
Abstract
Background:
Skip metastases, node metastases in the lateral neck sparing the ipsilateral central neck, challenge the current concept of central-to-lateral lymphatic spread. This study sought to delineate patterns of central and lateral neck involvement in unilateral papillary thyroid cancer (PTC) and medullary thyroid cancer (MTC).
Methods:
This was a retrospective correlative analysis of nodal patterns in surgical specimens from patients with unilateral PTC or MTC who had undergone thyroidectomy with at least ipsilateral central neck dissection between November 1994 and January 2024 at a tertiary referral center.
Results:
Included were 833 patients with unilateral PTC and 640 patients with unilateral MTC. Simultaneous presence or absence of node metastases was noted in ipsilateral central and lateral neck compartments in 76.6–78.1% of patients with PTC (both node positive in 27.0–54.7% and both node negative in 23.4–49.6%) and 77.3–80.0% of patients with MTC (both node positive in 26.6–33.2% and both node negative in 44.1–53.4%). Only one ipsilateral neck compartment was node positive in 21.9–23.4% of patients with PTC and 20.0–22.7% of patients with MTC. The ipsilateral central, but not the ipsilateral lateral compartment, was node positive in 8.8–16.9% with PTC and 8.6–8.8% of patients with MTC, whereas the ipsilateral lateral, but not the ipsilateral central compartment, was node positive in 6.5–13.1% with PTC and 11.3–14.1% with MTC. Ipsilateral lateral neck involvement sparing the ipsilateral central neck was 1.5–2 times more frequent in patients with node positive MTC than patients with node positive PTC (24.2–25.2% vs. 12.9–17.1%). Greater numbers of node metastases in the ipsilateral central neck compartment were associated with more frequent involvement of the ipsilateral lateral, contralateral central, and contralateral lateral neck compartments. Thyroid tumor diameter intensified nodal spread without changing nodal spread patterns.
Conclusions:
These histopathological findings, which need to be interpreted in light of the respective tumor biology, offer an unprecedented glimpse at the metastatic patterns of unilateral PTC and MTC. Customizing neck dissection to the patterns of nodal spread, considering operative status (initial vs. reoperative surgery) and experience with neck dissection, may require more frequent concomitant dissections of ipsilateral central and ipsilateral lateral neck compartments.
Introduction
Although they differ a great deal in embryology and cellular origin, papillary thyroid cancer (PTC) and medullary thyroid cancer (MTC) are notorious for spreading from the thyroid gland in the central neck to central and lateral neck nodes. 1,2 Systematic neck dissection is intended to enhance regional control rates, improving the efficacy of radioactive iodine therapy for PTC and achieving biochemical cure for MTC.
Follicular thyrocytes, which PTC derives from, are dispersed throughout the entire thyroid gland. Conversely, calcitonin-secreting parafollicular C cells, which MTC originates from, concentrate more in the central portions of the middle and upper thirds of the thyroid lobes. 3,4 These differences in distribution of the respective cells of origin within the thyroid gland conceivably cause diverging patterns of node metastases in PTC and MTC reflecting the position of the metastatic primary tumor within the thyroid gland.
Notwithstanding these differences, cancer cells are thought to migrate from the thyroid gland through the lymphatic system in a contiguous fashion to the central neck nodes, dubbed “the first echelon of lymph nodes in metastatic thyroid carcinoma,” 5 and from there to lateral neck nodes. 6,7 However, skip metastases, that is, lateral node metastases sparing the ipsilateral central neck compartment, 8 throw into question the current concept of central-to-lateral nodal spread.
Despite an abundance of literature on the subject, nodal patterns across a wide range of small and large thyroid tumors remain ill-defined for PTC and MTC alike. This lack of comprehensive histopathological data has produced differing recommendations for neck dissection, such as ipsilateral or bilateral central node dissection electively or as default, 9 –14 with or without differentiation by primary tumor size with a 1-cm cutoff, 9 or guided by serum calcitonin levels in MTC. 13
The present combined clinical and pathological investigation, capitalizing on a large amount of carefully examined surgical specimens from systematic compartment-oriented neck dissections at a tertiary referral center over three decades, was devised to map the anatomic patterns of nodal spread of thyroid cancer in far greater depth than currently available from the international literature.
