
Abstract
Introduction:
The 2015 American Thyroid Association (ATA) guidelines recommended thyroid lobectomy (TL) as an alternative to total thyroidectomy (TT) for the surgical treatment of low-risk differentiated thyroid cancer. Increasing use of TL has since been reported despite concerns for an increased risk of disease recurrence and need for reoperation. This study sought to compare reoperation rates among patients who underwent initial TL or TT for malignancy, characterize trends at centers based on operative volume, and examine factors associated with reoperation.
Methods:
We queried the Vizient Clinical Data Base for TL and TT performed preguideline change (pre-GC = 2013–2015) and postguideline change (post-GC = 2016–2021). Reoperations included reoperative thyroid surgery (RTS) and neck dissection (ND); timing was defined as early (≤180 days), thought to indicate inadequacy of initial operative choice, or late (>180 days), suggesting potential disease recurrence.
Results:
Of 65,627 patients, 31.8% underwent initial TL and 68.2% underwent initial TT; TL increased from 21.4% of total cases pre-GC to 37.0% post-GC (p < 0.001). Among TL patients, early RTS declined from 33.9% to 14.2% and ND declined from 0.8% to 0.4% (p < 0.001). Among TT patients, early RTS remained 0.2%, while ND increased from 0.4% to 0.7% (p < 0.001). TL-associated late RTS declined from 2.0% to 1.7%, while ND increased from 0.6% to 0.8% (p = 0.17). In TT patients, both late RTS and ND increased, from 0.2% to 0.3% (p = 0.04) and 1.7% to 2.1% (p < 0.01), respectively. There was no difference in the late reoperation rate for TL compared with TT post-GC (+0.2%, p = 0.18). TL volume grew annually by 12.5% [8.9−16.2%] at high-volume centers (HVCs) and 8.3% [5.6−11.1%] at low-volume centers (LVCs). TL-associated reoperations at HVCs declined annually by 12.6% [5.6−19.0%] and 10.8% [2.7−18.1%] at LVCs. Uninsured status and more recent initial operation were associated with an increased risk of late reoperation (HR = 1.84 [1.06−3.20] and HR = 1.30 [1.24−1.36], respectively). The type of index operation performed, however, was not predictive of late reoperation.
Conclusions:
The rate of early reoperations declined for TL after the 2015 ATA guideline release, but late reoperations remained unchanged despite a significant shift in practice patterns towards initial lobectomy. Patients appear to be receiving less aggressive, guideline-concordant care without a significant increase in the late reoperation rate for TL compared with TT.
Introduction
The publication of the 2015 American Thyroid Association (ATA) guidelines marked a major turning point in the surgical management of low-risk differentiated thyroid cancer (DTC). Following a growing number of studies that demonstrated non-inferior outcomes in patients who underwent thyroid lobectomy (TL) compared with total thyroidectomy (TT), the ATA updated its recommendation to offer either operation as “a reasonable surgical approach for patients with DTC measuring 1–4 cm without evidence of extrathyroidal extension or clinically apparent lymph node disease.” 1
This recommendation was widely considered to be the most controversial update of the 2015 revision due to concerns that a subtotal gland resection would result in higher rates of both disease recurrence and reoperation. 2,3 Subsequent studies have yielded conflicting results. Several retrospective studies have estimated that 43–59% of patients who would have been newly eligible for TL would be subsequently found on histopathology to have high-risk features that would necessitate completion thyroidectomy. 4 –9 Several large single-center retrospective studies have also reported higher recurrence rates and worse survival in patients with DTC who underwent TL compared with those who received TT. 10 Other studies, however, have found no significant increase in either recurrence or reoperation rates after TL. 11,12
Despite these concerns, increasing rates of lobectomy have been reported since publication of the 2015 guidelines. 13,14 True reoperation rates, however, remain unclear. No studies to date have examined case-specific reoperations at the national level to determine whether they have indeed increased, and none have investigated reoperation rates over the short and long term to differentiate reoperation for incomplete initial resection from reoperation for disease recurrence. Despite previously published studies suggesting differences in the rates of guideline awareness and compliance among high- and low-volume surgeons, 15 little is also known about how patterns in operative choice may have differed nationally between these two groups.
The primary aim of this study was thus to examine both early and late case-specific reoperations among patients who underwent either TL or TT for malignancy before and after the 2015 ATA guideline change (GC) in a national cohort. We additionally sought to characterize these trends at high-volume centers (HVCs), medium-volume centers (MVCs), and low-volume centers (LVCs) and to identify factors that were associated with late reoperations in the postguideline change (post-GC) period.
