
Abstract
Background:
Iodinated contrast is commonly used for radiological procedures, with one dose delivering several hundred-fold the daily requirements needed for normal thyroid hormone production. Risks of excess iodine include incident thyroid dysfunction, which is associated with adverse cardiac outcomes, yet there are no prospective studies investigating the changes in cardiac physiology following iodine contrast administration. This study was conducted to investigate the longitudinal relationships between the amount of iodinated contrast administration and changes in cardiac electrophysiology and structure.
Methods:
A longitudinal cohort study was conducted with prospectively enrolled participants who received iodine contrast for elective computed tomography or coronary angiography. Serum thyroid function tests, electrocardiograms (EKG), and transthoracic echocardiograms were obtained serially until 36 months. Trends of electrical and structural cardiac changes following iodine contrast administration were assessed using mixed effect models.
Results:
The cohort was composed of 129 patients (median age, 70 [interquartile range: 63, 75] years; 98% male). Larger amounts of iodine exposure were associated with increases in QRS and QTc durations and decreased ejection fraction (EF), and these associations were still observed for follow-up EF after additionally adjusting for baseline values (the high-iodine contrast group vs. the low-iodine contrast group, −4.23% [confidence interval, −7.66% to −0.79%]). Dose–response analyses also showed lower EF with larger amounts of iodine received; these trends were not significant for the EKG parameters studied.
Conclusions:
Over a period of up to 36 months, a larger amount of administered iodine contrast was associated with lower EF among participants. Further investigation is needed to elucidate the long-term trends of electrical and structural cardiac function after iodine contrast administration.
Introduction
Iodine is a micronutrient that is crucial for the production of thyroid hormone. Iodinated contrast is a common source of excess iodine in health care settings, with over 120 million iodine-enhanced computed tomography (CT) scans alone performed per year worldwide. 1 A single dose of iodinated contrast media confers several hundred-fold more than the daily iodine requirements needed for normal thyroid hormone production. 2 In certain susceptible individuals, excess iodine exposure has the potential to result in incident thyroid dysfunction (i.e., hypo- or hyperthyroidism), due to the established physiological principles of failure to escape from the acute Wolff–Chaikoff effect and of the Jod–Basedow phenomenon, respectively. 3
Iodine status can be assessed only on a population level and not among individuals due to its day-to-day variability. 4 An epidemiological study of the National Health and Nutrition Examination Study has shown that excess iodine, as defined by median urinary iodine concentrations, in the general U.S. population is associated with increased mortality risk. 5 Underlying mechanisms may include thyroidal but potentially also non-thyroidal pathways, and there is evidence that high thyroid hormone levels even within the normal range are associated with increased risk of atrial fibrillation 6,7 and cardiovascular risk factors, including diabetes and dyslipidemia, 8 as well as less overt cardiac function abnormalities such as diastolic overload, myocardial necrosis, myocardial fibrosis, and decreased left atrial strain. 9 However, to date, the evidence based on a prospective cohort study design is lacking on this topic.
In order to investigate the risk of excess iodine exposure on cardiac disease, we therefore conducted a prospective cohort study analyzing the relationships between iodinated contrast administration and serial changes of electrocardiogram (EKG) and transthoracic echocardiogram (TTE) parameters over a period of up to 36 months.
Materials and Methods
Subject population and demographic data
Study approval was obtained by the Veterans Affairs (VA) Greater Los Angeles Healthcare Sytem Institutional Review Board [IRB] (IRB #1615962), and written informed consent was obtained from all participants. Subjects were prospectively enrolled at the West Los Angeles VA Medical Center from September 2020 to December 2022 and monitored until study termination in September 2023. Inclusion criteria were adults aged ≥18 years who were scheduled for an elective CT scan or coronary angiography for a clinical indication that required iodinated contrast. Exclusion criteria were (1) history of other iodinated contrast radiologic study within 6 months; (2) previous history of or current thyroid dysfunction (hypo- or hyperthyroidism); (3) history of thyroid surgery, thyroid cancer, or radioactive iodine treatment; (4) current use of thyroid hormone or antithyroid drug therapy; (5) use of amiodarone within two years; (6) use of lithium or interferon-α within 6 months; (7) current pregnancy or lactation; or (8) use of hormonal contraceptive therapy.
