
Abstract
Background:
For patients with thyroid cancer, distant metastasis is a significant predictor of poor outcome. Since distant metastasis occurs in less than 10% of patients with differentiated thyroid cancer, correlates of survival in this vulnerable patient population remain understudied. This study aimed to identify prognostic groups among patients with differentiated thyroid cancer and distant metastases and to determine the role of, and interactions between, patient and tumor characteristics in determining survival.
Methods:
We identified adult patients diagnosed with differentiated thyroid cancer with distant metastases from the U.S. SEER-17 cancer registry (2010–2019). Analyses were performed using Cox proportional hazards regression, survival trees, and random survival forest. Relative importance of patient and tumor factors important for disease-specific and overall survival was assessed based on the random survival forest analyses.
Results:
Cohort consisted of 2411 patients with differentiated thyroid cancer with distant metastases followed for a median of 62 months. Most common histopathologic subtype (86.0%) was papillary thyroid cancer, and the most common sites of distant metastasis were the lungs (33.7%) and bone (18.9%). Cox proportional hazards model illustrated significant associations between survival and the following: patient age (p < 0.001), tumor size (p < 0.01), and site of distant metastasis (p < 0.05). Survival tree analyses identified three distinct prognostic groups based on disease-specific survival (DSS) (5-year survival of the prognostic groups was 92%, 64%, and 41%; p < 0.001) and four distinct prognostic groups based on overall survival (OS) (5-year survival of the prognostic groups was 96%, 84%, 57%, and 31%; p < 0.001). The first split in the survival trees for DSS and OS was by age at diagnosis (≤57 years vs. ≥58 years) with subsequent splits based on presence/absence of lung metastases, tumor size (≤4 cm vs. >4 cm), and patient age. A total of 558 patients (23.1%) died from thyroid cancer, and 757 patients (31.4%) died from all causes during the study period.
Conclusions:
This study identifies distinct prognostic groups for patients with differentiated thyroid cancer with distant metastases and highlights the importance of patient age, lung metastases, and tumor size for determining both disease-specific and overall survival. These findings inform risk stratification and treatment decision-making in this understudied patient population.
Introduction
Thyroid cancer has the ninth highest cancer incidence worldwide. 1 While the overall prognosis for most patients with thyroid cancer is excellent, clinical outcome is heterogeneous and influenced by factors such as patient age, tumor histology, and presence of metastasis. 2 –5 At the time of diagnosis, for patients with thyroid cancer in the United States, five-year survival rates can range from 53.5% for distant disease to 99.9% for localized disease. 6
Since distant metastasis, which is generally associated with worse prognosis, occurs in less than 10% of patients with differentiated thyroid cancer, 7 correlates of survival in this vulnerable patient population remain understudied. Historically, patients with metastatic differentiated thyroid cancer had limited treatment options. Since 2011, at least three targeted systemic therapies have been approved by the Food and Drug Administration for the treatment of locally advanced or metastatic, radioiodine-refractory differentiated thyroid cancers. 3 In this context, it is important that clinicians are able to risk stratify their thyroid cancer patients with distant metastases and are able to identify those patients at risk for worse outcome who may benefit from early initiation of novel systemic therapies or enrollment in clinical trials. Thus, the development of comprehensive prognostic groups for thyroid cancer patients with distant metastases is important to tailor treatment to disease severity.
This study aimed to identify prognostic groups among adult patients with differentiated thyroid cancer who presented with distant metastases and to determine the role of, and interactions between, patient and tumor characteristics in determining survival. The Surveillance, Epidemiology, and End Results Program (SEER) database, which collects comprehensive cancer incidence and survival data from population-based cancer registries from 22 geographic areas that are representative of the demographics of the entire United States population and is considered the premier source of cancer statistics in the United States, 8 was used to identify the cohort of thyroid cancer patients. We hypothesized that age at time of thyroid cancer diagnosis and tumor size would be the primary factors predicting disease-specific and overall survival.
