
Abstract
Background:
Longer follow-up after radiofrequency ablation (RFA) of benign thyroid nodules is needed to understand regrowth and other causes of delayed surgery and long-term complications.
Methods:
This retrospective study included consecutive patients treated with RFA for symptomatic benign nonfunctioning thyroid nodules between March 2007 and December 2010. RFA was performed according to the standard protocol. We followed up patients at 1, 6, and 12 months, then yearly, until August 2022, and calculated the volume reduction ratio (VRR) at each follow-up. We assessed the incidence of regrowth according to three published criteria, delayed surgery, and complications. The Kaplan–Meier method was used to evaluate the cumulative incidence of regrowth, and univariable and multivariable Cox regression analyses were performed to identify risk factors for regrowth.
Results:
This study included 421 patients (mean age, 47 ± 13 years; 372 women) with 456 nodules (mean volume, 21 ± 23 mL). The median follow-up period was 90 months (interquartile range, 24–143 months). The mean VRR was 81% at 2 years, 90% at 5 years, and 94% at ≥10 years. Overall regrowth was noted in 12% (53/456) of nodules and was treated with repeat RFA (n = 33) or surgery (n = 4) or left under observation (n = 16). Thyroid nodules with ≥20 mL initial volume had significantly higher risk of regrowth compared with nodules with <10 mL initial volume (hazard ratio, 2.315 [95% confidence interval, 1.183–4.530]; p = 0.014 on multivariable Cox regression analysis). Delayed surgery was performed in 6% (26/421) of patients because of regrowth and/or persistent symptoms (n = 4) or newly detected thyroid tumors (n = 22), one benign and 21 malignant. The overall complication rate was 2.4% (10/421), with no procedure-related deaths or long-term complications.
Conclusion:
RFA is safe and effective for treating benign thyroid nodules, with a high VRR at long-term follow-up. Regular follow-up after initial success is warranted because of the possibility of regrowth of ablated nodules and the need for delayed surgery in some patients.
Introduction
Thyroid nodules are commonly found in clinical practice, with a prevalence ranging from 3% to 4% on palpation to 17–67% on ultrasound (US) examination. 1 Although cytologically benign, asymptomatic thyroid nodules are observed without treatment, some nodules causing cosmetic problems or pressure symptoms require treatment.
For the last two decades, imaging-guided thermal ablation (TA), especially radiofrequency ablation (RFA) and laser ablation (LA), has been established as a treatment for symptomatic benign thyroid nodules. 2,3 Evidence from previous retrospective and prospective studies and meta-analyses suggests the safety and efficacy of TA for reducing the volume of nodules, 2,4 –9 with a pooled volume reduction ratio (VRR) of 77% and a pooled overall complication rate of 4% in a meta-analysis. 4 International guidelines support the use of RFA and LA for the treatment of benign nonfunctioning thyroid nodules with local symptoms. 10 –13
However, regrowth of ablated nodules with recurrence of symptoms 3 years or longer after TA has been reported in some studies, with the incidence ranging from 24% to 38%. 14 –16 This poses a challenge for the long-term management of thyroid nodules after TA, and additional TA or surgery is sometimes required. 16 –19 Although several studies reported follow-up results beyond 3 years, 7,14,16,20 –24 studies with longer follow-up periods are needed to better understand regrowth and other causes of delayed surgery or long-term unpredictable complications after TA.
A study examined 10-year outcomes for LA and reported a VRR of 59% after 10 years and regrowth in 6% (11/171) of ablated nodules, treated surgically. 21 However, to the best of our knowledge, no studies have evaluated the outcomes of RFA within such a time frame.
Therefore, we carried out this study to evaluate the long-term efficacy and safety of RFA for the treatment of benign thyroid nodules and to determine the incidence of regrowth and delayed surgery after RFA.
Materials and Methods
This retrospective study was approved by the Institutional Review Board of Asan Medical Center (2022–1291), and the requirement for informed consent was waived. All patients provided written informed consent for treatment prior to procedures.
