
Abstract
Background:
Obesity and hypothyroidism are common medical conditions that are associated with each other. Bariatric surgery (BS) is a common approach used to achieve substantial weight loss in obese patients. However, there is limited evidence regarding the need for postsurgery levothyroxine (LT4) dose adjustment in patients with hypothyroidism undergoing BS.
Methods:
This was a three-year prospective cohort study assessing postsurgery LT4 requirements with attention to body composition changes. The current study included 1030 patients with hypothyroidism, who underwent sleeve gastrectomy (SG) (n = 707, 88.3% women) or one anastomosis gastric bypass (OAGB) (n = 323, 92% women). Patients were followed for 36 months after surgery. A bioelectrical impedance analyzer was used for body composition assessment. LT4 requirements were assessed by generalized estimating equation (GEE) methods adjusted for weight as a time-varying covariate.
Results:
During the follow-up, TSH (mIU/L) and T4 (ng/dL) measurements did not significantly change in the OAGB group over time. However, in the SG group, TSH measurement decreased over time (ptrend = <0.001). In the third year of the follow-up, 56.1% and 33.3% of patients in the SG and OAGB groups experienced LT4 (μg/day) dose reduction, while 24.4% and 9.1% of the participants experienced LT4 dose increments, respectively. GEE analysis showed a significant increase in the LT4/fat mass (FM) (μg/kg) ratio after 36 months of follow-up compared with the baseline in both the SG [1.8 (1.5–2.2) to 2.7 (2.0–3.5), ptrend = 0.039)] and OAGB [1.7 (1.4–2.2) to 3.2 (2.7–4.8), ptrend = <0.001)] groups. Moreover, patients who underwent OAGB experienced greater LT4/FM (μg/kg) dose adjustments compared to those undergoing SG (pbetween = 0.060). In both groups, after the first year, the increase in LT4/FM (μg/kg) plateaued (pinteraction = 0.009).
Conclusion:
Most hypothyroid patients experienced either a reduction or no change in LT4 (μg/day) dosage after 36 months in both surgical groups. The LT4/FM (μg/kg) was significantly increased in patients undergoing either SG or OAGB with greater alterations in the latter. Further studies on larger populations and with longer duration of follow-up are needed to confirm our results.
Introduction
Obesity, a global health concern, and a systemic disorder, is associated with numerous comorbidities and endocrine abnormalities, including hypothyroidism. 1,2 The thyroid hormone axis regulates body energy expenditure and weight balance, and thyroid hormone deficiency (i.e., hypothyroidism) is associated with weight gain. 3 Consistent results have been shown by a Mendelian randomization study, which indicated an incremental association between the body mass index (BMI) and thyrotropin (TSH) levels. 1
In practice, 1.6–1.8 μg/actual weight (AW) (kg)/day is the starting dose of levothyroxine (LT4) for hypothyroid patients to achieve euthyroidism. 4 However, this routinely administered dose may not be suitable for patients with obesity, given the higher volume of distribution and delayed gastrointestinal absorption. 5 In this regard, lean body mass (LBM), ideal body weight (IBW), and body surface area (BSA) have been suggested as relatively more accurate parameters to guide for LT4 dose adjustment compared to AW. 6 –8 In obese patients, LBM has shown a positive correlation with LT4 degradation rate; however, this correlation is debated with regard to fat mass (FM). 9
Bariatric surgery (BS) is a widely used and effective approach that not only leads to substantial and sustained weight loss but also improves numerous obesity-related comorbidities. 10 Recently, a systematic review and meta-analysis, including nine trials and 519 participants, indicated that patients with hypothyroidism generally experienced significant LT4 dose reductions following BS. Nonetheless, a high level of heterogeneity was observed when pooling the results of these studies (I2 = 67%, p = 0.0007), which was mainly attributed to different follow-up lengths. 11 Of note, in addition to the short duration of follow-up, most previous investigations have been carried out on a limited number of strictly selected patients undergoing a specific type of surgery. In this study, we aimed to explore the postsurgery LT4 dose adjustment with attention to various body composition components. The duration of follow-up was three years, and two popular and common types of BS, sleeve gastrectomy (SG) and one-anastomosis gastric bypass (OAGB), were considered.
