
Abstract

Dear Editor:
Alterations in the rearranged during transfection (RET) gene are causative of several types of cancer. 1 Recently, selective inhibitors of RET (RETi) selpercatinib and pralsetinib have been successfully developed as a treatment for cancer harboring RET activating mutations and rearrangements. 2 Regardless of prior treatment with standard therapy of vandetanib or cabozantinib or first-line use, selpercatinib and pralsetinib demonstrated an excellent effectiveness and a favorable safety profile in patients with RET mutant medullary thyroid cancer (MTC) in phase I/II clinical trials, 3,4 which led to the approval of selpercatinib in Europe and the United States. In first line, a phase III clinical trial found selpercatinib compared with standard therapy to result in longer progression-free survival, treatment failure free survival, and higher objective response rate in patients with RET-mutant-naive MTC. 5 Similarly convincing activity was demonstrated in patients with radioiodine refractory differentiated thyroid cancer (TC) carrying RET-gene fusions. 3 Beyond its anticancer effect, selpercatinib has shown an excellent safety profile compared with those of the multikinase inhibitors (MKIs) used in clinical practice. 6 Indeed, most of the treatment-related adverse events (TRAEs) are of grade 1–2, according to the Common Terminology Criteria for Adverse Events, leading to a low-dose reduction rate and an even lower dose discontinuation rate, thus potentially enhancing the drug effect. Conceivably, TRAEs that were not observed in clinical trials have emerged after approval with longer time of treatment. Weight gain and chylous effusions have been recently described. 7,8
Sexual function is an important element of quality of life and frequently impaired in patients with cancer, especially if fatigue, depression, pain, or therapy-related anxiety coexist. 9
In male patients, this can lead to erectile dysfunction (ED), which may result from the previously mentioned conditions, or be specifically caused by certain medications. The investigators authoring this study independently observed males reporting ED shortly after the initiation of selpercatinib treatment for advanced TC.
Here, we systematically investigated ED related to selpercatinib treatment in a multicenter retrospective cohort study. The primary aim was to evaluate the prevalence of ED in patients treated with selpercatinib for advanced TC outside of clinical trials (i.e., in a Named Patient Programme or after approval) or within the LIBRETTO-201 Expanded Access Program (ClinicalTrials.gov NCT03906331). We also examined the management of ED in affected patients. Patient data were retrospectively collected at individual centers and anonymized. Patients were grouped according to whether ED was specifically investigated by physicians or spontaneously reported by patients. The study was approved by the ethics committee at the University of Würzburg, Germany (approval number 20221220-01) and was completed in accordance with the Declaration of Helsinki as revised in 2013.
From a database of 49 male patients with TC treated with selpercatinib, we evaluated 25 male patients for whom information about ED was spontaneously referred or specifically asked. Overall, 23 (92%) patients had MTC and 2 patients (8%) papillary thyroid carcinoma (Table 1).
Epidemiological, Pathological, and Clinical Data of the Study Cohort (n = 25)
ECOG, Eastern Cooperative Oncology Group; ED, erectile dysfunction; IQR, interquartile range; MTC, medullary thyroid carcinoma; PTC, papillary thyroid carcinoma.
Fourteen out of 25 patients (56%) had received other systemic therapies before starting selpercatinib treatment (Table 1).
Overall, 23/25 (92%) male patients reported ED. Five out of 23 (21.7%) had ED before starting selpercatinib, one of whom had a diagnosis of hypogonadism and was on testosterone replacement therapy, and another one had received radiotherapy of the pelvis before treatment with selpercatinib. Conversely, 18/20 (90%) patients, who had unimpaired sexual function before selpercatinib, reported experiencing ED during the treatment with selpercatinib (Fig. 1, panel A).