Demographic data were obtained of participants’ age, sex, race, ethnicity, place of birth, medication use, cigarette smoking history, and comorbidities (diabetes, dyslipidemia). Baseline measurements (obtained up to 1 month before iodinated contrast administration) included serum thyroid function tests (thyrotropin [TSH], free thyroxine [FT4], and total triiodothyronine [TT3]), EKG, and TTE. Follow-up serial monitoring was performed at 1, 3, 6 months and then every 6 months thereafter until 36 months. Participants were asked to visit the outpatient research unit for these follow-up monitoring visits and included in the final analysis if they had at least one follow-up cardiac study measurement (EKG and/or TTE) after their baseline assessment.
The sample size was calculated for our previous study 10 assessing the impact of iodine contrast administration on thyroid function 11 We include 133 participants in this cohort. As 4 patients did not return for follow-up study visits after their enrollment, there were 129 participants included in our final analysis, from whom all had follow-up EKG data (totaling 490 EKGs), and 71 patients had follow-up TTE data (totaling 216 TTEs) (Fig. 1).
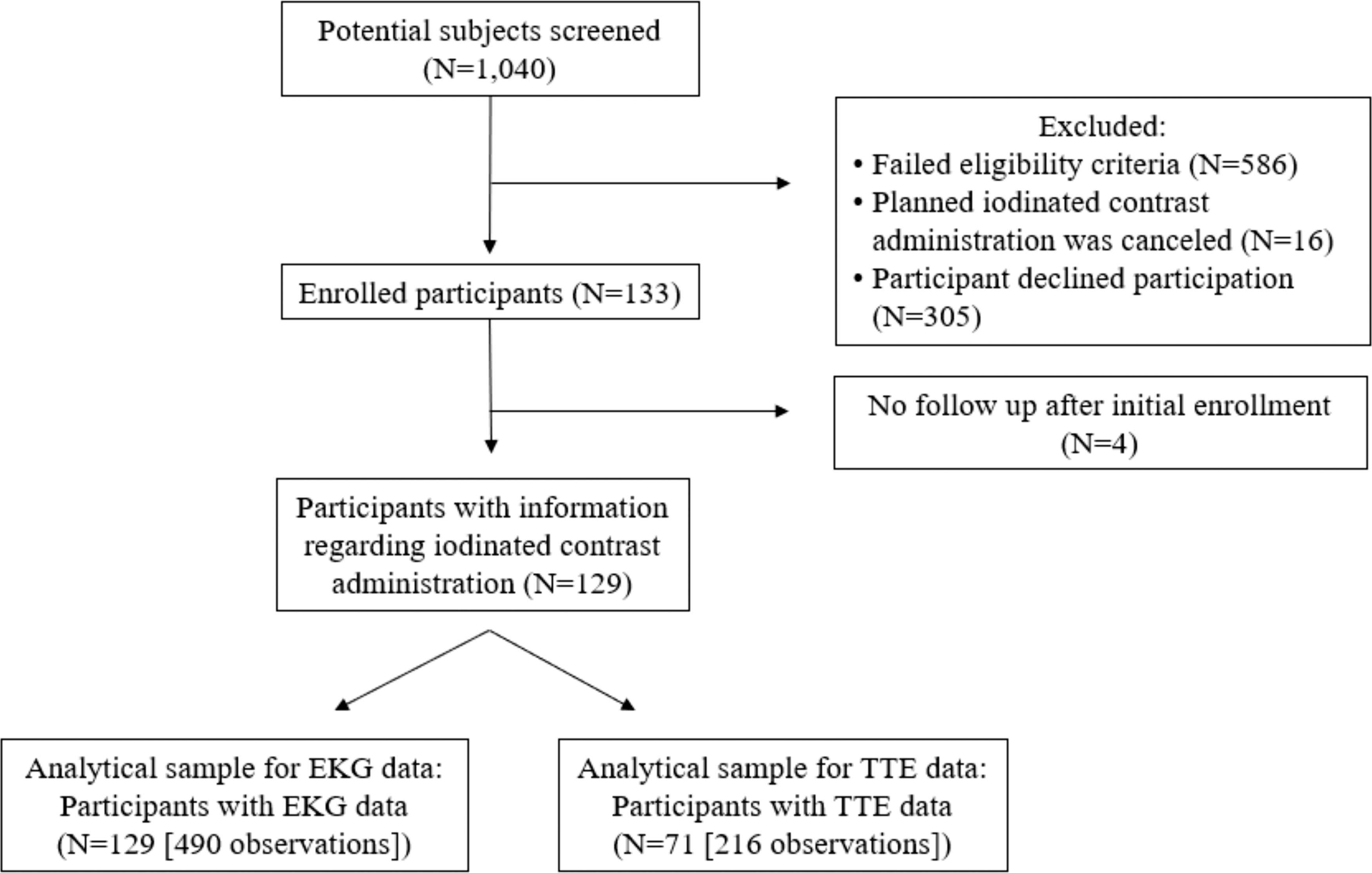
Flow of study sample selection.