Methods
Study design and sample population
This is a nonrandomized prospective cohort study. The data belonged to the patients enrolled in the Tehran Obesity Treatment Study (TOTS) from March 2013 to March 2021. The TOTS is an ongoing single-institution prospective study initiated in March 2013, the rationale and methodology of which have been explained in detail elsewhere. 12 This study was approved by the Institutional Review Board of the Research Institute of Endocrine Science, Shahid Beheshti University of Medical Science, Tehran, Iran (IR.SBMU.ENDOCRINE.REC.1401.126). The data were derived from the disease registry entitled “Registration of Patients in Tehran Obesity Treatment Center.” The study was also approved under the ethics code of “IR. SBMU.ENDOCRINE.REC1397.059” (date: 2018–05-08) by the local ethics committee. All participants provided written informed consent. The principles of the Declaration of Helsinki were followed during all procedures.
In this study, out of 5966 participants enrolled in the TOTS from March 2013 to March 2021, those who were <18 years or >65 years of age were excluded. Individuals with euthyroidism and chronic kidney disease, as well as those who received corticosteroids or underwent revisional or other types of surgeries, were also excluded. Finally, 1030 hypothyroid patients, diagnosed based on low free T4 (fT4) and high TSH, under LT4 therapy were included (SG = 707, OAGB = 323) (Fig. 1).
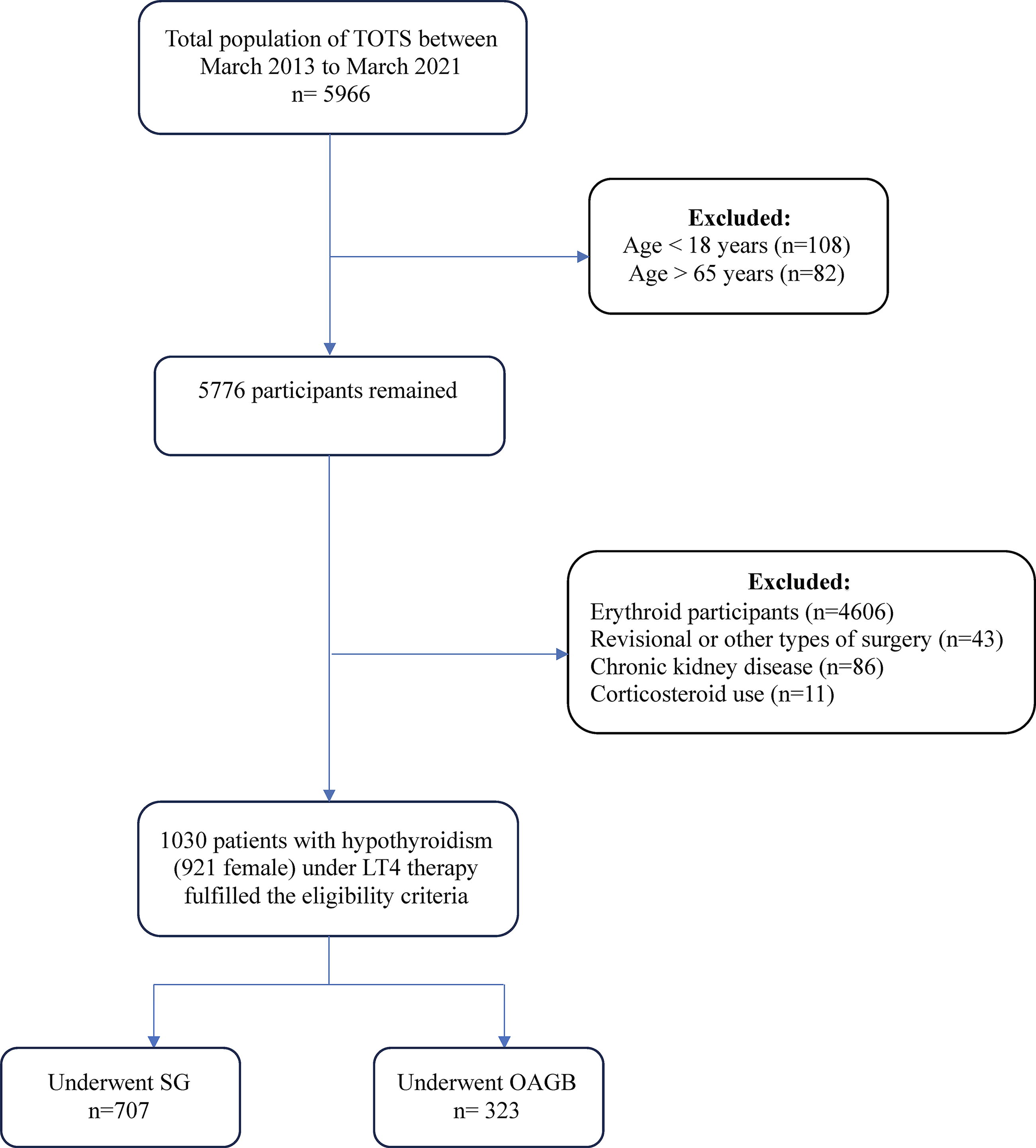
Study flowchart. Tehran Obesity Treatment Study; TOTS, sleeve gastrectomy; SG, one anastomosis gastric bypass; OAGB.
