
Abstract
Background:
Despite a good prognosis, survivors of differentiated thyroid cancer (DTC) may have reduced health-related quality of life (HRQOL) many years after treatment, and it is unclear how suppression of thyroid-stimulating hormone (TSH) may contribute to HRQOL. This study investigated changes in HRQOL in the 5 years following DTC treatment, the association between HRQOL and TSH suppression, and how HRQOL compares to the general population.
Methods:
In this nationwide prospective cohort study, 487 patients with DTC were identified between 2012 and 2017 from all Swedish hospitals treating patients with DTC. Patients treated with total thyroidectomy and planned for radioiodine answered the Swedish version of the Short Form-36 Health Survey (SF-36) and a study specific questionnaire at treatment and after 1, 3, and 5 years. Summary measures for physical and mental QOL were derived from the SF-36, and TSH values were collected from patient records. To study changes in HRQOL over time, linear mixed models were fitted on multiply imputed data, with all patients and measurement points included in the model.
Results:
In total, 351 patients consented to participate in the study. In the 5 years following DTC treatment, physical QOL did not change significantly with time, while mental QOL improved by on average 0.61 (p < 0.001) per year. TSH levels were not predictive of either physical or mental QOL, or their change over time. At 5 years, there was a significant difference in physical and mental QOL compared with the Swedish general population, but effect sizes were small (Cohen’s d = 0.29 and −0.21, respectively). The SF-36 domains general health, vitality, social functioning, and mental health were lower at 5 years compared with the general population (difference 8.7–13.3), and these differences were clinically significant.
Conclusions:
The mental component of HRQOL improves over time following DTC treatment. HRQOL in patients with DTC is not explained by TSH suppression. Although overall differences in physical and mental HRQOL compared with the general population were small 5 years after treatment, several specific psychosocial HRQOL domains were clinically meaningfully reduced. Psychosocial health issues should be screened for during DTC follow-up.
Introduction
Thyroid cancer has a generally good prognosis with a 5-year survival rate of over 90%. 1,2 The majority of thyroid cancers (more than 95%) are differentiated thyroid cancer (DTC). 3 Cross-sectional studies indicate that, despite a favorable prognosis, health-related quality of life (HRQOL) in survivors of DTC may be lower than that in the general population, even over a decade after treatment. 4,5 Moreover, HRQOL in DTC survivors has been found to be similar or worse compared with survivors of several other cancers with worse prognosis. 6 –8
Primary treatment of DTC consists of thyroid surgery, most often total thyroidectomy, which is followed by radioactive iodine (RAI) for those with a higher risk of recurrence. 9 To reduce the risk of recurrence following surgery and RAI, patients commonly receive levothyroxine in doses that suppress levels of thyroid-stimulating hormone (TSH), where patients with a higher risk of recurrence are recommended more aggressive TSH suppression. 10 Because the iatrogenic hyperthyroidism induced by TSH suppression can lead to adverse effects such as osteoporosis and cardiovascular disease, the potential benefit of TSH suppression must be balanced against the risks in order to decide an optimal degree of TSH suppression in the individual patient. 10 –14
It has been suggested that the symptoms of hyperthyroidism caused by TSH suppression could contribute to lower HRQOL in patients with DTC. However, the association between the two remains unclear, 15,16 and there is a lack of longitudinal studies. A previous study using a cohort of Swedish patients with DTC by Hedman et al. found that HRQOL improved from diagnosis to 1 year and found no linear association between TSH suppression and HRQOL. 17 Using the same cohort of Swedish patients with DTC, our primary aim was to study how HRQOL develops long term in the 5 years following treatment. The secondary aims of this study were to investigate how HRQOL and its development over time may be associated with levels of TSH, as well as whether HRQOL was lower in patients with DTC compared with the general population after 5 years.
