
Abstract
Background:
Differentiated thyroid carcinoma (DTC) in children is uncommon; clinical presentation over recent decades is incompletely characterized.
Methods:
This retrospective cohort study analyzed demographic and disease characteristics of consecutive juveniles with DTC treated from 1970 to 2015 at Poland’s largest pediatric DTC referral center, Maria Sklodowska-Curie National Research Institute of Oncology, Gliwice, who had available records. Sex, age, histopathological characteristics, and DTC stage were documented. We aimed to identify changes in these variables over time and independent risk factors for lymph node or distant metastases. Trends in these variables were assessed using the Cochran–Armitage test and Spearman correlation. Multivariable logistic regression was performed to identify risk factors associated with lymph node or distant metastases.
Results:
475 of 479 patients (99.2%) were included in the analysis; roughly half were age ≥15 years, 10%, <10 years. Papillary thyroid carcinoma (PTC) represented 88% of cases and follicular thyroid carcinoma (FTC) 11%. Tumors ≤2 cm constituted 56% of cases with relevant data; those >4 cm accounted for 12%. Multifocality was observed in 37% and extrathyroidal invasion in 22%. Lymph node metastases were noted in 59% and distant metastases in 16%. Over the observation period, significant trends among new cases included: increased proportion of adolescents >15 years; increased frequency of tumors ≤2 cm, decreased multifocality rates, and increased proportion of PTC versus FTC. Extrathyroidal invasion rates remained appreciable throughout, ranging from 17 to 28% during the 5-year study subperiods after 1990. Lymph node metastases significantly increased in frequency in the central neck, remaining consistently common in lateral sites; presence of distant metastases significantly decreased. In multivariable analysis, multifocality, extrathyroidal invasion, and tumor size were independently associated with lateral lymph node metastases and multifocality, larger tumor size, and N1b metastases with distant spread.
Conclusions:
Our observations of a rising proportion of diagnoses in adolescence, reductions in primary tumor size, and decreased frequency of multifocality and distant metastases may reflect increased detection of patients with less aggressive DTC at earlier disease stages. Nonetheless, we found persistently substantial rates of locoregionally advanced disease features (multifocality, extrathyroidal invasion, and lymph node metastases), which multivariable analyses suggested have significant associations with lateral lymph node and/or distant metastases.
Introduction
In recent decades, differentiated thyroid cancer (DTC) incidence has steadily increased in adults. Studies have shown this rise mainly to have been driven by small, clinically-silent papillary carcinomas, which have an excellent prognosis. 1 –4 This important observation has led to a de-escalation in intensity of routine diagnostic and therapeutic approaches in this setting. 5,6
Due to the low incidence of DTC in children, published data on the disease’s clinical presentation in this setting so far have usually been based on analyses of small groups 35 , while reports from cancer registries often lack complete clinical information regarding pediatric patients. 7 –17 Additional, long-term data on the clinical presentation of DTC in larger cohorts of children could serve as important evidence to help improve management of pediatric DTC.
Since 1970, several hundred children with DTC have been treated in our tertiary referral center. The large cohort as well as the long observation period furnish a unique opportunity to study the clinical presentation of pediatric DTC and trends in patients’ demographic and disease characteristics over recent decades. The large sample and protracted follow-up also allow robust analysis of risk factors for lymph node and distant metastases in this setting. We now report our analysis addressing these points.
Materials and Methods
Study design, patients, setting, and ethics
This retrospective cohort study analyzed demographic and disease characteristics around the time of presentation and the relationship of such variables with lymph node or distant metastases, in patients with DTC diagnosed at age ≤18 years. The patients were operated on from 1970 to 2015, and in the vast majority of cases, subsequently given radioiodine therapy in the Maria Sklodowska-Curie National Research Institute of Oncology, Gliwice Branch in Gliwice, Poland (MSC). Data for the analysis were obtained via medical record review by six co-authors (A.K., A.L., E.P.C., T.O., A.B., and D.H.J.), then cross-checked by A.K. (first author). After initial treatment, patients were followed at our center every 3–12 months.
For approximately the first four decades of the study period, MSC was Poland’s only major tertiary referral center for pediatric DTC; afterward, a few research and university hospitals began to also serve in this capacity. Therefore, our center’s catchment area covered all of Poland, especially the southern and western regions. The study cohort did not include any patients from outside Poland, e.g., Ukraine or Belarus.