Patients and Methods
Inclusion and exclusion criteria
Included in this retrospective study were all patients with unilateral PTC or MTC who had undergone thyroidectomy with at least ipsilateral central neck dissection between November 1994 and January 2024 at the Department of General, Visceral and Endocrine Surgery, which represented the standard of care at the time of operation. Informed consent had been obtained from each patient in accordance with the amended Declaration of Helsinki as revised in 2013 and respective national and local regulations (institutional review board approval reference 2020-237). Sporadic MTC and hereditary MTC were analyzed together because survival and outcome are similar for sporadic and hereditary MTC of the same tumor stage. 15
Excluded from analysis were all patients who met one or more of the following criteria: Node dissection at other hospitals before the initial referral—to avoid misclassification of previously cleared neck compartments as node negative; Multiple tumors in both thyroid lobes or in the thyroid isthmus on histopathological evaluation—to circumvent misallocation of node metastases to nonmetastatic neck sides; No dissection of the ipsilateral central neck compartment at the Department of General, Visceral and Endocrine Surgery.
Surgical morbidity, impacted by operative status and experience and the extent of surgery, and clinical outcome, influenced by tumor stage and differences in tumor biology between PTC and MTC, were outside the remit of this anatomic study of nodal spread.
Compartment-oriented neck dissection
Systematic dissection of the central neck nodes, extending vertically from the hyoid bone to the thoracic inlet and horizontally between the trachea and the carotid sheath (American Joint Committee on Cancer [AJCC] level VI nodes 16 ), had been prompted by clinical findings on high-resolution ultrasound imaging, typically evidence of enlarged nodes, with or without preoperative confirmation by fine-needle aspiration cytology, and/or on intraoperative frozen section. Reoperations after primary operations carried out at other facilities included completion thyroidectomy complemented by the addition of central neck dissection.
For lateral neck nodes suspicious on imaging, systematic lateral neck dissection had been added, proceeding laterally from the carotid sheath to the trapezius muscle and inferiorly from the subclavian vein to the hypoglossal nerve superiorly (AJCC level II–V nodes 16 ).
In patients with MTC, dissections had been guided also by the level of serum calcitonin, specifically when this had been high to start with, 17 or had persisted after thyroid surgery elsewhere.
All operations had been performed using optical magnification and bipolar coagulation, supported by intraoperative nerve monitoring starting in December 1997.
Histopathological examination
Surgical specimens of thyroid and neck compartments had been analyzed separately (thyroid vs. extrathyroid tissue and nodes) by experienced board-certified pathologists. Paraffin-embedded thyroid specimens had been stained with hematoxylin and eosin and calcitonin as appropriate.
A diagnosis of PTC or MTC was based on histopathologic criteria proposed by the World Health Organization. 18 Thyroid tumor size and tumor extension by continuity, irrespective of the degree of invasion, had been routinely determined on histopathological examination. A diagnosis of node metastasis, unlike a diagnosis of distant metastasis, always required histopathological confirmation.
RET screening
Patients with MTC had undergone REarranged during Transfection (RET) screening after genetic counseling under separate informed consent. For screening of relevant RET exons, DNA had been purified from peripheral blood leukocytes according to standard procedures.
Statistical analysis
Data were stratified by primary tumor diameter and evaluated for presence versus absence of node metastases per neck compartment.
Unless explicitly pointed out, missing data were not replaced, and the number of individuals analyzed per dissected neck compartment was specified throughout (worst-case scenario).
Neck compartments that had not been dissected and thus were excluded from initial analysis for lack of histopathological data on nodal status were reclassified as node negative on an exploratory basis and evaluated as node negative highlighting this fact (best-case scenario).
For statistical analysis, the software package SPSS® version 28 (IBM, Armonk, New York, USA) was used.