Patients
This study included consecutive patients treated with RFA for benign nonfunctioning thyroid nodules at a single tertiary center between March 2007 and December 2010. The inclusion criteria were as follows: (1) patients who underwent RFA for cytologically proven benign thyroid nodules confirmed on two separate fine needle aspiration (FNA) procedures, (2) cosmetic problems or pressure symptoms related to thyroid nodules, and (3) nonfunctioning thyroid nodules. Details of pretreatment evaluation and RFA procedures are described in the Supplementary Data S1.
Posttreatment follow-up
Patients were followed up at 1, 6, and 12 months after initial RFA, then yearly until August 2022, with US examination being used to calculate the nodule volume and a clinical evaluation used for symptom score and cosmetic grade. VRR was calculated as:
Changes in nodule volume and VRR were tracked after initial RFA for all ablated nodules. RFA was repeated if there was a residual vascularity within the undertreated nodule on color Doppler US with persistent symptoms or cosmetic problems. 22,25,26
Cure after RFA was defined as meeting all of the following criteria: (1) no change to a residual linear or flat hypoechoic lesion measuring <0.5 mL and with VRR ≥90%; (2) no vascularity inside the treated nodule; and (3) no symptoms or cosmetic problems related to the nodule.
Regrowth
Because there are different ways to define regrowth of ablated thyroid nodules, three criteria from the literature were adopted as follows: (1) >50% increase in volume from any previously recorded volume(s) 11,16,22,27 (criterion 1); (2) >20% increase in nodule volume from the volume at 1 year after RFA 28 (criterion 2); and (3) volume becoming larger than the initial nodule volume 29 (criterion 3). The incidence of regrowth was determined according to each criterion, and overall regrowth defined as meeting any of the three criteria was also calculated. The time to regrowth was defined as the interval between the initial RFA and the time point at which a certain criterion was met. If a nodule met two or three criteria for regrowth, the shortest interval was designated as the time to regrowth. The characteristics of the patients and nodules with regrowth and details of the management of regrown nodules were recorded.
Complications and side effects
Major and minor complications and side effects were reported according to the Society of Interventional Radiology reporting standards. 30 Major complications were defined as events leading to significant morbidity and disability, necessitating an increase in the level of care, admission to hospital, or a lengthened hospital stay. 30 All other complications were regarded as minor. Side effects were defined as expected undesired events that rarely resulted in significant morbidity. 30 Voice change persisting ≥1 month after RFA was considered major and that persisting <1 month was considered minor. 31 Pain resulting in cessation of RFA or persisting for more than 3 days was considered as minor. 31,32 Transient voice change occurring with lidocaine injection, a small amount of asymptomatic hemorrhage or parenchymal edema, and tolerable pain or discomfort were not considered as complications or side effects. 31,32 For each event, the time to recovery and its management were described.
Surgery
Data on patients who underwent thyroid surgery during follow-up after initial RFA were reported, including the interval between initial RFA and surgery, indication, extent (total thyroidectomy vs. lobectomy), pathology of the ablated nodule within the surgical specimen (if included), and presence or absence of lymph node or distant metastases in cases of malignancy. If an ablated nodule included in the surgical specimen was proven to be malignant, its subtype was reported and its initial FNA cytology sample was retrospectively reviewed by an experienced endocrinology pathologist (D.E.S.).
