
Abstract
Background:
Long-term management of intermediate- and high-risk differentiated thyroid cancer (DTC) involves thyrotropin (TSH) suppression with thyroid hormone to prevent potential stimulation of TSH receptors on DTC cells, leading to tumor growth. However, the current guidelines recommending TSH suppression are based on low- to moderate-quality evidence.
Methods:
We performed a systematic review and meta-analysis of studies evaluating the role of TSH suppression in intermediate- and high-risk DTC patients (≥18 years) treated as per regional guideline-based therapy with a follow-up duration of 5 years (PROSPERO #252396). TSH suppression was defined as “below normal reference range” or, when known, <0.5 mIU/L. Primary outcome measures included (i) composite of progression-free survival (PFS), disease-free survival (DFS), and relapse-free survival (RLFS), and (ii) composite of disease-specific survival (DSS), and overall survival (OS). Secondary outcome included a composite of cardiac or skeletal adverse events. All outcomes and comparisons were represented as TSH suppression versus TSH nonsuppression. Randomized controlled trials, cohort studies, and case–control studies were included for analysis. Pooled hazard ratio (HR) and 95% confidence interval (CI) were calculated using random-effects model.
Results:
Abstract screening was performed on 6,369 studies. After the exclusion of irrelevant studies and full-text screening, nine studies were selected for the final meta-analysis. Based on seven studies (3,591 patients), the composite outcome of PFS, DFS, and RLFS was not significantly different between TSH suppression and nonsuppression groups (HR: 0.75; 95% CI: 0.48–1.17; I 2 = 76%). Similarly, a DSS and OS composite outcome assessment based on four studies (3,616 patients) did not favor TSH suppression (HR: 0.69; 95% CI: 0.31–1.52; I 2 = 88%). Even after excluding studies of lower quality, the primary outcomes were not significantly different between the TSH suppression and nonsuppression cohorts. The secondary outcome, obtained from two studies (1,294 patients), was significantly higher in the TSH-suppressed groups (HR: 1.82; 95% CI: 1.30–2.55; I 2 = 0%). Significant study heterogeneity was noted for primary outcomes.
Conclusion:
TSH suppression in intermediate- and high-risk DTC may not improve survival outcomes but may increase the risk of secondary complications. However, the limited evidence and study heterogeneity warrant cautious interpretation of our findings.
Registration:
PROSPERO #252396.
Introduction
Differentiated thyroid cancer (DTC) has been categorized into a low-, intermediate-, and high-risk malignancy based on its likelihood of development of persistent/recurrent disease varying from <5%, through 5–20%, to >20–30%, respectively. 1 The initial treatment for DTC is tailored toward respective risk of recurrence and includes thyroidectomy (lobectomy, hemithyroidectomy, near total or total thyroidectomy), and in several instances, a lymph node dissection (central and/or lateral neck groups), and radioactive iodine (RAI) therapy, with the latter often utilized for patients with intermediate or high-risk patients. 1
One of the main stays of managing intermediate- and high-risk DTC is suppression of thyrotropin (TSH). According to the American Thyroid Association 2016 guidelines, a TSH suppression level of 0.1–0.5 mIU/L is recommended for intermediate-risk DTCs (weak recommendation, low-quality evidence), while a TSH suppression level of <0.1 mIU/L is recommended for high-risk DTCs (strong recommendation, moderate-quality evidence). 1 As evidenced in the guidelines, the quality of evidence for TSH suppression in intermediate-risk DTC is poor, and there is no clear evidence to suggest TSH suppression in this risk category. 1,2 For high-risk DTC, there is evidence from observational and cohort studies that TSH suppression may improve survival outcomes in DTC, although these still constitute as moderate-quality evidence. 2 –5 Since the publication of the guidelines, more recent cohort studies have identified that the benefits of aggressive TSH suppression on survival outcomes in DTC may in fact be questionable. 6,7 The rationale for TSH suppression is based on the fact that DTC cells express TSH receptors, and TSH can have a trophic effect on these cells. 8 However, the data supporting the mechanistic role of TSH in stimulating tumor growth is mainly based on in vitro studies. 9 Moreover, TSH also can act as a differentiation stimulus promoting synthesis of thyroglobulin, and sodium–iodide symporter. TSH requires the action of other growth factors, such as insulin, insulin-like growth factor-1, and epidermal growth factor to potentiate its growth-promoting effects, with discrepant downstream effects being noted in different in vitro models. 10 –12 Supraphysiologic doses of thyroid hormone (TH) are often necessary to achieve TSH suppression. 1 TH by itself could potentially act as a mitogen and promote the growth of tumor cells. TH has been shown to activate MAPK/ERK1/2 pathway through ανβ3 integrin receptors in various cancer cell lines. 13,14 Triiodothyronine can promote proliferation in papillary thyroid carcinoma cell lines through upregulation of cyclin D1 expression. 15 Of more clinical relevance is the increased risk of adverse effects from excess TH, such as cardiac (arrhythmias, atrial fibrillation, angina, myocardial infarction), or bone (osteopenia, osteoporosis, fractures) complications. 2,16,17
Therefore, the current clinical data regarding the optimal TSH level in DTC patients following initial therapy are equivocal and the guidelines at this time are more reliant on expert opinion due to suboptimal quality of evidence. Therefore, we aimed to perform a systematic review and meta-analysis that may serve future guidelines on the role of TSH suppression in the management of DTC. The objective of our study was to assess the association between TSH suppression and the survival outcomes as well as TH treatment-related adverse events.
