
Abstract
Background
: Although the impact of tumor-immune infiltrate has been reported on differentiated thyroid cancer (DTC) behavior, the expression of immune checkpoints [programmed cell death protein 1 (PD-1) and its ligand (PD-L1)] alone has not been able to predict response to immunotherapies. We aimed to identify tumor-infiltrating immune cells and checkpoints associated with DTC.
Methods
: We performed multiplex immunofluorescence on deparaffinized thyroid tissue collected at thyroidectomy from 17 adults with DTC to characterize the tumor immune microenvironment for leukocytes (CD45+), T cells (CD3+), T regulatory cells (Tregs) (CD3+FOXP3+), CD4+ T cells (CD3+CD4+), CD8+ T cells (CD3+CD8+), macrophages (CD68+), M2 macrophages (CD68+CD163+), M1 Macrophages (CD68+ inducible nitric oxide synthase [iNOS]+), and immune checkpoints PD-1 and PD-L1. We compared the mean percentage expression of immune markers between tumor and adjacent thyroid tissue from the same patient by paired t-test and performed spatial analysis along the tumor’s leading edge.
Results
: Immune checkpoints PD-1 and PD-L1 showed a significant increase in expression intratumorally as compared to adjacent thyroid tissue (p < 0.05). A higher trend for M2 macrophages was observed intratumorally compared to adjacent tissue. Along the leading edge, PD-L1 expression correlated negatively with CD45 and positively with CD163 intratumorally. On exploratory analysis, there was a nonsignificant trend for higher FOXP3 but less CD8 and iNOS expression in tumor from DTC with (n = 3) versus without distant metastases (n = 14). There was a nonsignificant trend for higher CD58 and iNOS expression in DTC with (n = 7) than without thyroiditis (n = 10).
Conclusions
: Higher tumoral PD-1 and PD-L1 expression indicate their role in DTC occurrence. A trend for more Tregs and M2 macrophages but less M1 macrophages intratumorally in patients with distant metastatic DTC, suggests their potential role as prognostic biomarkers. Future studies with larger sample sizes are needed to compare various clinicopathologic severities to harness tumor microenvironment for cancer prognostication and therapy.
Introduction
Thyroid cancer is the most common endocrine cancer worldwide and in the United States, with rising incidence predicted to make it the third most common cancer in women by 2030. 1 Most cases are follicular cell-derived differentiated thyroid cancer (DTC). Follicular cells also give rise to the more aggressive forms of thyroid cancer, including poorly differentiated thyroid carcinoma (PDTC) and anaplastic thyroid cancer (ATC), and a recently recognized entity of differentiated high grade thyroid carcinoma (DHGTC). 2 Although thyroid autoimmunity is associated with increased risk of thyroid cancer, 3 –7 there is conflicting evidence for its association with prognosis. 8 –13 Studies on specific tumor-infiltrating immune cells demonstrated that macrophages are associated with poor outcomes such as lymph node metastases, 14 larger tumor size 15 and reduced survival, 16,17 but detailed investigation of the pro-tumoral M2 macrophage phenotype in DTC has not been performed. Conflicting data regarding the association between CD8+ cytotoxic T cells and better 18 or worse prognosis 19 have been reported. T regulatory cells (Tregs) inhibit anti-tumor response by producing interleukin-10 and expressing immune checkpoints and, if present, can be associated with aggressive thyroid cancer. 20,21 Certain subtypes of natural killer cells are associated with tumor aggressiveness 22 while others with less aggressive DTC. 21 A recent study demonstrated that the tumor microenvironment (TME) is composed predominantly of myeloid cells with decreased lymphoid cells in pathologically aggressive thyroid cancer. 23 Increased circulating myeloid-derived suppressor cells are associated with advanced thyroid cancer, 24 while their infiltration into the tumor has been demonstrated only in mice. 25 Other studies have suggested a link between circulating immune phenotypes and thyroid cancer, 26 but remain limited due to lack of correlation with tumor-infiltrating immune cells.
A major driver mutation for thyroid cancer, BRAF-V600E, is associated with increased expression of the immune checkpoint programmed death-ligand 1 (PD-L1), thus suggesting its link with an immunosuppressive TME. 27 Higher PD-L1 expression in DTC tissue and higher programmed death protein 1 (PD-1) expression on lymphoid cells infiltrating the tumor or associated lymph nodes are linked to aggressive DTC. 20,28 Separate from DTC, some studies have demonstrated “cold or immune altered-excluded” TME in PDTC while “hot or immune altered-immunosuppressed” TME in ATC. 29 While most PDTC, 30 DHGTC, 2 and ATC arise from DTC, 31,32 the factors underlying these transitions remain to be fully elucidated.
