
Abstract
Background:
The current dogma is a life-long follow-up for patients treated for follicular-derived differentiated thyroid cancers (DTC). Our primary objective was to determine the time to recurrence in a series of DTC patients with an excellent response to therapy 6 months after total thyroidectomy and radioiodine therapy. The secondary objectives were to determine the time to suspicion of recurrence and to identify factors associated with recurrence.
Methods:
This retrospective cohort study included patients treated for DTC between 2008 and 2012 and in remission 6 months after total thyroidectomy and radioiodine treatment. The criteria for remission were negative imaging and suppressed thyroglobulin (Tg) <0.2 ng/mL or rh-TSH-(recombinant human TSH) stimulated Tg <1 ng/mL according to the 2015 ATA (American Thyroid Association) guidelines. Recurrence was defined by cytologically and/or histologically proven cervical lymph node metastasis or the administration of a second radioiodine treatment.
Results:
Among 721 patients treated for DTC, 158 were excluded because of persistent disease at 6 months, 71 because of missing follow-up data, and 492 were included. The mean and median follow-up time were 7.0 and 7.9 years (interquartile range IQR [2.1–11.3]). Recurrence occurred for 7 patients (1.4%), 1 initially classified as high recurrence risk, 3 as intermediate, and 3 as low risk according to the 2015 ATA guidelines. All relapses occurred within 10 years after initial management (4 within the first 5 years). For patients with recurrence, rise in Tg and/or suspicious lymph nodes were detected in six out of seven cases in the first 8 years and for the last case 10 years after initial surgery.
Conclusion:
Low and intermediate recurrence risk DTC patients with excellent response 6 months after total thyroidectomy and radioiodine and in remission 10 years later have an extremely low recurrence risk. Follow-up might be undertaken by primary care providers from this time point. These discharge recommendations should be confirmed by further prospective studies.
Introduction
Follicular-derived differentiated thyroid carcinoma (DTC) is the most common endocrine cancer. The overall clinical outcome of DTC is favorable, with a very low death rate. 1 –3 Retrospective studies published over the last decade have reported that excellent response to initial therapy, as defined by the American Thyroid Association (ATA) guidelines, confers a 1.4–2.9% risk of recurrence. 4 –7 This is in line with the dynamic risk stratification concept demonstrating a low recurrence risk for patients with excellent response to initial therapy whatever their initial recurrence risk. 8,9 However, guidelines have not adopted the idea of discontinuing surveillance for this specific group of patients, who constitute most newly diagnosed cases of DTC. Historical publications have demonstrated time to recurrence longer than 5 years and up to 40 years. 10 Thus long-term follow-up is the current dogma for patients with DTC despite the impact of long-course and intense follow-up on quality of life and the considerable burden on health care systems. 11 –13
The primary objective was to determine recurrence rate and time to recurrence in a cohort of patients in remission after total thyroidectomy and radioactive iodine therapy for follicular-derived DTC and thus to extrapolate timing of discharge from oncologic follow-up for DTC patients in remission after initial treatment. The secondary objectives were to determine the time to suspicion of recurrence based on detectable thyroglobulin (Tg) or Tg-antibodies (TgAbs) and/or suspicious neck ultrasound findings and to identify factors associated with recurrence.
Patients and Methods
Patient selection and study design
We conducted a retrospective cohort study of consecutive patients treated for follicular-derived DTC with total thyroidectomy and radioiodine therapy between 01/01/2008 and 31/01/2012, in remission 6 months after initial treatment and followed up in our tertiary care center. Data were collected prospectively as part of routine care on a dedicated database (EPITHYR, APHP registry number 20200115171338) and reviewed retrospectively from this database and medical records whenever necessary. Radioiodine therapy indication was discussed on a regular basis in multidisciplinary staff meetings in our center. Patients were excluded if they were not in remission at 6 months, had missing data (unknown status at 6 months) or had not a minimum of 12 months follow-up after total thyroidectomy.
Patients were considered in remission at 6 months if they met the criteria of “excellent response” according to the ATA 2015 guidelines: negative imaging and suppressed Tg <0.2 ng/mL or TSH-stimulated Tg <1 ng/mL without Tg antibodies. 7
For each tumor, AJCC/pTNM status was determined using the WHO 2022 classification. 14
Definition and diagnosis of recurrence
Patients were considered to present a recurrence, in the following cases: Loco-regional recurrence, including a thyroid bed, soft tissue, or neck lymph node recurrence assessed by histological and/or cytological analysis or radioiodine uptake in the neck; Administration of a second therapeutic dose of radioiodine; Distant metastases cytologically and/or histologically proven or with radioiodine uptake.
Suspicion of recurrence was defined by detectable Tg concentrations (Tg ≥0.2 ng/mL); and/or detectable TgAbs concentrations; and/or suspicious findings on neck ultrasound not proven histological and/or cytological analysis and without subsequent radioiodine treatment.
Assessment of recurrence risk
Recurrence risk was assessed retrospectively according to the ATA 2015 classification: low (≤5% of recurrence), intermediate (5–20%), or high (≥20%). 7
The patients in our series were considered at high risk of recurrence in the following cases: Macroscopic invasion of tumor into the perithyroidal soft tissues, Follicular thyroid cancer with extensive vascular invasion (>4 foci of vascular invasion), pN1 with any metastatic lymph node ≥3 cm at the largest point, Postoperative serum Tg suggestive of distant metastases.