Methods
We performed a systematic review and meta-analysis in accordance with the Preferred Reporting Items for Systematic review and Meta-Analysis (PRISMA) 2020 guidelines. 18 Our study protocol was registered with PROSPERO (#252396).
Eligibility criteria
Eligibility criteria were developed following the Population, Intervention, Comparator, Outcomes, and Study Design (PICOS) format. The inclusion criteria for each of these components were as follows: (i) Population: adult patients (18 years and older) of all races and ethnicities who were diagnosed with intermediate- and high-risk DTC and had undergone thyroidectomy and RAI as initial therapy or a regional guideline-based initial therapy and for whom at least two TSH measurement values and outcome data—time to death and/or time to progression were available during the follow-up. We utilized the American Thyroid Association 2016 guidelines for risk stratification. 1 (ii) Intervention: TSH suppression achieved through TH therapy. As the definition of TSH suppression is not uniform and may vary depending on the type of assay used, date of publication, and local guidelines, an exact numerical cutoff was not utilized as long as a given study had an intervention group identified as “TSH suppression,” or “below normal reference range,” or “subnormal TSH.” When available, a TSH of <0.5 mIU/L was accepted as a reasonable cutoff for TSH suppression for our study. (iii) Comparator: DTC patients with nonsuppressed TSH; defined as TH therapy resulting in average TSH 0.5–2 mIU/L (low-normal) or average TSH >2 mIU/L. Due to the possibility of fluctuations in these cutoffs because of reasons mentioned under “intervention,” an exact numerical cutoff was not utilized. However, if a given study had groups consisting of exclusively “elevated TSH” values or TSH defined as >4.5 mIU/L, such groups were excluded from the analysis. (iv) Outcomes: the primary outcomes of our study were I. Composite of progression-free survival (PFS), disease-free survival (DFS), and relapse-free survival (RLFS), and II. Composite of disease-specific survival (DSS), and overall survival (OS) in adults with intermediate- and high-risk DTC treated with local guideline-based initial therapy. The secondary outcome included a composite of cardiovascular and skeletal adverse effects in this population. The cardiovascular and skeletal adverse effects included the following: atrial fibrillation, heart attack, cardiac failure, myocardial infarction, osteoporosis, and fractures. If a given study provided data on the composite of these adverse effects, the composite data were preferred over the individual adverse effects from that study. (v) Study design: randomized controlled trials (RCTs), prospective and retrospective cohort studies, case–control studies with a follow-up duration enabling assessment of a 5-year survival rate were included for this analysis, whereas cross-sectional studies, case reports and case series, systematic reviews or meta-analysis, cost–benefit analyses, and qualitative research were excluded. The 5-year time point was not restricted to just average duration of follow-up, and we included any study in which 5 years of follow-up duration was a part of the range or interquartile range of follow-up. If duplicate data appeared, the most recent publication pertinent to the data was included. Only full-length articles or research letters published in English, human-only studies, and peer-reviewed studies were included, whereas the conference abstracts were excluded. Studies in which TSH values were represented only as a continuous variable or as ordinal data without clear dichotomization of suppression versus nonsuppression, or studies in which the numerical data of outcomes were not presented were excluded from the analysis. There were no limitations placed on the year of publication. In case any clarification or further information was required for a given study, the corresponding author of that study was contacted.
Search strategy
We conducted an electronic literature search in the following databases: PubMed/MEDLINE (NLM), PsycINFO (APA), CINAHL Plus (Cumulative Index to Nursing and Allied Health Literature—EBSCOhost), Web of Science, Core Collection (Clarivate Analytics), Embase (Elsevier), Scopus (Elsevier), and Cochrane Library (Wiley), and ClinicalTrials.gov. The initial search was conducted on May 6, 20221, and an updated search was conducted on February 1, 2024. The database search was conducted by an experienced information specialist (G.B.) (Supplementary Data S1).
Data collection and risk-of-bias assessment
Four independent reviewers (M.A.-J., S.C., S.G., J.K.G.) screened all titles and abstracts, with each abstract being assessed by at least two reviewers, and compared them against inclusion criteria to identify potential full-length articles for review. The abstracts were accepted for further review of the full-text article if they met the following mandatory criteria: (i) study design: RCTs, prospective and retrospective cohort studies, case–control studies, and (ii) outcome data enabling evaluation of 5-year PFS and/or DSS and/or OS. If an abstract did not contain full information based on our inclusion criteria, but met the above two criteria, it was accepted for full-text review under the following conditions: (i) The study had a heterogeneous group of patients but also included the subgroup of interest for our study, and (ii) lack of data on TSH level/TSH suppression in the abstract, but the study met other inclusion criteria and cohort was undergoing standard therapy. To satisfy the latter point, we screened the full-text articles to identify information on TSH levels/TSH suppression. Any disagreement was resolved through consensus, based on the evaluation by all four reviewers. Then, four independent readers (M.A.-J., P.F., SG., J.K.G.) performed a full-text screening to identify eligible articles based on all inclusion criteria. Only studies meeting all inclusion criteria were subject to meta-analysis, with any disagreement being resolved through consensus.