Exposure ascertainment
The formulation, brand, and volume of iodinated contrast used for participants’ radiological procedures were recorded. The amount of iodine administered was calculated as the product of the volume of the iodine contrast received (mL) and each formulation’s concentration of iodine according to the manufacturer’s labeling. All participants were administered iodinated contrast as one of two iodixanol formulations (Visipaque 270 or Visipaque 320), which is a nonionic, dimeric, and water-soluble contrast media containing 270 and 320 mg of iodine per milliliter, respectively.
Outcome ascertainment
The primary endpoints were changes in cardiac parameters captured by the serial EKGs and TTEs obtained following iodinated contrast administration. EKG parameters included ventricular rate, PR interval, QRS duration, and QTc intervals. Serial TTEs were analyzed for calculated ejection fraction (EF) using Simpson’s method. All EKGs and TTEs were performed by trained, certified technicians and read by experienced cardiologists, and angiograms were performed by experienced interventional cardiologists, in accordance with our usual hospital standards of care.
Statistical analyses
The descriptive data are presented as mean ± standard deviation (SD) or median with range as appropriate. Mixed effects models were used to assess changes in EKG and TTE parameters by iodine contrast administration (per 100 mL) during the follow-up period for each subject. In Model 1, we included age, sex, race, ethnicity, cigarette smoking status, comorbidities (i.e., diabetes and dyslipidemia), and baseline thyroid function tests (i.e., serum TSH, FT4, and TT3 levels) and the interaction term between iodine contrast administration and follow-up time in months. In Model 2, we additionally included the baseline values of the outcome in each model (i.e., PR interval, QRS duration, QTc duration, or EF) and type of radiologic examination (i.e., CT or coronary angiography). We also ran the same model using binary exposure (low vs. high) defined as either below or above the median amount of iodine contrast received (62 mL). Lastly, the dose–response relationships between iodine contrast administration and EKG or TTE parameters were investigated by using restricted cubic spline models fitted for mixed effects models with three knots at 10th, 50th, and 90th percentile of the amount of iodine contrast received. As an additional analysis, we calculated the number of participants who showed thyroid dysfunction (either hyperthyroidism or hypothyroidism) during the follow-up in the high-iodine contrast group and the low-iodine contrast group, respectively. All statistical analyses were performed using STATA version 18. Missing values were handled as an indicator variable in the regression models. p-Values of <0.05 were considered statistically significant.
Results
The baseline participants’ characteristics are shown in Table 1. The median age was 70 (interquartile range: 63, 75) years, and most were males (98.5%) and non-Hispanic (80.6%). The median serum TSH at baseline was 1.56 (interquartile range: 1.08, 2.33) mIU/L. Regarding the type of radiologic examination, 16 patients (12.4%) underwent CT scanning of a single location (i.e., neck, chest, heart, abdomen, pelvis, or urinary tract), 10 patients (7.8%) underwent CT scanning of multiple locations (i.e., abdomen/pelvis, chest/abdomen/pelvis, or neck/chest/abdomen/pelvis), and 103 patients (79.8%) underwent coronary angiography; among 71 patients with TTEs, 67 (94.4%) underwent coronary angiography. The median (interquartile range) amount of iodinated contrast administered was 62 (45, 90) mL among the overall study sample: 90 (90, 90) mL among participants who underwent CT scanning and 55 (44, 86) mL among those who underwent coronary angiography (CT scanning vs. coronary angiography, p-value <0.001; Supplementary Table S1). Participants were followed for a median duration of 11.3 months (interquartile range, 5.8–22.4 months).
Baseline Characteristics
EKG, electrocardiogram; FT4, free thyroxine; IQR, interquartile range; TSH, thyrotropin; TTE, transthoracic echocardiogram; TT3, total triiodothyronine.