Methods
Data source and study population
Cases of adult patients (age 18 years and older) with a diagnosis of differentiated thyroid cancer (ICD-9-CM code 193 and/or ICD-10-CM code C73) with distant metastases reported at initial staging (based on the “combined summary stage (2004+)” variable) were extracted from the SEER-17 cancer registry (2010–2019), which collects data from 17 geographic areas. 9 Pathologically confirmed primary neoplasms of the thyroid gland were identified based on International Classification of Diseases for Oncology, third edition [ICD-O-3] histological codes 8050, 8260, 8290, 8330, 8331, 8335, 8339, 8340–8344, 8350, 8450, 8452, 8453, and 8460. Distant metastases were characterized as having disease extension into distant lymph nodes and/or distant sites such as bone, brain, lung. Patients without complete records of variables and survival outcomes were excluded.
The University of Michigan Institutional Review Board determined this study to be of “not regulated” status based on its use of publicly available data set (HUM00234550).
Variables
We extracted the following patient variables from the SEER database: age at time of thyroid cancer diagnosis, sex, race and ethnicity, county-level median household income, and county type (metropolitan vs. nonmetropolitan). We also extracted information on the following tumor characteristics: histological subtype (papillary thyroid cancer, follicular thyroid cancer, and oncocytic carcinoma of the thyroid), size of the primary tumor (categorized as: less than 2 cm, between 2 and 4 cm, greater than 4 cm), and site of distant metastases (bone, brain, liver, lung, and other). Treatment variables included surgery type (no surgery, lobectomy and/or isthmectomy, total thyroidectomy, and other), radiation therapy (none or unknown, radioactive iodine, and other), and chemotherapy (received vs. not received/unknown). Disease-specific survival (DSS) was defined as time from thyroid cancer diagnosis to death from thyroid cancer. Overall survival (OS) was defined as time from thyroid cancer diagnosis to death due to any cause. Follow-up was defined as the time from thyroid cancer diagnosis until the patient is censored, with death from any cause treated as a censoring event.
Statistical analyses
The primary endpoints were DSS and OS. We used Cox proportional hazards regression to model DSS and OS (2 separate models) as a function of the patient and tumor characteristics. Since cancer staging models, including the American Joint Committee on Cancer (AJCC) staging for thyroid cancer, are performed at the time of diagnosis and based on only patient (i.e., age) and tumor characteristics, 4,10,11 we did not include treatment characteristics as a variable in the Cox proportional hazards model. Hazard ratio (HR) and corresponding confidence interval (CI) were calculated. p-Values of <0.05 were considered statistically significant.
We also used tree-based methods, which is a form of binary recursive partitioning that has previously been used in different patient cohorts by our team and others (Supplementary Data S1). 10,12 –15 These methods offer a natural way of “binning” patients, allowing comparison of risk estimates across the bins. Furthermore, they capture nonlinear and heterogeneous effects and can automatically detect interactions (i.e., without the need to having the interactions specified a priori). We performed survival tree analyses on DSS and OS to construct distinct prognostic groups. 15 –17 Kaplan–Meier survival curves were generated for each distinct prognostic group and compared using two-tailed log-rank tests. Five-year survival rates were calculated as summary measures for each final prognostic group.
Next, we performed a random survival forest analysis on the same data. A random survival forest is an ensemble (“forest”) of unpruned survival trees where the prediction is made by averaging the individual predictions across all trees in the ensemble. 18,19 Each tree is grown using bootstrap resamples of the original data, using random feature selection in the tree induction process. We grew 500 trees in both random forests of DSS and OS and calculated Breiman–Cutler variable importance. Variable importance was used to rank the variables in terms of their relative importance to survival.
All analyses were performed using the statistical software R. For the survival tree, random survival forest, and Cox regression analyses, we used the “rpart,” “randomForestSRC,” and “survival” packages in R, respectively. 20 –22
Results
The final patient cohort consisted of 2411 patients with differentiated thyroid cancer with distant metastases followed for a median of 62 months. Table 1 illustrates the descriptive characteristics and results from the Cox proportional hazard regression analyses for the association of patient and tumor characteristics with DSS and OS. The median patient age at time of thyroid cancer diagnosis was 62 years (range 18–99). Most patients were female (58.2%), White (77.1%), non-Hispanic (76.4%), and resided in a metropolitan area (90.7%) with a county-level median household income of greater than $60,000 (74.7%). The most common histopathologic subtype (86.0%) was papillary thyroid cancer, and the most common sites of distant metastasis were the lungs (33.7%) and bone (18.9%) (Table 1). Most patients underwent a total thyroidectomy (84.1%) and received adjuvant radioactive iodine therapy (58.2%). A total of 558 patients (23.1%) died from thyroid cancer, and 757 patients (31.4%) died from all causes during the study period.