The assessment of the risk of bias was performed using the National Heart, Lung, and Blood Institute (NHLBI) Study Quality Assessment Tool. 19 This tool was developed by the NHLBI in 2013 to assist reviewers with determining the internal validity of a given study. It has separate quality assessment tools for RCTs, observational studies, and for case–control studies. Each of these tools has 12–14 questions assessing the various components of a study (Supplementary Data S1). An in-depth guidance for dealing with each question is provided elsewhere. 19 The eventual quality of a study is adjudicated as “good,” “fair,” or “poor.” Two independent reviewers (S.G, J.K.G) performed the risk-of-bias assessment, and any disagreement was resolved through consensus.
Statistical analyses
Meta-analyses of hazard ratios were conducted using a random-effects pairwise meta-analysis with DerSimonian and Laird (DL) method. Pooled estimate of hazard ratios (HRs) and the corresponding 95% confidence interval (CI) were presented in forest plot. Where available, outcomes data from multivariate analyses were preferred for our meta-analysis, otherwise, the univariate data were utilized. Due to the variations in the effect sizes of the studies, random-effects model was utilized to describe HR and 95% CI.
Heterogeneity between studies included was assessed using the Cochran’s Q statistic (Q, Chi-squared test). Heterogeneity was present if Q > degree of freedom with p ≤0.10. Quantification of heterogeneity was obtained using inconsistency index (I 2 statistic). I 2-values of 0–29.99%, 30–59.99%, 60–74.99%, and 75%–100% indicate low, moderate, substantial, and considerable heterogeneity, respectively. Funnel plots were used to assess publication bias graphically and Egger’s test was used for testing asymmetry of the funnel plot. The p value from Egger’s test was provided only for the meta-analyses that contained 10 studies or more (in our case, subclassification of TSH comparisons in a given study were treated as separate studies) as at least 10 studies are required through this test to provide a p value. Data analyses were conducted by R version 4.1.3 and all p-values were two tailed and regarded as significant when p < 0.05 unless otherwise indicated. For the primary outcomes, a HR of >1 meant less favorable survival outcomes with TSH suppression, and for the secondary outcomes, a HR of >1 meant higher prevalence of adverse events with TSH suppression. All 95% CI results that did not include 1 were considered significant.
Results
The study flow diagram as per the PRISMA 2020 guidelines for new systemic reviews is represented in Figure 1. A total of 8,043 records were identified from the database search and 1,674 duplicate records were excluded. We screened 6,369 reports and identified 1,196 eligible reports for full-text screening. After excluding the reports for not satisfying one or more of the exclusion criteria, nine studies were identified for final review and meta-analysis. 6,7,17,20 –25 A summary of data from each of these studies is provided in Table 1. The publication years for these studies ranged from 1996 to 2019. The final list included five retrospective cohort studies, 7,17,21 –23 one prospective cohort study, 6 one case–control study, 25 and two RCTs. 24 All studies had over 5 years of duration of follow-up (either as a median or including the range/interquartile range). The definition of the ‘TSH suppression' group varied vastly among studies. Very low TSH cutoffs for suppression were utilized in Pujol et al., 23 in which suppression was considered as ≥10% of values of TSH being ≤0.05 mIU/L, and in Sugitani et al., TSH suppression group defined as <0.01 µU/mL. 24 Two studies (Esik et al. and Carhill et al.) did not provide specific TSH values for suppression. 