
Abstract
Background:
The National Institutes of Health (NIH) is the major funding agency for biomedical research in the United States. To initiate a scholarly dialog about research and career development in the thyroid field, here we reviewed recent trends in NIH funding for this area. We used the Research Portfolio Online Reporting Tool database to estimate the level of NIH extramural support during 2013–2022 (number of active grants/year and $amount/year weighed by the total number of active grants/year and $amount/year), provided by the NIH to the thyroid field. We determined that in 2013, the NIH supported ∼140 grants/year, totaling almost $50 million/year, the majority in the form of R01 grants. Within the thyroid field, support was evenly split between thyroid cancer and thyroid hormone metabolism and action subareas. In the subsequent years (2014–2022), the total number of active grants peaked at 150/year ($55 million) in 2014 but progressively decreased to about 100 active grants/year ($30 million) in 2022. This trend occurred while the NIH budget increased from $29 to $46 billion/year. Globally, the number of thyroid-related publications increased by ∼70% during the study period, and the fractional contribution of several countries remained relatively stable, except for China which increased by ∼600%. Remarkably, the fraction of thyroid-related publications in the United States sponsored by the NIH decreased from 5.5% to 3.1% of the global number.
Conclusion:
These results constitute a very concerning scenario for research and education in the thyroid field. We appeal to the NIH, the professional societies in endocrinology and thyroidology, and all other relevant stakeholders such as thyroid-related professionals and thyroid patients to engage in further discussions to identify the root causes of this trend and implement an action plan to stabilize and eventually reverse this situation.
Introduction
There is a rich legacy of research excellence and academic training in the specialized field of the thyroid gland and its disorders in the United States. Interest in this area initially stemmed from endemic iodine deficiency and a high prevalence of goiter in the Midwest. In the early 20th century, David Marine in Ohio conducted studies on iodine prophylaxis and the prevention of endemic goiter and its consequences, while George Crille (also in Ohio) and Charles Mayo in Minnesota focused on refining surgical techniques for thyroidectomy. The Mayo Clinic established a team of surgeons, physicians, and scientists with an interest in the thyroid gland who not only isolated thyroxine and advanced our understanding of thyroid diseases but also performed approximately 21,000 thyroidectomies between 1912 and 1922. 1 Such was the interest in the thyroid gland that, in 1923, a group of surgeons of the Illinois Clinical Club met in Bloomington and established a new organization called “The American Association for the Study of Goiter,” which later became the “American Thyroid Association (ATA),” a global professional medical society with more than 1700 members from 70 countries around the world. 2,3
From its creation through the postwar era, the ATA played a pivotal role in advancing thyroid research in the United States and Canada, as recounted by Gordon Fahrni. 2 After its inaugural gathering in Illinois, the association convened annually, welcoming both national and international guests, publishing proceedings, and recognizing outstanding contributions to thyroid research. By promoting collaboration among experts from diverse areas of thyroid research, the ATA facilitated the exchange of ideas, resulting in an enhanced understanding of thyroid function, advancements in diagnostic and surgical techniques, the introduction of antithyroid medications, measurement of protein-bound iodine, and the clinical application of radioactive iodine. 2
In 1955, the clinical and scientific investigation of the thyroid gland and its disorders received a significant boost. The National Institute of Arthritis and Metabolic Diseases (the predecessor of the National Institute of Diabetes and Digestive and Kidney Diseases [NIDDK]) established the Clinical Endocrinology Branch, and a multidisciplinary group of scientists was recruited to collaborate in the study of the physiology and diseases of the thyroid gland. 4
Around the same time, the National Institutes of Health (NIH) established extramural programs to support biomedical research outside the NIH, which for decades have funded thyroid research, training, and career development. 4 Together, the intra- and extramural NIH funding mechanisms have catapulted basic and clinical research, training, and career development focused on the thyroid gland and its diseases to the high level of excellence experienced today.