Absolute and relative frequencies of categorical variables were compared with the use of the two-tailed Fisher’s exact test. Continuous variables, reported as medians with interquartile ranges, were tested using the two-tailed Mann–Whitney–Wilcoxon test. Multiple testing was corrected for with the Bonferroni method as appropriate. 19
The level of statistical significance (all values were two-tailed) was set at p < 0.05.
Results
Figure 1 shows the flow of all 3231 patients with PTC or MTC referred for neck surgery to the authors’ institution.
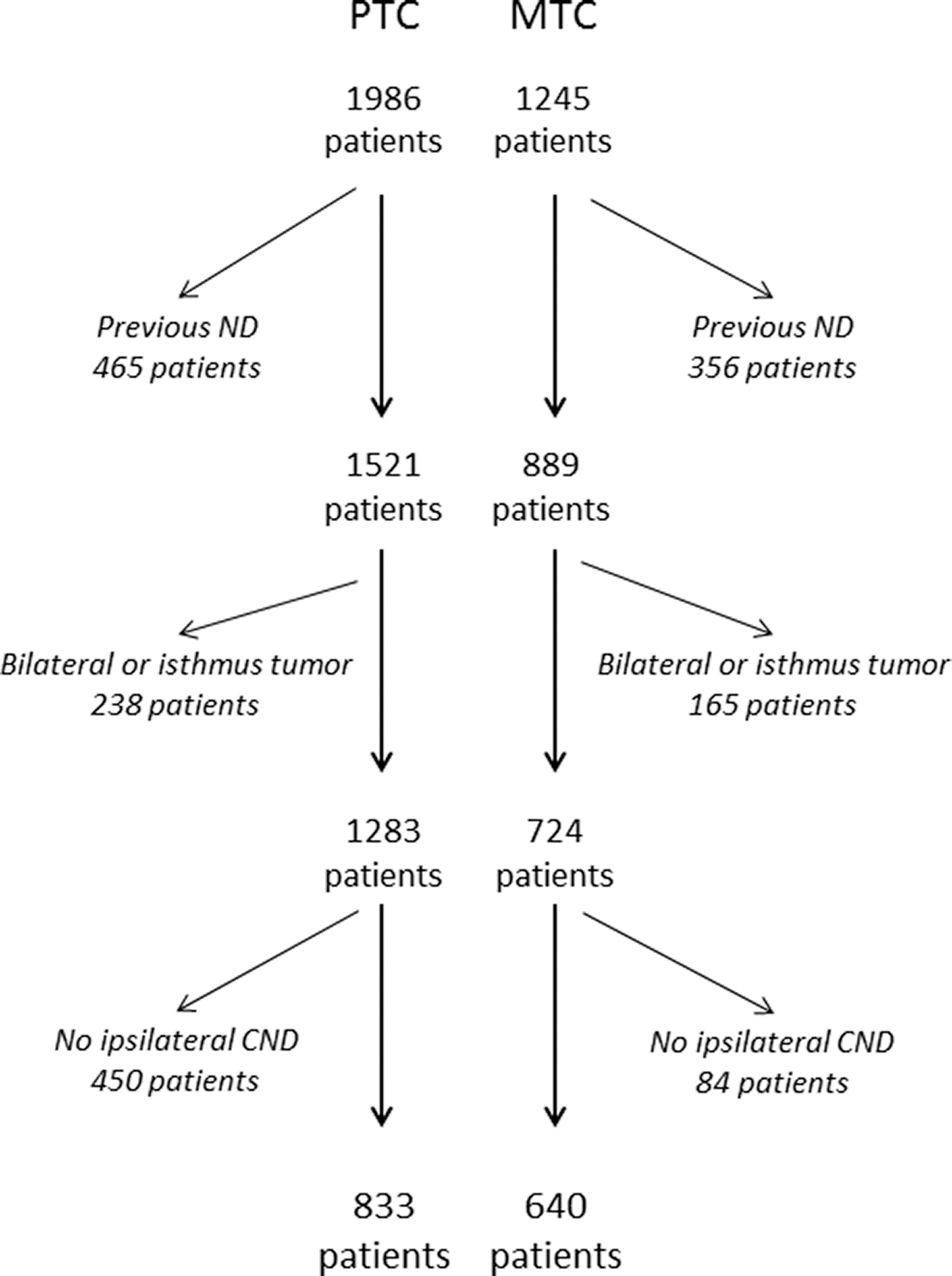
Patient flow. CND, central neck dissection; MTC, medullary thyroid cancer; ND, neck dissection; PTC, papillary thyroid cancer.