Statistical analysis
Continuous variables are presented as mean ± standard deviation and discrete variables as median with range. The incidence of complications and side effects was calculated as the number of events per patient and per session. The cumulative incidence of regrowth was determined at each follow-up point (6 and 12 months, then yearly) and presented as the total number of nodules that showed regrowth from 6-month follow-up to a certain follow-up point. The Kaplan–Meier method was used to evaluate the cumulative incidence of regrowth. Univariable and multivariable Cox regression analyses were performed to identify independent variables associated with regrowth. The Schoenfeld test was used to evaluate the proportional hazard assumption. Statistical significance was set at p <0.05. Statistical analyses were performed using MedCalc® Statistical Software version 20.218 (MedCalc Software Ltd, Ostend, Belgium), SPSS version 25.0 (SPSS Inc., Chicago, IL, USA), and R version 4.2.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Characteristics of the patients, nodules, and RFA
The baseline characteristics of the patients, nodules, and RFA are summarized in Table 1. Patient flowchart is shown in Figure 1. A total of 421 patients (mean age, 47 ± 13 years; 372 females) with 456 nodules were treated in 749 RFA sessions. The median number of RFA sessions per patient was one (range, 1–7), with 225 patients undergoing a single session of RFA. The median cosmetic grade and symptom score at initial RFA were four (range, 1–4) and two (0–10), respectively.
Baseline Characteristics of Patients, Nodules, and Radiofrequency Ablation
Not available for six nodules.
IQR, interquartile range; RFA, radiofrequency ablation; SD, standard deviation.
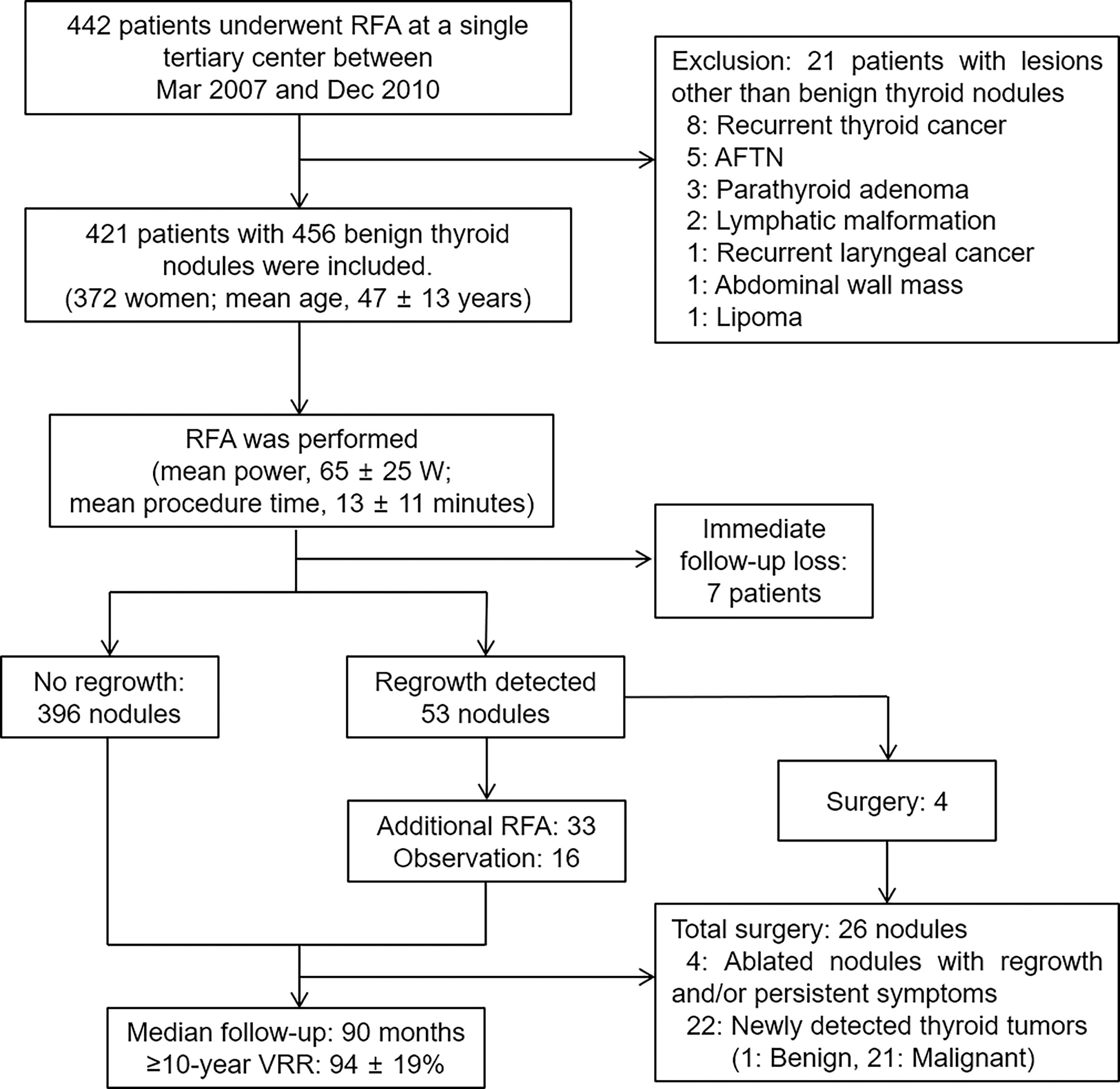
Patient flowchart. AFTN, autonomously functioning thyroid nodule; RFA, radiofrequency ablation; VRR, volume reduction ratio.