The NIH extramural programs constitute a vast nationwide funding initiative, which has been the largest and most influential funding mechanism for biomedical research in the United States since its creation. 5 Scientists or groups of scientists can apply for research grants (R-series), program projects and center grants (P-series), research training and fellowships grants (F- and T-series), career development grants (K-series), and cooperative agreements for high-priority research areas that require substantial involvement from NIH program or scientific staff (U-grants). Once the applications are submitted, they are reviewed and scored by the Center for Scientific Review through one of the hundreds of Study Sections, which are groups of experts in each field of biomedical research. Subsequently, the different NIH Institutes analyze the scored applications and decide whether to fund them according to their primary mission.
To assess the latest trends of NIH support in these areas, here we used the publicly available NIH RePORTER System (https://reporter.nih.gov/) and analyzed the R-, P-, F-, T-, K-, and U-series grants awarded through the extramural program during the 2013–2022 10-year period. We specifically focused on four major thyroid-related areas of interest: (i) thyroid cancer; (ii) thyroid hormone synthesis, metabolism, and action; (iii) clinical thyroid dysfunction; and (iv) endocrine disruptors.
Methods
The present study is based on the extraction, manual curation, and analysis of data from the RePORT (Research Portfolio Online Reporting Tool) database, which was created by the NIH to increase the transparency of the decision-making process for the different funding mechanisms. Along with its repository extension, RePORTER (RePORT Expenditures and Results; https://reporter.nih.gov/) the database contains data about the research supported by the NIH.
We also searched the Estimates of Funding for Various Research, Condition, and Disease Categories (https://report.nih.gov/funding/categorical-spending#/) website, which displays the annual support level for 315 research, condition, and disease categories based on grants, contracts, and other funding mechanisms used across the NIH, as well as disease burden data published by the National Center for Health Statistics at the Centers for Disease Control & Prevention. Unfortunately, no thyroid research, thyroid condition, or thyroid disease is included in the report.
To evaluate the number of “thyroid-related” publications, we searched the PubMed database using the advanced tool. The searches looked for the word “thyroid” in all fields, specific countries in the “affiliation” field, and specific years in the “publication date”. As indicated, in some cases, the search looked for NIH (and alternative acronyms) in the “funding” field.
NIH grant funding data extraction
Data were captured by querying RePORTER using the advanced search option. The fields (i) Project Title, (ii) Project Abstract and Public Health Relevance Statement, and (iii) Project Terms were searched using the following thyroid-related keywords: Thyroid OR Hypothyroidism OR Hyperthyroidism OR Goiter OR Iodine deficiency OR Thyroid nodule OR Thyroid cancer OR Thyroid hormone OR Thyroid hormone metabolism OR Hashimoto’s disease OR Graves’ disease. Using these parameters, we specifically focused on the number of grants being funded each year (active grants/year). For example, the totality of the database (from 1985 through August 11, 2023) returned 17,366 active grants/year, which were trimmed down to 5243 active grants/year after we restricted the search to the 10 years between January 1, 2013, and December 31, 2022. The data extracted were exported to an Excel file. Only active grants with a unique application ID were considered, independently of when funding started.
NIH grant funding data curation
To analyze the 5243 active grants/year (2013–2022), we first performed an operator-curated verification that thyroid-related definitions were present in at least one of the three fields defined in the description of an NIH-awarded project: (i) the project title, (ii) the project abstract or public health relevance statement, and (iii) the project terms. As a result, we excluded 1594 active grants/year that contained a thyroid-related keyword in the project terms, but a detailed analysis of the project title revealed insufficient thyroid-specific focus (Supplementary Fig. S1A). Next, we excluded 1143 active grants/year because an analysis of the project abstract and public health statement revealed insufficient thyroid-specific focus. We also excluded 463 active grants/year because they focused on the parathyroid gland or parafollicular thyroid cells research (Supplementary Fig. S1A). Finally, we excluded 744 active grants/year with activity codes described as training (T-series), intramural (Z-series), I-series, N-series, S-series, and subprojects (P- or U-series) (Supplementary Fig. S1A). The remaining 1299 active grants/year belonged to the F-, K-, P-, U-, and R-series and were assigned into four subareas of interest: (i) thyroid dysfunction (mostly studies of hypo- and hyperthyroidism); (ii) metabolism and action (thyroid hormone synthesis, metabolism, and action); (iii) thyroid cancer; and (iv) endocrine disruptor chemicals (EDC) that affect the thyroid gland and/or its hormones (Supplementary Fig. S1A).