Materials and Methods
Study design and population
A nationwide prospective cohort study was conducted in Sweden from 2012 to 2022. Patients with DTC were included between January 2012 and March 2017, from all 13 Swedish departments of oncology or surgery treating patients with DTC with RAI. Patients with DTC were included after surgery but before RAI treatment and were followed for 5 years. Inclusion criteria were as follows: age ≥18 years at inclusion, Swedish-speaking, able to read and write, a primary diagnosis of DTC and thyroidectomy. During the study period, guidelines in Sweden recommended RAI treatment to all patients with T1b tumors or larger, and therefore, only patients scheduled for RAI treatment were included. Exclusion criteria were as follows: DTC T1a, ongoing treatment for other malignancy, DTC recurrence at inclusion, or anaplastic, medullary, or poorly differentiated thyroid cancer. Patients were informed about the study by mail and gave their consent to participate by completing and returning questionnaires. This method of collecting consent was presented in the patient information and was approved by the Regional Ethical Review Board. Follow-up occurred after 1, 3, and 5 years, through mail and patient records. Nonresponders were sent up to three reminders. The study was approved by the Regional Ethical Review Board in Stockholm, Sweden (2011/718-31/2). Reporting of the study followed the STROBE Checklist for cohort studies whenever possible. 18
Data collection and categorization
Sociodemographic variables and comorbidities
Patients were asked to provide information regarding education, marital status, employment, and comorbidities at inclusion. Comorbidities were chosen based on their possible association with HRQOL or TSH suppression. Patients were asked in a yes/no format if they had the following comorbidities as diagnosed by a physician: previous myocardial infarction, atrial fibrillation, hypertension, stroke, diabetes, kidney failure, asthma, chronic obstructive pulmonary disease, osteoporosis, rheumatoid arthritis or osteoarthritis, depression requiring treatment, and other psychiatric disease. Comorbidities were further grouped into the variable “relevant comorbidities,” where only comorbidities with a theoretically and empirically hypothesized association with both HRQOL and TSH were included: previous myocardial infarction, 11 atrial fibrillation, 12 hypertension, 11 osteoporosis, 19 and depression. 20
Cancer-related variables
Information about the following clinical characteristics was collected from medical records at inclusion and after 1, 3, and 5 years: surgery, histology, tumor stage (TNM), RAI treatment, external radiotherapy, other thyroid cancer treatment, TSH, recurrent disease during follow-up, and treatment of recurrence. TSH was grouped into three strata according to American Thyroid Association guidelines, where TSH <0.1 mIU/L is moderate to complete suppression, TSH 0.1–0.5 mIU/L is mild suppression, and TSH >0.5 mIU/L is no suppression. 10 Participants were also divided into a prognostically low-risk and high-risk group depending on TNM status and according to European Thyroid Association guidelines: T1 or T2, N0 and M0 were categorized as low risk, while T3 or T4, N1 and M1 were categorized as high risk. 21
Health-related quality of life
To evaluate HRQOL, patients completed the Swedish version of the Short Form-36 Health Survey (SF-36) v2.0 at inclusion and after 1, 3, and 5 years. 22,23 The SF-36 is a multipurpose, standardized patient-reported survey of general health that is well-validated and commonly used in thyroid cancer publications. 15,24 The survey includes 36 questions regarding physical and mental health divided into eight domains: physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health. Responses to each domain were linearly transformed to a score 0–100, with higher scores indicating a higher HRQOL. 23,25 Two summary health components, the physical component summary (PCS) and mental component summary (MCS) scores, were derived by aggregating the results for the eight domains using previously established physical and mental factor score coefficients and transforming resulting summary scores to a t score with a mean of 50 and a standard deviation of 10. 23,25 All eight SF-36 domains contribute to both component scores, with physical functioning, role-physical, bodily pain, and general health contributing more to the PCS, while vitality, social functioning, role-emotional, and mental health contribute more to the MCS. 25
Statistical analysis
The analysis proceeded in SPSS Statistics 28.0.0.0, in accordance with an openly preregistered statistical analysis plan (Open Science Framework identifier: jbkw8). Key sociodemographic and clinical characteristics at inclusion were summarized.
Multiple imputation was used to account for missing data, which allows for unbiased estimates under the assumption that data are missing at random. 26 Linear mixed models were subsequently fitted on the multiply imputed data, with a random intercept and all participants and measurement points included in the model.
In primary analysis, the PCS and MCS scores were regressed, in separate models, on time coded 0–5 to represent the 5 years from inclusion. A two-sided 95% significance test of the time coefficient was conducted.