Approximately 10% of DTC patients have an aggressive course with a 5-year survival of 15.3%. 33 In advanced cases, the toxicities and partial response from aggressive multi-modality approaches have led to the exploration of immunotherapies 34 since expression of PD-L1 on malignant thyroid cells 35,36 supports the potential for response to anti-PD-L1 immunotherapies. 37 The current state of knowledge in the field of immunoediting of DTC is limited by evaluation of individual biomarkers or lack of data on patient outcomes and demographic factors. 16,20,23,24,38 Hence, selecting patients for such immunotherapies has been a challenge with poor or inconsistent response. 34,39 Additionally, PD-L1 expression has not correlated with the efficacy of these therapies 34 possibly due to resurgence of an immunosuppressive TME as shown in a murine thyroid cancer model. 40 The spatial organization of the TME has a complex effect on the response to therapy, particularly along the tumor-thyroid interface, which is characterized by unique immune cell profiles. The heterogenous region of the leading edge is distinct from the tumor core as it is characterized by spread of tumor cells and highly infiltrated by immune cells. Hence, understanding the immune infiltrate along the leading edge of DTC could be of prognostic and therapeutic benefit throughout the spectrum of thyroid cancer.
Methods
Sample and specimen collection
This IRB-approved (ID 0802-19-EP) retrospective study was performed by utilizing thyroid tissue samples from 17 adult patients (≥ 19 years) with DTC (Table 1). Study participants consented to have their data and banked biospecimens utilized for future research as part of their enrollment into the Thyroid Cancer and Tumor Collaborative Registry, which is a part of the Cancer Repository for Cancer Research (iCaRe 2 ). 41 Patients with MTC, PDTC, ATC, benign thyroid disease, and biospecimen unavailable for analysis were excluded. At the time of tissue collection, DHGTC was not defined as a separate entity. Formalin-fixed paraffin-embedded (FFPE) thyroid cancer specimens collected at the time of initial thyroidectomy were retrieved by an endocrine pathologist, cut into five μm sections, and mounted onto charged slides. Laboratory investigators were blinded to clinical data.
Demographic and Clinical Characteristics of 17 Adult Patients with Follicular Cell-Derived Thyroid Cancer Differentiated Whose Thyroid Cancer Tissue Was Analyzed for 12 Immune Markers via Multiplex Immunofluorescence to Compare Tumor to Adjacent Tissue
ATA, American Thyroid Association; AJCC, American Joint Committee on Cancer; T NM, tumor node metastasis; T P OAb, Thyroid peroxidase antibody.
Laboratory techniques of multiplex immunofluorescence
We performed multiplex immunofluorescence via an immune panel modified from our previous work in pancreatic cancer. 42,43 We deparaffinized and rehydrated FFPE tissue with xylene and ethanol-water gradient, and then performed antigen retrieval using a citrate buffer. The tissue was blocked in 1% bovine serum albumin (BSA) for one hour followed by a permeabilization step (1.5% triton). The tissue was stained using directly labeled antibodies and incubated overnight at 4°C. When pre-labeled antibodies were unavailable, immunoglobulins were tagged using labeling and purification kits: lightning link for the Cy7 and GE kits for Cy3 and 5. Working concentrations were verified to limit background staining. When no risk of cross-reactivity was present, unconjugated primary antibodies were followed by a secondary antibody incubated for 1 hour post wash steps (Table 1). The slides were washed in phosphate buffered saline (PBS) and cover slips mounted using mounting media with 4',6-diamidino-2-phenylindole to stain the nuclei. The slides were dried at room temperature for at least 48 hours. Once dried, the slides were scanned using a Panoramic 250 slide scanner (3D Histech, Budapest, Hungary) at 20× objective. The scanner utilizes light fluorescence to digitize specimens based on set parameters and allows for whole slide imaging on up to five channels in a high throughput manner. Slides were inverted for 24 hours in a 1× working concentration of PBS solution with gentle agitation at room temperature to facilitate the removal of coverslips. The fluorophores were quenched by incubating slides in 3% Triton for 10 minutes and an alkaline H2O2 solution for 15 minutes with rotation to allow for re-staining with a new round of antibodies. Subsequent staining and imaging rounds were repeated. Antibodies against specific antigens were used in three rounds of staining: round one included PD-1, PD-L1; round two included FOXP3, CD3, CD8, CD4; and round three included CD45, CD68, CD163, inducible nitric oxide synthase (iNOS) (Supplementary Table S1).