Funding estimates
The support provided/year by each NIH Institute was estimated for each year during 2013–2022 (Supplementary Fig. S1B). The output of our analysis was twofold: (i) the number of active grants/year (Fig. 1) and (ii) the total dollar ($) amount funded/year (Fig. 2), further segregated by type of grant and subarea of interest. The estimates were compared with the year 2013 (baseline) and weighed by the total number of grants (or total $funded) for each specific type of grant during each of the subsequent years. Some grants were not funded in the year 2013, so we used the first year of funding as a baseline instead: 2015 for R35 grants, 2016 for UG3 grants, 2017 for R61 grants, 2018 for K00 grants, 2019 for U44 grants to 2019, and 2022 for R16 grants.
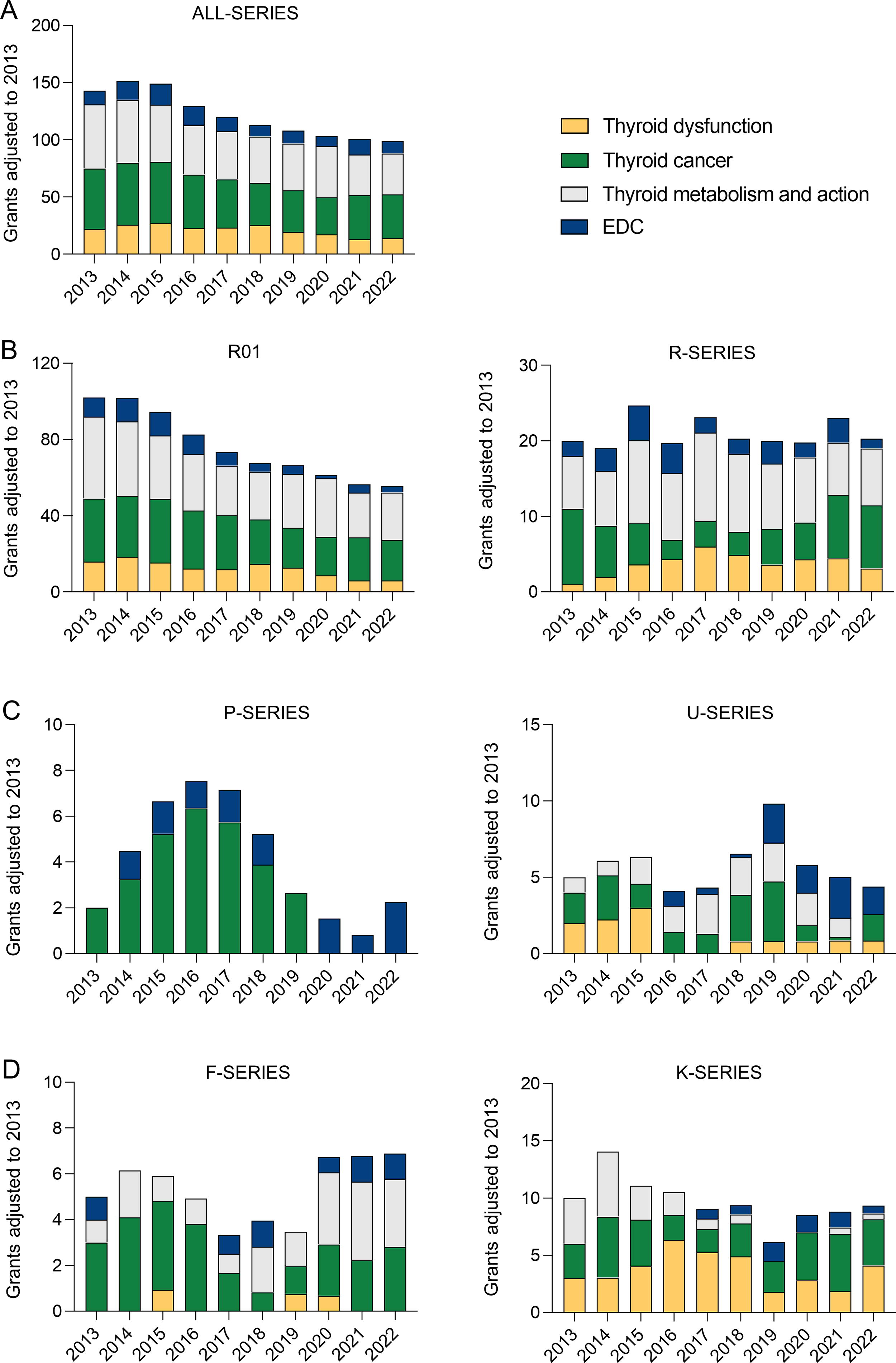
NIH active grants/year in the thyroid field.
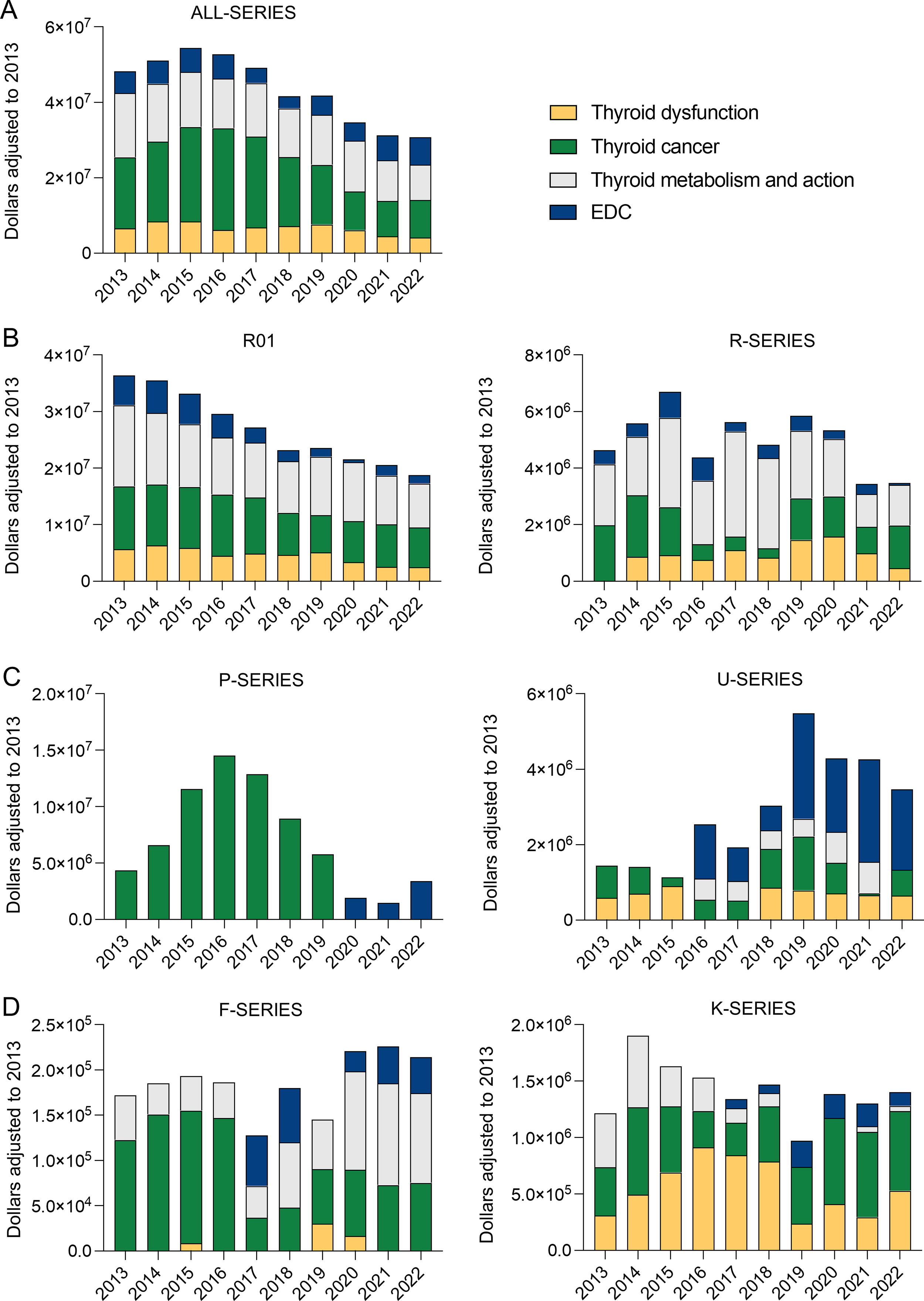
NIH funded $amount/year in the thyroid field.
Results and Discussion
In 2013, the NIH extramural program supported approximately 140 active grants/year in the thyroid field (Fig. 1A), totaling almost $50 million/year (Fig. 2A). The National Cancer Institute (NCI) picked up a large portion of the funding with