Anthropometric and biochemical measurements
Each patient underwent a comprehensive physical examination and was interviewed by a trained researcher to record demographic information and past medical history. Anthropometric indices, including weight (kg) and height (m), were determined according to the World Health Organization (WHO) recommendations. 13 BMI (kg/m2) was measured as weight divided by the square of height. Body composition components, including fat mass (FM, kg), fat-free mass (FFM, kg), fat mass percentage (FM%), and lean body weight (LBW), were assessed by a bioelectrical impedance analyzer (BIA, InBody 370, Biospace, Seoul, South Korea). Patients were advised to have overnight fasting, minimal physical activity for at least 12 hours, to abstain from alcohol consumption for at least 24 hours, and to maintain hydration for at least 5 minutes before the test. 14,15
Blood samples were collected after 12–14 hours of overnight fasting and before taking LT4 and kept at −20°C until biochemical measurements. Total cholesterol (TC), fasting plasma glucose (FPG), and triglyceride were assessed by an enzymatic colorimetric method. Low-density lipoprotein cholesterol (LDL-C) (mg/dL) was calculated according to the method of Friedwald et al. 16 Serum TSH (mIU/L) and fT4 (ng/dL) levels were quantified by the electrochemiluminescence immunoassay (ECLIA) using commercial kits and the Cobase 411 analyzer (Roche Diagnostics GmbH, Mannheim, Germany). Interassay and intra-assay CVs were 4.6% and 1.4% for TSH (mIU/L), and 3.3% and 1.3% for fT4 (ng/dL), respectively.
Follow-up and postoperative care
Patients in both SG and OAGB groups underwent a complete clinical assessment by a multidisciplinary team at the baseline and 1, 3, 6, 12, 24, and 36 months postsurgery to ensure their compliance with the treatment. At each visit, anthropometric indices and body composition components were assessed. LT4 requirements were adjusted at the discretion of the same team of endocrinologists based on the patient’s serum TSH and fT4 levels. Patients receiving proton pump inhibitors (PPIs) or those taking iron or calcium supplementation were advised to take LT4 with a time interval of at least 30 minutes or 4 hours in the case of taking PPIs or supplements, respectively.