In secondary analysis, the following 13 variables were added in multivariable linear mixed models: TSH value, age at inclusion, sex, cancer recurrence at any point during follow-up, risk classification, any relevant comorbidity at inclusion, time since diagnosis, and the interaction of the first six listed variables with time. Cancer recurrence, risk classification, and comorbidities were considered potential confounders in the relationship between TSH value and HRQOL. Conditional estimated means of PCS and MCS scores at each time point were presented as a function of recurrence. In a nonplanned auxiliary analysis suggested during the peer-reviewing process, we analyzed the association between RAI dose and HRQOL by repeating the imputation step and refitting the multivariable model with cumulative RAI therapy dose included as a variable.
For each of the two multivariable models (PCS and MCS), a two-sided 95% significance test of the TSH coefficient was conducted to determine whether TSH is predictive of HRQOL regardless of time point. In nonadjusted sensitivity analyses using the imputed data, the correlation between TSH value and each component summary score (PCS and MCS) was calculated for years 1, 3, and 5. In addition, the nonadjusted PCS and MCS scores were each compared over the three TSH suppression strata for year 5 using pairwise t-tests.
Based on multivariable models, estimated means for the PCS score, MCS score, and SF-36 domains were derived for year 5. These were then compared with Swedish norms weighted by age and sex to match the DTC sample. 23 Confidence intervals were not available for these reference means. In a sensitivity analysis, estimated means were therefore also compared with nonweighted reference values where confidence intervals were available. 23 Cohen’s d was calculated in order to evaluate effect sizes regarding PCS and MCS scores where a value of d = 0.2 was regarded as a small effect, d = 0.5 a moderate effect, and d = 0.8 a large effect. 27 For the eight SF-36 domains, the minimally important difference (MID) was used to evaluate if results were clinically significant. 28 The MID is defined as the minimum difference in score that patients would view as an important improvement or deterioration. 28 A difference of at least five points between groups was considered to be a minimal clinically important difference and a difference of 10–20 points a moderate difference. 29
Results