The patients in our series were considered at intermediate risk of recurrence in the following cases: Microscopic invasion of tumor into the perithyroidal soft tissues, Aggressive histology (tall cell, hobnail variant, columnar cell carcinoma), Papillary thyroid cancer with vascular invasion, Presence of radioiodine-avid metastatic foci in the neck on the first post-treatment whole-body radioiodine scan, Tumor classified cN1 or pN1 with >5 pathologic lymph nodes <3 cm at the largest point.
Patients were considered at low risk of recurrence if they met none of the above criteria.
Moreover, the MACIS prognostic score was calculated retrospectively, using the published formula: 3.1 (if aged less than or equal to 39 years) or 0.08 × age (if aged over or equal to 40 years), + 0.3 × tumor size (in centimeters), +1 (if incompletely resected), +1 (if locally invasive), +3 (if distant metastases present). 15
Follow-up
Patient follow-up data were obtained from a database (EPITHYR; APHP registry number 20200115171338), medical records, and periodic correspondence with patients or their referring physicians.
The follow-up protocol consisted of regular clinical examinations, serum Tg level measurement under Levothyroxine (LT4) after recombinant human TSH (rh-TSH) stimulation, detection of TgAbs, and neck ultrasonography. 7,16
Abnormal biochemical results were confirmed in our center if they led to suspicion of recurrence. Tg assay and TgAbs detection were performed by immunoassay (Beckmann Coulter Dxi 600). 17
At the end of the study, patients’ status was analyzed. Patients were considered, as defined by the ATA 2015 guidelines:
7
In remission (Tg <0.2 ng/mL or stimulated-Tg <1 ng/mL and negative imaging); Or presenting a biochemical incomplete response, defined by detectable Tg concentration (Tg >1 ng/mL or stimulated-Tg >10 ng/mL) or rising TgAbs levels in the absence of structural disease; Or presenting structural incomplete response, defined by persistent or newly identified loco-regional or distant metastases; Or presenting indeterminate response, defined by nonspecific biochemical or structural findings that cannot be confidently classified as either benign or malignant. This includes patients with stable or declining TgAbs levels without definitive structural evidence of disease.
Statistical analysis
Patient characteristics are reported as mean values, median values, IQR, and ranges (continuous variables) or absolute numbers and percentages (categorical variables). Time to recurrence was analyzed. Time to suspicion of recurrence was analyzed firstly considering patients that have presented a recurrence as defined above and secondly also including patients with biochemical incomplete response at the end of the follow-up.
Univariate Cox proportional hazards regression was used to identify variables associated with recurrence-free survival. Results were expressed as Hazard Ratio (HR) with 95%CI (Confidence Interval). Missing data were censored. Due to the small number of events (n = 7), multivariable analyses could not be performed. Survival curves were obtained with Kaplan–Meier estimates and compared with log-rank test. The proportional hazards assumption was checked for each model using graphical methods based on Kaplan–Meier curves and the scaled Schoenfeld residuals. All p-values were two-sided and the level of significance was set at p < 0.05. All analyses were performed using RStudio 2021.09.0 with the packages “tidyverse,” “ggplot2,” “gdata,” “survival,” and “survminer.”
Ethics
The study research was completed in accordance with the Declaration of Helsinki, as revised in 2013. 18 In accordance with French regulations, retrospective studies exclusively reliant on anonymized patient data are not mandated to seek approval from “committees for the protection of individuals.” Patient follow-up data were obtained from the database EPITHYR (APHP registry number 20200115171338), which has been approved by the Data Protection Officer of our University Hospital. A nonopposition form for use of anonymized clinical data for research is signed by patients before their inclusion in the EPITHYR database.
Results
Patient selection
Between 01/01/2008 and 31/01/2012, 721 patients were treated for follicular-derived DTC with total thyroidectomy and radioiodine therapy and followed up in our tertiary care center. Among these 721 patients, 229 patients were excluded: 158 patients were not in remission at 6 months (48 had structural incomplete response, 62 biochemical incomplete response, and 43 indeterminate response), 55 patients had missing data (unknown status at 6 months), and 16 patients had not a minimum of 12 months follow-up after total thyroidectomy. Among the 721 patients, 6 had distant metastases at diagnosis and none were in “excellent response” at 6 months, as a result, patients included in the final cohort were all M0 at diagnosis.
Among the 229 patients excluded from our study, the initial recurrence risk could be assessed for 194 patients and was, respectively, high for 30 patients (15.5%), intermediate for 79 patients (40.7%), and low for 85 patients (43.8%).
The final cohort included 492 patients in remission at 6 ± 2 months of radioiodine therapy (Fig. 1).