The mean initial volume of the 456 thyroid nodules was 21 ± 23 mL. A total of 172 nodules were smaller than 10 mL, 119 were between 10 mL and 20 mL, and 165 were 20 mL or larger. The mean RFA power was 65 ± 25 W and the mean procedure time was 13 ± 11 minutes.
Long-term outcomes of RFA
The median follow-up period per patient was 90 months (interquartile range, 24–143 months), and 162 patients (38%) were followed up for more than 10 years. Seven patients (2%) were lost to follow-up immediately after initial RFA.
Changes in nodule volume and VRR over a 10-year period are shown in Table 2 and Figure 2. At 6-month follow-up, the mean nodule volume was 9.0 ± 13.1 mL, with a mean VRR of 63% ± 19%. The mean VRR was 81% at 2 years and 90% at 5 years. The mean nodule volume at ≥10 years of follow-up was 2.6 ± 10.2 mL and the mean VRR was 94% ± 19%. Cure was achieved in 83 nodules (18%) in 76 patients (18%). The median cosmetic grade and symptom score at ≥10-year follow-up were two (range, 1–4) and zero (0–6), respectively.
Changes in Nodule Volume and Volume Reduction Ratio over a 10-Year Period After Radiofrequency Ablation According to Initial Nodule Volume
Numbers are mean ± standard deviation.
VRR, volume reduction ratio (ratio of the decrease in nodule volume to the initial volume).
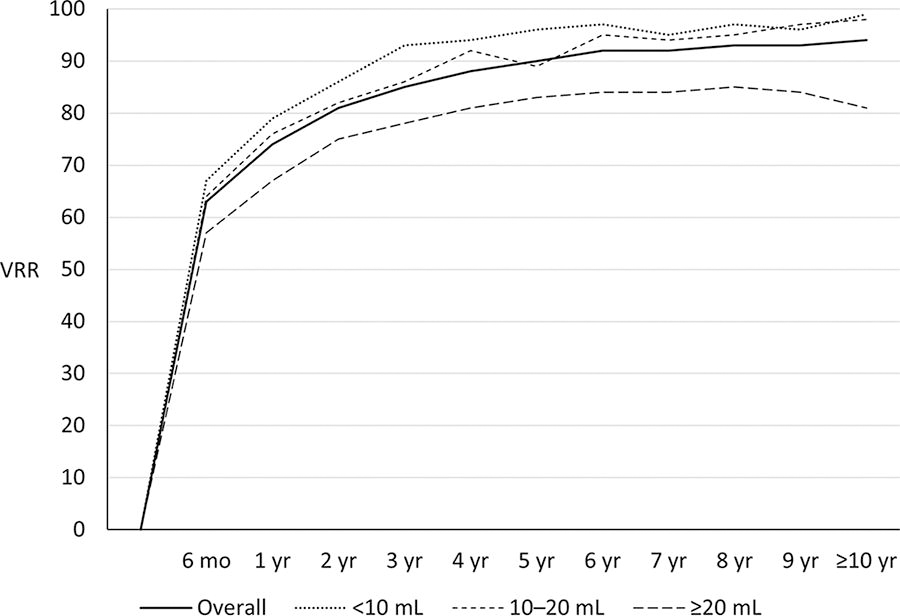
Changes in VRR (according to initial nodule volume) over a 10-year period after RFA.