During follow-up, seven patients (10.9%) were observed to have heart failure with reduced EF (defined by EF <40%) in the high-iodine contrast group, while four (6.2%) patients were observed to have heart failure with reduced EF in the low-iodine contrast group. Iodine contrast administration (per 100 mL) tended to be associated with changes in select EKG and TTE parameters during follow-up (QTc duration, +11.64 msec [confidence interval, CI, −0.69 to +23.96], p = 0.06; EF, −4.39% [CI, −8.87 to +0.09], p = 0.06) in Model 1 (Table 2). However, the associations were diminished after adjusting for the baseline values of these cardiac parameters in Model 2. When we dichotomized the amount of iodine contrast received, the high-iodine contrast group showed lower EF than the low-iodine contrast group, even after adjusting for the baseline EF (Model 1, −6.33% [CI, −11.88 to −0.77], p = 0.03; Model 2, −4.23% [CI, −7.66 to −0.79], p = 0.02) (Table 2). The results did not change when we excluded the patients who had undergone coronary angiography in the setting of a current myocardial infarction or heart failure (Supplementary Table S2).
Changes in Serial EKG and TTE Parameters Following Iodinated Contrast Administration
Mixed effect models were applied to assess the relationship between iodinated contrast administration and serial changes in EKG (PR interval, QRS duration, and QTc duration) and TTE (ejection fraction) parameters. Model 1 includes age, sex, race, ethnicity, cigarette smoking status, comorbidities (i.e., diabetes and dyslipidemia), and baseline serum thyroid function tests (i.e., serum TSH, FT4, and TT3 levels). Model 2 includes the baseline values of the outcome in each model (i.e., PR interval, QRS duration, QTc duration, or ejection fraction) and types of radiologic examinations (i.e., computed tomography or coronary angiography) in addition to the covariates in Model 1.