almost $20 million, followed by the NIDDK with about $10 million and the National Institute of Environmental Health Sciences with about $5 million; all the other institutes combined totaled approximately $10 million (Supplementary Fig. S1B). Accordingly, in 2013, about 80% of these grants were evenly split between the thyroid cancer and thyroid hormone metabolism and action subareas, whereas the remaining 20% were split between thyroid dysfunction and EDC subareas. As expected, the bulk of the NIH support was for research in the form of R01s. Accordingly, in 2013, we identified about 100 active thyroid-focused R01s (∼$35 million) and 20 other active grants in the R-series (∼$4.2 million), which were followed by 2 in the P-series (∼$5 million) and 5 in the U-series (∼$1.8 million). There were only 10 active grants/year in the K-series (∼$1.2 million) and 5 in the F-series (∼$170,000).
In the subsequent years (2014–2022), the total number of active grants remained stable until 2016, when it dropped to about 125 per year until 2022. In relative terms (considering all other grants funded through the same period), the adjusted total number of active grants peaked at 150/year in 2014 but progressively decreased, reaching about 100 active grants/year in 2022. The absolute number of active R01s decreased progressively to about 60/year in 2022, while the relative number decreased from ∼100 to ∼50 during the same period. Although the relative contribution of each Institute in the thyroid field remained stable (Supplementary Fig. S1B), the $amounts funded followed a similar pattern, peaking in 2015 at about $55 million/year and decreasing progressively to only $30 million/year in 2022.
Notably, funding for thyroid cancer relative to the other areas expanded between 2014 and 2019 but returned to similar levels as 2013 between 2020 and 2022. This seems to have resulted from a dramatic increase in funding for thyroid cancer in the P-series during the years 2014 through 2018, which tripled in 2016. During the same period, the number of active grants/year and $/year in the U-series remained relatively stable (Figs. 1C, 2C). Particularly troublesome is the fact that the number of active support for the F-series and K-series between 2013 and 2022 remained stable at very low levels, with only about 6 active F-grants/year (∼$200 thousand/year) and 10 active K-grants/year (∼$1.5 million/year) (Figs. 1D, 2D).