Image alignment of multiplex immunofluorescence
Verification of image alignment was performed via HALO, a digital image analysis platform by Indica Labs, Inc. Exposure of each marker was determined by the intensity of cytoplasmic staining and cellular structure. Visual thresholding was performed across ten samples. The thresholds were averaged and applied to all tissue specimens. To account for blood and other forms of autofluorescence, an unstained sequential cut was quantified alongside the stained sample and the percentage of positive cells in the control was subtracted from the test sample. Due to the optimized thresholding procedure, background noise was reduced and the proportion of cells expressing a particular marker could be determined from each round of staining.
Colocalization and quantification of staining
A priority list of cell types with biological significance was constructed to facilitate the recovery of internal colocalization outputs. Staining on thyroid tissue was compared with tonsil tissue as positive control. We identified cell-surface molecules for leukocytes (CD45+), T cells (CD3+), Tregs (CD3+FOXP3+), CD4+ T cells (CD3+CD4+), CD8+ T cells (CD3+CD8+), macrophages (CD68+), M2 macrophages (CD68+CD163+), M1 macrophages (CD68+iNOS+), and immune checkpoints PD-1 and PD-L1.
Statistical analysis of multiplex immunofluorescence
We calculated the sample size based on the results of Means et al. 23 who compared intra-tumoral and adjacent thyroid tissue from the same specimen obtained from study participants with DTC. Based on those findings, we expected the mean percentage of Tregs of 1.25% [standard deviation (SD) 1.6%] for adjacent non-cancerous thyroid tissue and 2.5% (SD 1.6%) for paired thyroid cancer tissue. We assumed a high correlation between the outcome measurements of paired tissues within each subject (r ≥ 0.5), and correspondingly SD of paired difference was estimated as ≤ 1.6%. A sample size of n = 17 pairs achieved 80% power to detect a mean of the differences of 1.25% between pairs with an estimated maximum SD of paired difference of 1.6%, with a significance level of 0.05. This provided an adequately powered sample to identify differences between important immune markers in cancerous versus adjacent non-cancerous thyroid tissue.
We compared the mean percentage expression of immune markers between tumor and adjacent thyroid tissue from the same patient by paired t-test assuming unequal variances, and in exploratory analysis by t-test assuming unequal variances between intra-tumoral tissue in DTC patients with distant metastases versus those without, and DTC patients with chronic lymphocytic thyroiditis versus those without. Analyses were performed in Prism 10.0.2 (GraphPad, San Diego, CA). A p value < 0.05 was used to classify statistically significant differences.
A correlation matrix was created using R packages for Pearson’s correlation analysis to identify correlation between the percentage of cells at specific locations. The leading edge of the tissue was divided into 100 µm bands, going into and out of the tumor for 1000 µm. The percentage of individual cell types within these bands was quantified and the correlation between the percentages of cells in each band was compared.
Results
The median age was 44 years and 65% were females; 94.1% had classical papillary and the rest follicular-variant papillary DTC. The majority (70.6%) did not have lymph node (LN) involvement, 17.6% had central neck LN involvement (N1a), and 11.8% had lateral neck LN involvement (N1b). Of all cases, 76.5% were of low American Thyroid Association (ATA) risk, 17.6% of intermediate risk and 5.9% of high risk for recurrence. The cohort was followed for a median of 2.4 years from thyroidectomy, during which 76.5% did not develop recurrence or progression. There were no cases of significant tissue necrosis or high rate of mitoses. Detailed characteristics are reported in Table 1.
Overall, in 17 DTC patient samples, most leukocyte (CD45+) infiltrate occurred along the leading edge towards the peritumoral thyroid tissue. Among the high expressing antigens (on average, <10% of the total cell population), PD-1 and PD-L1 were more within the tumor as compared to adjacent thyroid tissue (p < 0.05) despite less leukocytes (CD45+) intratumorally (p < 0.05). A trend for more CD163 staining (marker for M2 macrophages) was observed intratumorally compared to adjacent tissue. These comparisons are demonstrated graphically in Figure 1.