Descriptive Characteristics and Results from the Cox Proportional Hazard Regression Analyses for the Association of Patient and Tumor Characteristics with Disease-Specific Survival and Overall Survival
There was a statistically significant association between survival and the following variables: age at time of thyroid cancer diagnosis, size of the primary tumor, and site of distant metastasis (Table 1). Older patient age (continuous variable measured in one-year increments) was significantly associated with worse DSS (HR 1.05, 95% CI 1.04–1.05) and worse OS (HR 1.05, 95% CI 1.05–1.06). Size of the primary tumor was also an important predictor for DSS (compared with <2 cm tumors, HR for 2–4 cm tumors was 1.47 [95% CI 1.11–1.94] and HR for >4 cm tumors was 2.91 [95% CI 2.24–3.79]) and OS (compared with <2 cm tumors, HR for 2–4 cm tumors was 1.42 [95% CI 1.14–1.78] and HR for >4 cm tumors was 2.41 [95% CI 1.94–3.00]). Distant metastases to the bone (compared with patients with non-bone distant metastases, HR 1.51, 95% CI 1.23–1.85), brain (compared with patients with non-brain distant metastases, HR 3.01, 95% CI 2.07–4.38), liver (compared with patients with non-liver distant metastases, HR 1.56, 95% CI 1.04–2.36), and lung (compared with patients with non-lung distant metastases, HR 2.06, 95% CI 1.73–2.45) were important predictors for DSS. Similarly, for OS, distant metastases to bone (HR 1.37, 95% CI 1.14–1.64), brain (HR 2.71, 95% CI 1.91–3.84), and lung (HR 1.67, 95% CI 1.44–1.94) were important predictors of worse survival (Table 1).
Disease-specific survival (DSS) survival tree
Figure 1 shows the survival tree for DSS. At each level of the tree, we show the best splitter (covariate with cutoff point). Circles denote terminal groups in the tree. For each terminal group, we report the five-year DSS rate, the total number of patients in that terminal group, and the crude number of patients who died from thyroid cancer in that terminal group. The first split in the tree was by age ≤57 years versus ≥58 years. All subsequent splits were based on presence/absence of lung metastases, age, and tumor size. There are three prognostic groups. Group I (terminal nodes enclosed by solid black line), which has the highest five-year DSS, contains patients aged ≤57 years with no lung metastases and tumor size ≤4 cm; aged ≤57 years with no lung metastases and tumor size >4 cm; aged ≤39 years with lung metastases; and aged 58–72 years with no lung metastases and with tumor size ≤4 cm. Group II (terminal nodes enclosed by dashed black line) contains patients aged 40–57 years with lung metastases; aged 58–72 years with lung metastases and tumor size ≤4 cm; aged ≥73 years with tumor size ≤4 cm; and aged 58–82 years with no lung metastases and with tumor size >4 cm. Group III (terminal nodes enclosed by dotted black line), which has the worst five-year DSS, includes patients aged 58–82 years with lung metastases and tumor size >4 cm and patients aged ≥83 with tumor size >4 cm. Sensitivity analysis of patients aged ≤80 years who had undergone total thyroidectomy and received adjuvant radioactive iodine therapy (total analytic n = 1275) yielded similar results with three prognostic groups and splits in the survival tree based on age at time of thyroid cancer diagnosis and presence/absence of lung metastases, although tumor size was no longer an important prognostic factor (Supplementary Fig. S1).

Disease-Specific Survival (DSS) Prognostication in Patients with Differentiated Thyroid Cancer and Distant Metastases. The first split in the tree was by age ≤57 years versus ≥58 years. All subsequent splits were based on presence/absence of lung metastases, age at diagnosis, and tumor size. There are three distinct prognostic groups. For each terminal group, we report the five-year DSS rate (5YR), the 95% confidence interval (in parentheses), the total number of patients in that terminal group
Based on the random survival forest analysis, patient age at time of thyroid cancer diagnosis was most important in determining DSS, followed by lung metastases and tumor size. All other variables had a smaller role in predicting DSS.