Materials and Methods
Patient selection
Cases were queried in the Vizient Clinical Data Base, a healthcare analytics platform that collects claims data from over 1000 US hospital systems nationally, including 97% of academic medical centers and over 800 community hospitals. Patients aged 18 years and older who underwent either TL or TT between 2013 and 2021 for a diagnosis of thyroid cancer using the International Classification of Diseases (ICD) system, ICD-9-CM 193 or ICD-10-CM C73, were included. Patients who underwent neck dissection (ND) at the time of their initial operation were excluded, as these would have been indicative of more advanced disease that would not qualify for initial TL. Cases from facilities that did not have at least 1 year of data in both study periods were also excluded. A participant flow diagram is shown in Figure 1.
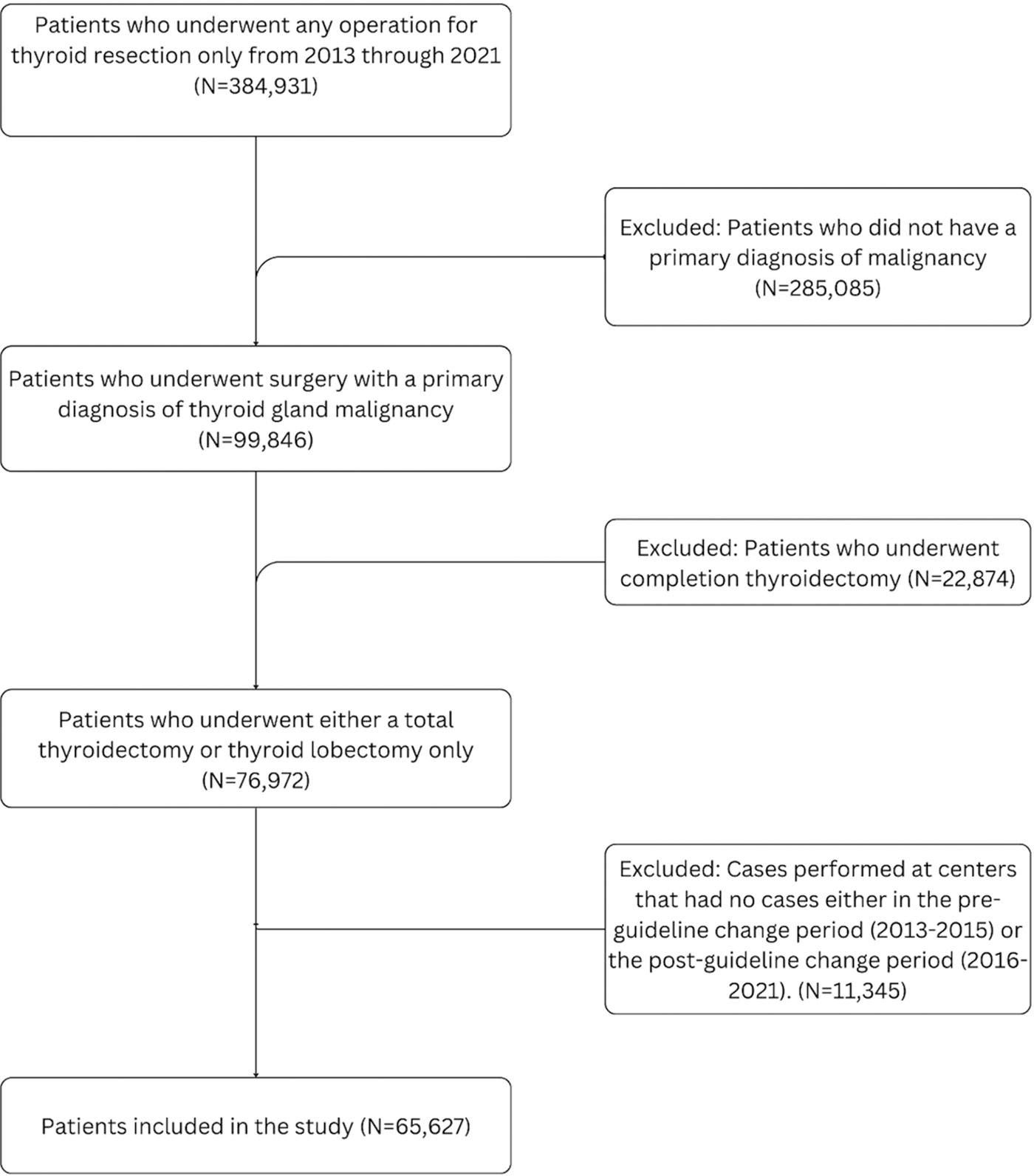
Participant flow diagram.
Study-defined variables
As the 2015 ATA guidelines were published in January 2016, the preguideline change (“pre-GC”) period was defined as 2013–2015 and the postguideline change (“post-GC”) period was defined as 2016–2021. Reoperations were categorized by ICD and Current Procedural Terminology (CPT) codes into two categories, reoperative thyroid surgery (RTS) and central/lateral ND. The RTS category comprises completion thyroidectomies, lobectomies, thyroid gland resections, and other procedures indicative of thyroid tissue removal. NDs included codes for removal of lymphatic tissue from the neck. Included ICD and CPT codes are provided in the Supplementary Table S1.