Demographic and disease characteristics, as well as their relationship with lymph node or distant metastases, were determined for the cohort as a whole. In addition, patients were stratified based on the date of the first thyroid surgery, and the subgroups’ demographic and disease characteristics around that time were analyzed and compared to determine clinical presentation trends. For this latter analysis, six periods were used, the first encompassing 1970–1990, the next five encompassing succeeding half decades through 2015. The longer initial period was intended to provide a subgroup more comparable in size to the subgroups from the later five periods, when more patients presented at our center.
Due to numerous changes in the TNM classification system over the long study period, only measurable tumor characteristics were used to assess the cancer stage. Since older histopathological reports did not distinguish between minimal versus extensive extra-thyroidal infiltration, we only evaluated the presence/absence of such invasion, rather than its extent. Vascular invasion was not included in the analysis due to minimal documentation regarding this variable. Lymph node metastases were assessed as present (N1) if neck lesions manifested within 12 months after initial surgery, regardless of whether such lesions were found on initial examination (via palpation or ultrasound), after the initial surgery, or after re-operation. If a patient had no lymph nodes removed, or the status of resected nodes was not indicated in the record, and nodal metastases were not found during clinical follow-up, the patient was classified as having no lymph node metastases (N0). According to the TNM definition, patients were defined as having N1a disease if they had mid-neck nodal metastases and as having N1b disease if they had lateral neck nodal metastases. Patients were classified as having M1 disease regardless of the time that distant metastases were identified, i.e., the M1 subgroup included three cases of lung metastases that were first documented >12 months post-surgery.
The study was approved by the MSC Ethics Committee in 2006 (DO/DOP/493–11/06), and approval was obtained for the retrospective data analysis alongside the prospective evaluation of complications in children treated for thyroid cancer. Due to its retrospective, strictly observational nature and the de-identification of the data to be reported, the requirement for patient or parent/guardian informed consent was waived by the Ethics Committee.
Statistics
Descriptive statistics (mean ± standard deviation (SD), median [minimum—maximum], number [percent], as applicable) for the overall cohort and the subgroups treated during the different periods included all patients in the cohort or subgroup, respectively.
Categorical variables were summarized in contingency tables. The independence of proportions was assessed by Fisher’s exact test. The existence of monotonic trends was assessed with the Mann–Kendall test for the whole cohort and with the Cochran–Armitage test for category proportions; for multilevel variables, one-versus-rest comparisons were performed. The trend magnitude was calculated using Spearman’s rank correlation rho. The sign (i.e., plus or minus) of the rho correlation coefficient indicates the trend direction, and based on the values of that coefficient, the strength of association can be interpreted as >0.3—low, >0.5—moderate, >0.7—high, and >0.9—very high. Due to a >30% rate of unavailable data regarding extrathyroidal invasion and multifocality in patients presenting from 1970 to 1990, this subgroup was excluded from the statistical analysis of trends in these tumor characteristics. Analyses of trends and associations of tumor size and other disease characteristics included all patients with available data for the variable of interest.
Univariate analysis and multivariable logistic regression analysis were performed regarding potential risk factors associated with lymph node or distant metastases. These factors included demographic and disease variables compiled in the study. In these analyses, only cases with available data regarding all analyzed factors were considered. For categorical variables, the lowest-value category or “no” was set as the reference. For each endpoint, three approaches are presented: univariate analysis for each variable, multivariable analysis using a full model containing all variables, and multivariable analysis using a “reduced model” obtained based on stepwise elimination of certain variables using the Akaike information criterion. For the multivariable analyses, odds ratios (OR) and their 95% confidence intervals (CI) are presented. The area under the receiver operating characteristic (ROC) curve (AUC) was used to assess goodness of fit of the models.
Analyses were performed using R environment for statistical computing version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria, http://www.r-project.org). Two-sided p values ≤0.05 were considered to be statistically significant.