Because they had been subjected to neck dissection elsewhere, 821 patients referred for reoperation were excluded, leaving 2410 patients.
Of these 2410 patients, another 403 patients were excluded owing to primary tumors in both thyroid lobes and/or the thyroid isthmus, leaving 2007 patients.
Finally, 534 (26.7%) of the 2007 patients with unilateral PTC or MTC had not undergone an ipsilateral central node dissection, leaving 833 patients with unilateral PTC and 640 patients with unilateral MTC for analysis.
Characteristics of patients with unilateral papillary versus medullary thyroid cancer
Table 1 compares the clinical characteristics of patients with unilateral PTC with patients with unilateral MTC referred to the authors’ institution.
Characteristics of Patients with Unilateral Papillary versus Medullary Thyroid Cancer a
Values in parentheses denote column percentages.
Patients with unilateral primary thyroid tumors only without prior neck dissection (excluding tumors in both thyroid lobes or in the isthmus).
No evidence of pathogenic RET germline mutation in codons 609, 611, 618, 620, 630, 768, 790, 804, 891, or 918.
Study inclusion criterion.
Statistically significant after correction for multiple testing.
IQR, interquartile range; MTC, medullary thyroid cancer; N/A, not assessable; PTC, papillary thyroid cancer.
Mirroring inherent tumor characteristics, patients with MTC were less often female (55.5 vs. 68.2%), older at thyroidectomy (medians of 55 vs. 44 years) and had been referred more often for initial operations (78.0 vs. 51.6%) than patients with PTC. The former also had smaller thyroid tumors (medians of 15 vs. 18 mm) with infrequent extrathyroid extension (16.9 vs. 34.4%) and more frequent distant metastases (10.0 vs. 5.5%) than the former (Table 1).
The percentages of ipsilateral and contralateral central neck dissection were comparable, whereas lateral neck dissections were more common in MTC (80.0 vs. 49.3% ipsilaterally and 64.1 vs. 19.7% contralaterally) than PTC, resulting in the removal of more neck nodes (medians of 45 vs. 18 nodes; Table 1).
Patterns of node metastases stratified by thyroid tumor size in unilateral papillary and medullary thyroid cancer (worst-case scenario)
Table 2 illustrates the patterns of node metastases for PTC and MTC, stratified by largest thyroid tumor diameter, for each dissected neck compartment under a worst-case scenario.
Patterns of Node Metastasis by Primary Tumor Size in Unilateral Papillary and Medullary Thyroid Cancer a (Worst-Case Scenario)
Numbers are percentages of involved neck compartments, with numbers of involved/dissected compartments added in parentheses.
Patients with unilateral primary thyroid tumors only without prior neck dissection (excluding tumors in both thyroid lobes or in the isthmus).
MTC, medullary thyroid cancer; PTC, papillary thyroid cancer.
In PTC (upper panel), percentages of node metastases always were greater in lateral than in central neck compartments (67.2 vs. 43.1% ipsilaterally and 37.8 vs. 22.3% contralaterally).
In MTC (lower panel), percentages of node metastases were greater in ipsilateral lateral (45.9 vs. 33.9%) than in ipsilateral central neck compartments, whereas the corresponding percentages for the contralateral lateral and central neck compartments were similar (16.5 vs. 18.1%).
Although larger PTCs and MTCs had developed more often node metastasis across all neck compartments, the patterns of node metastases, barring random variation, were independent of thyroid tumor diameter (Table 2).
Patterns of node metastases stratified by thyroid tumor size in unilateral papillary and medullary thyroid cancer (best-case scenario)
The greater involvement of lateral neck compartments, as compared with central neck compartments, provided clues to suggest that lateral compartments had been targeted more often for suspicious neck nodes than central neck compartments. To accommodate for this, data were reclassified such that undissected neck compartments were counted as node negative.