Reoperations were categorized as early (occurring within 180 days of the initial operation) or late (occurring more than 180 days after the initial operation). Reoperations performed early were presumed to be due to inadequacy of the initial operative choice, typically for final pathology findings that necessitate a completion thyroidectomy. Reoperations performed late were presumed to be undertaken for potential disease recurrence. While there is no time threshold that can definitively distinguish persistent disease from disease recurrence, 16 in the absence of tumor pathology reports, imaging findings, and biochemical data, 180 days was selected as the cutoff based on minimum time to recurrence values cited in the literature. 17 –20
Hospitals were stratified into LVCs, MVCs, or HVCs based on average annual case volumes of combined lobectomies and total thyroidectomies performed for any diagnosis, i.e., inclusive of benign disease; cases for benign disease were otherwise excluded from the analysis. Case volume values were sorted into tertiles to establish ranges for LVC, MVC, and HVC based on average annual case volumes among the included facilities: LVC = 1–49 cases, MVC = 50–135 cases, and HVC = 142–503 cases.
Statistical analysis
The chi-squared test was used to compare proportions of categorical variables and the Mann–Whitney U test was used to compare the medians of continuous variables. Joinpoint regression using a coincident pairwise comparison approach with logarithmic transformation was conducted to evaluate trends in annual case and reoperation rates by hospital volume. Cox regression analysis was performed to evaluate for factors associated with late reoperation in the post-GC period. Statistical analysis was conducted in IBM SPSS Statistics software v28.0.1.1 (14) (IBM Corp., Armonk, NY) and in Joinpoint Regression Program, v4.9.1.0 – April 2022 (Statistical Research and Applications Branch, National Cancer Institute). This study was granted a waiver from the Rutgers University Institutional Review Board review due to the use of a national deidentified patient database.
Results
A total of 65,627 patients across 281 hospitals were included in the study; 44,732 (68.2%) underwent TT and 20,895 (31.8%) underwent TL for thyroid cancer. Over the study period, the proportion of lobectomy relative to TT steadily increased from 19.4% of total cases in 2013 to 42.6% of total cases in 2021 (Fig. 2). There were no differences in age and sex between the TL and TT cohorts. Patients who underwent lobectomy were marginally more likely to be Asian (TL = 6.9% vs. TT = 5.8%, p < 0.001) and to have private insurance (TL = 61.9% vs. TT = 59.8%, p < 0.001) (Table 1). They were more likely to undergo operations at HVCs (TL = 60.3% vs. TT = 56.4%, p < 0.001) and to be treated as an outpatient (TL = 50.2% vs. TT = 28.8%, p < 0.01).
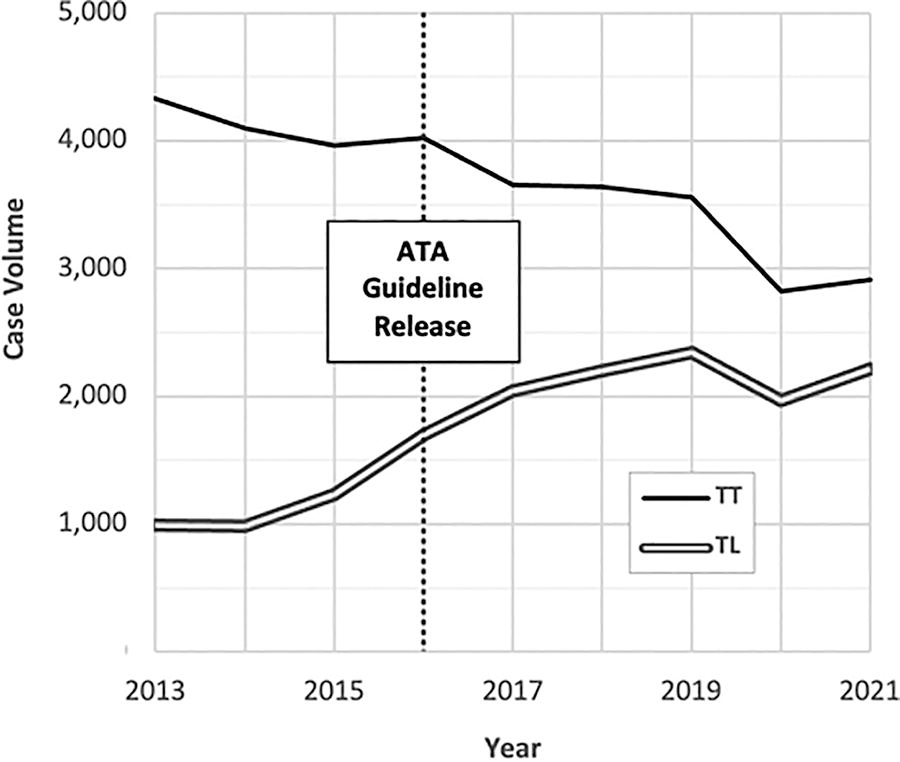
Annual case volumes by type of index operation. ATA, American Thyroid Association; TL, thyroid lobectomy; TT, total thyroidectomy.