Results
Overall cohort characteristics
The analysis involved 475 consecutive juveniles with available medical records; median [minimum—maximum] follow-up time was 11 [0.1–47.8] years. The group comprised 99.2% of pediatric DTC patients treated at MSC during the study period (Fig. 1). Tables 1 and 2, respectively, present the cohort’s demographic and disease characteristics. Among the 475 children, the girl:boy ratio was approximately 2.7 (346:129). Just over half of patients (240/475) were ≥15 years old at diagnosis, and 10% (47/475) were <10 years of age. Papillary thyroid carcinoma (PTC) was diagnosed in 88% (416/475), follicular thyroid carcinoma (FTC) in 11% (54/475). Primary tumor size was determined in 70% of children (333/475); cases without available data regarding this variable were mostly diagnosed from 1970 to 2000. Of tumors with known diameter, around 56% (187/333) measured ≤2 cm and a bit over 12% (41/333), >4 cm. Multifocality was found in some 37% of patients with available data regarding this disease feature (163/443), in almost half of cases, in both lobes. Extrathyroidal invasion was noted in approximately 22% (93/427) of patients with available data on this variable.
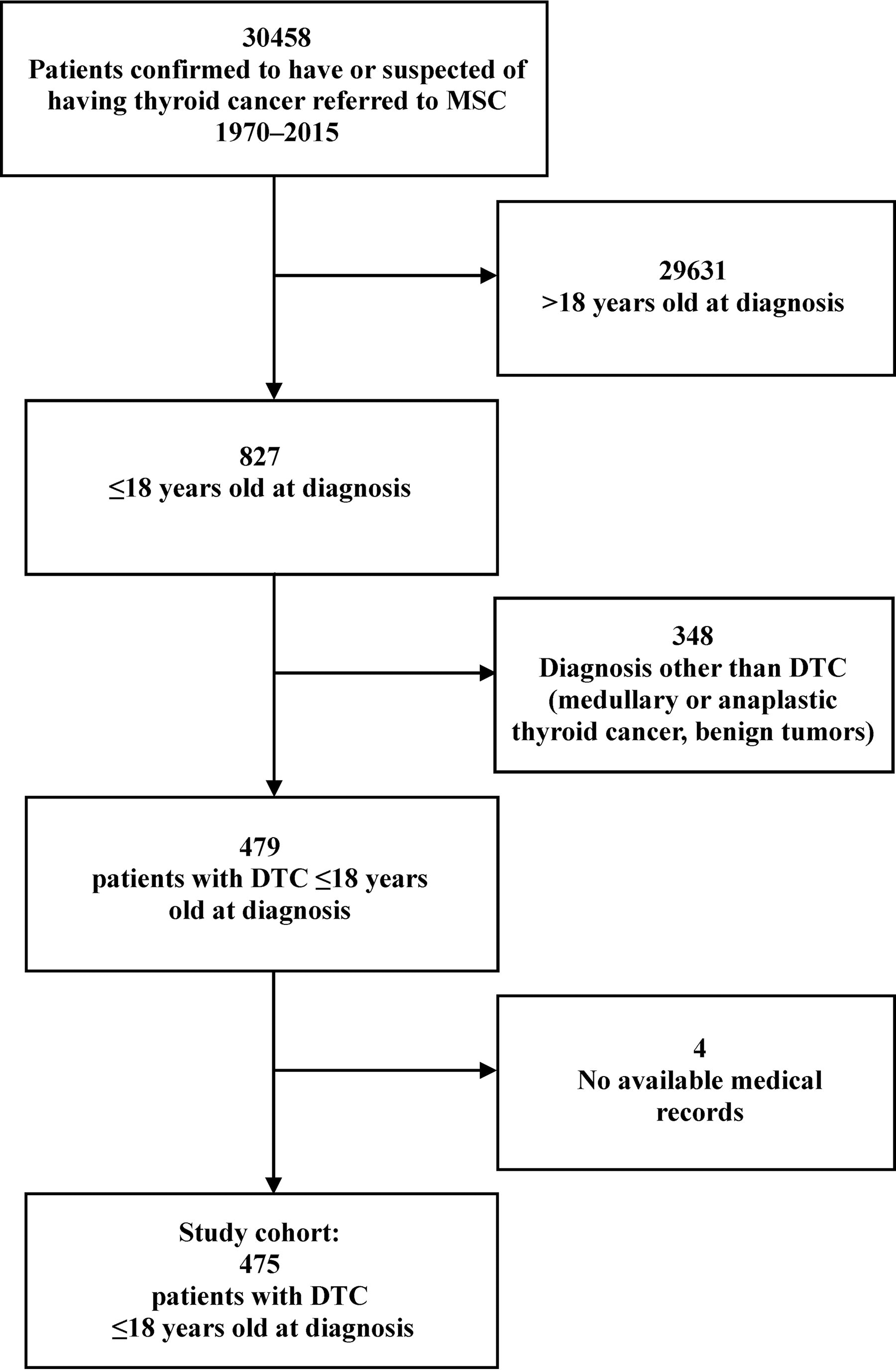
Participant flow diagram.