6,22 Restratification of TSH values into mean TSH scores was undertaken in the studies by Carhill et al. and Klubo-Gwiezdzinska et al. 6,7 Eight out of nine studies evaluated one or more of the primary outcomes, while the secondary outcomes were evaluated by two studies (Klein Hesselink et al., and Wang et al.). However, for Klein Hesselink et al., the outcomes stratified based on TSH suppression values were only represented in graphical format without the HR and 95% CI values. Therefore, raw data were procured from the corresponding author of the study and based on the available data points, we were able to not only perform Cox proportional hazards analysis for the secondary outcomes from the DTC cohort in this study, but also analyze their primary outcomes (DSS and OS). While the survival outcomes in most studies were assessed based on a single comparison: TSH-suppressed versus TSH-nonsuppressed groups, two studies (Carhill et al., and Klubo-Gwiezdzinska et al.) performed analyses through more than a single comparison by further categorizing TSH suppression levels. Both studies categorized the patients based on average TSH scores obtained during the follow-up period into: (i) suppressed TSH (score 1–1.99), (ii) subnormal to normal TSH (score 2–2.99), and (iii) normal to elevated TSH (score 3–4), and comparisons of survival outcomes were performed between subnormal/normal TSH (score 2–2.9) and normal/elevated TSH (score 3–4), and between suppressed TSH (scores of 1.0–1.9) and subnormal/normal TSH (score 2.0–2.9) in both studies, while Klubo-Gwiezdzinska’s study also included a comparison between normal/elevated TSH (score 3–4) and suppressed TSH (score1–1.99), whereas the exact TSH levels were provided in Klubo-Gwiezdzinska study, the actual TSH measurement values were not mentioned in the Carhill et al. study. We contacted the corresponding author for the study for the actual TSH values, but the study was closed by the Institutional Review Board and the data were not available. For our meta-analysis, we performed comparisons between (i) suppressed TSH (score 1–1.99) and normal/elevated TSH (score 3–4), and (ii) subnormal/normal TSH (score 2–2.99) and normal/elevated TSH (score 3–4). Carhill et al. and Klubo-Gwiezdzinska et al. were the only cohort studies that reported landmark analysis for the outcomes of interest in order to reduce time-varying covariate bias. As we possessed the raw data for Klubo-Gwiezdzinska et al., we were able to perform cumulative outcomes analyses. For Carhill et al., due to unavailability of raw data, we were able to obtain the HRs and 95% CIs for DFS and OS for stages II, III, and IV (non-low-risk) DTC from Supplementary Appendix 8 in their publication. Combining these individual HRs and 95% CIs, we calculated a weighted HR and 95% CI. The study quality is provided in Table 1, while a detailed risk-of-bias assessment for all the nine studies is provided in the Supplementary Data S1. One study was rated as “poor,” four were rated as “fair,” and the rest of the four studies were rated as “good.”
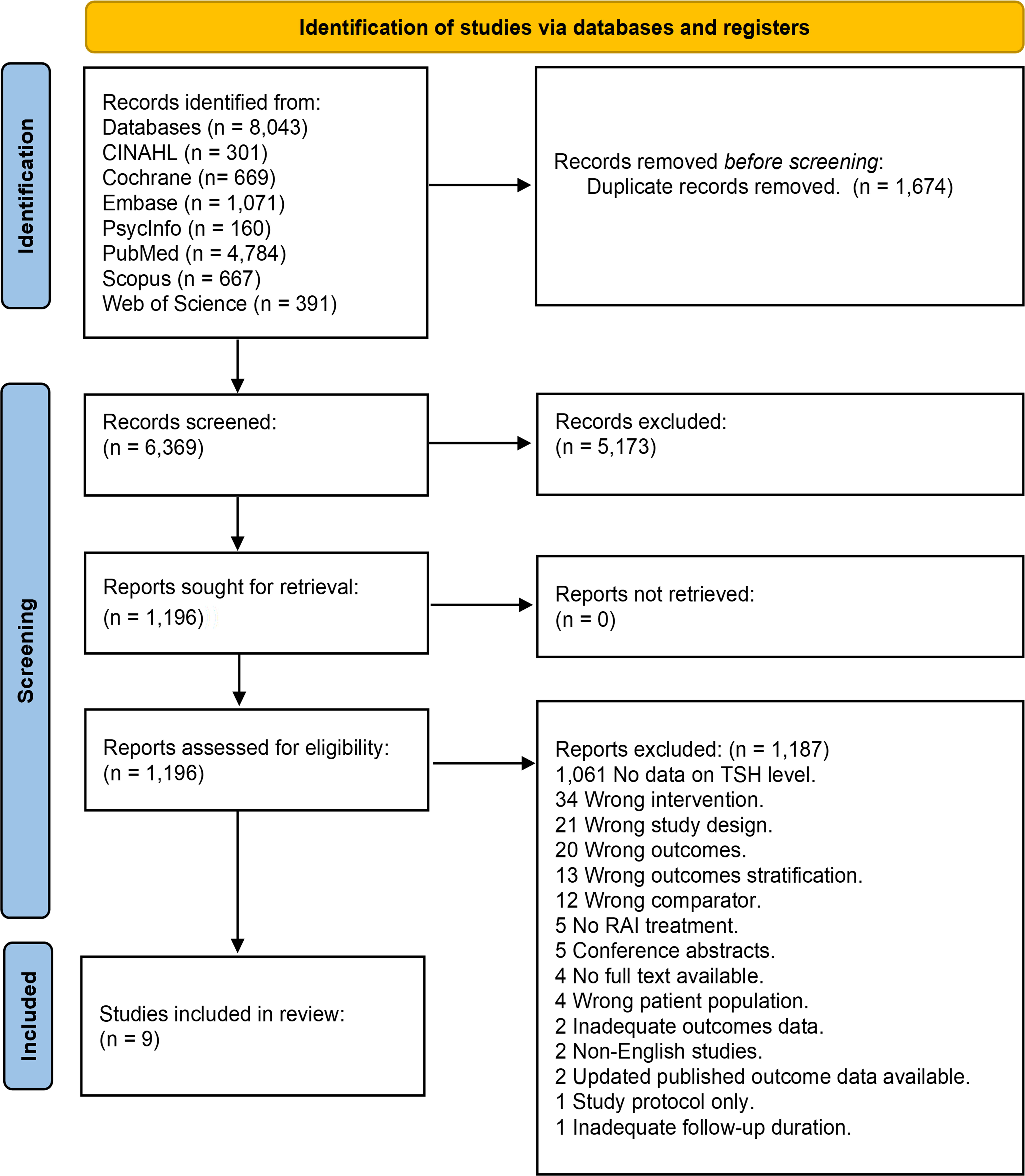
The PRISMA flow diagram for study selection.