Patient Demographics and Perioperative Factors by Type of Index Operation Performed, 2013–2021
Age is provided as the median value within each cohort. Figures reflect complications and death within the same admission as the index operation.
IQR, interquartile range; TL, thyroid lobectomy; TT, total thyroidectomy.
Reoperations pre-GC and post-GC
In total, 5,884 reoperations (9.0% of all index operations) were performed during the study period. The overall reoperation rate for patients who underwent TL decreased from 37.3% in the pre-GC period to 17.1% in the post-GC period. This change was driven primarily by a decline in early reoperations, from 34.8% to 14.6% post-GC (p < 0.001). Late reoperations after lobectomy remained unchanged at 2.6% pre-GC and 2.5% post-GC (p = 0.70) (Fig. 3). The overall reoperation rate for patients who underwent TT increased from 2.6% pre-GC to 3.3% post-GC. Early reoperations in this cohort increased from 0.7% to 1.0% of total cases (p < 0.001) while late reoperations increased from 2.0% to 2.3% (p = 0.01). The late reoperation rates for lobectomy and TT did not differ significantly after release of the 2015 ATA guidelines: compared with TT, the late reoperation rate for lobectomy was only 0.2% higher in the post-GC period (p = 0.18).
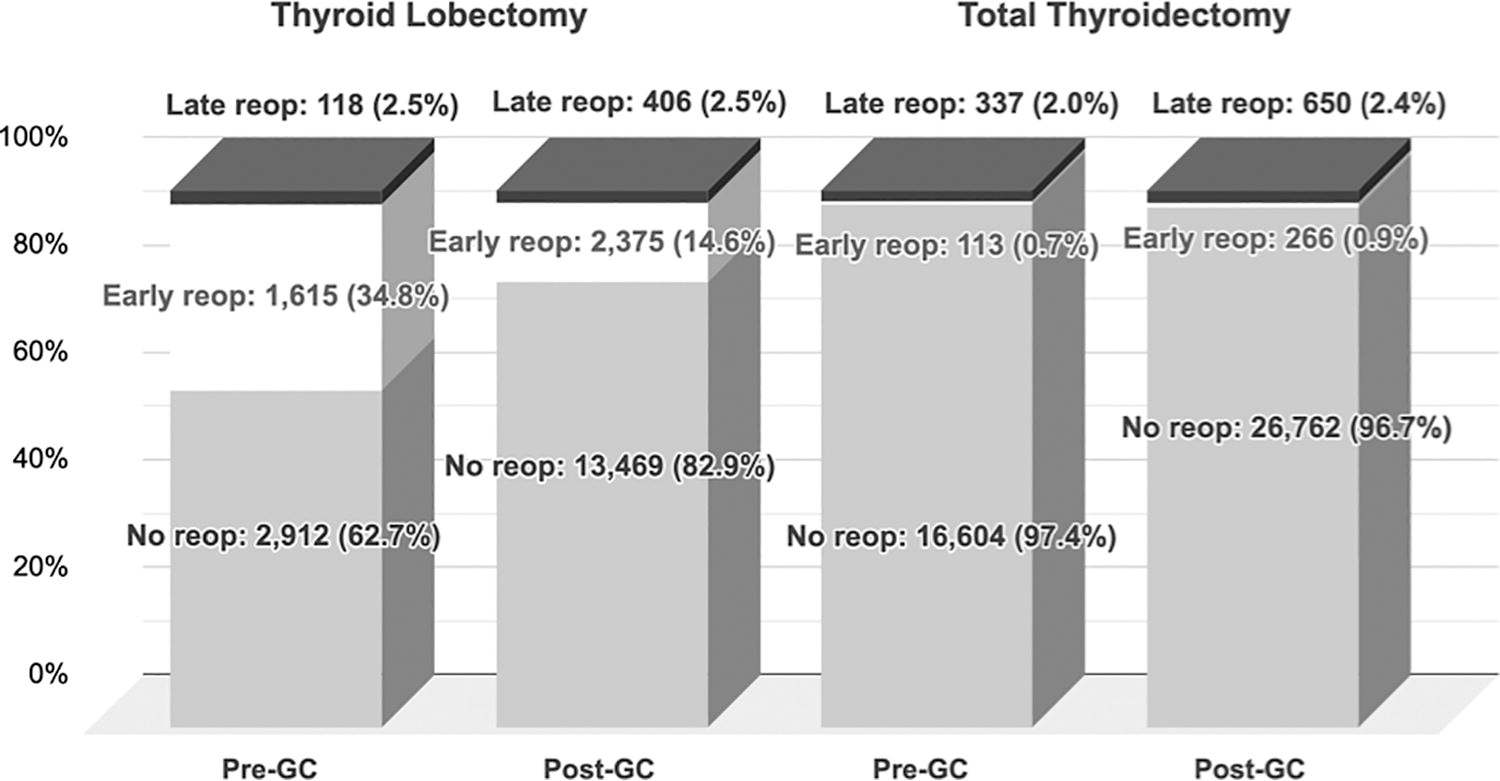
Reoperation rates by timing of reoperation. “Pre-GC” is defined as the preguideline change period (2013–2015) and “post-GC” is defined as the postguideline change period (2016–2021). Early reoperations are defined as those occurring within 180 days of the index operation, and late reoperations are defined as those occurring more than 180 days after the index operation. GC, guideline change.