Patient characteristics
Of 487 patients who met the inclusion criteria, 351 (72%) consented to participate in the study by answering the first questionnaire and at least 85% of included patients answered follow-up questionnaires at each time point (Fig. 1). At inclusion, the mean age was 51 years, the majority (71%) of patients were female, and 79% had no recurrence or metastasis of DTC during the 5-year follow-up time (Table 1). Nonresponders at inclusion were younger than responders (mean age, 43 years; p < 0.001), with a similar sex distribution (71% female; p = 0.939).
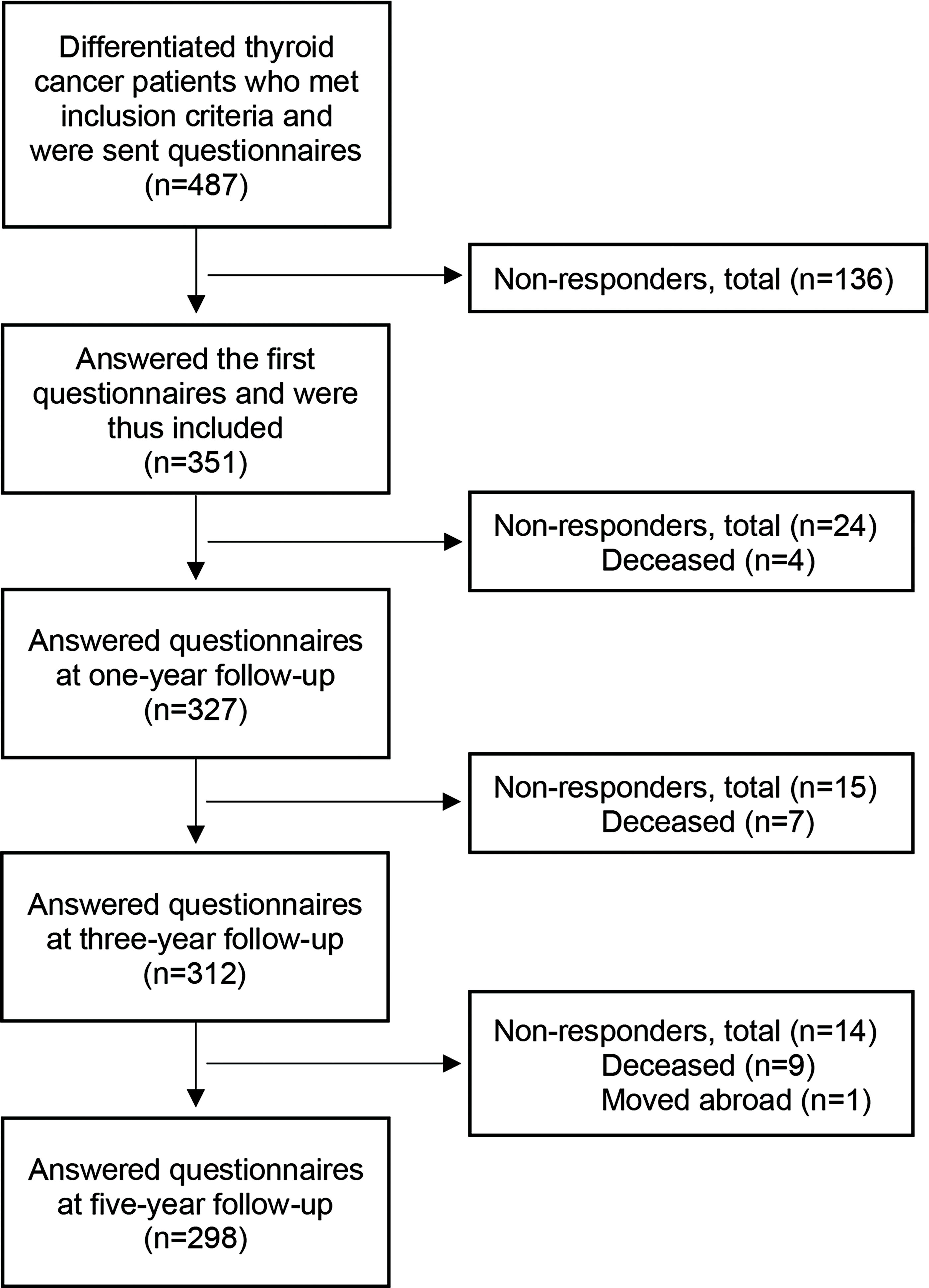
Flowchart showing inclusion of patients with differentiated thyroid cancer and numbers of responders and nonresponders to questionnaires at each year of follow-up.
Patient Characteristics, Treatment, and Recurrence in 351 Swedish Patients with Differentiated Thyroid Cancer
Comorbidities predictive of both HRQOL and TSH: myocardial infarction, hypertension, arrhythmia, osteoporosis, or depression. Reported at inclusion.
Tumor stage assessed after surgery and before radioiodine treatment.
According to European Thyroid Association guidelines.
Primary treatment. Surgery missing: n = 1 (0.3%). Neck dissection missing: n = 2 (0.6%).
Recurrence of DTC during the 5-year follow-up or persistent DTC. Missing: n = 12 (3.4%).
Treatment of recurrent or persistent disease at any time in the 5 years of follow-up after primary DTC treatment. One patient may be treated with several treatment types.
Cumulative RAI therapy dose over the 5 years of follow-up, including primary treatment.
Physical and mental component summary scores derived from aggregated results from the eight specific SF-36 domains transformed to t-scores with a mean of 50 and a standard deviation of 10.
SF-36 domains scored 0–100, with a higher score indicating a higher HRQOL.
DTC, differentiated thyroid cancer; RAI, radioactive iodine; GBq, giga Becquerel; HRQOL, health-related quality of life; TSH, thyroid-stimulating hormone; SF-36, Short Form-36 Health Survey; SD, standard deviation; PCS, physical component summary; MCS, mental component summary.
Change in health-related quality of life up to 5 years
The change in HRQOL, measured as PCS and MCS scores, in the 5 years after DTC treatment was analyzed. The mean PCS score did not change significantly over time (p = 0.069), whereas the mean MCS score improved significantly by an average of 0.61 per year (p < 0.001).