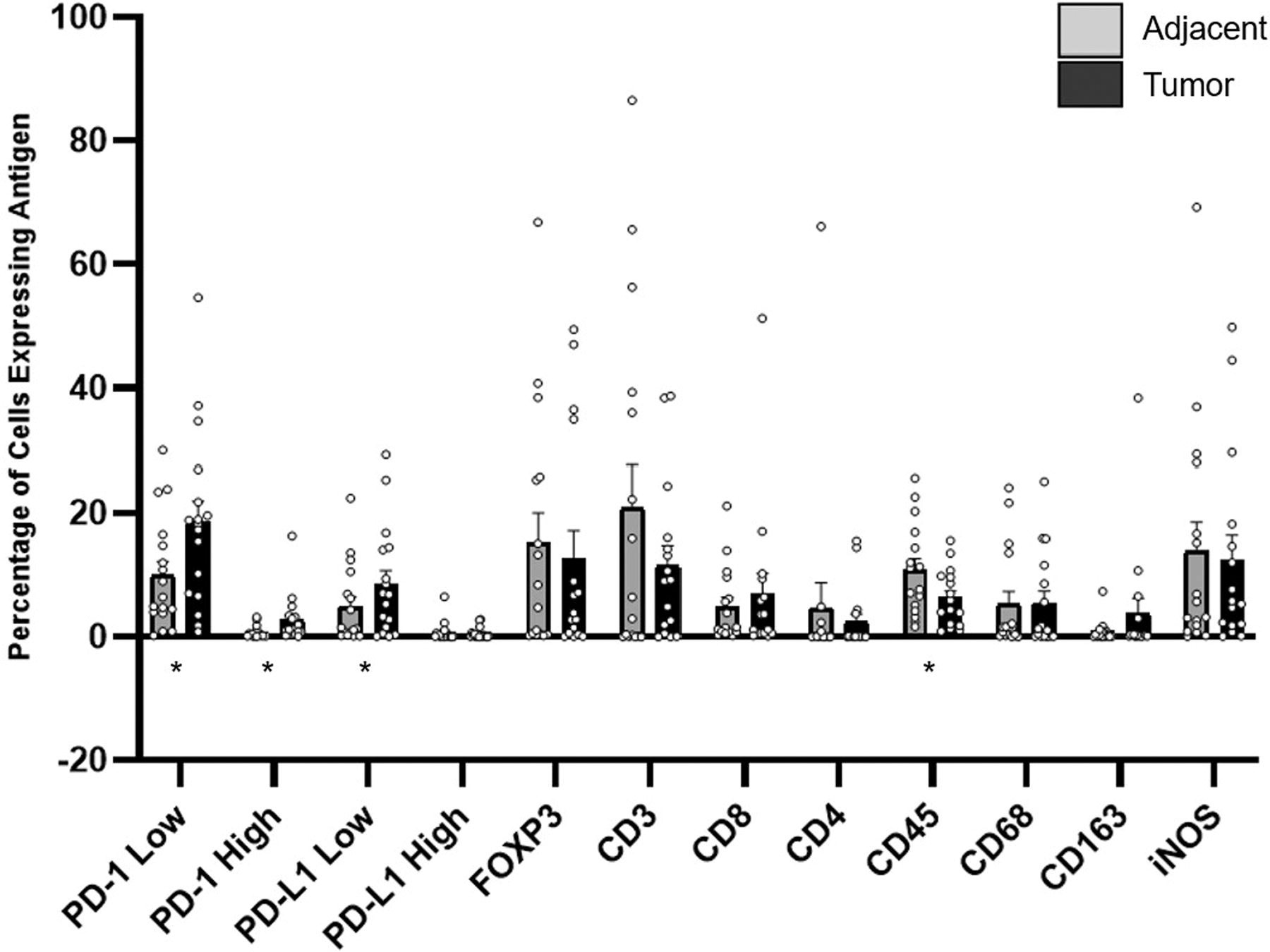
Comparison of antigen expression within the tumor and adjacent thyroid tissue showing more PD-1 and PD-L1 but less CD45 (marker for leukocytes) expression intratumorally; and showing a nonsignificant trend for more CD163 (marker for M2 macrophages) intratumorally. *p < 0.05. PD-1, programmed cell death protein 1; PD-L1, programmed death-ligand 1.