Definitions
The normal ranges of TSH (mIU/L) and fT4 (ng/dl) were considered ∼0.32 to ∼5.06 mIU/L and ∼0.91 to 1.55 ng/dl, respectively. 17 Excess weight loss (EWL%) was calculated as [(Initial Weight) − (Postoperative Weight)]/[(Initial Weight) − (Ideal Weight)] × 100, in which the ideal weight was defined as the weight corresponding to a BMI of 25 kg/m2. Total weight loss percentage (TWL%) was calculated as [(Initial Weight) − (Postoperative Weight)]/[(Initial Weight)] × 100. 18 IBW (kg) was defined as weight for height at the lowest risk of mortality and calculated as derived by the Devine formula [male: IBW (in kg) = 50 + 2.3 × (height-60 inches) and female: IBW (in kg) = 45.5 + 2.3 × (height-60 inches)]. 19,20 Adjusted body weight (ABW) (kg), as a more appropriate parameter for patients who weigh >30% above their IBW (kg), was calculated as ABW = IBW + 0.4 × (AW-IBW). 21 The current weight of the patient was defined as AW (kg). BSA (m2), a metric to use various pharmacological therapies, was calculated using the Du Bois method [BSA = 0.007184 × Height (cm).0725 × Weight (kg).0425]. 22,23
LT4 requirement
LT4 consumption during the follow-up period was evaluated by various methods based on different anthropometric indices and body composition components: absolute LT4 (μg/day), LT4 dose by LBW (μg/kg), LT4 dose by FM (μg/kg), LT4 dose by AW (μg/kg), LT4 dose by BSA (μg/m2), LT4 dose by IBW (μg/kg), and LT4 dose by ABW (μg/kg).
Statistical analysis
The normality of the distribution of continuous variables was evaluated using analytical (the Shapiro–Wilk test) and visual (histogram) inspection methods. Normally distributed and skewed continuous variables were described as mean ± standard deviation (SD) and median [interquartile range (IQR) of 25–75], respectively. Categorical baseline characteristics were reported as numbers and proportions (%). Baseline characteristics between the surgery groups were compared using the independent sample t-test, Mann–Whitney U test, and Chi-square test for normally distributed quantitative, skewed quantitative, and categorical variables, respectively. The generalized estimated equation (GEE) method (auto-regressive working correlation structure and identity-link function) was performed to assess changes in LT4 requirements and anthropometric indices during three years of follow-up after BS. GEE analysis was performed considering time-varying weight alterations to attenuate the potential confounding effect. Time-trend examination models were applied, and p-values for trends were described for each group separately. All analyses were performed using the statistical software package SPSS version 20 for Windows; the significance level was set at p < 0·05 (two tailed).
Results
Patient characteristics
Initially, 1030 patients with hypothyroidism (89.4% female) were included in the analysis. A total of 323 patients with a mean age of 42.4 ± 10.2 years and a mean BMI of 45 ± 6.3 (kg/m2) underwent OAGB, and 707 patients with a mean age of 41.4 ± 10.7 years and a mean BMI of 43.5 ± 5.6 (kg/m2) underwent SG. TSH (mIU/L), T4 (ng/dL), and LT4 (μg/day) in the OAGB group were 2.7 (25–75 IQ: 1.2–5.3), 8.9 ± 2.6, and 100 (25–75 IQ: 100–114.3), respectively, and the corresponding values in the SG group were 2.9 (25–75 IQ: 1.4–4.9), 9 ± 2.5, and 100 (25–75 IQ: 100–114.3). Also, FM (either in kilograms or percentage) was significantly higher in the participants who underwent OAGB. There was no statistically significant difference between the SG and OAGB groups regarding preoperative TSH (mIU/L), T4 (ng/dL), and LT4 (μg/day) (Table 1).
Baseline Characteristics of Severely Obese Participants with Primary Hypothyroidism
Data are presented as n (%) or mean ± SD, except for TSH, THR, and triglyceride, which are presented as median (25–75 IQ).
BMI, body mass index; FM, fat mass; LBW, lean body weight; BSA, body surface area; TSH, thyrotropin; LT4 intake, levothyroxine therapy; FPG, fasting plasma glucose; DM, diabetes mellitus; BP, blood pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure; HTN, hypertension; SG, sleeve gastrectomy; OAGB, one anastomosis gastric bypass.
Postoperative weight indices
According to Table 2 and Figure 2, during the study period, all weight indices, except for EWL (%) and TWL (%), showed significant reductions in both the SG and OAGB groups. Moreover, a significant difference was observed between the two groups comparing all the indices, excluding LBW (kg) (Pinteraction = 0.147 and Pbetween = 0.462).