Table 3 depicts the patterns of node metastases for PTC and MTC, stratified by largest thyroid tumor diameter, for each neck compartment under a best-case scenario.
Numbers are percentages of involved neck compartments, with numbers of involved/dissected compartments added in parentheses.
Patients with unilateral primary thyroid tumors only without prior neck dissection (excluding tumors in both thyroid lobes or in the isthmus).
Counting undissected contralateral central compartments and ipsilateral and contralateral lateral neck compartments as node negative.
MTC, medullary thyroid cancer; PTC, papillary thyroid cancer.
In PTC (upper panel), now exclusively lower percentages of node metastases were obtained for lateral than for central neck compartments (32.3 vs. 43.1% ipsilaterally and 7.2 vs. 21.4% contralaterally).
In MTC (lower panel), the percentages of node metastases were still greater in the ipsilateral lateral than in the ipsilateral central neck compartment (36.4 vs. 33.9%) and still lower in the contralateral lateral than in the contralateral central neck compartment (10.4 vs. 17.0%).
Although nodal patterns were unaffected by thyroid tumor diameter, larger thyroid tumors were associated with more frequent node metastasis across all neck compartments (Table 3).
Figure 2 provides a condensed graphic illustration of the patterns of nodal spread for unilateral PTC and MTC.
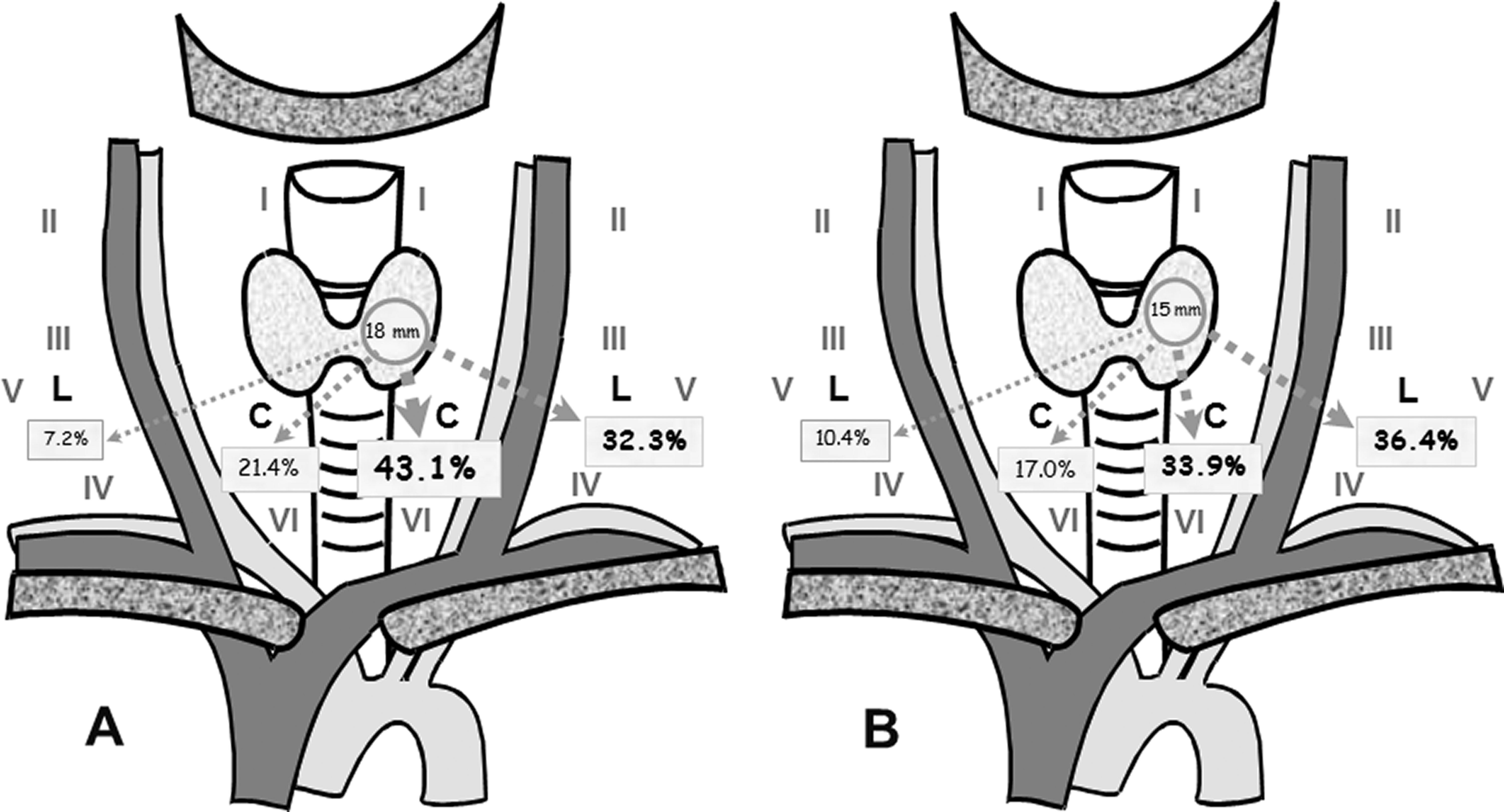
Patterns of nodal spread in unilateral papillary and medullary thyroid cancer (best-case scenario).
Patterns of node metastasis by primary tumor diameter and ipsilateral central node metastases in unilateral papillary and medullary thyroid cancer (best-case scenario)
To determine the suitability of the ipsilateral central neck compartment for predicting involvement of the other neck compartments, patterns of node metastases were stratified by thyroid tumor diameter and number of ipsilateral central node metastases under a best-case scenario.
On these exploratory analyses (Tables 4 and 5), greater numbers of node metastases in the ipsilateral central neck compartment were paralleled by more frequent involvement of the ipsilateral lateral, contralateral central, and contralateral lateral neck compartments, independent of thyroid tumor diameter.