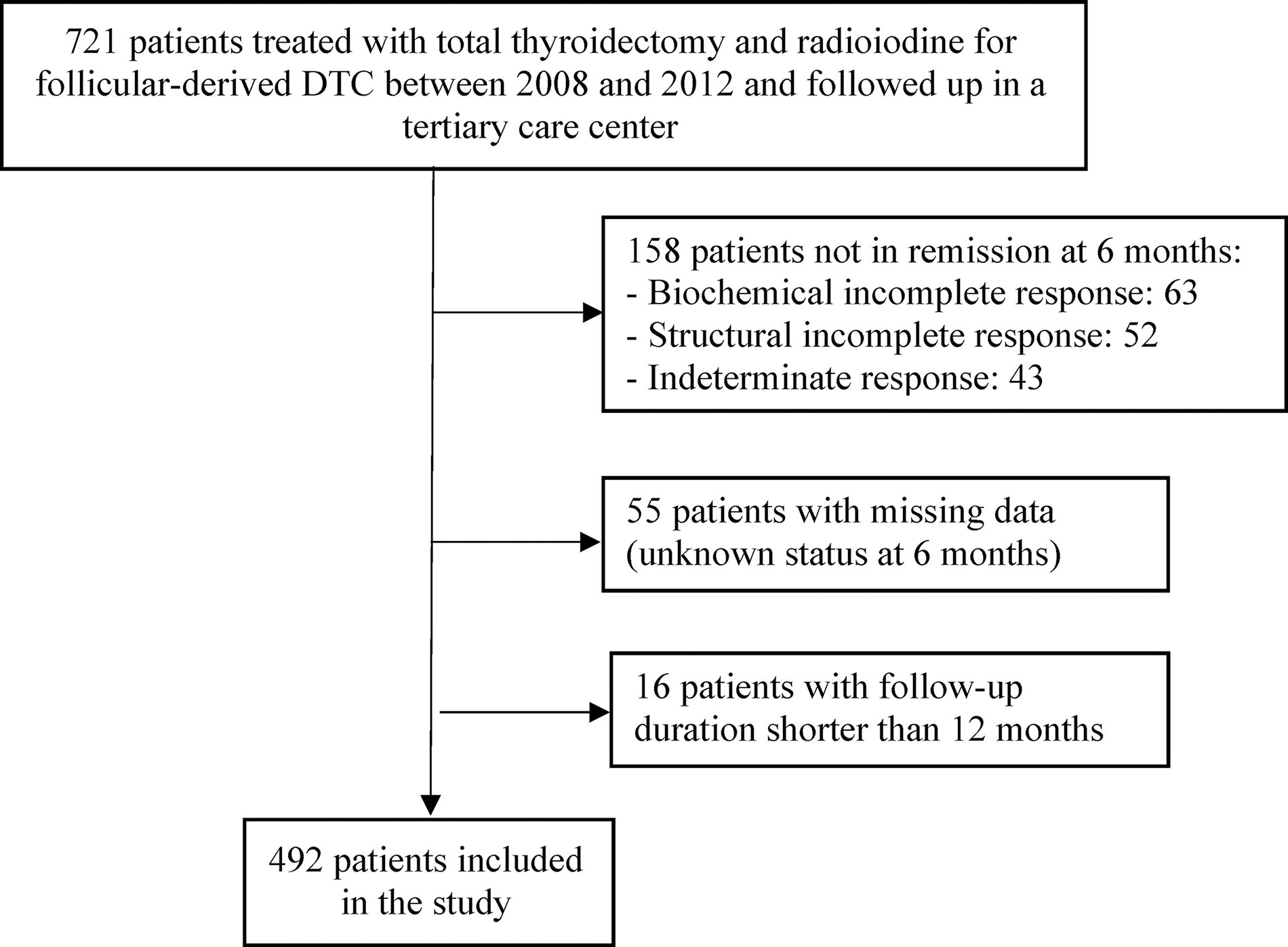
Participant flowchart.
Characteristics of the study population
Table 1 shows the characteristics at baseline of the 492 patients included. Mean age was 48.6 years (±14.1). Papillary carcinoma accounted for 90% of the cohort. Aggressive histology types and subtypes accounted for only 2% of the series. Most patients met the ATA criteria for low recurrence risk (66.9%). Table 2 indicates on which criteria the ATA risk level was established. The MACIS score was below 6 for 91.9% of patients.
Characteristics of the Study Population at Baseline
Tumor size was unknown for one patient.
Number of vascular invasion foci was unknown for 12 patients with vascular extension.
Tg after surgery was available for 340 patients: 5 patients with recurrence and 336 patients without recurrence.
ATA, American Thyroid Association; ETE, ExtraThyroidal Extension; GBq, Gigabecquerel; IQR, InterQuartile Range; RAI, RAdioIodine; Tg, Thyroglobulin.
Characteristics of Study Population with ATA Intermediate or High Recurrence Risk Level
Follow-up
The median and mean follow-up time were, respectively, 7.9 years (IQR 2.26–11.3) and 7.0 years. The duration of follow-up exceeds 10 years for 179 patients (36.3%) and 8 years for 242 patients (49.1%). Among the 492 patients in remission 6 months after initial treatment, 7 (1.4%) presented with a recurrence.
At the end of the study, out of the patients without recurrence, 471 (95.7%) were in excellent response, 2 (0.4%) presented with a biochemically incomplete response, and 12 (2.4%) an indeterminate response (n = 5 with nonspecific imaging findings and n = 7 with Tg 0.2–1 ng/mL or stimulated Tg 1–10 ng/mL).