The type of reoperation differed in patients undergoing lobectomy compared with TT. RTS constituted the majority of reoperations after lobectomy whereas NDs were the most common type of reoperation performed after TT. Among early reoperations after TL, RTS decreased from 33.9% of cases to 14.2% post-GC (p < 0.001, Table 2). The late RTS rate declined from 2.0% to 1.7% post-GC (p = 0.04), indicating that most completion thyroidectomies were done in the first six months after the initial operation.
Reoperations by Type of Index Operation and Guideline Period
“Pre-GC” is defined as the preguideline change period (2013–2015), and “Post-GC” is defined as the postguideline change period (2016–2021). Days to reoperation are calculated as median values within each cohort. Percentages are calculated as percent of total cases performed in each period.
GC, guideline change; ND, neck dissection; RTS, reoperative thyroid surgery.
Case volumes at LVCs, MVCs, and HVCs were also examined (Table 3). LVCs, which performed a median of 14 cases annually (interquartile range [IQR] = 6–27), constituted 57.7% of facilities and accounted for 12.4% of all operations for malignant disease, whereas HVCs, performing a median of 234 cases annually (IQR 142–503), accounted for 17.1% of facilities and 57.6% of operations. Operations for malignancy constituted 32.7% of cases at LVCs, 34.7% of cases at MVCs, and 36.5% of cases at HVCs.
Facilities by Operative Volume, 2013–2021
Low-, medium-, and high-volume categories are calculated based on the average annual case volumes of combined TLs and TTs performed for any indication. Annual case volume is provided as the median value within each facility type.
Reoperation trends were similar across hospitals of different operative volume (Table 4). While all hospitals experienced a decline in early reoperations after lobectomy, HVCs saw the largest declines (from 17.4% to 9.0%, p < 0.001), followed by MVCs (from 11.8% to 3.9%, p < 0.001) and LVCs (from 5.5% to 1.8%, p < 0.001). Late reoperations for both TT and TL changed by <0.5% regardless of hospital volume, and were not significantly different after the release of the 2015 ATA guidelines.