Numbers denote involved neck compartments, with percentages of involvement per neck compartment in parentheses.
Patients with unilateral primary thyroid tumors only without prior neck dissection (excluding tumors in both thyroid lobes or in the isthmus).
Counting undissected contralateral central compartments and ipsilateral and contralateral lateral neck compartments as node negative.
Numbers denote involved neck compartments, with percentages of involvement per neck compartment in parentheses.
Patients with unilateral primary thyroid tumors only without prior neck dissection (excluding tumors in both thyroid lobes or in the isthmus).
Counting undissected contralateral central compartments and ipsilateral and contralateral lateral neck compartments as node negative.
These patterns of nodal spread across neck compartments were comparable in PTC (Table 4) and MTC (Table 5).
Breakdown of ipsilateral central and lateral neck involvement in unilateral papillary versus medullary thyroid cancer (worst-case scenario vs. best-case scenario)
Table 6 details absolute and relative frequencies for various constellations of ipsilateral neck involvement in unilateral PTC and MTC, enabling calculation of percent range estimates marked by worst-case and best-case scenarios.
Breakdown of Ipsilateral Central and Lateral Neck Involvement in Unilateral Papillary versus Medullary Thyroid Cancer b
Numbers denote neck compartments, with column percentages in parentheses. Owing to rounding, not all percentages match up.
+ indicates the presence of node metastases, whereas - indicates the absence of node metastases in the respective neck compartment.
Patients with unilateral primary thyroid tumors only without prior neck dissection (excluding tumors in both thyroid lobes or in the isthmus).
Counting undissected ipsilateral lateral compartments as node negative.
MTC, medullary thyroid cancer; PTC, papillary thyroid cancer.
Simultaneous presence or absence of node metastases was noted in ipsilateral central and lateral neck compartments in 76.6–78.1% of patients with PTC (both node positive in 27.0–54.7%, and both node negative in 23.4–49.6%) and 77.3–80.0% of patients with MTC (both node positive in 26.6–33.2% and both node negative in 44.1–53.4%).