A total of two deaths unrelated to the thyroid cancer were reported during the study time.
Description of recurrences
Among the 7 patients (1.4%) with recurrence, 3 patients had additional neck surgery because of cytologically-proven locoregional recurrence (2 recurrences in the lateral compartment of the neck, 1 both in the central and lateral compartment, and 1 in the central compartment only) and 4 received a second radioiodine treatment.
Among the 3 patients with cytologically-proven neck recurrences, one of them had isolated elevation of Tg concentration under LT4, 3.6 years prior to neck recurrence. The two other neck recurrences were detected due to abnormal routine imaging.
For 4 patients, second radioiodine treatment was indicated because of ascending slope of Tg (Tg under LT4 above 2 ng/mL or stimulated Tg above 5 ng/mL. For 3 of 4 patients (patients 1, 2, and 5), the second radioiodine treatment was also motivated because of small suspicious lesions seen on neck ultrasound or FDG-PET outside surgical indications due to their small size (patient 1) or to their localization (patients 2 and 5). Patient 6 presented with normal imaging before second radioiodine treatment despite an increase of Tg under LT4 from 0.3 to 4.4 ng/mL in 14 months). Before second radioiodine treatment, stimulated-Tg was 6.8 ng/mL for patient 1 and Tg under LT4 were, respectively, 6.4, 8.6, and 4.4 ng/mL for patients 2, 5, and 6.
Time to disease recurrences
Characteristics of patients with recurrence and time to recurrence and to suspicion of recurrence are shown in Table 3.
Patients with Recurrences
FDG, FluoroDeosoxyGlucose; FNA, Fine Needle Aspiration; RAI, RAdioIodine; Tg, Thyroglobulin, in ng/mL; TgAb+, positive Thyroglobulin Antibodies; TSH, (mUI/L); US, UltraSound.
Median and mean time to suspicion of recurrence (Tg ≥0.2 ng/mL and/or suspicious findings on neck ultrasound) were, respectively, 5 and 5.9 years (3.9–8.8). Median and mean time to recurrence were, respectively, 8 and 7.4 years (3.9–10.4). For patients 1 and 5, ultrasensitive Tg became detectable 8.1 and 3.9 years after radioiodine ablation and they finally received additional radioiodine therapy at 9.7 and 8 years.
Recurrences were suspected within 6.8 years in 91.4% of the cases and all of them were suspected within 8.8 years. Recurrences occurred within 9 years in 91.4% of the cases and all of them within 10.4 years. Recurrence-free survival is represented in Fig. 2. Time to recurrence and to suspicion of recurrence are represented in Fig. 3.
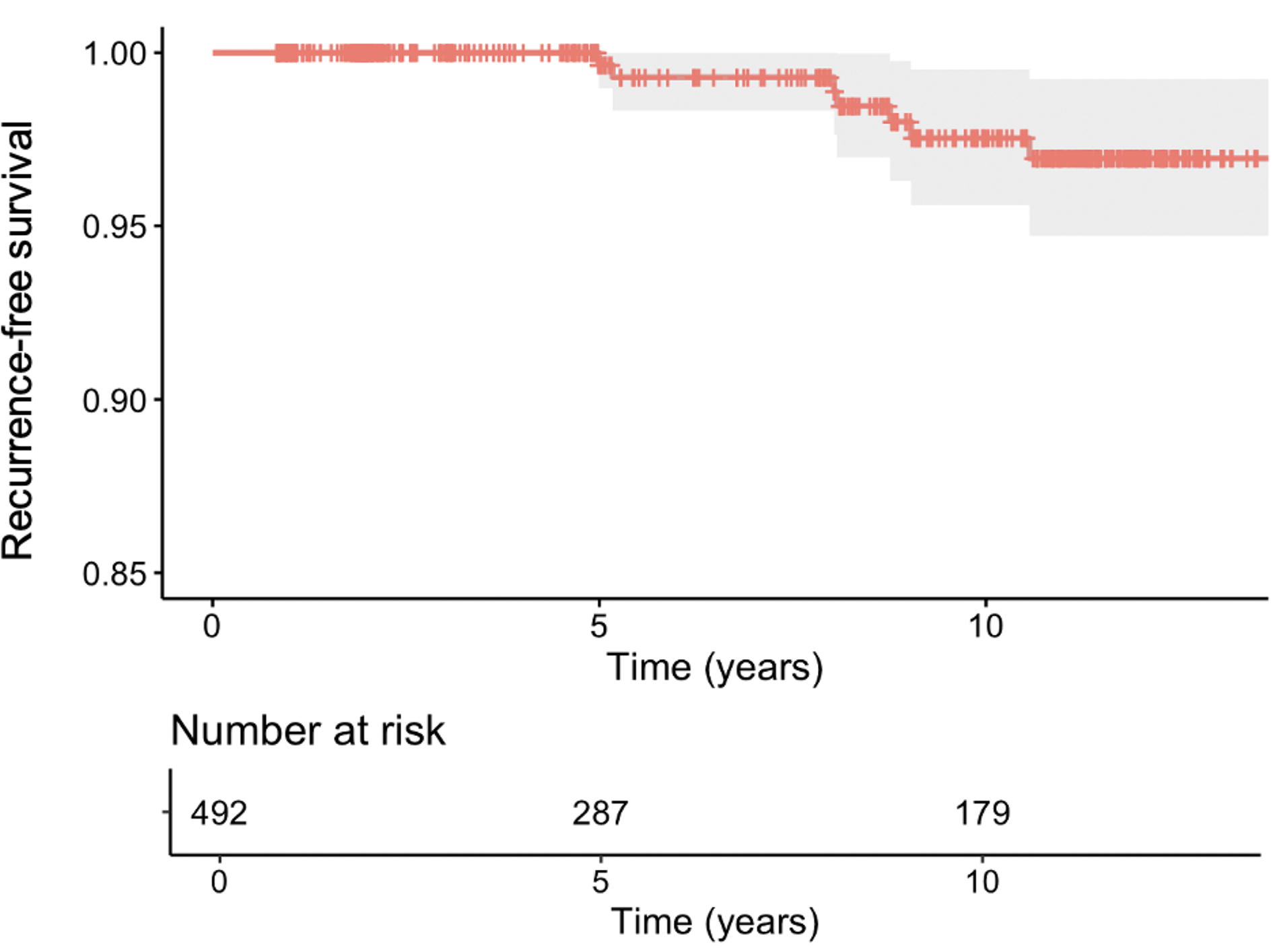
Recurrence-free survival among patients in excellent response 6 months after total thyroidectomy and radioiodine (n = 492).