Within the cohort of 17 DTC cases, three patients had distant metastases, five had central or lateral neck LN involvement, and the rest had DTC localized to the thyroid gland. To better understand the differences in DTC behavior and prognosis, we compared tumoral immune infiltrates between DTC with (n = 3) versus without distant metastases (n = 14) showing a nonsignificant trend for higher FOXP3 (marker for Tregs) but lower CD8 (marker for cytotoxic T cells) and iNOS (marker for M1 macrophages) expression (Supplementary Figure S1). To understand the impact of serologic or pathological evidence of chronic lymphocytic (Hashimoto’s) thyroiditis, the tumoral immune infiltrate in DTC patients with chronic lymphocytic thyroiditis (n = 7) showed a nonsignificant trend for higher CD68 (marker for all macrophages) and iNOS (marker of M1 macrophages) expression than those without thyroiditis (n = 10) (Supplementary Figure S2). In our cohort, 85.7% of patients with chronic lymphocytic thyroiditis had localized DTC while 50% of patients without it had a localized DTC (p = 0.3). Within the cell cluster implicated in adaptive immune response, we identified an aggregate of CD4+ and CD8+ T cell subtypes. Due to limited sample size, significant differences in immune cell subtypes between tumor and adjacent tissue were not observed. A trend towards increased subtypes CD8+ T cells not expressing PD-1 in the tumor-rich regions was observed with increased PD-L1 staining intensity. Greater proportions of CD8+ Tregs were noted in the tumor compared to adjacent tissue. Greater proportions of M2 macrophages were identified intratumorally relative to M1 macrophages.
A banding invasion analysis (Fig. 2B) along the leading edge was performed by dividing the tissue into 100 μm bands going into and out of the tumor along the leading edge. We found increased PD-1 (Fig. 2A and F) and PD-L1 expression (Fig. 2E) within the tumor despite a greater proportion of CD45+ cells (Fig. 2D) detected outside of the tumor. A discernible trend associated with macrophage infiltration could not be demonstrated (Fig. 2C).
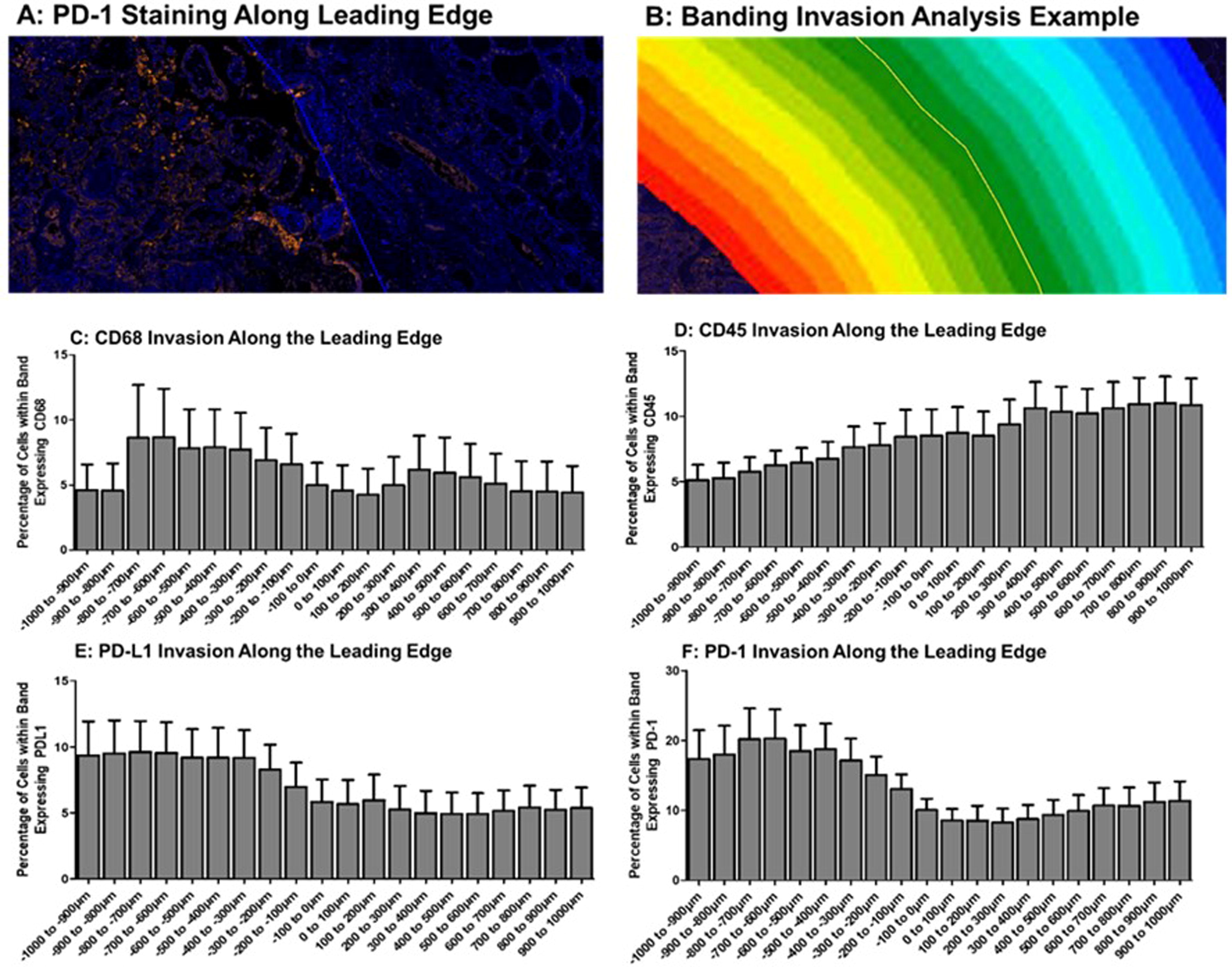