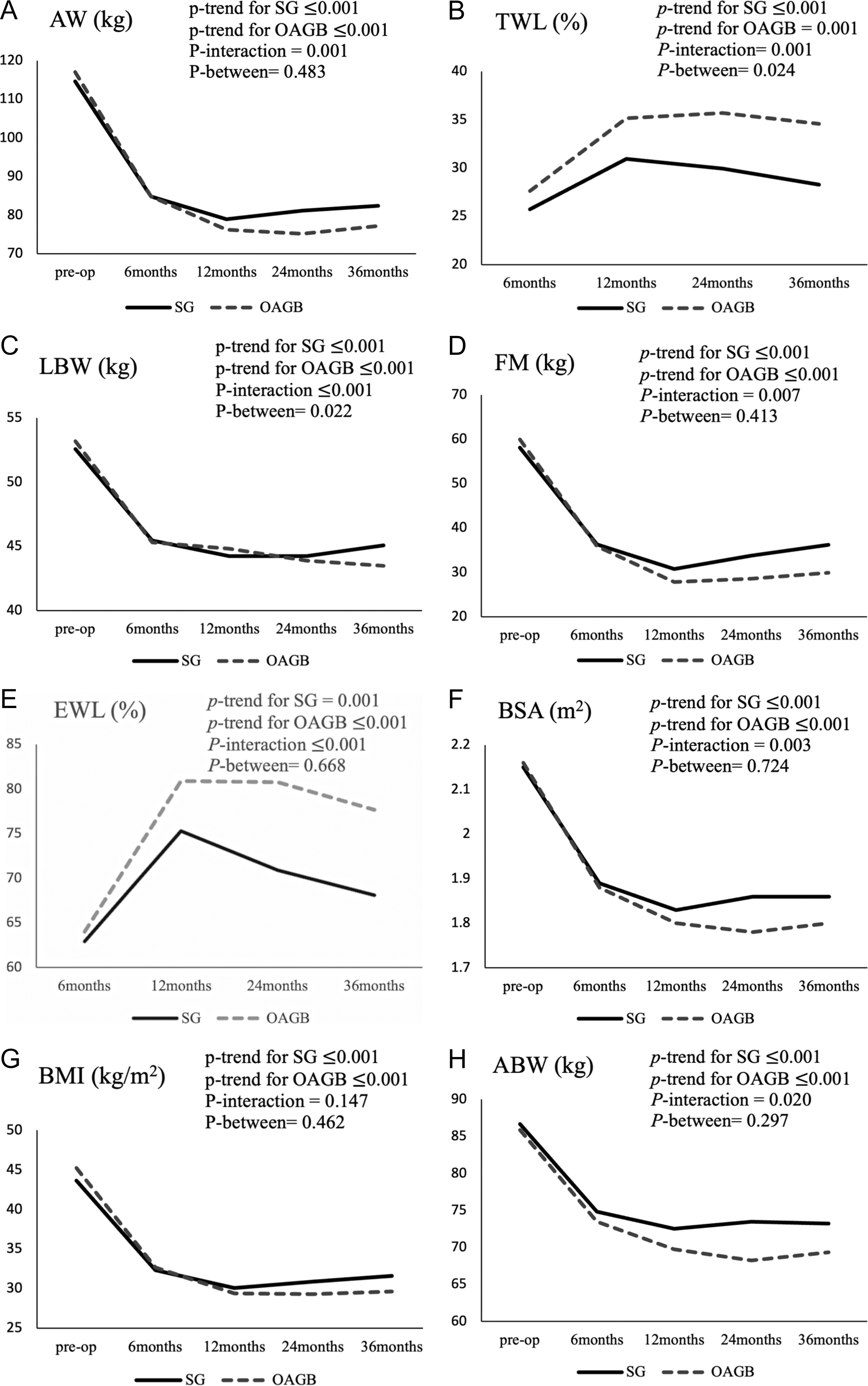
Alterations of weight indices during three years of follow-up in patients undergoing sleeve gastrectomy (SG) or one anastomosis gastric bypass (OAGB).
Weight Indices’ Alterations During Three Years of Follow-up After Bariatric Surgery
Data are presented as mean ± SD.
BMI, body mass index; TWL, total weight loss; EWL, excess weight loss; FM, fat mass; AW, actual weight; LBW, lean body weight; BSA, body surface area; ABW, adjusted body weight; n, number of patients.