Summary of All the Included Studies for Meta-Analysis
Klein Hesselink et al., and Wang et al. evaluated secondary (cardiovascular and/or skeletal adverse events) outcomes.
For Carhill et al. and Klubo-Gwiezdzinska et al., vales and outcomes of cumulative data (instead of 5-year landmark data) are provided in this table.
This number is from the entire cohort in a given study and not specifically from intermediate- or high-risk patients. Some values are provided as percentage (%) if the article has provided these values in only % and not the actual number of patients.
For Bӧhm et al., under the “Number of patients in each TSH category” column, the “% of patients” have been converted to “number of patients” (rounded to the nearest whole number).
All comparisons are represented as suppressed TSH vs. non-suppressed TSH. Any variations or sub-categorizations of TSH suppression patterns, if present in a given study, are described for that respective study in this column.
AMES, age, metastases, extent, and size; CSD, cause-specific death; CV, cardiovascular; DTC, differentiated thyroid cancer; DFS, disease-free survival; DSS, disease-specific survival; HR, hazard ratio; IRMA, immunoradiometric assay; LN, lymph node; OS, overall survival; PFS, progression-free survival; RAI, radioactive iodine; RIA, radioimmunoassay; RLFS, relapse-free survival; TSH, thyrotropin; 95% CI, 95% confidence interval.
Evaluation of the composite of PFS, DFS, and RLFS
The composite analysis is represented in Figure 2. Seven studies evaluated the outcomes: PFS in one study, 7 RLFS in two studies, 21,23 and DFS in four studies, 6,17,20,24 consisting of 3,591 patients in total (Table 1). TSH suppression was not associated with better survival outcomes (HR: 0.75; 95% CI: 0.48–1.17; I2 = 76%; Egger’s test p = 0.012) (Fig. 2A). Meta-analysis of only “good” quality studies (3,109 patients) also demonstrated no beneficial effect of TSH suppression on the composite outcome (HR: 0.98; 95% CI: 0.64–1.5; I2 = 75%) (Fig. 2B). We performed another set of meta-analysis in which the individual HRs and 95% CIs were from the outcome data from each stage (II, III, and IV) of Carhill et al. study. Even here, TSH suppression did not demonstrate significant benefit (HR: 0.71; 95% CI: 0.46–1.08; I2 = 82%; Egger’s test p = 0.031) (Fig. 2C). However, considerable heterogeneity was noted among studies in all of these meta-analyses. As the 5-year landmark outcomes data were already available for Carhill et al. (DFS), and Klubo-Gwiezdzinska et al. (PFS), we performed a meta-analysis on these outcomes, and no benefit was demonstrated with TSH suppression, with low heterogeneity between studies (HR: 1.11; 95% CI: 0.79–1.57; I2 = 0%) (Fig. 2D).

Meta-analysis demonstrating the forest plots for the composite outcome of progression-free survival, disease-free survival, and relapse-free survival.
Evaluation of DSS and OS
Two studies, Esik et al. and Klein Hesselink et al., reported DSS (with DSS being reported as “cause-specific death” in Esik et al.), OS was evaluated in two other studies (Carhill et al. and Klubo-Gwiezdzinska et al.) as landmark outcomes, but we calculated cumulative outcomes as described earlier. The DSS and OS outcomes for Klein Hesselink et al. were calculated by us from raw data. The composite DSS and OS outcome analysis, derived from a total of 3,616 patients in these four studies demonstrated no beneficial effect from TSH suppression when analyzing studies of all qualities (HR: 0.69; 95% CI: 0.31–1.52; I2 = 88%) (Fig. 3A) as well as studies of “good” quality consisting of 2,693 patients (HR: 0.46; 95% CI: 0.17–1.23; I2 = 81%) (Fig. 3B). A meta-analysis for DSS alone and OS alone showed no significant effect of TSH suppression on survival outcomes (Fig. 3C, D). However, there was a net benefit from TSH suppression noted on OS when outcome data from each stage (II, III, and IV) of Carhill et al. study was included instead of weighted outcome data (HR: 0.48; 95% CI: 0.23–0.99; I2 = 91%; Egger’s test p = 0.023) (Fig. 3E). Considerable study heterogeneity was again noted with all of the analyses. A 5-year landmark OS analysis for Carhill et al., and Klubo-Gwiezdzinska et al. also did not support TSH suppression (HR: 0.87; 95% CI: 0.31–2.41; I2 = 53%) (Fig. 3F).