Reoperations by Hospital Volume and Guideline Period
“Pre-GC” is defined as the preguideline change period (2013–2015), and “Post-GC” is defined as the postguideline change period (2016–2021). Percentages are calculated as percent of total cases performed in each period.
HVC, high-volume center; LVC, low-volume center; MVC, medium-volume center.
Annual trends by hospital volume
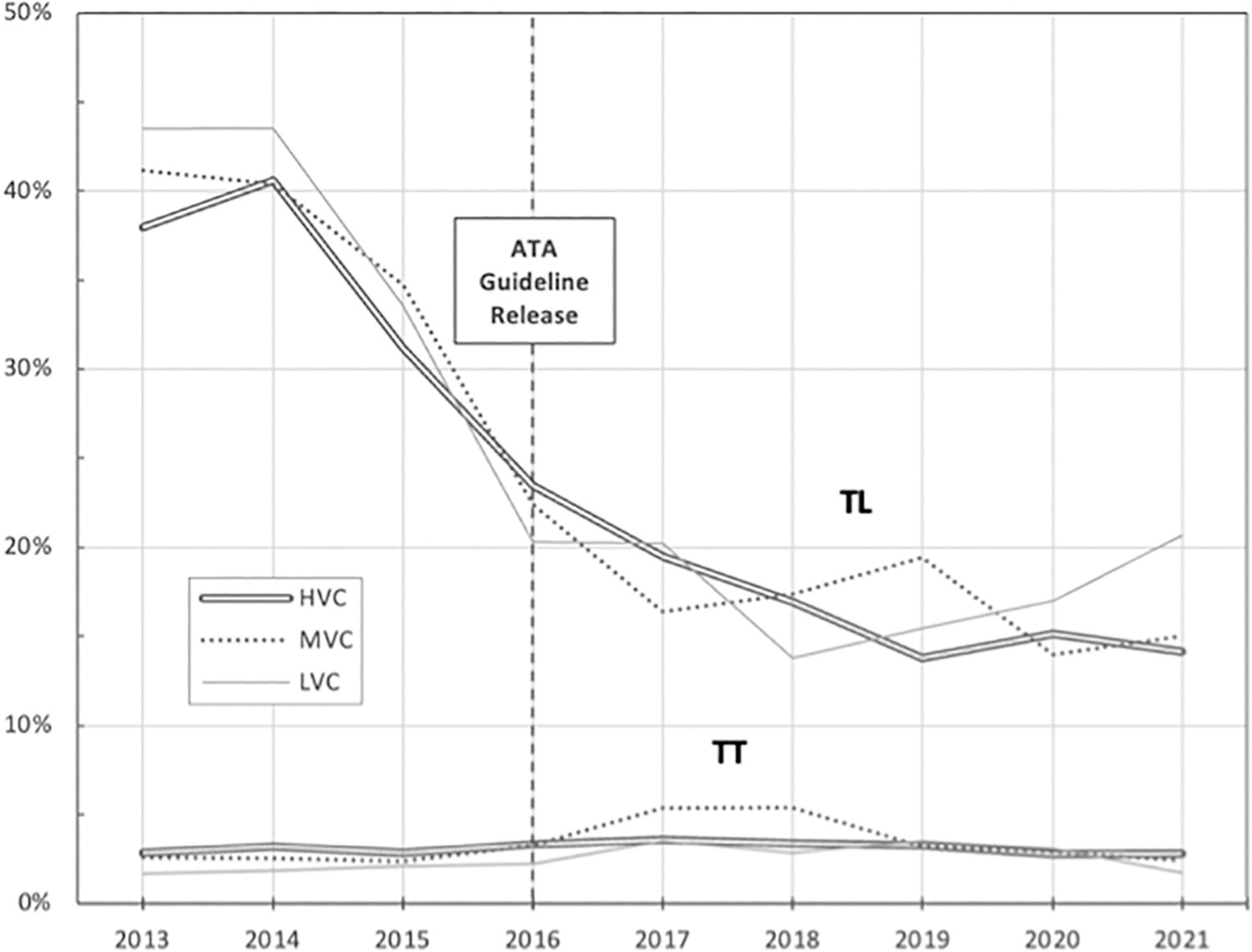
Use of TL at LVCs, MVCs, and HVCs increased each year of the study period, although year-over-year growth declined in later years (Fig. 4). At HVCs, lobectomy rates grew annually by 18.8% ([confidence interval (CI): 11.3−26.8%], p = 0.002) from 2013 to 2017, then by 6.4% ([CI: −0.3−13.6%, p = 0.06]) from 2017 to 2021 (periods are determined by the year in which the growth rate changed based on joinpoint analysis). At MVCs, use of lobectomy increased annually by 15.1% ([CI: 9.3−21.1%], p = 0.002) from 2013 to 2017 and 4.9% ([CI: −0.3−10.4%], p = 0.06]) from 2017 to 2021. At LVCs, use of TL increased annually by 14.3% ([CI: 8.7−20.2%], p = 0.002) from 2013 to 2017 and 2.7% ([CI: −2.4−8.0%], p = 0.22) from 2017 to 2021. HVCs had the highest rate of growth of TL compared with MVCs and LVCs (both p < 0.05).
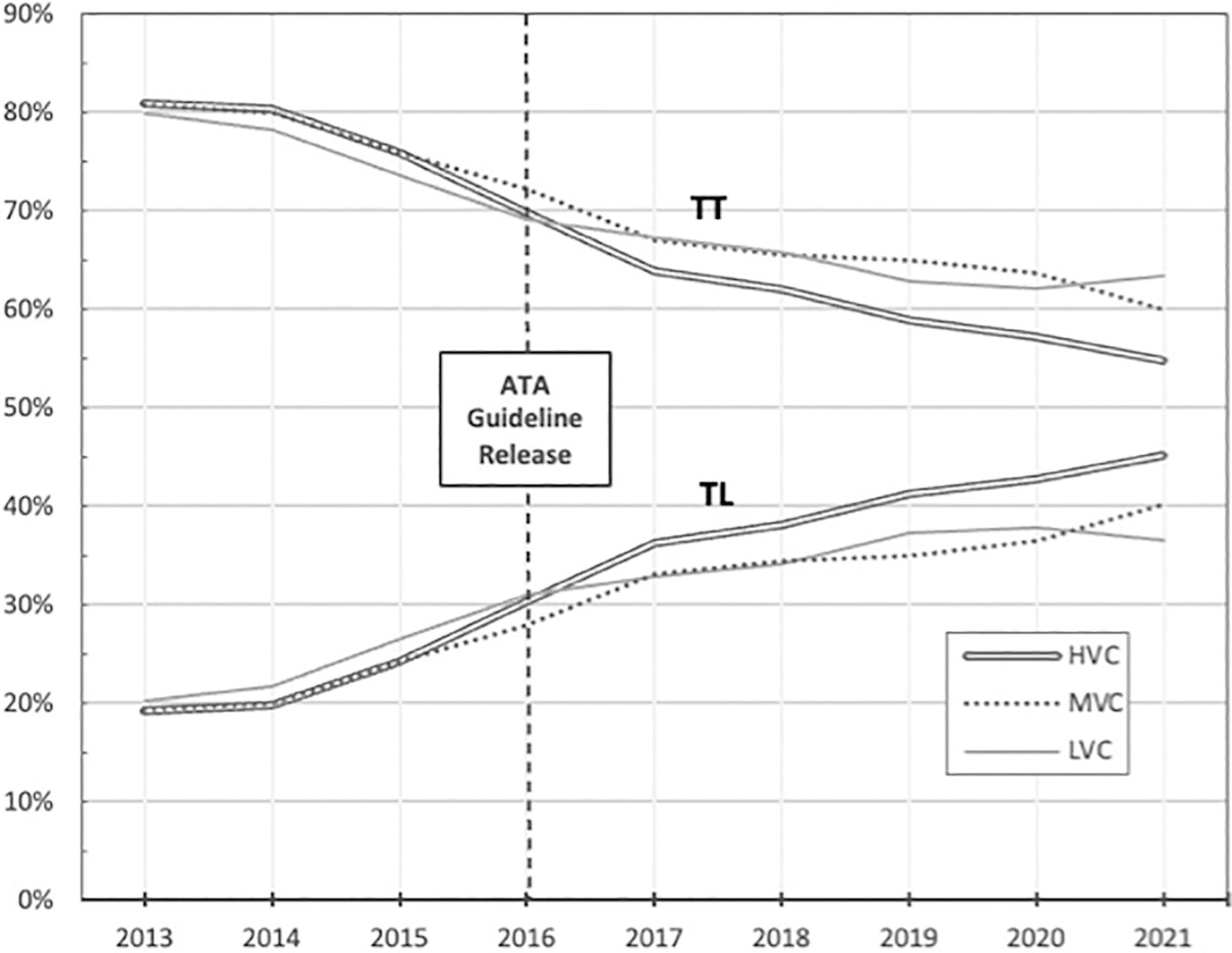
Annual TT and TL rates by hospital volume for HVCs, MVCs, and LVCs. HVC, high-volume center; LVC, low-volume center; MVC, medium-volume center.
Annual reoperation trends by hospital volume are depicted in Figure 5. TL-associated reoperations performed at HVCs declined annually by an average of 12.6% ([CI: 5.6−19.0%], p = 0.001) over the study period. At MVCs, lobectomy-associated reoperations declined at an annual rate of 13.4% ([CI: 8.5−18.1%], p < 0.001). At LVCs, they declined annually by 10.8% ([CI: 2.7−18.1%], p = 0.01). Trends in annual percent change were similar across all three types of facilities ([HVC vs. MVC] p = 0.44, [HVC vs. LVC] p = 0.08, [MVC vs. LVC] p = 0.36). There were no significant overall changes in TT reoperation rates across centers.
Annual reoperation rates by hospital volume for HVCs and LVCs.