LT4 (μg/day) intake during the follow-up
Any increase or decrease in LT4 requirements was recorded during the follow-up. In total, in the first, second, and third years of follow-up, 50.4%, 42.7%, and 46.8% of the patients experienced LT4 (μg/day) dose reduction, respectively. At the end of the third year, the number of patients who experienced a dose reduction was significantly greater in the SG group compared to the OAGB group (p-value = 0.018). On the other side, 15.3% of the patients experienced LT4 (μg/day) dose increase after the third year. The need for dose increment was significantly more prevalent in the OAGB compared to the SG group (p-value = 0.027). A total of 37.8% of the patients maintained steady doses of LT4 (μg/day) after surgery compared to the preoperative period (Table 3).
Levothyroxine (μg/Day) Consumption During the Three Years of Follow-up After Bariatric Surgery Among Patients with Hypothyroidism
Data are presented as n (%) or median (IQ 25–75).
Mean ± SD of alterations compared to the baseline.
Evaluating the difference between two types of surgery and values <0.05 were considered statistically significant.
LT4, Levothyroxine—Decreased: Any decrease in LT4 (μg/day) requirements to achieve euthyroidism; Increased
Postsurgery LT4 dosage and body composition components
Among various body composition components, LT4/FM (μg/kg) was the only parameter showing a significant increase in both the SG (ptrend = 0.039) and OAGB (ptrend = <0.001) groups. Furthermore, patients in the OAGB group experienced a greater change in LT4/FM (μg/kg) during the follow-up (B = 0.032, pbetween = 0.060, pinteraction = 0.009) compared with the SG group. However, LT4/FM (μg/kg) alterations reached a plateau after the first year of follow-up in both the SG and OAGB groups. In contrast to those undergoing OAGB, the average change in LT4/IBW (μg/kg) was statistically significant among SG participants (ptrend = 0.049). Weight, as a time-varying covariate, was adjusted in all models, excluding LT4/AW (μg/kg) for which this adjustment was inapplicable (Table 4 and Fig. 3).
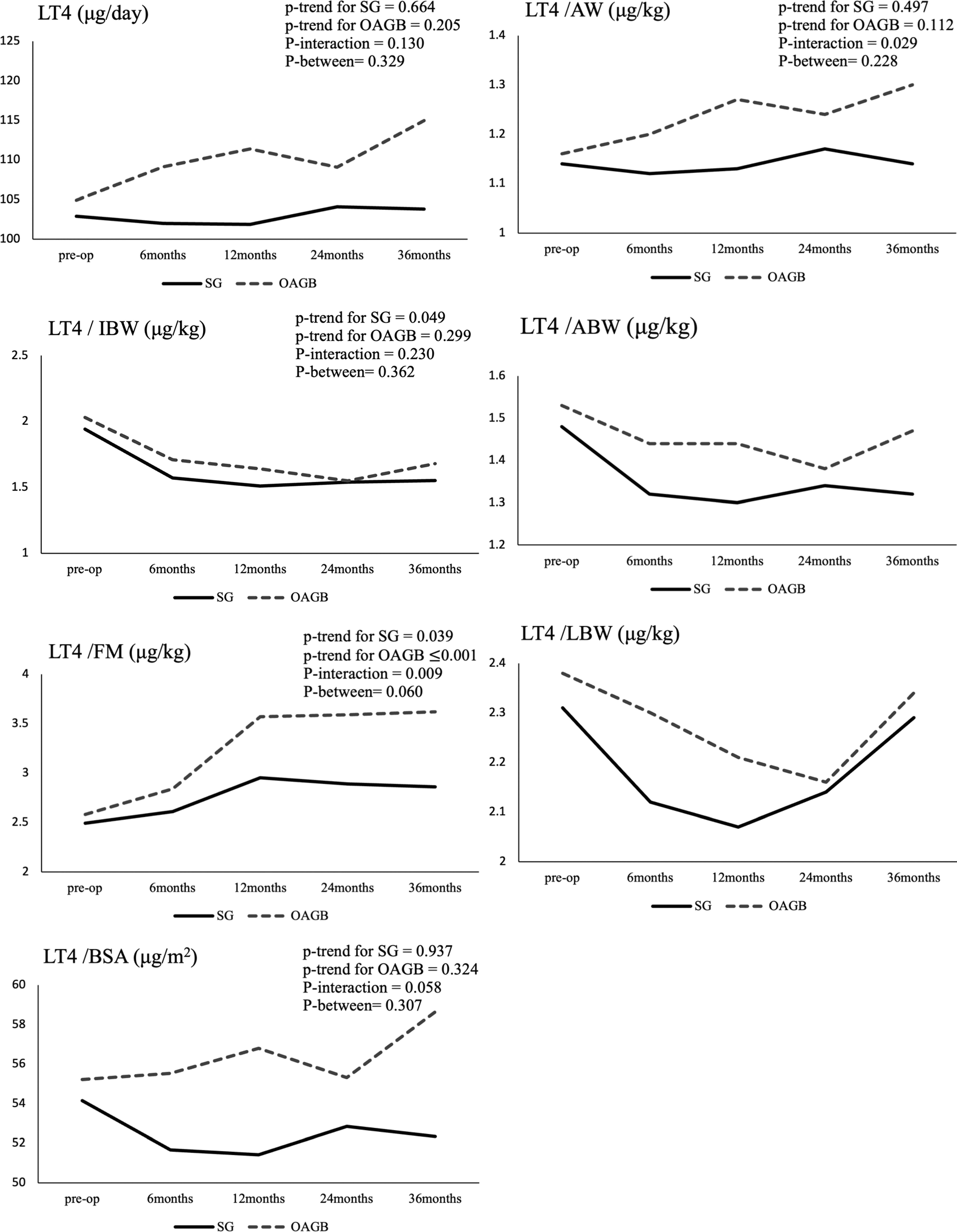
Changes in levothyroxine requirement during three years of follow-up in patients undergoing sleeve gastrectomy (SG) and one anastomosis gastric bypass (OAGB). LT4, levothyroxine; FM, fat mass; AW, actual weight; LBW, lean body weight; BSA, body surface area; IBW, ideal body weight; ABW, adjusted body weight. p-values for between-group comparison have been presented.