In subgroup analysis according to initial nodule volume, the median number of RFA sessions was one (range, 1–4) for nodules with initial volume of <10 mL and 10–20 mL, and two (range, 1–7) for nodules with initial volume of ≥20 mL. For nodules with initial volume of <10 mL or 10–20 mL, the mean VRR of >80% was achieved at 2 years after initial RFA, whereas this level of VRR was reached at 4 years for nodules with initial volume of ≥20 mL. At ≥10 years of follow-up, the mean VRR was 99% ± 3% for nodules with initial volume of <10 mL, 98% ± 6% for those of 10–20 mL, and 81% ± 33% for those of ≥20 mL. The proportion of cured nodules was 34% (58/172) for nodules with a <10 mL initial volume, 18% (22/119) for 10–20 mL nodules, and 2% (3/165) for ≥20 mL nodules.
Incidence, characteristics, and risk factors of regrowth
The incidence and characteristics of regrown thyroid nodules after initial RFA are shown in Table 3. Overall regrowth (meeting any of the criteria 1–3) was noted in 12% (53/456) of thyroid nodules in 52 patients. Using the three different criteria, the incidence of regrowth per nodule was 11% (49/456) for criterion 1 (>50% increase from previously recorded volume), 7% (32/456) for criterion 2 (>20% increase from volume at 1 year), and 1% (5/456) for criterion 3 (follow-up volume larger than initial volume).
Characteristics of 53 Thyroid Nodules (in 52 Patients) with Regrowth During Follow-Up After Radiofrequency Ablation According to Three Different Criteria
Greater than 50% increase in nodule volume from any previously recorded volume(s).
Greater than 20% increase in nodule volume from the volume at 1 year after RFA.
Volume becoming larger than the initial nodule volume.
All were benign on surgical pathology.
One patient subsequently underwent surgery for a newly developed thyroid tumor.
The median time to regrowth was 4 years (range, 0.5–10 years) and the mean initial volume of regrown nodules was 29 ± 27 mL. The content of the regrown nodules was solid in 33 nodules (62%), predominantly solid in 17 nodules (32%), and predominantly cystic in three nodules (6%). The echogenicity was isoechoic in 47 nodules (89%) and hypoechoic in six nodules (11%). Vascularity was <25% in 25 nodules (47%), 25%–50% in 21 nodules (40%), 50–75% in six nodules (11%), and ≥75% in one nodule (2%).
The cumulative incidence of regrowth over a 10-year period after initial RFA is shown in Figure 3A. Regrowth was most frequently observed 1–4 years after initial RFA, with an incidence of 9–15 nodules per year. After 4 years, regrowth was noted in 2–4 nodules per year. The management of regrown nodules is summarized in Table 3. Repeat RFA was performed for 33 nodules and surgery for four nodules. The other 16 nodules were left under observation owing to the absence of cosmetic problems or symptoms related to the nodules and the refusal of further treatment. A patient among those observed subsequently underwent surgery for a newly developed thyroid tumor.