Predictors of health-related quality of life
In multivariable linear mixed models, factors significantly predictive of a lower PCS score in the DTC sample were a higher age at inclusion, female sex, and comorbidities at inclusion (Table 2). Cancer recurrence during follow-up was not significantly associated with a lower PCS score (Table 2, Fig. 2). Factors significantly predictive of a lower MCS score were cancer recurrence, a lower age, female sex, low-risk DTC, comorbidities, and less time since treatment (Table 2, Fig. 2). The only variable found to moderate a change in physical and mental HRQOL over time was age, where for every year lived at inclusion, a reduction of 0.02 would be expected per year for both PCS and MCS scores (Table 2). When cumulative RAI dose was included as a variable in auxiliary analysis, no significant association was found between RAI dose and physical QOL [b (CI): 0.05 (−0.30–0.39); p = 0.794] or its change over time [b (CI): 0.00 (−0.08–0.07); p = 0.908]. RAI dose was also not predictive of mental QOL [b (CI):−0.16 (−0.61–0.28); p = 0.479] or the development of mental QOL over time [b (CI):−0.00 (−0.11–0.11); p = 0.995].
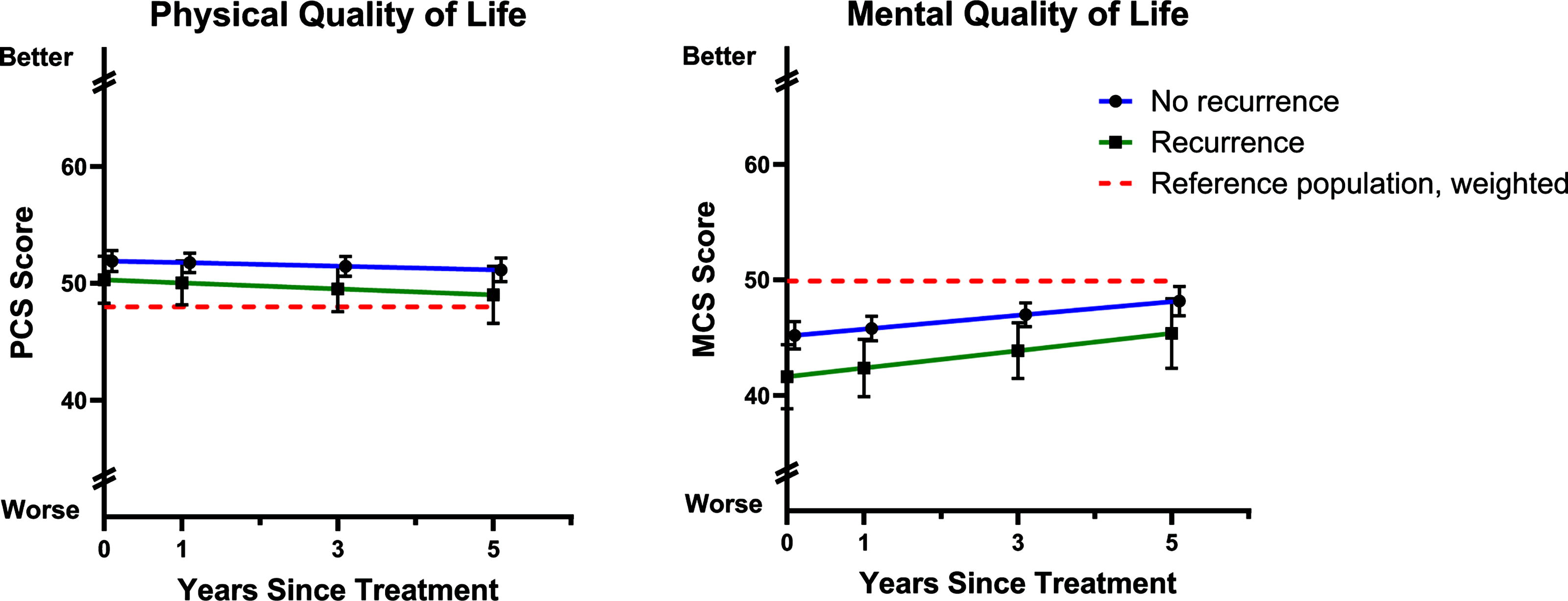
Change in mean health-related quality of life (HRQOL) in terms of the physical (PCS) and mental (MCS) component summary scores, as modeled using multivariable linear mixed models up to 5 years after primary treatment for differentiated thyroid cancer (DTC). Scores were derived from the Short Form-36 Health Survey (SF-36). Error bars represent 95% confidence intervals. Note that the Y axis is broken.