Characteristics of the Overall Cohort (n = 475)
DTC, differentiated thyroid cancer.
Histopathology and Metastatic Involvement (n = 475)
*FTC, follicular thyroid carcinoma; PTC, papillary thyroid carcinoma; PTC-FV, follicular variant of papillary thyroid carcinoma.
Micrometastases were defined as lesions detectable by iodine-131 scintigraphy, but not radiography.
Lymph node metastases were noted in about 59% of patients, in lateral neck compartments in approximately 45% of cases. Distant metastases were found in 16%. Disseminated disease was preponderantly seen in the lungs (92%); nearly half of pulmonary lesions were micrometastases, i.e., diagnosed scintigraphically, and not visible radiologically.
Trends in clinical presentation
Table 3 presents changes over time in demographic and clinical characteristics of children with DTC treated at our center over the 45-year study period. The number of pediatric DTC cases presenting annually significantly increased over that time (p < 0.001). In the 1970s–1980s, only individual patients presented. The peak number of children was referred to our center in 1995–1997. Subsequently, numbers of new cases fluctuated between 11 and 22 per year, approaching 30/year in 2015 (annual data shown in Fig. 2).
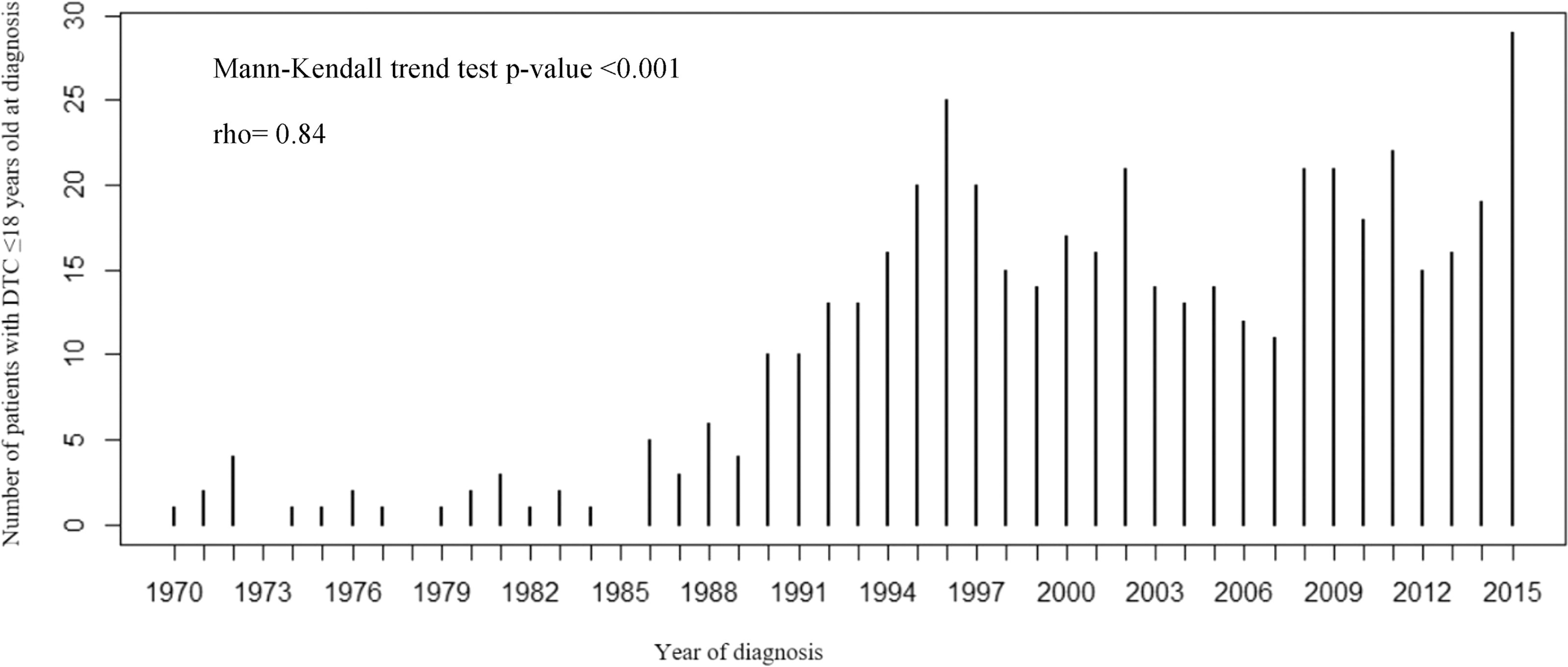
Number of children with DTC treated at MSC in consecutive years.