Post-Bariatric Surgery Levothyroxine Requirement Based on Body Composition Components During Three Years of Follow-up
Data are presented as median (25–75 IQ).
Values were adjusted for weight alteration, excluding LT4/AW (μg/m2) (not applicable), and values <0.05 were considered statistically significant.
SG, sleeve gastrectomy; OAGB, one anastomosis gastric bypass; LT4, levothyroxine; FM, fat mass; AW, actual weight; LBW, lean body weight; BSA, body surface area; IBW, ideal body weight; ABW, adjusted body weight; n, number of patients.
Thyroid function
In the case of TSH (mIU/L) measurements over time, we observed a significant decrease in the SG group (ptrend = <0.001), but not in the OAGB group (ptrend = 0.59). However, we observed no significant change in T4 (ng/dL) levels in either group (Table 5).
Thyroid Function Status During the Three Years of Follow-up After Bariatric Surgery
TSH values are reported as median (25–75 IQ), and T4 values are reported as mean ± SD.
p values <0.05 were considered statistically significant.
n, number of patients; TSH, thyrotropin; SG, sleeve gastrectomy; OAGB, one anastomosis gastric bypass.
Discussion
In this prospective study on obese individuals with hypothyroidism undergoing BS, there was no significant change in TSH (mIU/L) and T4 (ng/dL) levels after BS in the OAGB group. However, TSH (mIU/L) decreased in the SG group. At the end of the third year of follow-up, most participants undergoing BS experienced a reduction in the total LT4 (μg/day) intake, and this reduction was more prominent among the SG group. In contrast, a minority of participants, mostly in the OAGB group, experienced dose elevation. Evaluating the LT4 requirements during the follow-up in considering different body composition components demonstrated that LT4/FM (μg/kg) was the only parameter that significantly increased in both the surgery groups. Interestingly, patients who underwent OAGB experienced a greater elevation of LT4/FM (μg/kg) compared to the SG group. Moreover, given that a great percentage of fat reduction occurs during the first year following the surgery, intensive dose adjustments during this period are to be expected.