Cellular invasion analysis along the leading edge of tumor. (A) Example area of PD-1 staining (orange) along the primary tumor leading edge (depicted by blue line). (B) Example of banding strategy along the tumor leading edge. (C) Mean expression of CD68 (marker for macrophages) along the tumor leading edge for all samples. (D) Mean expression of CD45 (marker for leukocytes) along the tumor leading edge for all samples. (E) Mean expression of PD-L1 along the tumor leading edge for all samples. (F) Mean expression of PD-1 along the tumor leading edge for all samples. PD-1, programmed cell death protein 1; PD-L1, programmed death-ligand 1.
Spatial correlation between antigens (Fig. 3) was quantified from the invasion analysis. Intratumorally, PD-L1 expression correlated negatively with CD45 (leukocyte marker) and positively with CD163 (M2 macrophage marker) expression. PD-L1 expression correlated positively with PD-1 in adjacent but not intratumoral tissue.
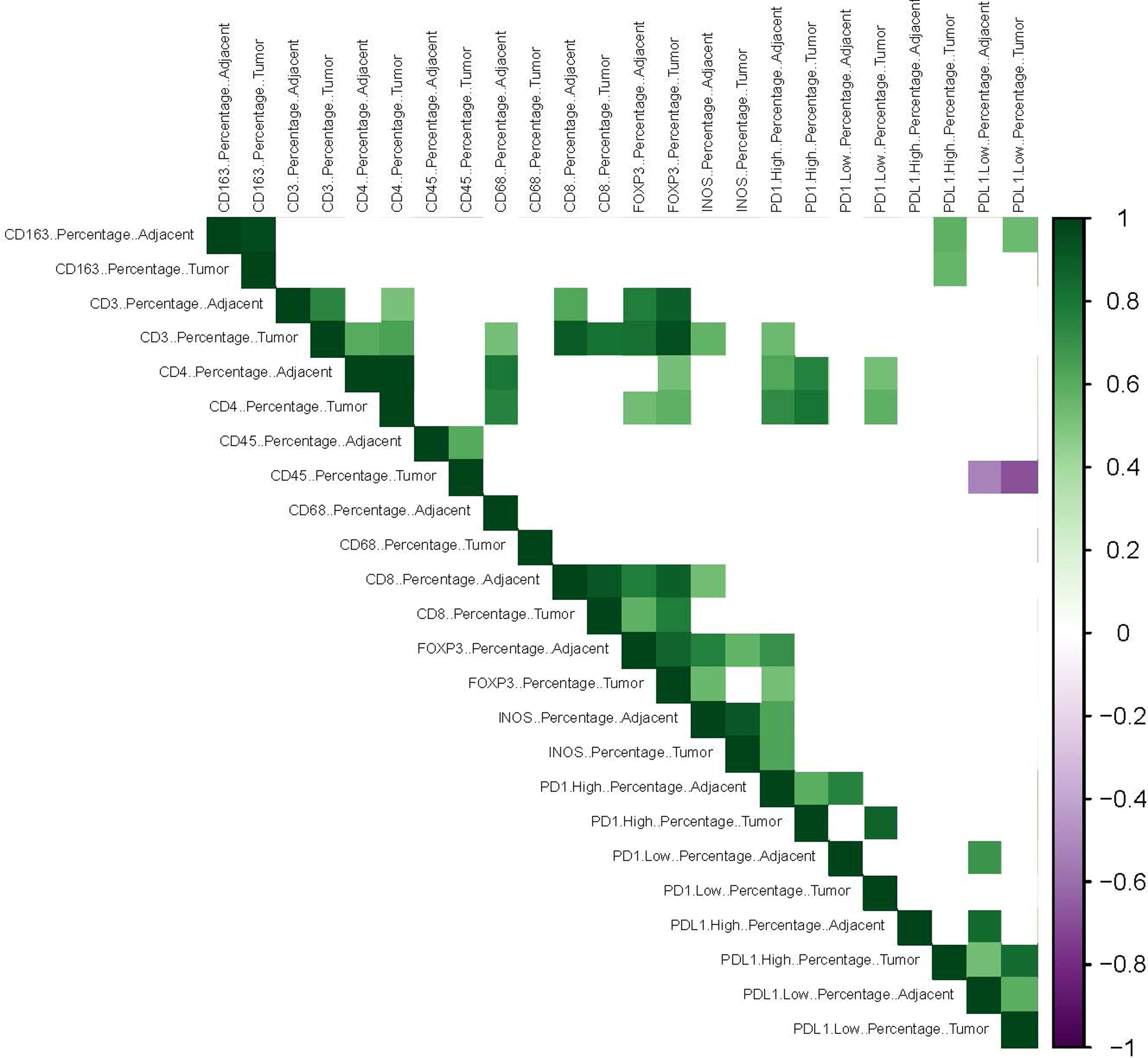
Pearson’s Correlation matrix for spatial analysis of immune cell and checkpoint staining along the leading edge of tumor, intratumorally and in the adjacent tissue. The percentage of CD45+ (marker for leukocytes), CD68+ (marker for macrophages), PD1+ and PDL1+ cells was quantified from the invasion analysis. Positive correlations between the percentage of cells in each band are shown in green and negative in purple. All nonsignificant correlations (p > 0.05) are left blank. PD-1, programmed cell death protein 1; PD-L1, programmed death-ligand 1.
Discussion
While the role of tumor-infiltrating immune cells has been investigated in DTC previously, some studies have not performed detailed investigation into the subtypes of immune cells, while others have not collected information on clinically relevant outcomes. Hence, our study investigating these immune cell subtypes along the leading edge of tumor from 17 adults with DTC with clinical information adds significantly to the knowledge about the impact of the TME on the occurrence and behavior of DTC.