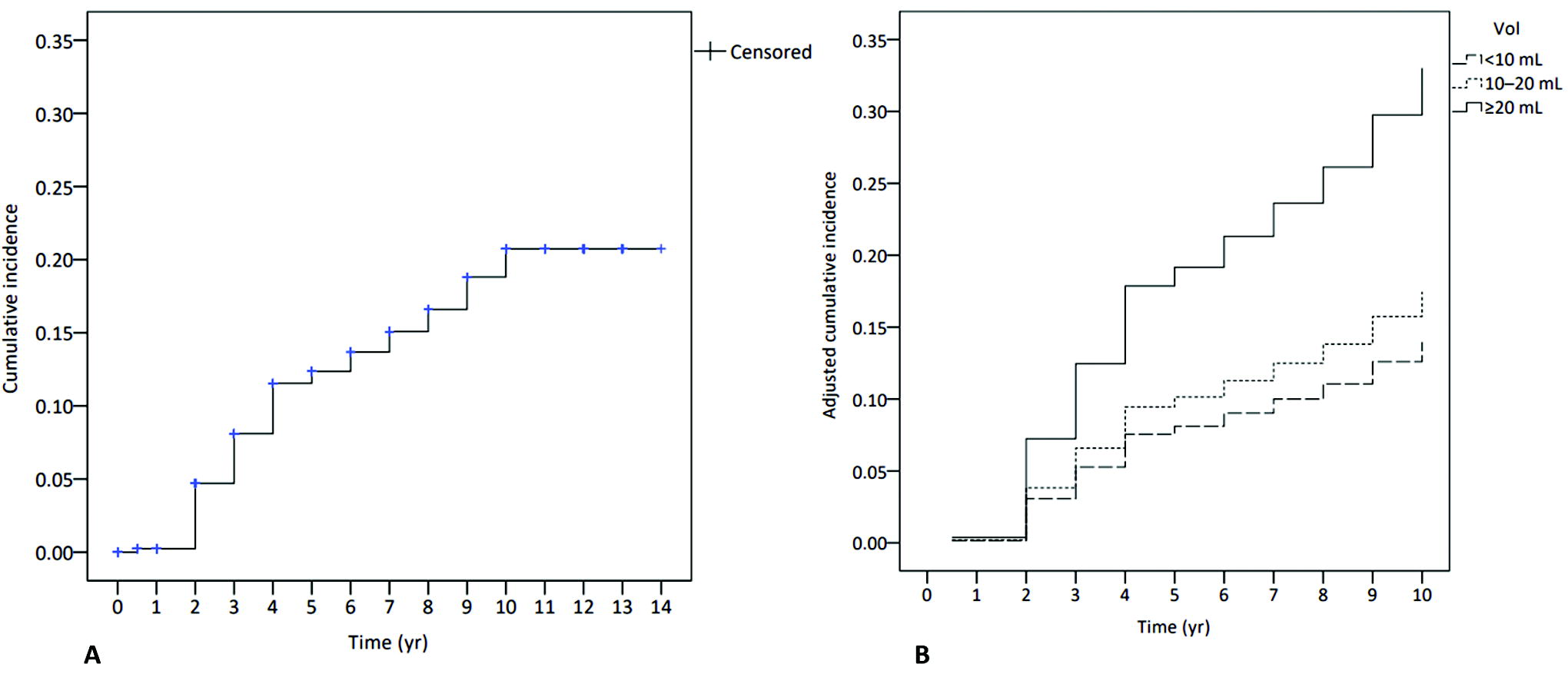
Cumulative incidence of regrowth among ablated thyroid nodules.
The results of univariable and multivariable Cox regression analysis of variables associated with regrowth are shown in Table 4. Thyroid nodules with an initial volume of ≥20 mL had a significantly higher risk of regrowth than nodules with an initial volume of <10 mL (hazard ratio, 2.315 [95% confidence interval (CI), 1.183–4.530]; p = 0.014 on multivariable Cox regression analysis). The adjusted cumulative incidence of regrowth according to initial nodule volume is shown in Figure 3B.
Univariable and Multivariable Analysis of Variables Associated with Regrowth
CI, confidence interval; Inf., infinite.
Complications of RFA
The complications and side effects of RFA are summarized in Table 5. The overall complication rate was 2.4% (10/421), with four major (1.0%) and six minor (1.4%) complications. The sole major complication was voice change (n = 4), which took 1–6 months for recovery. The minor complications were voice change taking <1 month for recovery (n = 2), pain resulting in cessation of RFA or persisting for more than three days (n = 3), and vomiting (n = 1). The incidence of side effects was 4.5% (19/421). All major and minor complications and side effects were conservatively managed.