Changes in Demographic and Disease Characteristics over Time
*“Considered subgroup” denotes patients with available complete data regarding the given variable.
**Percentages refer to a number of patients by year of diagnosis.
***Due to an >30% rate of unavailable data regarding this variable among patients diagnosed from 1970–1990, children diagnosed during this period were excluded from the trend analysis.
p values denote statistical significance at p ≤0.05.
↑, increase; ↔, no change; ↓, decrease; FTC, follicular thyroid carcinoma; PTC-FV, papillary thyroid carcinoma-follicular variant.
Fisher’s exact test.
Cochran–Armitage test or Mann–Kendall test.
Spearman’s rank correlation coefficient.
The girl:boy ratio did not change significantly over time (p = 0.56), although a slight upward trend in the proportion of girls has been noted, coinciding with the pattern in Polish National Cancer Registry data. 25 The proportion of adolescents (≥15 years of age) significantly increased over the study period, while that of the much smaller group of the youngest patients (<10 years of age) remained stable.
The proportion of cases with FTC declined 10-fold over time, from 20% in 1970–90 to 2% in 2011–15 (p < 0.001), with a commensurate increase in the proportion of PTC cases.
The percentage of patients with the largest tumors, those >4 cm, was stable over the study period, never reaching 11% in any time interval. Simultaneously, the proportion of the smallest tumors, those ≤1 cm or from 1 to 2 cm, significantly increased (p < 0.001 and p = 0.005, respectively). It is notable that our first case of a unifocal DTC <1 cm was only registered in 1995, albeit such lesions cannot be ruled out in the approximately 30% of patients treated from 1970 to 1990 with undocumented tumor size.
There was a decreasing trend in multifocality over time, with the highest statistical significance in this trend for tumors ≤1.0 cm (p < 0.001), and borderline significance for tumors >1–2 cm (p = 0.055). The proportion of cases with extrathyroidal invasion was stable over the study period.
The proportion of cases with lymph node metastases slightly increased over time. However, the upward trend was only significant regarding mid-neck nodes (N1a), while the frequency of lateral node metastases (N1b) decreased, albeit nonsignificantly, since 2000.
The frequency of distant metastases decreased significantly over time (p = 0.003).
Primary tumor size and relationship of other potential risk factors with lymph node or distant metastases
As seen in Table 4, which presents disease characteristics according to primary tumor size, extrathyroidal invasion, any N1b disease, bilateral N1b disease, and distant metastases each became significantly more frequent as the primary tumor size category reflected increasing diameter. Therefore, the frequency of isolated nodal metastases to the central compartment decreased in larger tumors. Multifocality occurred in a substantial proportion of patients regardless of the primary tumor size category, and although such involvement was likelier for tumors >4.0 cm, multifocality was not significantly associated with tumor diameter category. Notably, the rate of extrathyroidal invasion reached approximately 45% in lesions cm, but invasion was seen even in tumors ≤1.0 cm (around 8% of cases). The smallest tumors (those ≤1 cm) were likeliest to metastasize exclusively to the central neck nodes, while the largest tumors (>4.0 cm) were much likelier to also metastasize to lateral nodes than to central lymph nodes only: the rates of N1a and N1b disease were, respectively, 26.0% and 22.7% in the former, versus 5.0% and 59.0% in the largest primary tumor size category.
Disease Characteristics According to Primary Tumor Size
Considered subgroup denotes patients with available complete data on the evaluated variables. Percentages refer to a number of patients belonging to a category within specified primary tumor size.
p values in bold type denote statistical significance at p ≤0.05.