Conversely, only one ipsilateral neck compartment was node positive in 21.9–23.4% of patients with PTC and 20.0–22.7% of patients with MTC. The ipsilateral central, but not the ipsilateral lateral compartment, was node positive in 8.8–16.9% with PTC and 8.6–8.8% of patients with MTC, whereas the ipsilateral lateral, but not the ipsilateral central compartment, was node positive in 6.5–13.1% with PTC and 11.3–14.1% with MTC.
Ipsilateral lateral neck involvement sparing the ipsilateral central neck was 1.5–2 times more frequent in patients with node positive MTC than patients with node positive PTC (24.2–25.2% vs. 12.9–17.1%).
These data were fairly accurate, as reoperations revealed. Previously unappreciated node metastases were subsequently removed from initially node negative ipsilateral central neck compartments in one patient with PTC and in two patients with MTC 53, 116, and 145 months after the initial operation, and from two patients with MTC 181 and 205 months after the first reoperation at the authors’ institution (data not shown).
Discussion
This large-scale anatomical study of locoregional metastatic patterns in 1473 patients with unilateral PTC or MTC found that involvement or noninvolvement was concordant between ipsilateral central and ipsilateral lateral neck compartments in more than 75% of patients. Greater numbers of node metastases in the ipsilateral central neck compartment signaled more frequent involvement of ipsilateral lateral and, to a lesser degree, of contralateral central and contralateral lateral neck compartments. Larger thyroid tumors slowly, but steadily intensified nodal spread without changing nodal spread patterns.
These findings, which were consistent across thyroid tumor entities and apply to other clinical settings, demonstrated that neck compartments do not represent self-contained anatomical units but form one interwoven lymphatic drainage system holding clinically important information for surgeons.
A key strength of our data was biological plausibility, reflecting the distribution of thyrocytes throughout the entire thyroid gland in PTC and parafollicular C cell accumulations in the central portions of the middle and upper thirds of the thyroid lobes in MTC. As for skip metastases, the position of the metastatic primary tumor within the thyroid gland may be clinically more relevant than tumor entity:
20
–22
upper thyroid: spreading through lymphatic channels along the superior thyroid vein to the ipsilateral lateral neck, giving rise to “skip” metastases;
mid and lower thyroid: spreading first through lymphatic channels along the middle thyroid vein to the ipsilateral central and lateral neck and through lymphatic channels along the inferior thyroid vein to the central neck.
thyroid isthmus: spreading first through lymphatic channels along the inferior thyroid vein and the thyroid ima vein to the ipsilateral and contralateral central neck and the upper anterior mediastinum.
This large correlative study of surgical specimens was limited by its retrospective design, specifically the inability to control for bias. Easier detection of suspicious neck nodes in the lateral neck, which are concealed less by concomitant thyroid pathology than central neck nodes, triggered more lateral neck dissections, generating greater percentages of node metastases in the lateral neck—although lateral nodes overall were dissected less often than central neck nodes (Table 2). For this reason, detection bias should have affected patients with PTC more than patients with MTC. This rationale prompted reclassification of all “undissected” neck compartments as “node negative” and exploratory reanalysis of reclassified data. It cannot be ruled out, though, that this exploratory approach may have misclassified some neck compartments harboring occult node metastases as “node negative.”
Referral bias, enriching tertiary surgical centers with patients with advanced disease, is another noteworthy point. Intense nodal spread commonly translates into larger, more suspicious neck nodes which, representing the “tip of the iceberg,” are easier to pick up on imaging than nodal micrometastases. However, the maximum diameter of node metastases had not been systematically recorded for each neck compartment, precluding evaluation of nodal spread by maximum nodal size. That said, nodal spread, how extensive it may be, is unlikely to differ by the lymphatic pathways recruited, yielding similar patterns of neck involvement.