Figure 2 shows the Kaplan–Meier curve for DSS for each of the three distinct prognostic groups identified by survival tree analysis (p < 0.001). Group I conferred the most favorable outcome, and group III had the worse survival. Five-year survival in group I was 92% (95% CI: 90%, 94%) compared with 64% (95% CI: 61%, 68%) and 41% (95% CI: 34%, 48%) in groups II and III, respectively. Table 2 lists these three prognostic groups and their respective 5-year DSS.
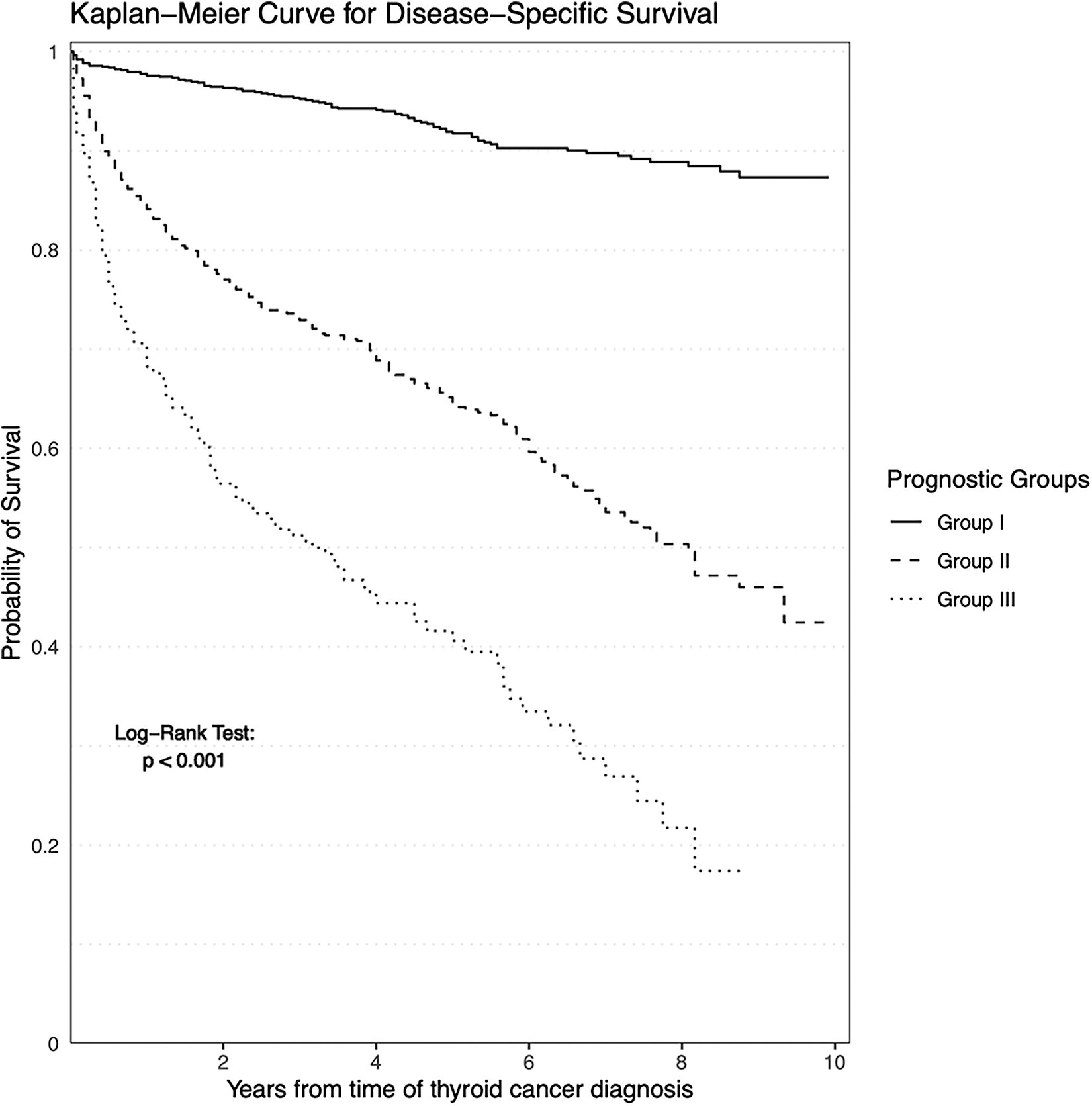
Kaplan–Meier curve illustrating the disease-specific survival for each of the three distinct prognostic groups of patients with differentiated thyroid cancer and distant metastases identified by survival tree analysis. Five-year survival in group I was 92% compared with 64% and 41% in groups II and III, respectively.