List of Complications and Side Effects of Radiofrequency Ablation of Benign Thyroid Nodules
Surgery during follow-up after RFA
Thyroid surgery was performed in 6% (26/421) of the patients during follow-up after initial RFA, and its details are summarized in Table 6. The median interval between the initial RFA and surgery was 7.5 years (range, 1–11). The reasons for surgery included regrowth of ablated nodules and/or persistent symptoms (n = 4) and newly detected thyroid tumors (n = 22), with these consisting of one benign and 21 malignant tumors (9 out of 21 were multiple malignancies). Total thyroidectomy and lobectomy were each performed in 13 patients.
Surgery in 26 Patients During Follow-Up After Radiofrequency Ablation and Characteristics of Newly Detected Thyroid Cancers
AUS, atypia of undetermined significance; FNA, fine needle aspiration; FVPTC, follicular variant of papillary thyroid carcinoma; MIFC, minimally invasive follicular carcinoma; PTC, papillary thyroid carcinoma; PTMC, papillary thyroid microcarcinoma; WIFC, widely invasive follicular carcinoma.
In total, 23 surgical specimens included ablated nodules. Thirteen ablated nodules were pathologically benign lesions (nodular hyperplasia or follicular adenoma), and ten were proven as thyroid cancers. All four nodules excised for regrowth or persistent symptoms were benign. Of 21 patients with newly developed thyroid cancers, six showed metastasis (lymph node metastases in five and distant metastasis in one). All six patients with metastasis had new thyroid cancers outside the ablated nodules. There were no cases of recurrence among the 21 thyroid cancer patients up to the end of the study period.
Discussion
This study evaluated long-term outcomes of RFA for benign nonfunctioning thyroid nodules. RFA achieved improvement of symptoms and cosmetic problems with a 94% VRR at ≥10-year follow-up. Its efficacy was more pronounced in nodules with an initial volume of <20 mL, with a VRR at ≥10 years of ≥98%. Our study showed two problems during follow-up, regrowth, and delayed surgery. Regrowth was observed in 12% (53/456) of nodules, and 62% (33/53) of the regrown nodules were treated with additional procedures. A large initial nodule volume (≥20 mL) compared with an initial volume of <10 mL was significantly associated with regrowth (hazard ratio, 2.315 [95% CI: 1.183–4.530]; p = 0.014). Delayed surgery was performed in 6% (26/421) of patients because of regrowth and/or persistent symptoms (n = 4) or newly detected thyroid tumors (n = 22), one benign and 21 malignant. The overall complication rate was low at 2.4% (10/421), with no procedure-related deaths or unpredictable long-term complications. Therefore, RFA is safe and effective for treating symptomatic benign nonfunctioning thyroid nodules, with a high VRR at long-term follow-up. Regular follow-up after initial success is warranted because of the possibility of regrowth of ablated nodules and the need for delayed surgery in some patients.
The safety of TA was reported in previous meta-analyses, 4,9 which showed a pooled complication rate of 4%. 4 Our study confirmed the safety of RFA with a low complication rate and no delayed unpredictable complications. A previous 10-year study on LA revealed the long-term benefits and safety of LA. 21 Compared with this previous study, 21 our study showed a higher final VRR (94% vs. 59%), consistent with the 3-year VRRs of previous meta-analyses (80–87% for RFA vs. 44–46% for LA). 4,9 The difference in VRR might be explained by the number of treatment sessions (multiple-session RFA vs. single-session LA). In addition, RFA is performed using a highly maneuverable electrode with the moving-shot technique, 4,6,18 which enables ablation of undertreated nodule margin while avoiding damage to surrounding tissue, 2 whereas LA uses delivery fibers with ablation focused on the center of the nodule. 33 The relatively low rate of cure (18%) compared with 94% final VRR is possibly because of our strict definition of cure, which required stability of a residual linear or flat hypoechoic lesion measuring <0.5 mL and with VRR ≥90%, without intranodular vascularity, and without nodule-related symptoms or cosmetic problems.