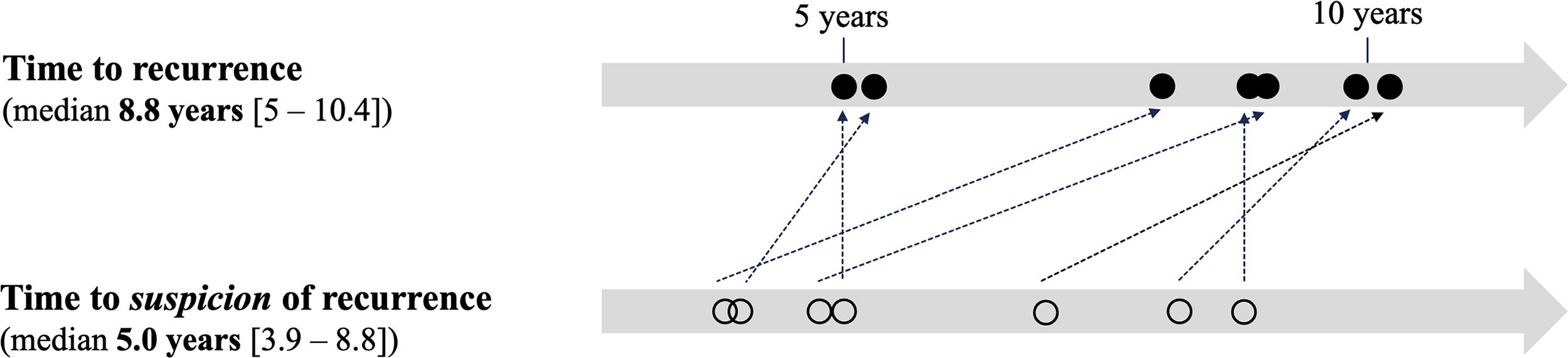
Median time to recurrence and to suspicion of recurrence.—
None of the 4 patients who received a second radioiodine treatment had an excellent response after treatment. None of them presented with radioiodine-avid cervical or extra-cervical uptake on the post-treatment scan. Patient 1 presented with indeterminate response 4 months after a second radioiodine treatment (Tg under LT4 0.2 ng/mL, multiple intermediate cervical lymph nodes). Patient 2 was classified as radioiodine refractory because of the absent radioiodine uptake in a suspicious lymph node. Patient 5 presented with a biochemical and structural incomplete response 3 months after second radioiodine treatment (Tg under LT4 5.6 ng/mL, persistence of a cervical lymph node without radioiodine uptake, appearance of pulmonary micronodules). Patient 6 presented with a biochemical incomplete response 2 years after a second radioiodine treatment (Tg under LT4 12 ng/mL).
Factors associated with recurrences
Women represented 71.4% of patients with recurrence (5/7). Histological type was papillary cancer in 71.4% of the cases (5/7). The mean tumor size of the initial thyroid carcinoma was 30.3 mm (±19.9 mm). Initial ATA recurrence risk of patients with recurrence was high for 1 patient (14.3%), intermediate for 3 patients (42.8%), and low for 3 patients (42.8%). Rates of recurrences of patients with ATA low, intermediate, and high recurrence risk were, respectively, 0.9%, 1.9%, and 14.3%. The MACIS mean and median scores were 5.43 and 4.9, respectively, for patients with recurrence.
Comparison of patients with and without recurrence is shown in Table 4. The rates of histological characteristics (poorly differentiated vs. other histological types), vascular invasion, number of vascular foci, tumor size, and MACIS score were significantly different between the two groups. Regarding histology, papillary cancer was less represented among patients with recurrence (p = 0.01, HR 14.4 [1.7–120.5]). Patients with recurrence more often presented with vascular invasion (p = 0.04, HR 8.1 [1.8–36.3]) and number of vascular foci was higher in these patients (vascular foci ≥4 or <4, p = 0.01).