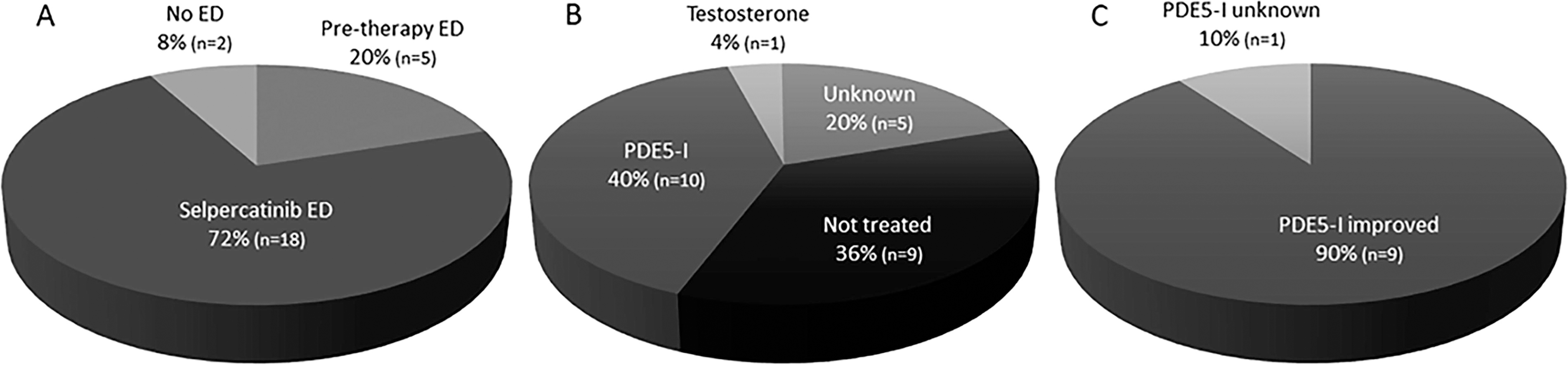
Prevalence of erectile disfunction (ED) in the study cohort
The prevalence of ED was higher when the treating physician asked about sexual dysfunction, particularly ED. Only 2/18 (11.1%) patients in our cohort spontaneously reported ED, while 16/18 (88.9%) patients, although they had already developed ED, reported it only after specific questioning (Table 1). Concomitant diseases and drugs potentially influencing ED in the study population are reported in Table 1. ED, regardless of whether ED occurred before or after the commencing selpercatinib, was managed according to local standard of care during follow-up (Fig. 1, panel B). In patients for whom specific treatment of ED with phosphodiesterase-5 inhibitors (PDE-5i) was started, improvement of ED was reported in 9/10 (90%) treated cases (Fig. 1, panel C). This improvement was independent of whether selpercatinib was started as first or second/third-line treatment. In 6/18 patients (33%) who experienced ED during selpercatinib treatment, serum LH, FSH, and testosterone were evaluated before and during the treatment, and none of the patients had hypogonadism before starting treatment. However, as gonadal hormones during selpercatinib treatment were not routinely evaluated by the treating physicians, emergent hypogonadism in some patients cannot be excluded.
To our knowledge, this is the first report that specifically addresses ED in patients with RET-altered TC treated with selpercatinib. We found a relatively high proportion of patients who developed ED after starting selpercatinib. Our findings contrast with the data of LIBRETTO-531 clinical trial 5 where ED was reported in 12/115 (10.6%) male patients treated with selpercatinib and in none of the patients treated with cabozantinib or vandetanib. Our results also contrast with the ARROW clinical trial 4 where ED was reported in 10/142 (7%) male patients treated with pralsetinib. The significantly higher prevalence of ED rate in our cohort may be multifactorial. First, patients were specifically questioned for the presence of sexual dysfunction in most centers. It is known that ED is frequently underreported to treating physicians. 10 The high proportion of symptomatic patients may be related to increased awareness of treating physicians at specialist endocrine tumor centers. Second, at variance to the LIBRETTO-531 trial, most of our patients were pretreated with MKIs. This may have caused endothelial dysfunction and increased the likelihood of ED. 11 Our observation of frequent ED is relevant in considering the quality of life of these patients. Recognizing and treating ED may enhance sexual well-being, particularly in a type of cancer that often remains responsive to treatment for many years. Control of tumor-related symptoms on selpercatinib is frequently rapid, durable, and quality of life is good with infrequent and mild TRAEs. 5 Hence, sexual dysfunction is a relevant concern for patients treated for advanced TC with selpercatinib.