This pattern was supported by the longitudinal trends shown in Fig. 2. Dose–response analyses using a restricted cubic spline curve also showed lower EFs in those who had received higher amounts of iodine contrast while the trends plateaued when the amount exceeded approximately 75 mL (Fig. 3). We also observed some signals of shorter PR duration, longer QRS duration, and longer QTc durations with higher amounts of iodine received, but these were not significant. During the follow-up, 12 patients (18.8%) were noted to have developed thyroid dysfunction (4 hyperthyroidism and 8 hypothyroidism) in the high-iodine contrast group, while there were 5 patients (23.1%) who developed thyroid dysfunction (3 hyperthyroidism and 12 hypothyroidism) in the low-iodine contrast group (p = 0.55).
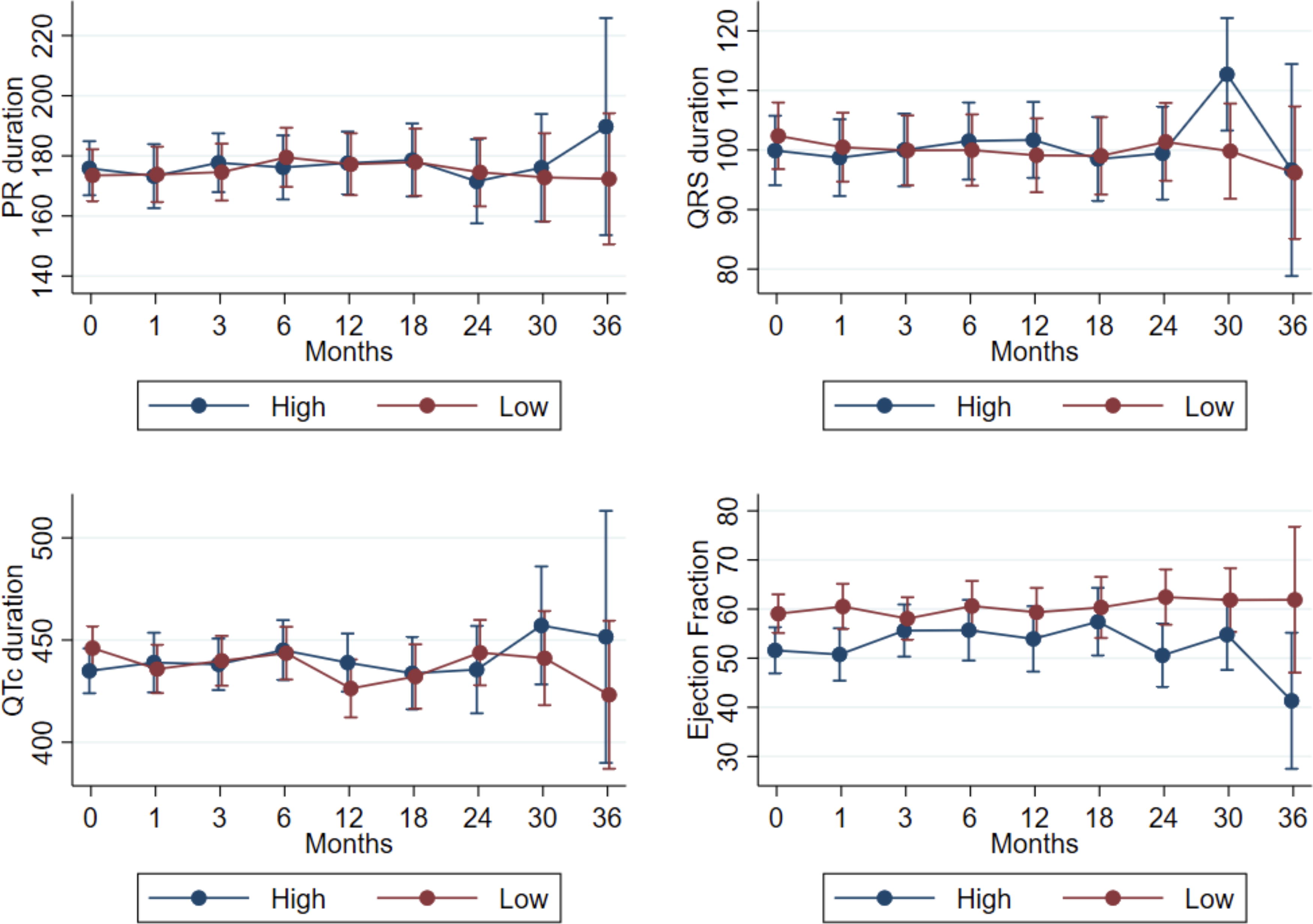
Longitudinal trends in EKG and TTE parameters following iodinated contrast administration. Mixed effect models were applied to assess the relationship between iodinated contrast administration (low [defined as ≤median] versus high [defined as >median]) and parameters of serial EKGs (PR interval, QRS duration, QTc duration) and TTEs (ejection fraction). Model includes age, sex, race, ethnicity, cigarette smoking status, comorbidities (i.e., diabetes and dyslipidemia), baseline thyroid function tests (i.e., serum TSH, FT4, and TT3 levels), and the interaction term between iodinated contrast administration and follow-up time in months. EKG, electrocardiogram; FT4, free thyroxine; TSH, thyrotropin; TT3, total triiodothyronine; TTE, transthoracic echocardiogram.
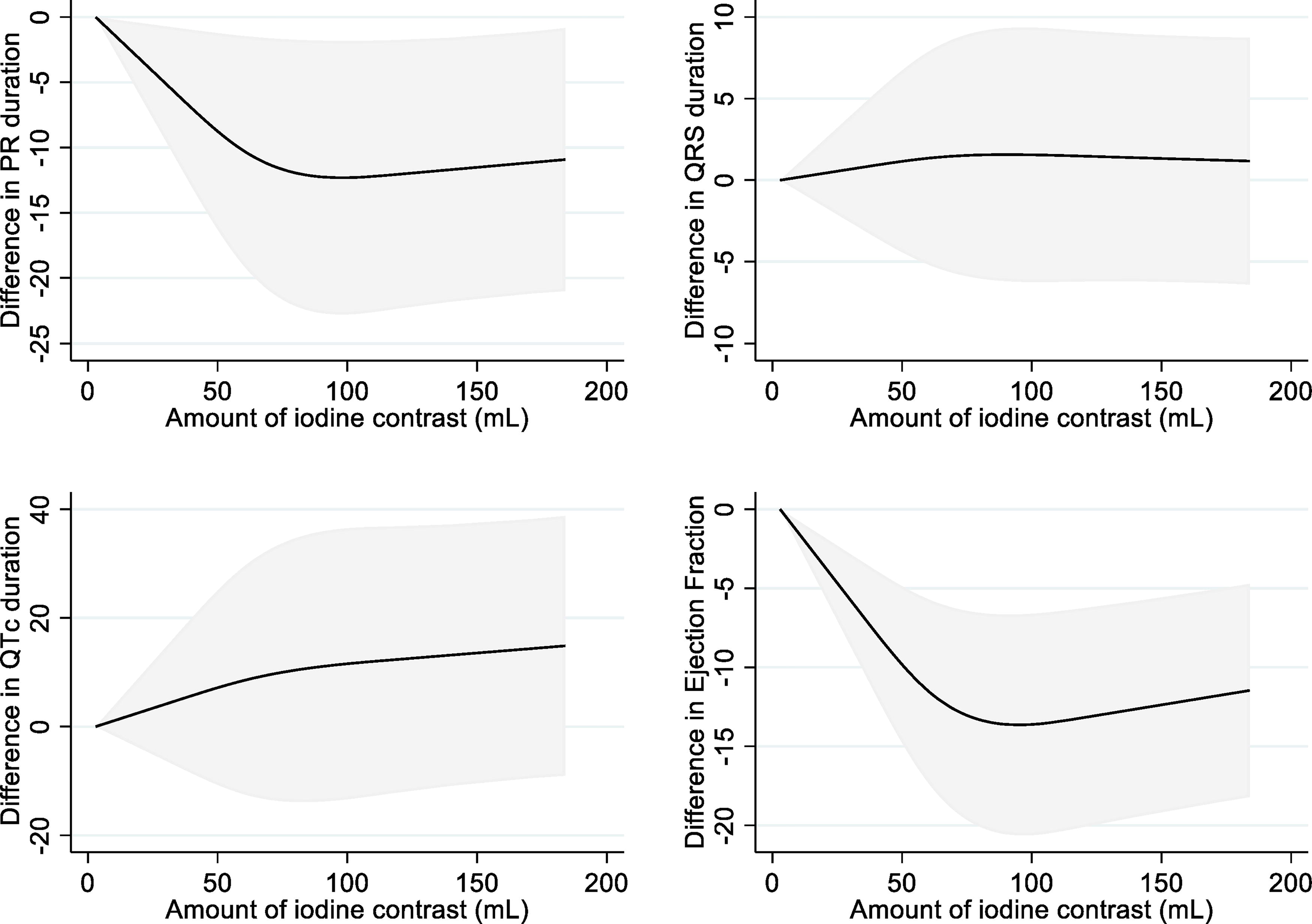