In spite of these commonalities, there are considerable biological differences between PTC and MTC resulting in different clinical outcomes for comparable tumor stages. Radioiodine therapy represents effective nonsurgical treatment for PTC, whereas no equally effective nonsurgical treatment exists for MTC. Because of their miliary growth, node metastases from MTC generally are too small for fine needle aspiration, eluding most advanced imaging technologies, whereas node metastases from PTC tend to be larger and visualize on radioiodine scans.
Owing to biomarker-based risk stratification, 17 patients with MTC had lateral neck compartments dissected more often (80.0% in MTC vs. 49.3% in PTC ipsilaterally, and 64.1% in MTC vs. 19.7% in PTC contralaterally; Table 1) than patients with PTC. Unless nodal spread is massive, compartment-oriented neck surgery in experienced hands can accomplish long-term locoregional control.
Recent evidence from sporadic MTC
23
points towards the usefulness of a more dynamic, personalized concept that starts off with a diagnostic ipsilateral central neck dissection for clinically in apparent primary thyroid tumors: When the ipsilateral central neck specimen is node negative on frozen section, it is generally safe to forgo dissection in the ipsilateral lateral neck. When the ipsilateral central neck specimen is node negative in conjunction with a thyroid tumor in the upper third of the thyroid lobe,
22
the ipsilateral lateral neck may be considered for exploration with the use of intraoperative frozen section, in particular when lateral nodes are suspicious on imaging. When the ipsilateral central neck specimen is node positive on frozen section, the ipsilateral lateral neck should be considered for exploration, in particular when lateral nodes were suspicious on imaging or metastatic based on fine-needle aspiration cytology with or without thyroglobulin and calcitonin washout, respectively. When the ipsilateral lateral neck compartment is node positive, the ipsilateral central neck compartment typically is node positive as well, calling for ipsilateral central neck dissection.
14,22
When ipsilateral neck compartments are tumor-free, the contralateral lateral neck compartment is rarely node positive, requiring dissection for clinically suspicious nodes only. Although larger tumors are associated more often with node metastasis, this does not change the patterns of node metastases, as detailed in Tables 2–5. This observation argues against the use of primary tumor size as a major selection criterion for systematic neck dissection.
Avoidance of bilateral central neck dissection, when oncologically justified, protects the contralateral parathyroid glands and the contralateral recurrent laryngeal nerve, limiting the risk of postoperative hypoparathyroidism and recurrent laryngeal nerve palsy. 14
Conclusions
To sum up, careful evaluation of our large body of real-word evidence data uncovered similar percentages of node metastasis in the ipsilateral central and ipsilateral lateral neck compartments, both of which were positive or negative in more than 75% of patients with unilateral primary thyroid cancers, and greater percentages of skip metastases in patients with node positive MTC (24.2–25.2%) than in patients with node positive PTC (12.9–17.1%), reflecting drainage of the upper thyroid third through superior lymphatic channels.
These histopathological data offer an unprecedented glimpse at the metastatic patterns of PTC and MTC, which spread via the same lymphatic neck channels. Although they need to be interpreted in light of the respective tumor biology, the present results lay important groundwork for personalized treatment strategies marrying ultrasound screening with frozen section-guided neck surgery. Upfront localization of the primary thyroid tumor and suspicious neck nodes by ultrasound imaging and cognizance of the patterns of nodal spread form a starting point for planning compartment-oriented neck dissection for node positive PTC and MTC. Customizing neck dissection to the patterns of nodal spread, considering operative status (initial vs. reoperative surgery) and experience with neck dissection, may require more frequent concomitant dissections of ipsilateral central and ipsilateral lateral neck compartments than currently appreciated.
Footnotes
Authors’ Contributions
A.M.: Conceptualization, methodology, validation, formal analysis, investigation, and writing—original draft; K.L.: Investigation and writing—review and editing; F.W.: Investigation and writing—review and editing; H.D.: Conceptualization, methodology, investigation, writing—review and editing, and supervision.
Author Disclosure Statement
A.M., K.L., F.W., and H.D. have no conflict of interest to declare that could be perceived as prejudicing the impartiality of the research reported.
Funding Statement
A.M., K.L., F.W., and H.D. did not receive any specific grant for this research from any funding agency in the public, commercial, or not-for-profit sector.