Predictors of Health-Related Quality of Life in 351 Patients with Differentiated Thyroid Cancer as Measured by Physical and Mental Component Summary Scores Derived from Short Form-36, Analyzed as Simple Fixed Effects and Their Interaction with Time Using Multivariable Linear Mixed Models
PCS, physical component summary score; MCS, mental component summary score; DTC, differentiated thyroid cancer; CI, confidence interval; TSH, thyroid-stimulating hormone.
Coding of variables for the analysis as dichotomous (0 or 1) or continuous (range).
Coefficients and p-values derived from multivariable linear mixed models. Bold text indicates p < 0.05.
Cancer recurrence at any point in time during 5-year follow-up.
One or more of the following comorbidities at inclusion: myocardial infarction, hypertension, arrhythmia, osteoporosis, or depression.
These values were centered for the analysis.
Role of TSH suppression
In the multivariable linear mixed models, the level of TSH was not found to be predictive of either PCS or MCS scores when analyzed as a simple fixed effect, and there was also no interaction with time (Table 2). In nonadjusted sensitivity analyses, there were no significant correlations between TSH value and HRQOL outcomes for years 1, 3, or 5 (Supplementary Table S1). There were also no significant differences in PCS or MCS scores when compared over the three TSH suppression strata at year 5 (Supplementary Fig. S1).
Comparison to reference population at 5 years
Estimated means for the PCS score, MCS score, and eight SF-36 domains 5 years after DTC treatment were compared with Swedish reference population means, weighted by age and sex (Table 3, Fig. 3). At 5 years, the mean physical component of HRQOL (PCS) was significantly higher in the DTC sample compared with the reference population, although the effect size was small (d = 0.29). In contrast, the mean mental component of HRQOL (MCS) was significantly lower compared with the reference population, also with a small effect size (d = −0.21). Estimated means of the individual SF-36 domains were also significantly lower with a moderate clinically important difference for general health, vitality, and social functioning and a small clinically important difference for mental health (Table 3).

Health-related quality of life in 351 Swedish patients with differentiated thyroid cancer 5 years after treatment compared with the Swedish general population. Estimated means of health-related quality of life measures derived from Short Form-36 and modeled using multivariable linear mixed models. Error bars represent 95% confidence intervals. Note that the Y axis is broken. DTC, differentiated thyroid cancer; SF-36, Short Form-36 Health Survey; PCS, physical component summary score; MCS, mental component summary score; PF, physical functioning; RP, role-physical; BP, bodily pain; GH, general health; VT, vitality; SF, social functioning; RE, role-emotional; MH, mental health.
Health-Related Quality of Life Measured with Short Form-36 in 351 Swedish Differentiated Thyroid Cancer Patients 5 Years After Treatment Compared with the Swedish General Population
SF-36, Short Form-36 Health Survey; DTC, differentiated thyroid cancer; CI, confidence interval; PCS, physical component summary; MCS, mental component summary; HRQOL, health-related quality of life.
Estimated mean scores at 5 years derived from linear mixed models, compared with weighted and nonweighted Swedish reference population equivalents.
Weighted by age and sex to match the sample of patients with DTC.
Physical and mental component summary scores derived from aggregated results from the eight SF-36 domains transformed to t-scores with a mean of 50 and a standard deviation of 10. A higher score indicates a higher HRQOL.
SF-36 domains scored 0–100, with a higher score indicating a higher HRQOL. Scores printed in bold correspond to a minimum of small clinically significant difference, i.e., ≥5 points, between scores in patients with DTC and weighted Swedish population means.
Cohen’s d. Calculated using the model-implied mean score difference, divided by the pooled standard deviation as based on the observed values of the DTC sample and the nonweighted population estimates. 0.2 = small effect size, 0.5 = moderate effect size, 0.8 = large effect size.
In sensitivity analysis, estimated means were compared with a nonweighted reference population with confidence intervals where the mean age was 43 years and the sex distribution was 52% female. 23 When compared with nonweighted reference population means, estimated means that were significantly different from the weighted reference population remained statistically significant with at least an equally clinically important difference (Table 3).
Discussion
This nationwide prospective cohort study showed that mental QOL improves over time in the 5 years following treatment for DTC. Patients’ HRQOL could not be explained by TSH suppression. Although there were only small differences in physical and mental HRQOL in patients with DTC at 5 years compared with the general population, several individual HRQOL domains primarily related to psychosocial health were clinically meaningfully reduced.