↑, increase; ↔, no change; ↓, decrease.
aFisher’s exact test.
bCochran–Armitage test or Mann–Kendall test.
cSpearman’s rank correlation coefficient.
Tables 5 and 6 display the results of univariate and multivariable analyses of the relationship of primary tumor size and other potential risk factors with N1a metastases or N1b metastases or with distant metastases, respectively. Follow-up regarding lymph node metastases (at diagnosis) were 12 months; the median (minimum—maximum) follow-up time regarding distant metastases was 11 (0.1–47.8) years.
Potential Risk Factors Associated with Neck Lymph Nodes Metastasis
Percentages refer to proportions of patients by metastasis status within a given category.
p values denote statistical significance at p ≤0.05.
The analysis included only patients with available data for all analyzed factors (315/475, 66.3%).
The full model contained all variables, whereas the reduced model contained variables after stepwise elimination based on the Akaike information criterion. CI, confidence interval; OR, odds ratio; ref., reference.
Median [minimum—maximum].
OR refers to a year of increasing age.
Potential Risk Factors Associated with Distant Metastasis
The analysis included only patients with available data for all analyzed factors (311/475, 65.5%). Percentages refer to proportions of patients in a given category.
p values denote statistical significance at p ≤0.05.
The full model contained all variables, whereas the reduced model contained variables after stepwise elimination based on the Akaike Information Criterion.
Median [minimum—maximum].
OR refers to a year of increasing age.
CI, confidence interval; OR, odds ratio; ref., reference.
Altogether, the analyses regarding lymph node metastases included 315/475 patients, 66.3% with N1a or N1b or N0 disease and available data on all analyzed factors. In the final, reduced multivariable model involving only N1a and N0 patients (n = 187/475, 39.4%), no studied variable appeared to have a significant association with central lymph node metastases (goodness-of-fit AUC 0.586, with very low predictive ability AUC 0.15; Supplementary Fig. S1A).
In the reduced multivariable model regarding risk for N1b versus N0 status (n = 253/475, 53.3%), extrathyroidal invasion and multifocality along with increasing tumor sizes were the independent risk factors for lateral lymph node metastases. This model showed good fit (goodness of fit AUC 0.757, predictive ability AUC 0.7; Supplementary Fig. S1B).
The analogous analysis regarding distant metastases, also involved only patients with available data on all analyzed factors (n = 311/475, 65.5%). In the reduced multivariable model, multifocality and increasing primary tumor diameter along with presence of lateral, i.e., N1b neck lymph node metastases also were independent risk factors, but extrathyroidal invasion was not. Probably due to the low number of tumors in the 3.1–4.0 cm range, multivariable analysis showed no significance in this particular group (p = 0.08). Nonsignificant risk factors remaining in the reduced model were younger age at diagnosis and presence of central, i.e., N1a neck lymph node spread. Goodness of fit was very high, with AUC 0.898 and predictive ability AUC 0.844 (Supplementary Fig. S2).
Discussion
To our knowledge, this analysis involved one of the largest pediatric DTC cohorts and longest study periods yet reported. The analysis had four major findings.
First, we observed an increased number of cases and an apparent diminution of severity in clinical presentation over time, including a rising proportion of diagnoses in adolescence, reductions in primary tumor size, and in the frequency of multifocality and distant metastases.
The notable increase in cases starting in the mid–late 1990s may in part have been attributable to the publication of the first Polish treatment guidelines for thyroid cancer in 1995, 22 heightening awareness of the diagnosis and referrals to a specialist center. A relationship with the radiation exposure related to the Chernobyl disaster is in our opinion unlikely, as our cohort included no Russian, Belarussian, or Ukrainian children. In addition, in Poland, iodine prophylaxis was implemented shortly after the accident, largely mitigating resultant radiation exposure, which was appreciably lower than in, e.g., Ukraine or Belarus. 23,24
Our observations of an increased number of cases and an apparent diminution in their severity at presentation over time may reflect increased detection in patients with less aggressive DTC, and at earlier disease stages, in our sample in recent years. This finding is consistent with patterns observed in adults. It is still debated whether the increased incidence of DTC in the latter is exclusively due to overdiagnosis resulting from more frequent screening and improved imaging, or whether changes in environmental risk factors also play a role. 2,26,27 The widespread strong correlation between DTC incidence in adults and in children suggests that overdiagnosis is, even if not the only cause, an important driver of the growing numbers of pediatric DTC cases. 2,8 For example, the United States has seen a sharply increased DTC incidence among children of 9%–11% per year since 2006, a trend including not just cancers confined to the thyroid, but locoregionally advanced and disseminated cases. 10,11,18 In Japan, a screening study of children after the 2011 Fukushima nuclear power plant accident found an increase in small papillary carcinomas—in half of cases, <10 mm. Based on patients’ ages at the time of the accident and the latency period since that event, as well as the tumors’ molecular profile, the Japanese investigators concluded that the high number of cases was due not to radiation exposure, but only to increased detection of clinically silent PTCs. 28,29 Diagnosis of such tumors might rise in future, if prophylactic thyroid ultrasonography becomes more frequent, a development that the present authors unequivocally advise against.