We raise three main hypotheses for the pathogenesis of ED on selpercatinib. First, hypothalamic–pituitary–gonadal (HPG) axis may be impaired and lead to hypogonadism during the treatment. The marked improvement of ED after treatment with PDE-5i in our patients cannot exclude the presence of hypogonadism a priori, because more than 70% of patients, also in the presence of low blood testosterone levels, respond to PDE-5i. 12,13 Second, a direct vascular impact of selpercatinib may cause ED. It is worth noting that most of our patients already had received antiangiogenic drugs as first/second line for the treatment of advanced TC, thus potentially impairing for their mechanisms of action against vascular endothelial growth factor receptor, the vascular endothelium. Lastly, glial cell-derived neurotrophic factor (GDNF) is a neurotrophin that, in concert with other neurotrophins, has demonstrated the capability to restore erectile function in animal models of ED by either providing neuroprotection or promoting neural regeneration of the cavernous nerve. 14 GDNF is also implicated in the spermatogenesis. 15 Of note, GDNF signaling is mediated by the activation of the RET receptor tyrosine kinase. 16 Therefore, in patients who are treated with RETi, a decreased action of GDNF leading to potential impairment in the nerves trophism should be considered.
Both selpercatinib and PDE-5i are mainly metabolized through the hepatic isoenzyme cytochrome P450 (CYP) 3A4 pathway. 17 However, it is important to note that in all cases of ED treated with PDE-5i, no reduction in selpercatinib dose was recorded. It follows that only drugs with a moderate-to-strong inhibition or induction of CYP3A4 should affect selpercatinib dose modifications, and PDE-5i are not included in this group. 18
Specific studies about the pathogenesis of ED in patients treated with selpercatinib are desirable. In particular, prospective clinical trials on selective RET inhibitors should systematically assess ED and explore optimal management strategies. Furthermore, biochemical evaluation of the HPG axis and doppler ultrasound of penile arteries should become part of clinical routine in patients treated with selective RET inhibitors who report ED.
In conclusion, our report showed that a high prevalence rate of patients with RET-altered TC treated with selpercatinib. In this preliminary observational study, PDE-5i treatment appeared to improve ED in some patients, which may imply that this Adverse Event (AE) can be manageable. Further prospective studies with a larger number of patients are needed to confirm our preliminary observations.
Footnotes
Acknowledgment
The authors would like to thank Eli Lilly and Company for reviewing this study.
Authors’ Contributions
A.M.: Conceptualization (lead); methodology (lead); data collection and analysis (lead); writing—original draft (lead); writing—reviewing and editing (lead). M.K.: Conceptualization (lead); methodology (lead); data collection and analysis (lead); writing—original draft (lead); writing—reviewing and editing (lead). M.L.G.: Data collection and analysis (lead); writing—original draft (supporting); writing—reviewing and editing (supporting). S.H.: Data collection and analysis (lead); writing—original draft (supporting); writing—reviewing and editing (supporting). C.M.S.: data collection and analysis (lead); writing—original draft (supporting); writing—reviewing and editing (supporting). R.S.: Data collection and analysis (lead); writing—original draft (supporting); writing—reviewing and editing (supporting). C.G.: Data collection and analysis (lead); writing—original draft (supporting); writing—reviewing and editing (supporting). A.P.: Data collection and analysis (lead); writing—original draft (supporting); writing—reviewing and editing (supporting). M.I.H.: Data collection and analysis (supporting); writing—original draft (supporting); writing—reviewing and editing (lead). B.G.R.: Data collection and analysis (lead); writing—original draft (supporting); writing—reviewing and editing (supporting). R.E.. Conceptualization (lead); methodology (lead); data collection and analysis (supporting); writing—original draft (supporting); writing—reviewing and editing (lead).
Author Disclosure Statement
A.M. is consultant for Eli Lilly and investigator for clinical trials of Eli Lilly. M.K. received research funding, speaker honoraria, reimbursement of travel costs and consultancy fees from Eli Lilly, research funding from Ipsen, speaker honoraria and travel costs from Sanofi, and consultancy fees from Roche, Eisai, and Bayer and is principal investigator (PI) for clinical trials of Eli Lilly. B.G.R. is an advisor to Eisai, Exelixis, and Eli Lilly and investigator for Eli Lilly and Exelixis. M.I.H. is in the steering committee and site PI for clinical trials of Eli Lilly. R.E. is a consultant for EISAI, Eli Lilly, Ipsen, and Bayer and is PI for clinical trials of Eli Lilly. M.L.G., S.H., C.M.S., R.S., C.G., and A.P. have nothing to disclose.
Funding Information
No funding was received in general and from the sponsor for conducting this study and for the maintenance of the database from which data were collected.