Dose–response relationships between iodinated contrast administration and serial longitudinal EKG and TTE parameters. Restricted cubic spline curve with three knots was applied to assess the dose–response relationship between the amount of iodinated contrast and parameters of serial EKGs (PR interval, QRS duration, QTc duration) and TTEs (ejection fraction). Mixed effect models include age, sex, race, ethnicity, cigarette smoking status, comorbidities (i.e., diabetes and 0dyslipidemia), baseline thyroid function tests (i.e., serum TSH, FT4, and TT3 levels), the baseline values of the outcome in each model (i.e., PR interval, QRS duration, QTc duration, or ejection fraction), and type of radiologic examinations (i.e., computed tomography or coronary angiography).
Discussion
This longitudinal cohort study of prospectively enrolled subjects is the first to investigate the relationships between iodinated contrast administration and changes of serial EKG and TTE parameters over long-term monitoring. The existing literature has primarily focused on kidney injury 12 and thyroid dysfunction following iodine contrast administration, 2 including recent data of the U.S. Food and Drug Administration adverse event reporting system that demonstrated increased risks of hypothyroidism and hyperthyroidism, particularly in those who had received the iodixanol formulation of iodine contrast, 13 the same iodinated formulation assessed in the current study. From serial assessments over a period of up to 36 months, a larger amount of iodine contrast administration was associated with lower EF evaluated by TTEs. In addition, there were some signals in select EKG parameters (longer QRS and QTc duration) with larger amounts of iodine received, although the associations were diminished after adjusting for the baseline values of these cardiac parameters. These patterns were also observed in dose–response analyses.