Prognostic Groups for Disease-Specific Survival (DSS)
In terms of the treatment received, most patients in all three prognostic groups underwent total thyroidectomy (93% in group I, 82% in group II, and 59% in group III). Postoperatively, most patients in groups I and II were treated with radioactive iodine therapy (69% in group I and 52% in group II compared with 36% in group III).
Overall Survival (OS) Survival Tree
Figure 3 shows the survival tree for OS. The first split in the tree was by age ≤57 years versus ≥58 years. All subsequent splits were based on presence/absence of lung metastases, age, and tumor size. There are four prognostic groups as follows: Group I (terminal nodes enclosed by solid black line), which has the highest five-year OS, contains patients aged ≤41 years with no lung metastases. Group II (terminal nodes enclosed by dashed black line) contains patients aged 42–57 years with no lung metastases; aged ≤39 years with lung metastases; and patients aged 58–72 years with no lung metastases and with tumor size ≤4 cm. Group III (terminal nodes enclosed by dotted black line) includes patients aged 40–57 years with lung metastases; aged 58–72 years with lung metastases and with tumor size ≤4 cm; aged 58–72 years with no lung metastases and with tumor size >4 cm; and patients aged ≥73 years with tumor size ≤4 cm. Group IV (terminal nodes enclosed by alternating dashed and dotted black line), which has the worst five-year OS, includes patients aged 58–72 years with lung metastases and with tumor size >4 cm and patients aged ≥73 years with tumor size >4 cm. Sensitivity analysis of patients aged ≤80 years who had undergone total thyroidectomy and