In our study, we found that, on average, mental QOL improves over time, although the average improvement per year was small, while physical QOL does not change up to 5 years after treatment for DTC. In recent years, several longitudinal studies have been conducted examining HRQOL following DTC treatment. These have found that HRQOL scores improve over time following treatment, although these studies have all had a shorter follow-up time than our study. 30 –35 HRQOL in patients with DTC has been found to be lowest in conjunction with treatment, after which HRQOL scores often recover to varying degrees. 30 –33 Similar findings showing an improvement in both physical and mental HRQOL over time following treatment have also been demonstrated in patients with other cancers. 36 –38
Symptoms due to TSH suppression have previously been suggested as a cause of reduced HRQOL in patients with DTC. 39 We found that TSH levels were not predictive of HRQOL or the change in HRQOL over time. Previous studies have also not found a clear association between TSH suppression and HRQOL 15,17,40 or between levels of other thyroid hormones and HRQOL. 41 Restoration to euthyroidism has also not been found to improve HRQOL in patients with a history of DTC. 16
Interestingly, our study found that low-risk DTC was associated with a lower mental QOL than high-risk DTC. While health care providers might perceive low-risk DTC as a favorable diagnosis, patients may still see it as life-threatening and life-changing, and this clash of perceptions may affect mental QOL. 42 It is also possible that the shorter follow-up could contribute to lower mental QOL in low-risk patients with DTC.
Our results indicate that there was a significant difference in physical and mental HRQOL summary measures in patients with DTC compared with the general population 5 years after DTC treatment, but these differences were small and unlikely to be clinically meaningful. However, several more specific HRQOL domains were decreased compared with the reference population at the 5-year follow-up with a clinically important difference, of which differences in general health, vitality, and social functioning were moderate. HRQOL domains that were reduced compared with the reference population were predominantly domains that primarily contributed to the mental component of HRQOL, such as vitality, social functioning, and mental health. 23
Previous studies comparing HRQOL in patients with DTC with the general population have shown mixed results but suggest that there may be a need to primarily address mental QOL concerns. A review by Watt et al. focusing on HRQOL as measured using the SF-36 found that HRQOL was impacted across a broad range of domains compared with reference populations. 43 However, another systematic review by Walshaw et al. including studies using a wider range of HRQOL instruments concluded that a majority of studies found that HRQOL in patients with DTC was good compared with normative populations. 15
In individual studies, Hoftijzer et al. not only found that HRQOL was reduced several years after diagnosis but also that fatigue, depression, and anxiety were significantly worse in patients with DTC compared with controls. 40 Moreover, Lee et al. showed that patients with DTC had a decreased HRQOL compared with the general population and that anxiety, depression, and fatigue were the strongest determinants for most HRQOL domains. 44 Another study by Husson et al. found that thyroid cancer survivors had significantly lower HRQOL scores with regard to both physical and psychosocial functioning than the general population in the long term. 5 Furthermore, the SF-36 domains that predominantly contribute to MCS that were decreased in our study were also found to be decreased 14–17 years after diagnosis compared with the general population in a previous study of long-term HRQOL in Swedish patients with DTC, 4 suggesting that these aspects of HRQOL may remain affected in patients with DTC many years after treatment. That fatigue and mental health issues are important contributors to impacted HRQOL in DTC survivors is also reflected in the finding by Singer et al. that patients with thyroid cancer themselves rank fatigue and psychosocial issues as among the most relevant QOL issues they face. 45 Our findings in the context of these previous studies suggest that health care providers involved in the care of patients with DTC should be educated in asking about and recognizing symptoms related to psychosocial issues and fatigue, so that support can be offered when indicated. Such support may include being referred to psychological and behavioral interventions that have previously been shown to have positive effects on HRQOL in patients with DTC. 46,47
Strengths and limitations
Strengths of this study included the large number of patients with DTC and the 5-year longitudinal follow-up, a longer follow-up time than previous longitudinal studies. Furthermore, we conducted a nationwide study where patients were included from all Swedish clinics treating DTC with RAI. There was also a low rate of missing data, with at least 85% of patients completing each assessment point. In addition, the use of state-of-the-art statistical modeling techniques allowed us to account for missing data, and we were able to fit multivariable models of change in HRQOL over time using data from all patients with DTC in the sample.