The NIH funds projects to principal investigators (PIs) based both inside and outside the United States, sometimes supporting more than one project per PI and also funding projects with multiple PIs (MPI). During the 2013–2022 period, NIH-based thyroid-related grants were predominantly (∼98%) awarded to PIs in the United States (Supplementary Fig. S2A). While most PIs held only one grant at a time, ∼14% of PIs held up to five grants simultaneously (Supplementary Fig. S2B). Notably, the decline in the number of grants during 2013–2022 affected PIs holding one grant as well as multiple grants (Supplementary Fig. S2C). About 21% of the grants involved more than one PI (MPI) (Supplementary Fig. S2D), and this proportion increased from ∼13% to ∼21% over the 2013–2022 period, indicating that the reduction in funding predominantly impacted grants with only one PI (Supplementary Fig. S2E-F).
To estimate the impact of reduced funding on the thyroid field, we searched for the thyroid-related publications listed in PubMed (Table 1). Globally, the number of thyroid-related publications increased approximately 1.7-fold between 2013 and 2022 (Table 1). During the same period, the growth of the USA-based thyroid-related publications was similar to the global estimates, so that the USA contribution remained stable between 12% and 15% (Table 1). A similar trend was observed with France-based publications (stable between 2.9% and 3.6%), whereas in Brazil, Germany, and Japan, there was a notable growth during about 5 years that subsided by the year 2022 (Table 1). Remarkably, the global contribution of the thyroid-related publications funded by the NIH progressively declined from 5.5% to 3.1% during the 2013–2022 period (Table 1).
Number of Thyroid-Related Publications and Global Contribution per Country per Year
Numbers were obtained from PubMed using the advanced search tool. The name of the country was identified under “affiliation.” NIH indicates a publication that acknowledged the NIH under “funding.” % was calculated for each country based on the “world” numbers for each year.
NIH, National Institutes of Health.
Overall, we believe that the present results reveal a very concerning trend in NIH support in the thyroid field, with the absolute and relative level of funding for career development, research, and publications dropping by almost half in the past 10 years. The fact that these numbers were weighed for the total number of grants/year and funding/year for each grant series indicates that research in the thyroid field is shrinking in this country. Notably, the NIH budget has increased from $29.3 to $46.2 billion/year during the same 2013–2022 period. 6 The negative impact on the thyroid field is obvious. Whereas, globally, the fractional contribution of USA-based thyroid-related publications has remained stable in comparison with countries in Asia, Europe, and South America, the contribution of NIH-funded publications has shrunk by almost half (Table 1). The trend of declining funding is most unfortunate and is in contrast with the strong support for thyroid studies provided by the NIH since the 1950s. Given the very limited support for the F- and K-grants, there is a real possibility that the current trend is driving a trajectory that could be hard to reverse. F- and K-grants are the key mechanisms that support the career development of new scientists and clinician- and physician-scientists with an interest in academic medicine.
It is difficult to get to the root cause of this trend. Among multiple possibilities, we could be experiencing a general decrease (i) in interest in pursuing a career in thyroid research and/or (ii) in the quality of the current grant applications and/or (iii) in NIH interest in funding thyroid research. Knowing the annual number of thyroid-related proposals submitted to the NIH and their success rate would be key to elucidating this. Nonetheless, after reaching out to the NIH Endocrine and Metabolic Systems Review Branch and the Office of Extramural Research, we learned that as per NIH data access policy, 7 this information is not made public. However, the fact that the number of thyroid-related publications in the United States has grown by about 50% (albeit less than Germany and China) contrasts sharply with the shrinkage in the NIH-funded publications (about 50%) during the same time, suggesting that there is still interest in pursuing a career in thyroid research and that investigators might be seeking funding elsewhere.
For the past 100 years, the ATA has provided leadership for the thyroid field in North America. We hope that the ATA will continue its historical support for research and career development and see the present study as an opportunity to assess the problem and take action. They could partner with the NIH and with other professional societies such as the Endocrine Society and initiate a thorough analysis of the situation so that a plan to reverse this trend can be put in place. The data housed at the NIH containing the number of applications as well as the demographics of the investigators are critical for a better understanding of the problem. Objectively, is there a decline in the number of thyroid-related applications? Are thyroid-related submissions being evaluated by thyroid experts? What has the success rate been for thyroid-related submissions when compared with other fields? Have any changes in PI demographics, or sex, racial, and ethnic inequities, occurred that correlate with and could explain the present scenario? While we understand the restrictions imposed by the NIH data-access policies in place, one would hope that the ATA leadership could find an interlocutor within the NIH leadership who is sensitive to the problem and obtain access to the information. If this fails, the ATA would be within its right to use the Freedom of Information Act to get access to the data.