Table 4. Factors Associated with Recurrence (Univariate Analysis)
As the 2 reported deaths were unrelated to thyroid cancer and these patients still had “excellent response” at their last visit, they were considered freed of disease at the end of follow-up in this analysis.
Tg after surgery was available for 340 patients: 5 patients with recurrence and 336 patients without recurrence.
p trend.
CI, confidence interval; ETE, Extrathyroidal extension; IQR, InterQuartile Range.
Given the small number of patients with high ATA recurrence risk (n = 6), this subgroup was grouped with intermediate-risk patients. Comparison of the ATA risk level showed no statistical difference between groups (p = 0.2). Among the six patients with high ATA risk level, one showed recurrence (1.4%) after a follow-up of 8.1 years, while the remaining 5 patients were in remission at the end of the follow-up. Fig. 4 shows Kaplan–Meier curves comparing carcinomas with low, intermediate/high risk of recurrence (p = 0.2).
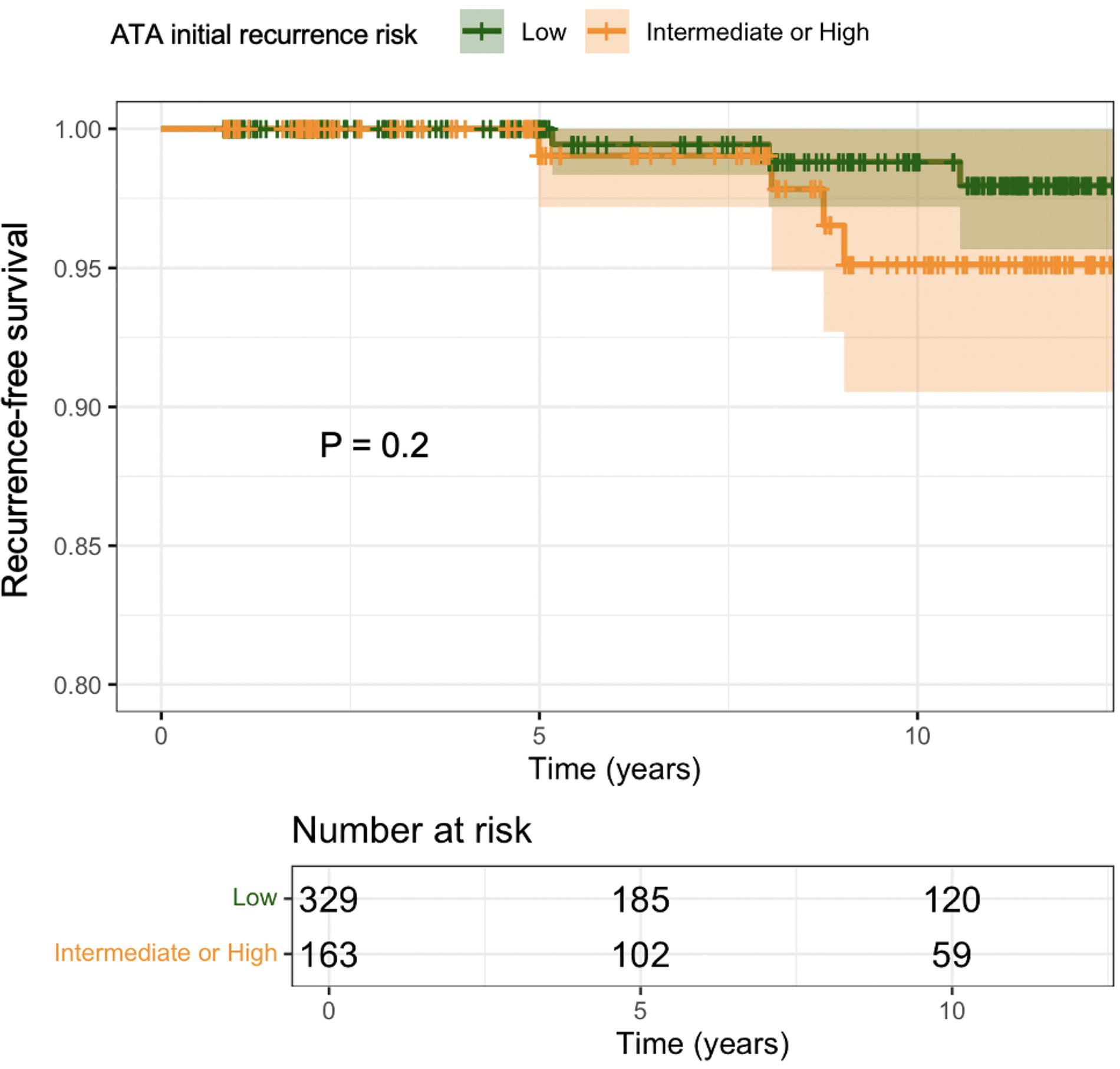
Recurrence-free survival depending on ATA initial recurrence risk. ATA, American Thyroid Association.
Comparison of other characteristics showed no statistical difference between groups.