A limitation in the study was the possible self-selection of patients who chose to participate in the study versus those who did not. This may be a potential source of selection bias that could affect the external validity of the results. Although we had data regarding age and sex in nonresponders, the lack of more extensive information about nonresponders is a limitation. However, we could not collect additional data regarding nonresponders owing to Swedish ethical legislation since nonresponse was taken as nonconsent to participate in the study. Loss to follow-up may have been another source of bias, although a response rate of ≥85%, as in this study, should be considered acceptable during a long-term follow-up. Another important limitation is that we could not obtain accurate confidence intervals for the weighted Swedish reference population mean estimates. Instead, we regarded these as true population values, which may have impacted the conclusion of comparisons to the DTC group at year 5. Having said this, we deem it unlikely that the large discrepancies seen in the specific domains of general health, vitality, social functioning, and mental health were driven entirely by the modeling approach. In terms of the physical and mental component tests, there was likely no clinically important difference regardless. Our findings are also corroborated by the sensitivity analyses versus nonweighted population means, for which we could obtain confidence intervals. Another limitation was that the general HRQOL questionnaire SF-36 was used rather than a validated DTC specific HRQOL questionnaire since this did not exist in Swedish when the study was initiated, with the risk that aspects of HRQOL specific to patients with DTC may not be captured. In our study we have also only included patients planned for RAI therapy, meaning that our results may not be generalizable to patients with DTC not treated with RAI. Furthermore, we did not have data on surgical complications and therefore do not know how these may have affected HRQOL. However, the rate of surgical complications after thyroid surgery in Sweden is low and unlikely to have a significant effect on long-term HRQOL. 48,49
Conclusion
To the best of our knowledge, this is the largest longitudinal study of HRQOL in patients with DTC with the longest follow-up time. We found that although mental health (measured as MCS) improves with time after DTC treatment, the HRQOL domains of general health, vitality, social functioning, and mental health are significantly lower in patients with DTC compared with the general population 5 years after treatment. Moreover, lower HRQOL in patients with DTC is not explained by TSH suppression. The study’s results suggest that patients with DTC should routinely be screened with regard to psychosocial health issues and fatigue during follow-up and be offered support in the case of significant symptoms in order to optimize well-being.
Footnotes
Acknowledgments
The authors want to express their sincere gratitude to all patients who participated in the study. Investigators who included patients: Helene Hörberg, Mälarsjukhuset Eskilstuna; Maria Annerbo, County Hospital Falun; Åsa Bergström Morelius, County Hospital Gävle; Johanna Svensson, Sahlgrenska University Hospital; Viveka Bergman, Linköping University Hospital; Åsa Harnesk, Karlstad Central Hospital; Pernilla Asp, Skåne University Hospital; Petra Flygare, County Hospital Sundsvall; Maria Sandström, University Hospital of Umeå; Tanweera Khan, Uppsala University Hospital; Karin Hubertsson, Västerås Central Hospital; and Kristina Engström, Örebro University Hospital.
Author Contribution Statement
Conceptualization: J.W., E.A., L.B.B., C.I.L., C.H.; Methodology: J.W., E.A., L.B.B., C.I.L., C.H.; Software: J.W., E.A., C.H.; Validation, J.W., E.A.; Formal analysis: J.W., E.A., C.H.; Investigation: J.W., E.A., C.I.L., C.H.; Resources: E.A., L.B.B., C.I.L., C.H.; Data Curation: J.W., E.A., C.H.; Writing—Original Draft: J.W., E.A., L.B.B., C.I.L., C.H.; Writing—Review & Editing: J.W., E.A., L.B.B, C.I.L., C.H.; Visualization: J.W., E.A., L.B.B, C.H.; Supervision: E.A., L.B.B., C.H.; Project administration: J.W., C.H.; Funding acquisition: E.A., L.B.B, C.I.L., C.H. All authors revised the article and approved the final submitted version.
Author Disclosure Statement
The authors have no actual or potential conflicts of interest to disclose.
Funding Information
This study was supported by grants from The Sjöberg Foundation (JW),
Supplementary Material
Supplementary Data