Our investigation utilizing multiplex immunofluorescence on whole slides of thyroid tissue allowed us to characterize the immune infiltrate along the tumor leading edge and compare intra-tumoral versus the adjacent thyroid tissue from the same DTC surgical sample. Increased expression of immune checkpoints that suppress the immune system — PD-1 and PD-L1 — was identified along the leading edge within the tumor (cancerous) region as compared to the adjacent thyroid tissue. This finding is consistent with previous studies demonstrating increased expression of PD-L1 in malignant thyroid cells. 35,36 Higher tumoral PD-L1 expression is corroborated by a meta-analysis showing a link between increased thyroidal PD-L1 expression, BRAFV600E mutation, and worse disease-free survival. 27 On spatial correlation analysis, PD-L1 expression positively correlated with PD-1 in adjacent but not intratumoral tissue suggesting differences in immune milieu and an active engagement of the immunosuppressive PD-1/PD-L1 axis responsible for inhibiting the anti-tumor immune response. Additionally, PD-L1 expression negatively correlated with CD45+ leukocytes intratumorally suggesting immune exhaustion being associated with less infiltration by immune cells. A previous study demonstrated elevated PD-1+ T cells 20 in the circulation in more aggressive thyroid cancer, opposite of the pattern we observed intratumorally during colocalization analysis. Altogether, these findings point towards immune exhaustion intratumorally which may not be apparent in the circulation.
The expression of immune checkpoints has not been strongly predictive of response to immunotherapies in advanced thyroid cancer, 34 highlighting the need to identify additional immunosuppressive markers in the TME. Hence, we performed exploratory analysis within the cohort of 17 patients with DTD. Tumors from patients with distant metastases also demonstrated a trend for higher intratumoral FOXP3 (marker for Tregs), and colocalization analysis demonstrated more Tregs intratumorally relative to adjacent thyroid tissue. French et al. 20 also previously reported increased Tregs in lymph nodes involved by papillary DTC associated with extrathyroidal extension, supporting their link to histologically aggressive DTC. Tregs inhibit the anti-tumor response by producing IL-10 and expressing immune checkpoints. Our findings, and supporting data demonstrate T cell exhaustion intratumorally and highlight the potential role of Tregs as a key predictive and prognostic biomarker in DTC.