On Cox multiple regression, two factors were associated with an increased risk of late reoperation in the post-GC period: uninsured status (HR = 1.84, [CI: 1.06−3.20], p = 0.03) and undergoing initial operation in more recent years, i.e., later in the time period analyzed (HR = 1.30, [CI: 1.24−1.36], p < 0.001) (Table 5). The choice of initial lobectomy instead of TT, however, was not predictive of late reoperation (HR = 1.05, [CI: 0.92−1.20], p = 0.47). No factors investigated were associated with a decreased risk of late reoperation.
Cox Regression of Factors That Are Associated with Late Reoperation in the Postguideline Change Period (2016–2021)
CI, confidence interval.
Discussion
This is the first study to examine patient-specific reoperations at the national level to evaluate how clinical practice patterns and reoperation rates have shifted since publication of the 2015 ATA guidelines. Our findings are congruent with those of earlier studies that reported an increasing use of TL for the surgical management of low-risk DTC. 13,21,22 We add further to the discussion by investigating whether reoperation rates have increased due to the more liberal use of TL, and examine these trends by center operative volume. In this national cohort, we found similar late reoperation rates between patients who underwent TT and those who underwent TL despite a steady rise in lobectomy volumes. Moreover, this trend was consistent across centers of differing operative volumes.
The initial concerns of disease recurrence raised by critics of the 2015 ATA GC were backed by several large retrospective studies that reported higher rates of locoregional recurrence with lobectomy. 3 In this study, we found a 58% decline in early reoperations in the post-GC period. Much of this decline is likely due to the liberalization of criteria necessitating complete resection as well as decreased use of radioactive iodine treatment, thus allowing for low-risk tumors up to 4 cm in diameter to be managed with lobectomy. Recent advancements in imaging and molecular testing may have also improved the preoperative risk stratification of patients, 23 –25 further reducing the number of patients with intraoperative findings that lead to upstaging of disease.