However, the greater abundance of pediatric DTC cases observed in high-income countries may partly be due to changes in diet and lifestyle. Among the latter may be more widespread air travel, since, for example, flights between Europe and the United States are associated with 30–70 µSv of ionizing radiation exposure, some 25%–50% of the dose provided by a chest X-ray. Another important factor may be greater use of computed tomography, since exposure to even low doses of ionizing radiation during childhood medical procedures is associated with increased risk of thyroid cancer. 30 Over the past 30 years, a number of qualitative changes have occurred in Poland: household incomes have doubled, and standards of living, health care, and related medical procedures have much more closely approached those of Western Europe and the United States. This situation may help explain the apparent gradual increase in the same period in the number of new DTC cases in children at our center.
A second and unexpected, major finding of this analysis was the continuing elevated prevalence of lymph node metastases in our patients. Such disease occurred in almost 60% of the cohort, with an upward trend over time for central neck nodes metastases. This number is much higher than in adults, where it is around 30%. 16,31 Our observation may be related to an increased rate of small PTC lesions, the size category that has the highest risk of isolated metastases to the central lymph node compartment. It is also possible that we are facing a higher detection rate, perhaps due to the standardization of surgical procedures and the considerable detail in modern histopathology reports. 10 Notably, the prevalence of N1b tumors remained high, and statistically unchanged, in our patients throughout the study period: such lesions affected roughly one-third to one-half of patients, depending on the subperiod. However, the number of larger tumors, that is, tumors with the highest risk for lateral metastases (Table 5) also remained stable, a finding that could explain the consistent frequency of N1b disease. Together, these observations suggest that the natural course of thyroid cancer in children is aggressive, but earlier detection of smaller lesions reduces the risk of metastases to more distal nodal sites (i.e., lateral ones) at presentation. Also of interest, in our multivariable analysis, only lateral nodal lesions, but not central nodal metastases, were significantly independently associated with distant metastasis. These data support the concept, proposed in the 2015 American Thyroid Association pediatric DTC management guidelines 32 and suggested by other retrospective analyses, 19,33 that sparse metastases in the middle cervical lymph nodes are not a negative prognostic factor in children with DTC.
A third main finding of our analysis was that features of locally advanced disease remained common among our patients. Multifocality declined in frequency over time, but even in the most recent subperiod, 2011–2015, >13% of children with primary tumors ≤1cm, and almost 22% of those with primary tumors >1–2 cm manifested multiple thyroid lesions. In addition, the rate of extrathyroidal invasion among our patients was statistically unchanged, and consistently appreciable, throughout the study period, ranging from approximately 17%–28% depending on the sub-period. This observation is in line with several studies suggesting that perithyroidal infiltration by DTC is significantly more common in children versus adults, e.g., the respective rates were 24% versus 15% in the Mayo Clinic from 1946 to 1977 and 53% versus 38% in Saudi Arabia from 1998–2011. 16,34 Notably, our multivariable analyses showed multifocality to be an independent significant risk factor for both lateral lymph node and distant metastases and extrathyroidal invasion to be one for N1b status. In addition, multifocality has been found by others to be a risk factor for persistent or recurrent disease, 19,20,40 while extensive extrathyroidal invasion is a recognized high-risk factor for relapse and cause-specific mortality, albeit conflicting results have been obtained for minimal/microscopic infiltration. 19,33
Our multivariable analysis also demonstrated that lateral lymph node metastases are an independent risk factor for distant metastases. Over time, we observed a significant decrease in the risk of distant metastases, which aligns with a decrease, though not a statistically significant one, in the frequency of lateral lymph node metastases. It should be emphasized that the period with the highest frequency of distant metastases also had the highest frequency of lateral lymph node metastases.