Action is imperative because tens of millions of individuals in the United States continue to be affected by thyroid diseases. These conditions vary from genetic abnormalities resulting in neonatal hypothyroidism or deficiencies in thyroid hormone action and transport to autoimmune diseases causing hypo- or hyperthyroidism and various forms of thyroid cancer. Ultimately, it is the mission of the NIH to “seek fundamental knowledge about the nature and behavior of living systems and the application of that knowledge to enhance health, lengthen life, and reduce illness and disability,” or, in simpler terms, to enhance the nation’s health. Importantly, the widespread awareness among patients and the public regarding the insufficient funds allocated to thyroid research and education underscores the urgency for action. There are at least two active public petitions (one is U.S. based and was initiated by a patient, 8 and the other is based in the United Kingdom and was initiated by a clinician-scientist 9 ) with almost 20,000 signatures, asking for more funds for thyroid research and education.
What are the possible actions that could be taken to reverse this scenario? While that might ultimately depend on the root cause of the problem, one could envision the Advisory Council to the NIDDK, NCI, or other NIH Institutes recommending the creation of specific Program Announcements, Request for Applications, or direct solicitations focused on research and career development with earmarked funding for the thyroid field. These are a standard mechanism used by NIH Institutes to stimulate research in areas deemed of high importance by their Advisory Council. Of note, strongly focused funding has led to highly successful research programs in other countries. For example, the German Collaborative Research Consortium “Local Control of Thyroid Hormone Action” (CRC/Transregio 296, LOCOTACT; https://locotact.de/), which provides thyroid-specific funding to numerous centers, has resulted in prolific and very innovative research.
The present analysis is not without limitations. Assigning the grants to each of the four subareas was done manually and according to subjective criteria followed by the two authors. Nonetheless, the figures obtained match the level of funding calculated for each NIH institute. In addition, we excluded several types of grants from our analyses, that is, T-series, Z-series, I-series, N-series, and S-series, either because they were not typical extramural support or because of the difficulty in assigning their level of thyroid-specific focus. Also, we did not have access to NIH data that were not publicly available, such as the number of funding applications received.
In conclusion, the level of NIH funding for thyroid research has decreased markedly in the past 10 years, while the NIH budget has increased ∼60%, and millions of individuals in the United States continue to suffer from thyroid diseases. The interested stakeholders in this dialog, that is, thyroidologists, thyroid researchers, thyroid patients, along with the leadership of professional societies, should engage the NIH to determine the root cause of this trend and develop an action plan to reverse this concerning scenario.
Footnotes
Acknowledgment
All of the research was performed with publicly available data and meets the ethics guidelines.
Authors’ Contributions
J.H.-A. performed the database searches, retrieved, curated, and analyzed the results and prepared the article. A.C.B. conceived and directed the studies, curated the results, and prepared the article.
Author Disclosure Statement
A.C.B. is the past president of the ATA. He served as a regular member of the Molecular and Cellular Endocrinology NIH Study Section (2005–2009) and as a regular member of the Board of Scientific Counselors of the NIDDK (2011–2016) and is currently a regular member of the Cell Signaling and Molecular Endocrinology NIH study section (2021–2025). He is the recipient of grants from the NIDDK (DK58538, DK65055, DK77148, DK15070) and is a consultant for Abbvie, Allergan, and Synthonics. J.H.-A. has no relevant disclosures. The views expressed here reflect those of the authors.
Funding Information
No specific funding was used in the preparation of this article.
Supplementary Material
Supplemental Material Figure S1
Supplemental Material Figure S2