Patients with biochemical incomplete response at the end of the follow-up
Among the 2 patients with a biochemically incomplete response at the end of the follow-up, time to elevation of Tg or first observation of TgAbs were 1.9 and 11 years and Tg under LT4 were 1.47 and 1.50 ng/mL. For the patient with first observation of abnormal Tg results at 11 years, it is notable that this patient was in remission until 4 years after initial management but lost to follow-up without any Tg dosage until 11 years after total thyroidectomy. ATA initial recurrence risk was low for these 2 patients. No further imaging (i.e., FDG-PET, neck, and chest CT) besides neck ultrasound (US) was performed as Tg under LT4 did not exceed 1.5 ng/mL. As these 2 patients can still be considered at high recurrence risk during subsequent follow-up, median time to suspicion of recurrence was also assessed including them and found to be 5.2 years.
Patients with indeterminate response at the end of the follow-up
Among 12 patients with indeterminate response at the end of the follow-up, 5 had unspecific structural findings on neck ultrasound, 7 presented with elevation of Tg that did not meet the definition of biochemical indeterminate response. ATA initial recurrence risk was intermediate for 8 patients (66.7%) and low for 4 patients (33.3%). None of them had had a high initial risk of recurrence.
Discussion
The prognosis of DTC is overall favorable and recurrences are rare. 4 –6 No guidelines recommend stopping surveillance at any particular time point. However, series published in the last decade have demonstrated that the vast majority of recurrences occurred within the first 8 years after initial treatment for patients with excellent response to initial therapy: 80% within 5 years, almost all of them within 8 years according to Jeon et al., 19 77% within 5 years and all of them within 8 years according to Durante et al. 6 In another recent work published by Palyga et al., 5 1.4% patients treated for DTC between 1998 and 2021 presented with recurrences, among which 62.5% occurred within 5 years and 87.5% within 10 years. In this cohort, one patient with pT1aNxM0 papillary thyroid cancer showed structural recurrence 16 years after surgery. Time to suspicion of this structural recurrence would have been an interesting piece of data but was unfortunately unavailable in this series reporting patients managed over a wide interval of time (1998–2021).
The duration of follow-up for patients in remission after the initial treatment for DTC is an important concern, as lifelong surveillance can significantly affect their quality of life. Such extended monitoring is associated with lower mental health scores, 11,20 more frequent somatic complaints, 12 and notable impacts on professional life 21 for these patients.
Our series of 492 patients in remission after total thyroidectomy and radioiodine therapy for DTC demonstrated that all recurrences were diagnosed within 10 years after initial management. Our study is original in that, in addition to the time to recurrence, we analyzed the time to suspicion of recurrence and found that all recurrences were suspected within 8 years after initial management. Indeed patients 1, 5, and 6 who received additional radioiodine therapy 8–9 years after initial treatment presented with elevated Tg concentrations between 4 and 7 years of follow-up. Patient 3 who was treated for locoregional recurrence after 10 years of follow-up presented with detectable TgAbs within 6 years from initial therapy.
Furthermore, for the 2 patients with biochemical incomplete response at the end of the follow-up without recurrence, time to elevation of Tg or first observation of TgAbs were 1.9 and 11 years. It is notable that the patient who presented with a first abnormal biochemical results at 11 years of follow-up was lost to follow-up after 4 years from initial treatment.
Of note, our study population characteristics, recurrence rates, and median time of follow-up that is., 7.1 years were similar to previous studies. 4 –6,19
The median time to recurrence was slightly longer in our cohort than that reported in the study published in 2013 by Durante et al. (8 years vs. 3.6 years) but time to suspicion of recurrence was relatively similar (5 years).
Based on our results, we suggest that patients with an “excellent response” 6 months after total thyroidectomy and radioiodine treatment, without recurrence and with undetectable Tg and TgAbs and normal neck ultrasound after 10 years might not benefit from further oncologic monitoring as they have virtually no recurrence risk and that cessation of patient surveillance, excluding TSH surveillance, at that time point, is possible. Alternatively, monitoring could be spaced out considerably and undertaken by primary care providers from this time point. 1,5,6,19,22 Successful experiences of follow-up by primary care providers were reported, potentially providing significant economic benefit for the healthcare system. 23 In our center, patients with excellent response at the first post-treatment evaluation are offered to be discharged to primary care providers with specific instructions for follow-up (frequency of clinical examination, Tg measurement, and neck ultrasound). Patients 1 and 5 were indeed followed up by their secondary care endocrinologist and referred to our center due to elevated Tg levels. However, data on the nature of the monitoring is not available for all patients in our cohort and prevents any formal conclusion concerning the efficiency of follow-up by primary care providers. Further prospective studies must be carried out to examine the outcomes of strategies for the transfer of oncological follow-up from specialists to primary care providers.
In our series, only 15 patients (3%) did not have an excellent response at the end of the follow-up. For these patients, we suggest continuing oncological monitoring.
Regarding prognostic factors for recurrence, age, 24 –26 sex, 25,26 family background of cancer, 27 pTNM, 28 vascular invasion, 29 extra-thyroidal extension, 30 –32 lymph node involvement, 26,30,33 and metastasis 32 have previously been established as predictors. Comparison of patients characteristics with and without recurrence revealed, as previously reported, that histology, 34,35 invasion (vascular or extra-thyroidal versus none), 32 number of vascular foci, tumor size, and MACIS score 29 differed between the two groups and were associated with recurrence. Unfortunately, the low number of events did not allow for an adjusted analysis. Interestingly, stimulated-Tg at the time of radioiodine ablation was not associated with recurrence, in contrast with previous studies. 36 However, the fact that our study focused specifically on patients with excellent response 6 months after total thyroidectomy and radioiodine therapy could explain the discrepancy with previous literature.