Our last main observation was that the frequency of FTC decreased and that of PTC increased dramatically over time. Poland was iodine deficient throughout much of the 20th century, a status that only lately has changed. As is well known, iodine deficiency is associated with higher incidence of FTC. 37,38 This correlation likely explains the decreased frequency of FTC over time in our sample. It may also be relevant, however, that in the past, the follicular subtype of PTC was not infrequently diagnosed as FTC. 39 Indeed, a converse situation in which FTC is diagnosed as the follicular variant of PTC could explain our low recent rate of FTC relative to that reported in other pediatric DTC cohorts.
We close by acknowledging that although this analysis had the strengths of a large sample size, inclusion of >99% of potential subjects, and long follow-up duration, the work also had certain limitations. The analysis was constrained by its retrospective nature and study period beginning more than five decades ago. For example, changing surgical practices over time, e.g., greater use of prophylactic central neck dissection since 2000, might help explain the increase in frequency of N1a disease. In addition, clinical and documentation processes during the initial years of the study period were associated with some unavailability of detailed histopathological information. Thus, our multivariable analyses of potential risk factors for lymph node or distant metastases excluded approximately one-third of patients because these children lacked available data regarding all covariates. As well, heterogeneity in archival material precluded us from distinguishing extensive from minimal extrathyroidal invasion, while very limited record-keeping regarding vascular invasion precluded our analyzing that variable. However, limitations of this nature also affect registry data, from which a big part of accepted knowledge regarding pediatric DTC derives. 9 , 11 , 12 , 18 , 21 , 36 , 41
A further limitation, potentially hampering the generalizability of our results, was the single-center nature of this analysis, although the nationwide catchment area of our institution may partly mitigate this issue. Further, the single-center nature of our study likely also provides a strength: consistency of data collection compared with that of comparably sized registry cohorts. For example, all data entry was double-checked to limit error.
Further, some caution should be exercised in interpreting our multivariable analyses of risk factors for metastases. The results of these analyses may contain some bias, e.g., the limited numbers of tumors >3–4 cm in diameter may have prevented detection of a statistical association of such lesions with distant metastases, as was seen with tumors 2–3 cm or >4 cm in diameter. Lastly, our results may have suffered from selection bias related to our institution’s specialization attracting complicated cases.
Conclusions
In one of the largest pediatric DTC series and longest study periods yet published, we observed notable changes in the clinical manifestation of pediatric DTC in recent decades. These changes included increases in the proportion of adolescent cases and significant reductions in primary tumor size, the frequency of multifocality and distant metastases, and the frequency of FTC. These findings are consistent with global trends reported in population-based studies and single-center studies in pediatric as well as adult patients with DTC. Nonetheless, our study also was noteworthy for finding persistently high rates of locoregionally advanced disease features, namely multifocality, extrathyroidal invasion, and lymph node metastases. Our multivariable analyses suggested that these features may have significant independent associations with lateral lymph node or distant metastases, or both.
Footnotes
Acknowledgment
Robert J. Marlowe, Spencer-Fontayne Corporation, Jersey City, NJ, USA, edited this article.
Authors’ Contributions
A.K.: investigation, data curation, data cross-checking, formal analysis, and writing—original draft. A.L.: resources and data curation. E.P.C.: resources and data curation. T.O.: resources and data curation. A.B.: resources and data curation. M.K.: methodology, formal analysis, visualization, and writing—review and editing. A.W.: methodology, formal analysis, visualization, and writing—review and editing. A.C.: methodology and supervision. A.Cz.: resources. B.J.: supervision; D.H.J.: conceptualization, data curation, supervision, and writing—review and editing.
Authors’ Disclosure Statement
A.K.: Travel grants and lecture fees from Genzyme Sanofi. A.L.: Travel grants and lecture fees from Genzyme Sanofi and Polatom. E.P.C.: Travel grants from Berlin Chemie. D.H.J.: Travel grants and lecture fees from Genzyme Sanofi and Polatom. B.J.: Travel grants and lecture fees from Genzyme Sanofi and Polatom. T.O., A.B., M.K., A.W., A.Co., and A.Cz. declare no competing interests related to the present work.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2