The incidence of regrowth in our study (12%, 53/456) was higher than that in the 10-year study on LA (6%, 11/171). 21 This can be explained by the fact that the previous study referred patients for surgery before regrowth occurred, as reflected by the higher number of patients who underwent delayed surgery in their study (12%, 21/171). In addition, we combined three criteria to evaluate overall regrowth. Most patients with regrowth could be managed with additional RFA (n = 33) or observed (n = 15) without further treatment.
Regarding the risk factors for regrowth after TA, previous studies reported that a large initial nodule volume, 14,34 –37 high vascularity, 34,36 nonspongiform nodule composition, 15 nodule location close to critical structures, 38 and lower energy delivered 34 were predictive of regrowth. In our study, only a ≥20 mL initial volume (compared with a <10 mL initial volume) was associated with regrowth, while nodule vascularity or content did not show significant associations. We speculate that higher nodule vascularity or solidity might be less important factors as far as vascularized, solid parts of a nodule are approachable and sufficient energy can be delivered.
Previously, delayed surgery after TA was reported only in LA studies. 14,21,23,24 In our study, delayed surgery was performed in 6% (26/421) of patients, which is less than the range of 10–35% in previous studies. 14,21,23,24 One notable difference is that all delayed surgeries in previous studies were indicated for regrowth and/or persistent symptoms, 14,21,23,24 whereas only four patients (15%) in our study underwent surgery for the same reasons. This might suggest the efficacy of RFA for preventing or treating regrowth.
We found that 5% (21/421) of patients underwent surgery for newly detected malignant tumors (10 within ablated nodules). Similarly, few cases of surgically proven malignancies in ablated nodules were reported in two previous studies. 23,24 Such occurrences might be related to false-negative results on initial FNA cytology. Although the risk of false-negative cytology results is reported to be very low after two separate FNAs, 12 our study suggests it is not negligible. Therefore, careful monitoring of changes in nodule volume or US features after RFA is required.
This study has few limitations. First, this was a retrospective study from one institution; therefore, there is a possibility of selection bias and the study might not be generalized. We tried to minimize the risk of selection bias by consecutively enrolling patients who underwent RFA; however, multicenter studies including centers across the world are needed to confirm our results. Second, a significant proportion of patients was not followed up for longer than 10 years, and there might have been unrecognized regrowth or malignancies among these censored patients. Third, management after initial RFA was not standardized, which might have contributed to lower rates of delayed surgery in our study. Finally, considering the incidence of regrowth and delayed surgery during the late period, longer follow-up studies might be required for understanding the real incidence of problems.
In conclusion, RFA is safe and effective for treating symptomatic benign nonfunctioning thyroid nodules, with a high VRR at long-term follow-up. Regular follow-up after initial success is warranted because of the possibility of regrowth of ablated nodules and the need for delayed surgery in some patients.
Footnotes
Authors’ Contributions
S.I.P.: Data curation (lead); formal analysis (lead); and writing—original draft (lead). J.H.B.: Data curation (equal); formal analysis (equal); and writing—review and editing (lead). D.H.L.: Data curation (equal). S.R.C.: Writing—review and editing (equal). D.E.S.: Writing—review and editing (equal). W.G.K.: Writing—review and editing (equal). T.Y.K.: Writing—review and editing (equal). T.Y.S.: Writing—review and editing (equal). K.-W.C.: Writing—review and editing (equal). J.H.L.: Writing—review and editing (equal).
Author Disclosure Statement
J.H.B. holds a patent for a unidirectional ablation electrode and has served as a consultant for two radiofrequency companies, STARmed and RF Medical, since 2017. The other authors have no disclosures to declare.
Funding Information
This work has received no funding.
Supplementary Material
Supplementary Data S1