Potential mechanisms of our findings include changes in thyroid function after iodine contrast administration. Thyroid hormone has direct actions on the heart through both genomic and nongenomic pathways and plays an important role in regulation of the cardiac and peripheral vascular systems. 14,15 Thyroid dysfunction is a well-established risk factor for adverse cardiac outcomes, including heart failure, atrial fibrillation, and cause-specific and overall mortality. 16 –21 In retrospective cohort analyses of the U.S. Veterans Health Administration electronic health records, we reported that iodine contrast is associated with a 39% increased risk of incident thyroid dysfunction, 10 and there are increased further long-term risks of heart failure and atrial fibrillation in those found to have abnormal serum thyroid function after receipt of iodine contrast. 22,23 Furthermore, in the same prospective cohort used in the present study, we found that half of 20 subjects with subclinical hyper- or hypothyroidism (6 preexisting cases and 14 newly developed cases after iodine contrast administration) had persistently showed abnormal thyroid function during follow-up. 24 In addition, while the primary role of iodine is thyroid hormone production, it may have extrathyroidal functions 25 given the ability for the sodium/iodide symporter to be expressed in various non-thyroidal organs. 26,27 Although we did not find a statistical difference in the occurrence of thyroid dysfunction between the high-iodine contrast and the low-iodine contrast groups, the sample size was too small to scrutinize this potential mechanism. Further prospective studies with a larger sample size and detailed follow-up information on both thyroid and cardiac function are warranted.
The strengths of this study include the prospective nature of the study design, the capture of multiple repeated measurements from serial EKGs and TTEs performed by a limited set of technicians at the same hospital center (thereby reducing interobserver variability), and the availability of detailed electrical and structural cardiac data that would not be possible in a retrospective or cross-sectional study.
There are also several limitations in this study. First, the sample size is limited to a convenience sample of patients who received their usual clinical care from a single center—thus, an age- and sex-matched control group is not available—although this sample represents the largest such prospective study on the topic to date. Second, our findings may be skewed by confounding bias (e.g., confounding by indication) given that patients had a wide array of comorbidities and thus varied indications for receiving iodinated contrast; participants were not necessarily excluded if there were any active comorbid conditions, including chest pain. Additional comorbidities than those reported, as well as detailed cardiovascular history and the trend of renal function laboratory tests, were not ascertained. Third, not all participants were able to complete the planned schedule of study assessments, although all had follow-up EKG data and the majority had follow-up TTE data. Fourth, details regarding any percutaneous coronary intervention performed, which may be mitigator of EKG and TTE changes, following the administration of iodine contrast was not available. Fifth, since the sample size of this prospective cohort study was calculated for another study 10 and not for the present study, we did not have sufficient statistical power for some analyses; subgroup analyses were unable to be performed due to limitation of the sample size. Finally, it is possible that some participants may have received additional iodine contrast during the follow-up period, although any dose–response relationships observed would have biased the findings toward the null if so. The potential importance of multiple exposures (i.e., repeated iodinated contrast doses in a single individual), detailed information regarding the temporality and duration of an initial iodinated contrast dose risk, and the potential reversibility of these risk (i.e., through correction of any observed thyroid dysfunction) also deserve additional study in future investigations. It would also be important to perform subgroup analyses of these questions in participants with preexisting chronic kidney disease.
The data from this study add further understanding to the risks of this common medical agent on cardiac outcomes, which have been only rarely studied and limited to our two retrospective studies that show increased risks of atrial fibrillation among those with iodine contrast-induced hyperthyroidism (adjusted hazard ratio [HR] 1.19, [CI 1.06–1.33]) 23 and of heart failure in those with iodine contrast-induced hypothyroidism (adjusted HR, 1.11 [CI, 1.01–1.22]). 22 Our findings indicate the need for larger prospective studies in more diverse populations, in order to elucidate the long-term cardiac burden of receiving iodinated contrast media and examine underlying mechanisms potentially mediated through kidney injury and thyroid dysfunction.
Footnotes
Authors’ Contributions
K.I.: Conceptualization, methodology, interpretation of the data, and writing (initial draft, review, and editing). M.T.B.: Methodology, data acquisition, interpretation of the data, and writing (reviewing and editing). A.L.W., R.E., N.V.N., J.W.C., S.Y.S., C.M.R., and M.L.L.: Writing (interpreting the data, reviewing, and editing). A.M.L.: Conceptualization, data acquisition, interpretation of the data, and writing (initial draft, reviewing, and editing). All authors approved the final version of the article and agreed to be accountable for all aspects of the work.
Author Disclosure Statement
None of the authors have any relevant disclosures.
Funding Information
A.M.L. was supported by the U.S. Department of Veterans Affairs 5|01CX001845. The study sponsor was not involved in study design, data interpretation, writing, or the decision to submit the article for publication. No funding was received for K.I., M.T.B., A.L.W., R.E., N.V.V., J.W.C., S.Y.S., C.M.R., and M.L.L. to declare.
Supplementary Material
Supplementary Table S1
Supplementary Table S2