Comparison of the intra-tumoral to adjacent thyroid tissue demonstrated a trend, albeit nonsignificant, for more CD163 (marker for M2 macrophages) intratumorally. Colocalization analysis showed more M2 relative to M1 macrophages intratumorally demonstrating enrichment of the immunosuppressive macrophage subtype in the TME. Exploratory analysis revealed a trend for lower iNOS (marker for pro-inflammatory or anti-tumor M1 macrophages) expression in the tumors from patients with distant metastases as compared to those localized to the neck. These findings are similar to previous literature demonstrating that tumor infiltrating macrophages are associated with poor outcomes including lymph node metastases, 14 larger tumor size 15 and reduced survival. 16,17 Spatial correlation analysis showing tumoral PD-L1 expression correlating positively with the CD163 (marker for anti-inflammatory or pro-tumor M2 macrophages) further lends insight into the role of macrophages in thyroid carcinogenesis.
A functional relationship between chronic inflammation and cancer has been supported by clinical evidence in thyroid cancer, 5,44 the pathophysiological basis being increased COX-2 expression, a marker mediating the inflammatory process in the initial stages of tumorigenesis. 45 The effect of chronic lymphocytic thyroiditis in this cohort was seen with nonsignificant trend for higher likelihood of localized DTC and correspondingly with higher tumoral expression of CD68 (marker for all macrophages) and iNOS (marker for M1 macrophages). These trend differences suggest more anti-tumoral M1 macrophage infiltration in the tumors of DTC with chronic lymphocytic thyroiditis which is in line with less histopathological invasiveness. 8 –10
The limitations of this pilot study include small sample size which was sufficiently powered to compare the tumoral to adjacent thyroid tissue from each DTC sample, not to find significant differences in immune markers associated with the stage, type, ATA risk category of DTC or the co-occurrence of chronic lymphocytic thyroiditis. The lack of cytokine and interleukin testing, as well as lack of flow cytometry, in our study due to the nature of tissue is a limitation hence does not definitively prove the functional status of the immune cells. Statistical co-localization comparisons were limited due to the sample size. Only three patients had distant metastases, and none demonstrated significant tissue necrosis or high rate of mitoses, hence we were not able to definitively identify immune markers associated with DTC prognosis. Nevertheless, the trend for higher expression of markers for the immunosuppressive Tregs but lower expression of markers for immune effector cytotoxic T cells and M1 macrophages in distant metastatic DTC primary tumor as compared to locoregional DTC primary tumor, despite being inadequately powered, are important findings.
In summary, we demonstrate that an immunosuppressive TME is associated with the occurrence of DTC. Increased PD-L1 could be utilized as a marker for the presence of cancerous thyroid tissue when there is diagnostic uncertainty by current pathological criteria. A trend for more Tregs and M2 macrophages but less M1 macrophages intratumorally in patients with distant metastatic DTC, suggests their potential role as prognostic biomarkers. Our findings provide a foundation for future research into the functionality of immune infiltrate and for development of therapeutic approaches directed towards the entire immunosuppressive TME rather than only the immune checkpoints to favorably impact outcomes of patients with thyroid cancer.
Footnotes
Acknowledgments
This publication was made possible by support from the Nebraska Cancer and Smoking Disease Research Program Award (NE DHHS-
Authors’ Contributions
A.K.: Conceptualization (lead); methodology (equal); formal analysis (supporting); writing—original draft (equal); writing—review and editing (equal). K.V.: Conceptualization (supporting); methodology (equal); formal analysis (lead); writing—original draft (equal); writing—review and editing (equal). K.H.: methodology (supporting); formal analysis (supporting); writing—review and editing (equal). A.Y-V.: Methodology (supporting); writing—review and editing (supporting). B.S.: Methodology (supporting); writing—review and editing (supporting). E.M.D.: Methodology (supporting); writing—review and editing (supporting). O.S.: Methodology (supporting); writing—review and editing (equal). M.H.: Software (lead); writing—review and editing (supporting). H.B.: Conceptualization (supporting); writing—review and editing (supporting). W.G.: Conceptualization (supporting); writing—original draft (equal); writing—review and editing (equal).
Author Disclosure Statement
All authors have nothing to declare.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Funding Information
A.K.: 1. Nebraska Cancer and Smoking Disease Research Program Award (NE DHHS-
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1