received adjuvant radioactive iodine therapy (total analytic n = 1275) yielded three prognostic groups with splits in the survival tree similarly based on age at time of thyroid cancer diagnosis, although presence/absence of lung metastases and tumor size were no longer important prognostic factors (Supplementary Fig. S2).
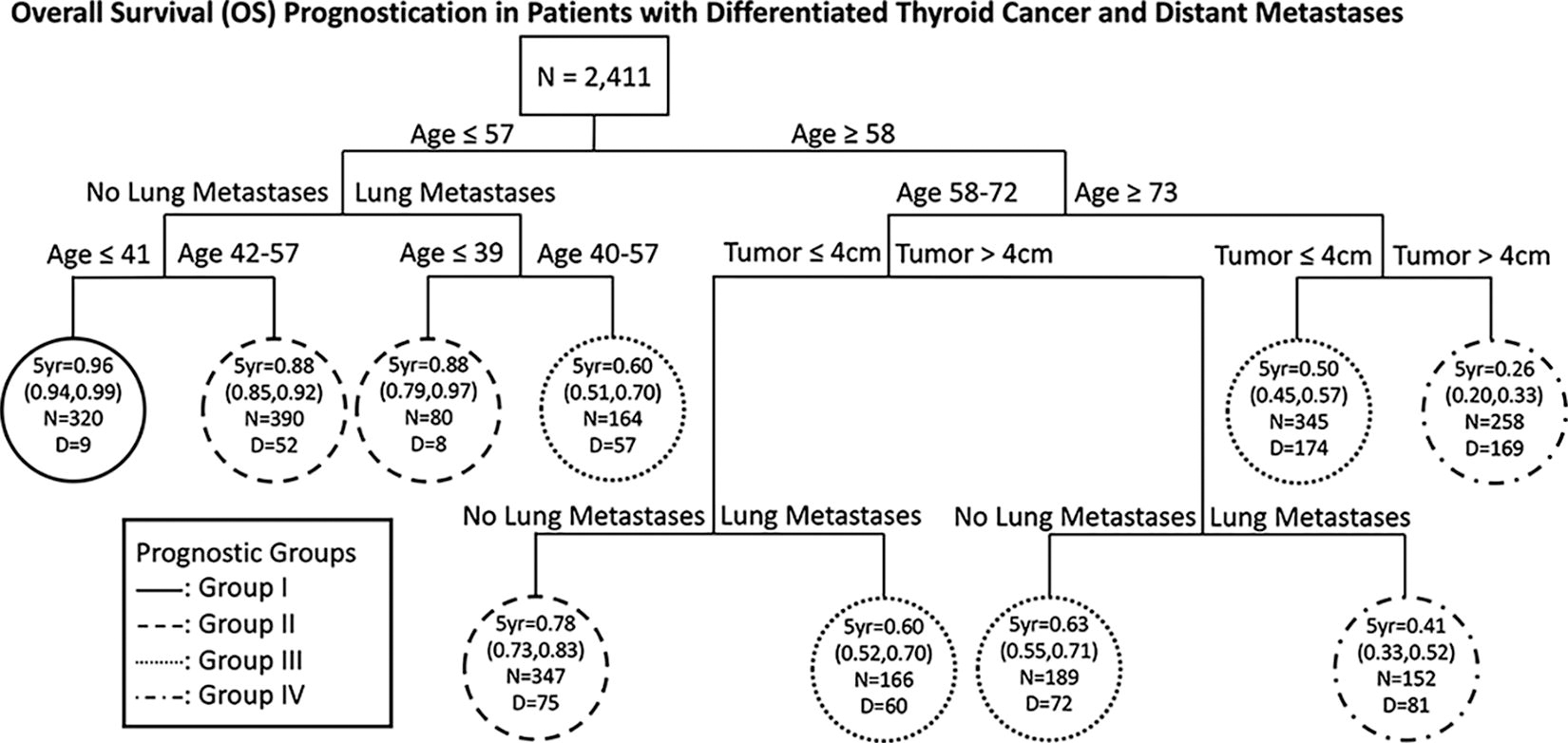
Overall Survival (OS) Prognostication in Patients with Differentiated Thyroid Cancer and Distant Metastases. The first split in the tree was by age ≤57 years versus ≥58 years. All subsequent splits were based on presence/absence of lung metastases, age at diagnosis, and tumor size. There are four distinct prognostic groups. For each terminal group, we report the five-year OS rate (5YR), the 95% confidence interval (in parentheses), the total number of patients in that terminal group
Based on the random survival forest analysis, the most important factors in determining OS were patient age at time of thyroid cancer diagnosis, followed by lung metastases and tumor size. All other variables had a smaller role in predicting OS.
Figure 4 shows the Kaplan–Meier curve for OS for each of the four distinct prognostic groups identified by survival tree analysis (p < 0.001). Group I conferred the most favorable outcome, and group IV had the worse survival. Five-year overall survival in group I was 96% (95% CI: 94%, 99%) compared with 84% (95% CI: 81%, 87%), 57% (95% CI: 53%, 61%), and 31% (95% CI: 26%, 37%) in groups II, III, and IV, respectively. Table 3 lists these four prognostic groups and their respective 5-year OS.
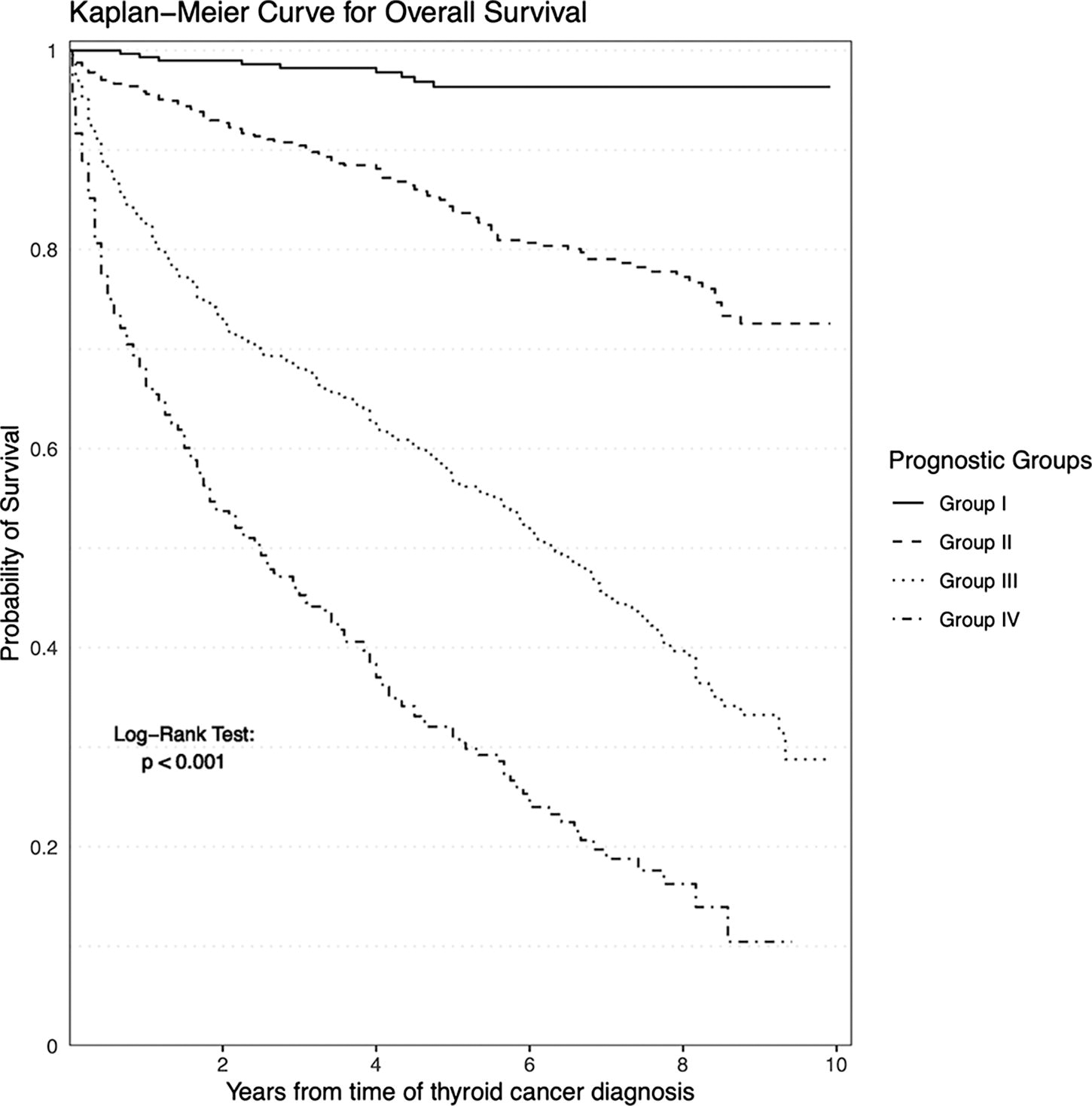