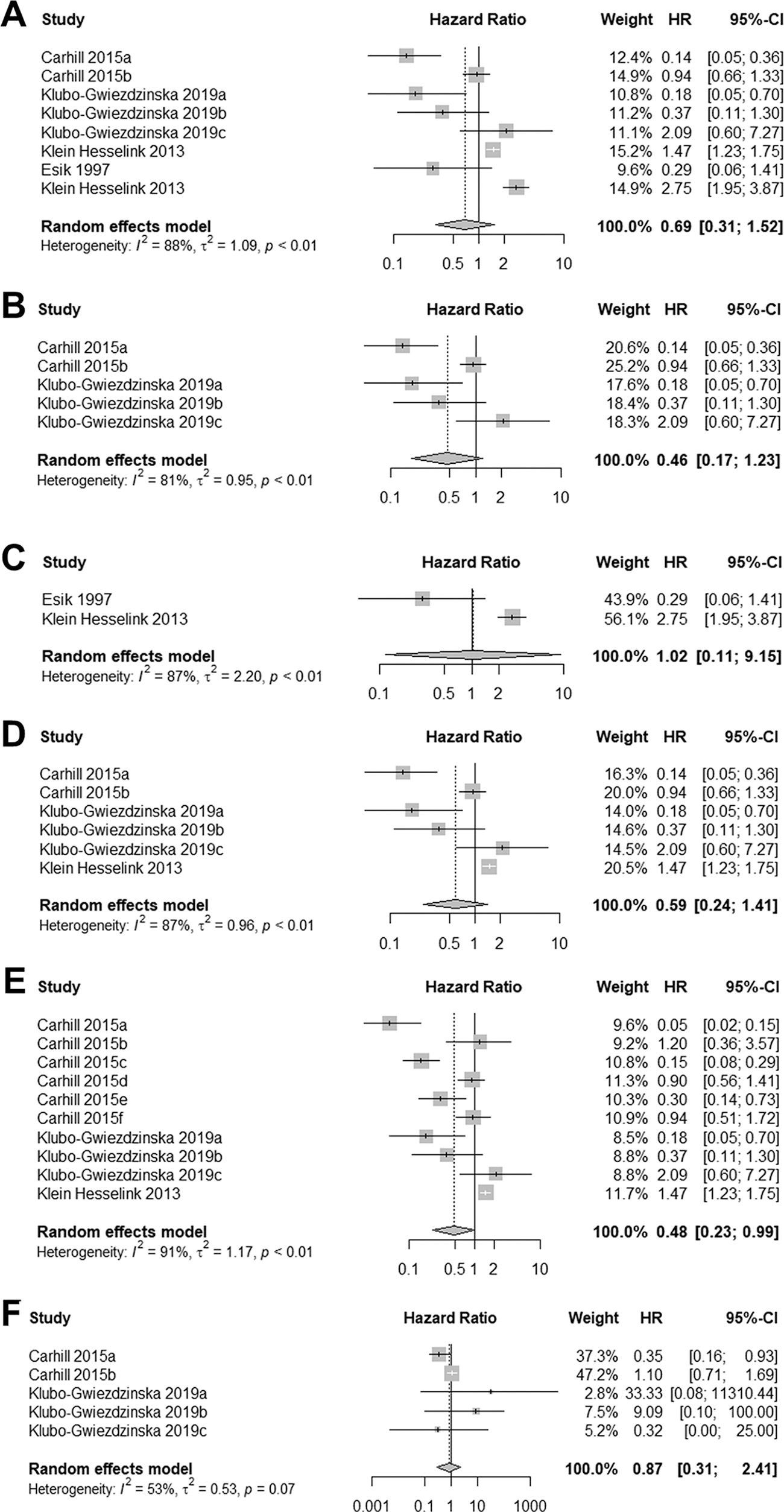
Meta-analysis demonstrating the forest plots for DSS, and OS.
Evaluation of secondary outcomes
Two studies evaluated secondary outcomes in a total of 1,294 patients. Wang et al. evaluated for the composite outcome of atrial fibrillation and osteoporosis risk in DTC patients. 17 For Klein Hesselink et al., we extracted parameters of interest from the raw data and calculated HR and 95% CI for cardiovascular disease-related mortality in the TSH suppressed group (TSH <0.02 and 0.02–0.2 mIU/L) versus TSH nonsuppressed group (TSH >0.2 mIU/L). Skeletal complications outcome was not available in this study. The risk for developing cardiovascular and/or skeletal complications was significantly higher with TSH suppression (HR: 1.82; 95% CI: 1.30–2.55; I 2 = 0%), with low study heterogeneity (Fig. 4). The funnel plots for all the primary and secondary outcomes are provided in the Supplementary Data S1.

Meta-analysis demonstrating the forest plot for secondary composite outcome of cardiovascular and skeletal adverse events, documenting increased risk of adverse events associated with TSH suppression. TSH, thyrotropin.
Discussion
We performed a systematic review and meta-analysis of nine studies to evaluate the effect of TSH suppression on survival and adverse effect outcomes in intermediate- and high-risk DTC. We demonstrate that TSH suppression is generally not associated with better survival outcomes in DTC, but the risk for cardiovascular and skeletal adverse events is significantly higher with TSH suppression. Our results held true even after exclusion of ‘poor’ and ‘fair’ quality studies and with enrichment of studies containing higher quality data.