Anatomical and physiological alterations in the gastrointestinal tract following BS may influence the absorption of a wide spectrum of medications at multiple levels. 24 –26 The influence of BS on the absorption and pharmacokinetics of LT4 is still under investigation. 27,28 From a physiological perspective, the administration of antacid drugs and creating a smaller gastric pouch increase gastric PH, 29,30 and this is while LT4 absorption is PH dependent and requires PH equal to 1 for complete solubility. 4,31
In this study, evaluating the LT4 requirements according to different body composition components, we showed that LT4/FM (μg/kg) was the only parameter demonstrating increases over time in both the surgery groups. In contrast to our results, Trimboli et al. 32 followed 40 Swedish adults for 12 months after BS and observed no significant change in TSH after surgery. Moreover, they indicated that, despite a significant weight reduction following the surgery, the daily dose of LT4 (μg/day) remained unchanged, accompanied by an increasing trend in LT4/AW (μg/kg). In another retrospective observational study on 31 participants, Richou et al. 33 found an absolute reduction in the dosage of LT4 (μg/day) one year after SG. Likewise, Azran et al., 11 in a meta-analysis of 9 trials (including 519 participants), declared that BS could significantly reduce LT4 requirements; however, we did not observe such an association after adjusting for weight. Of note, Azran et al. reported a high degree of heterogeneity among the included studies (I 2 = 67%, p = 0.0007), mainly attributed to differences in follow-up durations. Recently, Valina et al. 34 analyzed 48 individuals who underwent SG and RYGB, and absolute LT4 and LT4/IBW (kg) remained unchanged after 12 months of follow-up irrespective of the type of surgery. However, they also reported that LT4/BSA (m2), LT4/AW (kg), LT4/ABW (kg), LT4/FM (kg), and LT4/LBM (kg) showed increments. 34
We acknowledge that our study has several limitations. First, our complete follow-up rates at 6, 12, 24, and 36 months postsurgery were approximately 86%, 91%, 70%, and 67%, respectively. Second, LT4 dosage was adjusted based on the patient’s TSH and fT4 levels and at the discretion of an endocrinologist without any predefined protocol. Third, hypothyroid participants were enrolled regardless of the underlying etiology (Hashimoto or postablative hypothyroidism), yet postablative hypothyroidism was infrequent (n = 27). Fourth, this was a prospective observational cohort study without randomized assignment of participants to surgery groups, so there were some differences in baseline characteristics between the groups. Despite these limitations, to the best of our knowledge, our study was the first observational prospective cohort study with three years of follow-up, evaluating LT4 dose requirements with attention to various body composition components and weight alterations. In addition, our study provided valuable information regarding the outcomes of OAGB, which is understudied compared to RYGB and SG.
Conclusion
Most of our participants with primary hypothyroidism required a dose reduction of LT4 (μg/day) or at least had no change in dose requirements until 36 months after SG or OAGB. LT4/FM (μg/kg) increased among patients who underwent SG or OAGB, suggesting that FM, as an important body composition component, could have a potential impact on post-BS LT4 requirements. Our results are important for consideration in the care of hypothyroid patients undergoing BS. However, larger prospective studies with a longer duration of follow-up are needed to confirm our results.
Footnotes
Acknowledgments
The authors thank the hospital staff, assistants, and coordinators who participated in this research. Also, special thanks to Mohammadreza Golsibi for his assistance and support with the electronic data collection system.
Authors’ Contributions
M.B.: Study design, data collection, coordination of patients’ issues, article preparation, and the final approval of the article; D.M.: Data collection, literature review, and article preparation; M.M.: Data analysis, data interpretation, and article preparation.; A.K.: Study design, performing surgeries, and the final approval of the article; S.S.: Data collection, literature review, and article preparation; M.V.: Study design, revising the article, and final approval of the article; F.A.: Study design, revising the article, and final approval of the article; F.H.: Study design, article preparation, revising the article, and final approval of the article. All authors reviewed and approved the final draft.
Author Disclosure Statement
The authors declare that they have no financial or nonfinancial competing interest.
Funding Information
The study was supported by the deputy of research and technology of Shahid Beheshti University of Medical Sciences (![]() ). Each author confirms that their research is supported by the Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, where education and research are the primary functions.
). Each author confirms that their research is supported by the Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, where education and research are the primary functions.