Kaplan–Meier curve illustrating the overall survival for each of the four distinct prognostic groups of patients with differentiated thyroid cancer and distant metastases identified by survival tree analysis. Five-year survival in group I was 96% compared with 84%, 57%, and 31% in groups II, III, and IV, respectively.
Prognostic Groups for Overall Survival (OS)
In terms of the treatment received, most patients in all four prognostic groups underwent total thyroidectomy (94% in group I, 92% in group II, 83% in group III, and 63% in group IV). Postoperatively, most patients in groups I–III were treated with radioactive iodine therapy (73% in group I, 68% in group II, and 54% in group III compared with 35% in group IV).
Discussion
Our population-based study of more than 2000 patients with differentiated thyroid cancer and distant metastases at the time of diagnosis identifies distinct prognostic groups for DSS and OS and illustrates the importance of patient age at time of thyroid cancer diagnosis, lung metastases, and tumor size to both disease-specific and overall survival.
Unique from many other studies, not only does our study use Cox proportional hazards model to identify variables that have a global effect on prognosis, such as presence of brain metastases, we also use survival tree analysis to identify variables that have a subgroup effect on DSS and OS. For example, the presence of lung metastases has a subgroup effect on prognosticating DSS in patients aged 58–72 years with tumor size of ≤4 cm, as well as for other prognostic groups. These findings have important clinical implications as they provide more granular data for risk stratification and treatment decision-making for this understudied patient population.