In this study, the choice of initial lobectomy was not an independent predictor of reoperation, but undergoing initial operation in more recent years was associated with a 30% increased likelihood of reoperation. This finding may be driven by the declining use of prophylactic central ND and radioactive iodine in recent years, which may result in increased recurrences. Similarly, with fewer total thyroidectomies being performed for low-risk cancers, a greater proportion of the patients who undergo a total resection may be those presenting at more advanced stages, with an inherently higher risk of both residual and recurrent disease.
In regards to hospital volume, lobectomy adoption rates at both HVCs and LVCs have increased, albeit at a significantly faster rate among HVCs (12.5% vs. 8.3% at LVCs). Using a statewide private payor database in Michigan, Ellsworth et al. reported similar percentage increases in the lobectomy rate among high- and low-volume surgeons (4% vs. 5%, respectively) after the GC with no difference in the rate of reoperation for completion thyroidectomy. 26 This study’s findings suggest that similar trends may be occurring at the national level.
While the majority of thyroidectomies in the United States are performed at LVCs, 27 a significant proportion of the literature on TL adoption has come from large, academic tertiary centers where practice patterns may not be reflective of broader trends. 28 –30 Additionally, it has been suggested that lower-volume surgeons are less likely to be aware of the ATA guidelines and less likely to recommend lobectomy over TT for low-risk DTC. 15 Our findings suggest that surgeons at HVCs, MVCs, and LVCs have increasingly performed lobectomy, with adoption accelerating in the years preceding and immediately following the GC (2013–2017).
Concurrently, postlobectomy reoperation rates at both HVCs and LVCs declined over the study period, although initially more rapidly at LVCs (rate of change = 22.0% from 2013 to 2018 vs. 16.9% from 2013 to 2019). Facility operative volume was also not found to be predictive of reoperation after the GC. Postoperative outcomes have been shown to be superior at HVCs due in part to higher levels of technical experience and greater availability of resources. 31,32 If LVCs where such resources may be more limited are not encountering increased reoperation rates, it is possible that less aggressive surgical intervention may be safe, although further studies are needed to test this hypothesis.
A limitation of this study is the lack of tumor stage and histopathologic data to confirm (1) that all included cases would have been eligible for either lobectomy or TT under the 2015 guideline criteria or (2) the actual indications for reoperation. Despite this limitation, our estimated late reoperation rates of 2.0−2.6%, suggestive of disease recurrence, are comparable with figures provided in other studies where patient tumor and histological characteristics were known: in a meta-analysis of nine large database studies comprising almost 14,000 patients, Schaap et al. calculated a recurrence rate of 2.3% after TT and 2.8% after lobectomy. 33
Several factors present in this study may have led to an underestimation of reoperation rates. No cutoff period was set for capturing reoperations data; as such, the follow-up time for reoperations ranged from 2 to 10 years, with each subsequent year having a shorter follow-up. However, sensitivity analysis performed by analyzing only the first three years of the study period and the last three years revealed similar findings, suggesting to us that this limitation does not have a statistically significant effect. The impact of lower operative volumes seen during the peak of the COVID pandemic may also have affected operative volumes. 34 –36 Additionally, the database is restricted to reoperations that were performed within the same center or hospital network; any reoperations performed at outside facilities, including other participating centers within the Vizient Clinical Data Base, are thus not captured. Finally, as this analysis is based on claims data, individual follow-up is not available.
Conclusion
Patients undergoing initial TT or TL for a diagnosis of thyroid cancer had no significant difference in the late reoperation rate after publication of the 2015 ATA guidelines. This study’s findings suggest that undergoing TL was not associated with an increased risk of reoperation when compared with TT, even at LVCs. However, research from data sets with more detailed clinical and pathological information is needed to confirm these findings.
The 2015 ATA guidelines adopted a neutral stance between the choice of TL and TT for low-risk DTCs. Since its publication, across the United States, patients with thyroid cancer may be receiving less aggressive guideline-concordant care without incurring an increased risk of reoperation.
Footnotes
Authors’ Contributions
M.K. designed the study, analyzed the data, and wrote the article. A.M. provided significant assistance with data acquisition and analysis, and additionally reviewed and made edits to the article. J.C.C. and A.M.L. contributed to the study’s design, methods, and review of the existing relevant literature; they additionally reviewed and edited the article. T.B. conceived the study, provided critical feedback, and made edits to the article.
Author Disclosure Statement
The authors have no relevant conflicts of a personal or financial nature to disclose.
Funding Information
No funding was provided for the specific creation of this article.
Supplementary Material
Supplementary Table S1