Our results support the dynamic risk stratification concept based on the response to initial treatment, 37 especially for initial low- and intermediate-risk patients. This concept initially published in 2010 8 demonstrated that the recurrence risk of patients with excellent response after initial therapy drops to 0–4% 37 and suggested an adapted approach to follow-up not based solely on the initial risk stratification. However, the validity of this concept for the rare high-risk patients in remission after initial therapy remains disputable. In our series one out of the five patients (16.7%) with ATA high initial recurrence risk was diagnosed with a recurrence after a follow-up of 8.1 years, the remaining six patients being in remission at the end of the follow-up. This result is consistent with the first publication regarding the dynamic risk stratification concept 8 where the recurrence rate among high-risk patients in remission after initial treatment was of 14% (2/14). 8
The small number of initial high-risk patients having excellent response 6 months after initial therapy in our study (n = 6) precludes any definitive conclusion regarding the duration of follow-up required in this, by definition, rare category of patients. Given the greater proportion of recurrence among high-risk patients compared to other risk categories, a rigorous monitoring remains probably mandatory.
It is interesting to highlight that in our cohort, all patients with recurrence had either elevated Tg concentration or detectable TgAbs at the time of suspicion of recurrence. None of our patients with locoregional recurrences had isolated neck ultrasound structural lesions with undetectable Tg and no TgAbs. This result is in line with the high sensitivity of Tg dosage, especially ultrasensitive Tg to detect recurrence and the exceptional cases of neck recurrence without biochemical abnormalities. As previously reported, low- and intermediate-risk PTC patients with no evidence of disease after thyroidectomy, especially negative US findings and undetectable or even low Tg concentrations can be safely followed with unstimulated serum Tg dosages and additional neck US only in case of increasing Tg levels and/or appearance of Tg Ab. 38,39 However, our study was not designed to specifically address this issue.
One limitation of our study is the median follow-up below 10 years (7.9 years) even if a substantial proportion of patients were followed-up longer than 8 and 10 years (respectively, 47.6% and 31.3%). We deliberately focused on patients treated between 2010 and 2012 to extrapolate our results to current patients with similar follow-up protocols, unlike other studies reporting patients managed as early as 1990 6 or 1998. 5 All patients treated and monitored for a thyroid cancer in our institution are included in a database named EPITHYR and patient follow-up data are obtained for all patients included in this database besides the medical records from town council registers and periodic correspondence with patients or their referring physicians. As our center is a tertiary care center, any patient lost to follow-up but diagnosed with a late recurrence or an abnormal check-up would normally have been referred to us for further treatment. This off-site long-term follow-up implies that all Tg and TgAb dosage were not performed in our center resulting in some heterogeneity.
We did not account for confounders in our analyses due to limited study size and event rates. Moreover, missing data, inevitable in a retrospective study, may have biased the analysis. In particular, 55 patients were excluded because of missing status at 6 months and 16 patients had not a minimum of 12 months follow-up after total thyroidectomy: however, we assume that these patients would have been referred to our center for further investigation if they later showed any clinical or biochemical abnormality. Finally, we agree that our data are limited in external generalizability as they apply to patients with low- and intermediate-risk DTC treated with total thyroidectomy and radioiodine therapy and the results may not apply to patients who were treated with other approaches that is lobectomy.
Our study supports our current follow-up protocol consisting in discharging patients with an excellent response after initial management to primary patients care, providing explicit guidelines regarding follow-up protocols (target TSH, frequency of ultrasensitive Tg dosage, frequency of neck US if necessary, and indications for referral for specialist care).
Low and intermediate recurrence risk DTC patients with excellent response 6 months after total thyroidectomy and radioiodine therapy and still in remission 10 years later have an extremely low recurrence risk and may be considered for discharge from tertiary care oncologic follow-up. Further prospective studies must be conducted to validate our extrapolated findings on discharge from oncologic care.
Footnotes
Acknowledgments
The authors are grateful to all the doctors and nurses of Hôpital Pitié-Salpêtrière, who were responsible for patients follow-up. The authors also thank Mrs. Liz Atzel for English language editing and review services.
Authors’ Contributions
A.A.: Investigation, Data curation, Formal analysis, Writing—Original Draft, Visualization; E.T.: Investigation, Resources, Writing—Review and Editing; A.J.: Formal analysis, Validation; C.G., M.R., N.C.: Resources, Data Curation, Writing—Review and Editing; C.L.-L., F.M., S.H.: Resources, Writing—Review and Editing; L.L.: Resources, Data Curation, Supervision, Writing—Review and Editing; C.B.: Conceptualization, Methodology, Writing—Review and Editing, Supervision, Project administration.
Author Disclosure Statement
The authors have nothing to disclose.
Data Availability
Data in this study are available upon request from the corresponding author. These data cannot be made public due to the privacy of patients’ data.
Funding Information
No funding to declare.