Patient age at time of thyroid cancer diagnosis is a well-established prognostic factor in thyroid cancer survival. 23 The eighth edition of the AJCC staging system for differentiated thyroid cancer utilizes an age cutoff of 55 years such that patients aged <55 years with distant metastases (M1) have stage II disease and patients aged ≥55 years with distant metastases have stage IVB disease. 4 Consistent with this established paradigm and the age cutoff used by the AJCC staging system, our study identified patient age at time of thyroid cancer diagnosis as one of the most important factors in determining both disease-specific and overall survival with the first split in both survival trees by age ≤57 years and ≥58 years. In addition, our study findings suggest that for thyroid cancer patients with distant metastases, utilizing age as a continuous variable and providing more than one age cutoff category may provide a greater level of granularity in prognostication and better inform clinicians when risk stratifying patients as part of the treatment decision making process. For example, as per the AJCC staging system, both a 72-year-old patient with primary tumor size of ≤4 cm and non-lung metastases and an 83-year-old patient with primary tumor size of >4 cm and distant metastases would have stage IVB disease, which is associated with a 10-year DSS of <50%. 4 In contrast, according to our study findings, the 72-year-old patient would have a five-year DSS of 86%, whereas the 83-year-old patient would have a five-year DSS of 27%. Furthermore, patients younger than 55 years with distant metastases have AJCC stage II disease, which is associated with a 10-year DSS of 85–95%. 4 In comparison, according to our study findings, while patients aged ≤39 years with lung metastases have a five-year DSS of 89%, patients aged 40–57 years with lung metastases have a significantly lower five-year DSS of 62%.
In our study cohort of patients with differentiated thyroid cancer, the most common site of distant metastasis was the lungs (33.7%) followed by the bone (18.9%), which is consistent with prior studies. 24 –26 Furthermore, our study highlights the relative importance of lung metastases in determining disease-specific and overall survival, especially for certain subgroups of patients. Prior studies have reported variable prognostic effect of lung metastases among patients with thyroid cancer, with some, 27,28 but not all, studies similarly reporting an association with worse prognosis. 24,26 This heterogeneity is likely due to differences in the study methodology used. Unique from traditional methodologies such as Cox proportional hazards regression, the survival tree and random survival forest methodology used in this study allow for the identification of prognostic groups, assessment of relative importance of multiple factors in predicting survival, and discovery of interactions between multiple factors included in the analyses.
Our study has several strengths, including a relatively large population-based cohort of patients with metastatic differentiated thyroid cancer; use of methodologies that permit for the assessment of interactions between multiple factors; and inclusion of a comprehensive set of patient, tumor, and treatment variables. The sensitivity analyses performed is another strength of the study although the new patient cohort was smaller, which likely contributed to differences in the subsequent results. The study’s limitations should also be noted. First, inherent to all national cancer registries, although it is comprehensive, SEER lacks some granular details such as the molecular phenotype of the thyroid cancer that may have provided additional insight into the mechanism by which lung metastases influenced survival outcomes. Second, SEER lacks additional information on the volume of distant metastases, whether patients had multiple sites of distant metastases, extent of iodine-avid disease, and use of systemic therapeutics, including tyrosine kinase inhibitors, which may have provided additional insight into the role of treatment differences on the different prognostic groups. 29 –32
Our study has important clinical implications for patients and clinicians. The distinct prognostic groups for disease-specific and overall survival can be used to inform treatment decision-making and how best to tailor long-term surveillance to disease severity. For example, patients with characteristics associated with poor survival may be candidates for more intensive treatment with closer follow-up and the potential for earlier initiation of systemic treatment options. Conversely, patients with characteristics associated with excellent survival may be candidates for less intensive treatment and may be able to transition their long-term surveillance from specialists to primary care physicians earlier than patients with characteristics associated with poor survival. Furthermore, our study’s identification of those patients at highest risk for poor survival outcomes can be used to influence clinicians’ recommendations about whom to recruit and enroll into thyroid cancer clinical trials.
Footnotes
Acknowledgments
Nada Fanous, MD, assisted with background research as part of the study design. Arya Bose participated in the preliminary analysis for this study.
Author’s Contributions
D.W.C.: conceptualization, data interpretation, and writing (original draft). G.C.: data curation, formal analysis, data interpretation, and writing (review and editing). F.P.W.: data interpretation and writing (review and editing). C.M.V.: conceptualization, data interpretation, and writing (review and editing). M.R.H.: conceptualization, methodology, data interpretation, and writing (original draft). M.B.: conceptualization, methodology, data analysis and interpretation, and writing (original draft).
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Statement
D.W.C. is supported by the
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Data S1