The only other meta-analysis on TSH suppression and DTC survival outcomes was reported in 2002, 26 in which TSH suppression was associated with a lower risk (RR = 0.73; 95% CI = 0.60 ± 0.88; p < 0.05) of disease progression, recurrence, and death. However, the meta-analysis was performed on 10 heterogeneous studies, including case series and retrospective studies, with no risk stratification of DTC, and the beneficial effect of TSH suppression on survival outcomes based on study quality assessment from the meta-analysis was deemed “questionable” or “likely.” Moreover, these studies were conducted from 1971 to 1998, during which the treatment guidelines were vastly different, with less-sensitive TSH immunoassays being utilized in several of these studies. Our meta-analysis included data from more recent studies that likely utilized more sensitive TSH immunoassays, and we focused on the intermediate- to high-risk population from the included studies in whom TSH suppression is mainly utilized.
Regarding primary outcomes in our meta-analysis, five studies did not favor TSH suppression in non-low-risk DTC, 7,17,22,24,25 while three studies favored TSH suppression, 20,21,23 and the two studies that evaluated for secondary outcomes did not favor TSH suppression. 17,27 Moreover, all of the ‘good’ quality studies in our meta-analysis did not favor TSH suppression. Nevertheless, it should be noted that the number of studies was small in the individual DSS and OS meta-analyses, especially only two outcome measures in the DSS analysis with one study being of “poor” quality. In their study, Carhill et al. found that survival benefit was not noted upon comparison between moderate TSH suppression and aggressive TSH suppression (subnormal–undetectable TSH), even among patients with distant metastasis, further questioning the role of aggressive TSH suppression on improving survival outcomes in advanced DTC. 6 Interestingly, we noted that when we incorporated individual HRs from each of stage II, III, and IV from Carhill et al. instead of the weighted HRs (obtained from combining all three stages), TSH suppression was associated with better OS (Fig. 3E). However, among the individual components of the study, only those comparisons between moderate TSH suppression and no suppression (TSH scores of 2–2.99 vs. 3–4) favored TSH suppression. The likely reason for this finding is because the group of TSH score 3–4 also included elevated TSH values, which by themselves can serve as a growth stimulus to DTC, thereby confounding the results. This has been demonstrated in other studies in which elevated TSH has been associated with worse DTC survival outcomes. 28 Apart from Carhill et al., which utilized data from the National Thyroid Cancer Treatment Cooperative Study Group (NTCTCS) registry, at least two other studies (Cooper et al. and Jonklaas et al.) have utilized data from the same NTCTCS registry to evaluate the association between TSH suppression and DTC recurrence, but the analysis occurred earlier (with smaller sample size and shorter follow-up duration), hence only the latest data analysis of Carhill et al. was included in this meta-analysis. Cooper et al. demonstrated that age, disease stage, and RAI therapy predicted DTC progression, and TSH suppression was not a factor determining disease progression in multivariate models. 3 In the other NTCTCS registry-based study conducted by Jonklaas et al., TSH suppression between subnormal and undetectable levels was associated with better DSS and OS in stage II DTC patients, and so was TSH suppression to undetectable levels in high-risk patients. 4 More recent retrospective data from Japan demonstrated similar DFS between TSH suppressed and unsuppressed subgroups with intermediate-risk DTC followed for more than 5 years. 29 However, we did not include this study for our meta-analysis as the Cox proportional hazards for DFS was not available.
The debate on whether TSH suppression is necessary in non-low-risk DTC is likely to continue, however, specific characteristics of intermediate- and high-risk DTC, such as serum thyroglobulin, tumor margins, extent, size of lymph node metastases, and extrathyroidal extension may help fine tune the recommendations for TSH suppression. For instance, in a retrospective cohort study by Tian et al., rate of disease recurrence was assessed in intermediate- and high-risk DTC patients with preablation serum thyroglobulin level <1 ng/mL according to TSH levels measured at 1-year time point after initial therapy. 30 The 1-year TSH was categorized into 4 groups: (i) TSH < 0.1 mIU/L, (ii) TSH 0.1–0.5 mIU/L, (iii) 0.5–2 mIU/L, and (iv) >2 mIU/L. During a median follow-up of 5.8 years, the rate of disease recurrence was not significantly different among the different TSH groups. Another study by Back et al. evaluated the risk of locoregional DTC recurrence in patients with tumors having microscopic positive margins. 31 Although microscopic positive tumor margin was not associated with locoregional recurrence, risk factor analysis revealed that increasing TSH levels were associated with risk for locoregional recurrence. A vastly unexplored aspect in this field is the relation between the molecular landscape of DTC and TSH suppression. This is mainly because molecular testing on DTC tumor samples is infrequently performed in clinical practice. Furthermore, TSH suppression is debatable in more dedifferentiated thyroid cancers as TSH receptor protein expression and mRNA levels have been partly or completely lost in these subset of tumors. 8,32,33
