF and ICSI group among women with TAI are limited. TAI is an important factor affecting female fertility, owing to its high prevalence in women with infertility and its association with adverse pregnancy outcomes. 1,2,4,5 Some studies reported significantly lower fertilization rates and grade A embryo rates in women with TAI and speculated that ICSI could mitigate the adverse effects of an abnormal follicular microenvironment and improve pregnancy outcomes in women with TAI. 10,24 Rao et al. performed a subgroup analysis to demonstrate the effects of TAI on clinical outcomes in IVF and ICSI cycles and reported similar fertilization rates, embryo quality, and pregnancy outcomes among different groups. 25 Another recent study that included 185 IVF cycles and 116 ICSI cycles performed in women with TAI reported a lower clinical pregnancy and live birth rates in the ICSI group than the IVF group; however, the difference did not reach statistical significance. 26 Our study included a large sample size, and we observed that both live birth rates after the first ET cycle and cumulative live birth rates from initiated stimulative cycles were significantly lower in the ICSI group than in the IVF group among women with TAI.
The mechanisms involved in the observed decreased live birth rates in women fertilized by ICSI in TAI group remains unclear. Several hypotheses have been proposed to explain the adverse impact of TAI on the ovarian microenvironment and follicle development. The presence of thyroid antibodies in the follicular fluid retrieved from women with TAI and the expression of thyroid peroxidase in ovarian granulosa cells support the hypothesis for an abnormal ovarian microenvironment and antibody-mediated cytotoxicity causing damage to oocytes. 10 Our previous study detected the percentage of inflammatory lymphocytes and the expression of inflammatory chemokines and cytokines in follicular fluid obtained from women with TAI. We observed significant activation of the CXCR3 inflammatory cascade, indicating a considerable immune imbalance in the follicular microenvironment of women with TAI. The abnormal ovarian microenvironment may affect the development of oocytes and make them prone to be injured. 11 Compared with conventional IVF, ICSI is an invasive technique that may damage oocytes. The pipette triggers physical breakage in the oocyte membrane during injection, and a small amount of medium, which may contain harmful components, is inevitably injected into the oocytes. Previous studies have reported a higher risk of oocyte degeneration and chromosomal aberrations in embryos fertilized by ICSI, and embryos with chromosomal aberrations can develop into blastocyst stage, suggesting that the fate of an embryo cannot be predicted by its morphological assessment. 27 –30 Thus, pregnancy outcomes may be more valuable markers to reflect the developmental potential of embryos.
The strength of our study lies in the large number of included participants. However, our study has some limitations. First, our study was retrospective, and the biases introduced from retrospective data collection could not be avoided. Second, there was a significant difference in the cause of infertility between the IVF and the ICSI groups, as ICSI is commonly performed in couples with male factors infertility in our country; however, we performed multivariable logistic regression analysis to adjust for this factor, and we further performed subgroup analysis based on the different causes of infertility. Further prospective clinical trials performed in patients with non-male factor infertility are required to confirm our findings. Third, owing to its retrospective design, our study did not investigate the use of levothyroxine; however, we evaluated thyroid function before COH and thyroid function markers, including fT4 and TSH, were within normal ranges in both groups, and we adjusted for fT4 and TSH levels when analyzing pregnancy outcomes. We reviewed studies about the impact of the use of levothyroxine (LT4) in assisted reproductive outcomes, and several studies have reported that there was no significant difference on pregnancy outcomes between euthyroid patients without LT4 treatment and euthyroid patients after LT4 treatment. 31 –33 Fourth, our study was conducted in a single center, and the generalizability of our results needs to be confirmed by future multicenter studies.
In conclusion, our study showed that using ICSI in women with TAI was not associated with better assisted reproductive outcomes, which raises questions about the value of ICSI in assisted reproductive technology among these women. Although our subgroup analysis in women with unexplained infertility suggested a significantly higher cumulative live birth rates in TAI-positive women fertilized by ICSI compared with those fertilized by IVF, the sample size in this subgroup was limited. Future prospective clinical trials are needed to confirm our findings.
Footnotes
Availability of Data and Materials
All datasets generated and analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Authors’ Contributions
N.H., H.C., and J.Q. conceived the study, and all the authors contributed to the discussion. N.H., L.C., and H.W. participated in the patient follow-up. N.H., L.Z., and Z.Y. contributed to the statistical analyses. N.H. initially drafted the article, and all the authors contributed to the article revision. All authors contributed to the article and have read and approved the submitted version.
Author Disclosure Statement
All authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This study was supported by the
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Table S1