Our meta-analysis demonstrated that the risk for cardiac and skeletal adverse effects was significantly higher in the TSH suppression group. Several studies in the past have demonstrated the adverse effects of excess TH treatment on cardiovascular and bone health, including ischemic heart disease, atrial fibrillation, and osteoporosis. 16,25,27,34 Cardiovascular disease has been identified as the most common cause for non-cancer-related mortality in thyroid cancer patients. 35 Recently, Qiang et al., demonstrated in their meta-analysis of seven studies that DTC survivors could be at a higher risk for cardiovascular mortality and atrial fibrillation compared with the general population after adjusting for confounders. 36 In the study by Klein Hesselink et al., after a median follow-up of 8.5 years, DTC patients had a 3.35-fold higher risk for cardiovascular mortality, and for every 10-fold reduction in the geometric mean TSH values, there was a 3.08 times higher risk for cardiovascular mortality. 25 In a recent meta-analysis of 10 studies evaluating cardiovascular outcomes in DTC patients followed for a median of 8.6 years, long-term TSH suppression was associated with higher risk of atrial fibrillation but no significant differences in heart failure, ischemic heart disease, or cardiovascular mortality compared with healthy controls. 37 Another recent meta-analysis of 16 studies demonstrated increased risk of atrial fibrillation in thyroid cancer patients on TSH suppression, and a subanalysis of six homogeneous studies revealed higher mean systolic and diastolic blood pressures compared with controls. 38 The effects of TSH suppression on bone health are comparatively equivocal. A meta-analysis of 16 case–control studies by Kwak et al. demonstrated that a TSH suppression to <0.1 mIU/L was associated with worsened lumbar spinal bone mineral density (BMD) in postmenopausal women who had undergone thyroidectomy for thyroid cancer compared with controls. 34 However, not all studies have demonstrated detrimental effects of TSH suppression on bone. Data from small cohorts of male, premenopausal and postmenopausal female DTC patients, have failed to show detrimental effects on BMD or bone turnover markers after short-term (1–2 year) TSH suppression compared with controls, 39 and it is likely that longer duration of TSH suppression may be necessary to see adverse effects on BMD. 40 Interestingly, some meta-analyses have demonstrated worsening BMD with TSH suppression only in postmenopausal women, but no such effects in premenopausal women or men, 41 or even an increase in BMD in premenopausal women, 42 suggesting potential protective effects of estrogen and testosterone against excess TH-induced bone loss. However, significant study heterogeneity was often noted in most of these meta-analyses.
Our study has certain strengths. We utilized strict inclusion criteria, which allowed us to enrich our cohort with intermediate- and high-risk DTC patients and exclude low-risk DTC patients as much as possible. As our final set of studies was all conducted within the past 25 years, there were lesser chances of utilization of obsolete treatments and older (first- or second-generation) immunoassays. We also carefully evaluated the individual studies in the final meta-analysis for the potential of confounding effects of elevated TSH levels in the comparator groups and excluded these datasets from our analysis. Our study does have limitations. Most studies were either observational or cohort studies, which can be flawed due to lack of randomization, inadequate controls, or inadequate sample size. Considerable heterogeneity was noted among the studies. The definition of TSH suppression was not uniform across the studies. The possibility of varying adherence of patients to their TH regimen potentially leading to fluctuations in TSH levels throughout the duration of follow-up cannot be ruled out. Furthermore, the details on the type of TSH assay and utility of third-generation or more sensitive TSH assays were not mentioned in several studies (Table 1). Due to heterogeneity of data and the limited number of studies, subanalyses based on the risk level of DTC (intermediate-risk alone or high-risk alone), age groups, or the degree of TSH suppression, could not be undertaken. The type of survival outcomes used was different among the various studies, which necessitated us to pursue composite outcome analyses. This small sample size also precluded robust evaluation for publication bias for certain outcomes.
In conclusion, TSH suppression in intermediate- and high-risk DTC may not improve survival outcomes but can be associated with increased risk for adverse effects of supraphysiologic TH therapy. However, the high data heterogeneity and the suboptimal quality of several studies included in our meta-analysis warrants a cautious interpretation of the results. The findings of this meta-analysis may hopefully serve as an impetus for future large-scale studies as well as multicenter RCTs to unequivocally establish the role of TSH suppression in non-low-risk DTC.
Footnotes
Acknowledgment
The authors sincerely thank Dr. Joop D. Lefrandt, the corresponding author of the Klein Hesselink et al. article, who generously provided us the relevant raw data from their study.
Authors’ Contributions
Initial drafting of the article: S.G., M.A.-J. Protocol drafting, selection criteria development, risk-of-bias assessment: M.A.-J., S.C., and J.K.-G. Data extraction, screening, data collection, quality assessment: S.G., M.A.-J., S.C., P.F., and J.K.-G. Provision of clinical expertise: S.G., M.A.-J., and J.K.-G. Search strategy development and testing: G.B. Statistical analysis: S.A. and E.C.W. Study conceptualization: J.K.-G.
Data Availability
Data from this article can be shared by the corresponding author upon reasonable request.
Author Disclosure Statement
All authors have no conflicts of interest to declare.
Funding Information
This study was supported by the intramural program of the National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health (grant No. 1ZIADK047053-17).
Supplementary Material
Supplementary Data S1