
Abstract
Background:
Papillary thyroid cancer (PTC) and lymphocytic thyroiditis (LT) co-occur with a prevalence of about 30%. PTC harboring BRAFV600E (PTC-BRAF) confers a worse prognosis, but it is unclear if LT alters prognostic features and recurrence of PTC.
Objective:
We compared the prevalence of PTC-BRAF with and without LT. The risk of adverse pathological features in (i) PTC in the presence and absence of BRAF mutation, irrespective of LT status, was compared to (ii) PTC in the presence and absence of LT, irrespective of BRAF status.
Methods:
We searched PubMed, Embase, and Web of Science Core Collection for observational studies published from 2010 to June 2023 on adult patients with PTC. The search strategy yielded 47 studies with relevant data. Data of baseline characteristics, clinicopathological features, and the quality assessment tool were extracted by two reviewers. The study was registered with PROSPERO (CRD42023437492).
Results:
Of the 47 studies, 39 studies with a total cohort of 28 143, demonstrated that the odds of PTC-BRAF were significantly lower in the presence of LT compared to its absence (odds ratio [OR] 0.53, 95% confidence interval [CI]: 0.48–0.58, p < 0.00001). In PTC-BRAF patients, there was a positive association of central neck nodal disease (CNND), PTC > 1 cm, extra-thyroidal extension, American Joint Committee on Cancer (AJCC) Stage 3–4, and multifocality with pooled ORs of 1.54 (95% CI: 1.16–2.04), 1.14 (95% CI: 0.82–1.58), 1.66 (95% CI: 1.40–1.97), 1.53 (95% CI: 1.35–1.75), and 1.24 (95% CI: 1.11–1.40) respectively, compared to wild-type PTC, irrespective of LT status. In the same studies, PTC with LT patients had lower pooled ORs of 0.64 (95% CI: 0.51–0.81) for CNND, 0.83 (95% CI: 0.73–0.95) for PTC > 1 cm, 0.71 (95% CI: 0.58–0.86) for ETE, 0.84 (95% CI: 0.75–0.94) for AJCC Stage 3–4 compared to PTC without LT, irrespective of BRAF status. PTC recurrence was not affected by BRAF or LT, with pooled ORs of 1.12 (95% CI: 0.66–1.90, p = 0.67) and 0.60 (95% CI: 0.28–1.30, p = 0.20) respectively. Similar results were seen with recurrence expressed as hazard ratio in this limited data-set.
Conclusion:
The odds of PTC-BRAF are significantly lower in the presence of LT than without. PTC with LT, irrespective of BRAF status, was significantly associated with better prognostic factors. Further studies are required to evaluate if LT inhibits PTC-BRAF, and whether this is relevant to the role of immunotherapy in advanced thyroid cancer.
Introduction
Papillary thyroid cancer (PTC) is the most common thyroid cancer, accounting for 80–90% of thyroid cancer cases. Lymphocytic thyroiditis (LT), also known as Hashimoto’s thyroiditis, is an autoimmune disease that is the most common cause of hypothyroidism in developed countries. PTC and LT co-occur with a prevalence of about 30%, raising the possibility of LT as a risk factor for PTC. 1 However, most of the evidence is retrospective, rendering a causal relationship controversial.
Within thyroid cancer, a mutation in BRAF occurs in about 60% of PTCs and activates the oncogenic MAPK signaling pathway. 2 Its presence confers a worse prognosis, with an increased association with tumor size, neck nodal disease (NND), extra-thyroidal extension (ETE), vascular invasion, multifocality, tumor size, and increased recurrence. 3,4
Regarding concurrent LT and PTC, most studies have demonstrated favorable histological features 5 and better survival of PTC with thyroiditis. 6 However, other studies on coexisting LT with PTC showed an increased frequency of multifocality and no effect on ETE and NND. 7
As such, the association between LT and PTC with BRAFV600E (PTC-BRAF) has not been adequately evaluated. PTC-BRAF was reported to occur less often with concurrent LT, 8 but there are inconsistent data. 9 In addition, PTC-BRAF with the coexistence of LT has also been shown to be associated with favorable prognostic features, 10 but again, inconsistencies are present in the literature. 11 Plausibly, LT may be a host immunological response resulting in PTCs with a better prognosis. The immune response to PTC with LT may help to identify targets for immunotherapy in advanced thyroid cancer.
To further clarify the relationship, we conducted a systematic review with meta-analysis to evaluate if there is an association between LT and PTC-BRAF. We aim to evaluate (i) the prevalence of PTC-BRAF with LT and PTC-BRAF without LT and (ii) the odds of adverse pathological features, namely tumor size, lymph node disease, multifocality, extrathyroidal extension, stage of disease, and recurrent disease in (a) PTC with and without mutant BRAF, irrespective of LT status, compared to (b) PTC with and without LT, irrespective of BRAF status.
Methods
We searched PubMed, Embase, and Web of Science Core Collection for observational studies published from 2010 to April 3, 2024, on adult patients with PTC. The search strategy included terms such as “thyroiditis,” “papillary thyroid cancer/carcinoma,” and “BRAF” or “B Raf kinase”, using the Boolean “and/or” operator. Both free text and MeSH searches for keywords were employed (details in Supplement). The protocol for this systematic review and meta-analysis was registered in PROSPERO (CRD42023437492).
The checklist and principles provided by the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline were used to report the meta-analysis. Studies were selected based on the presence of sufficient data to permit the analysis of the odds ratio(OR) for PTC subsets, including PTC-BRAF, PTC with LT, and associated clinicopathological features.
Eligibility criteria
Inclusion criteria were: (i) observational or cohort studies of PTC patients with and without BRAF mutation from 2010 to April 2024 that reported comparative data on the presence or absence of LT and histopathological features, and (ii) LT definition to include histopathological features alone or a combination histological, ultrasound (US), and thyroid antibodies. Exclusion criteria were: (i) non-English studies, (ii) pediatric population (< 18 years), (iii) grey literature, editorials, and conference abstracts, and (iv) animal or tissue studies. If more than one study used the same data source, the larger and most informative study was used.
Extraction of data and risk of bias assessment of eligible studies
Studies were screened independently by two reviewers (S.P. and K.W.) using the Covidence platform. Full text review of studies that met eligible criteria and were potentially suitable was conducted independently by the reviewers. Data extraction with standardized tables for baseline characteristics, clinicopathological features, and quality assessment was done using excel. The quality of included studies was rated using the Quality in Prognosis Studies (QUIPS) tool. 12 Risk of bias assessment was conducted over six domains (study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding, and statistical analysis and reporting) and categorized as low, moderate, or high risk by S.P. and K.W. independently. Disagreements in selection and evaluation were resolved by discussion.
Data analysis
For the analysis of aim, (i) a dichotomous model was undertaken comparing PTC-BRAF with LT and PTC-BRAF without LT. For aim, (ii) the risk of adverse features in PTC was evaluated in a dichotomous model according to the following groups:
PTC in the presence or absence of BRAF mutation, irrespective of LT status. PTC in the presence or absence of LT, irrespective of BRAF status.
The adverse outcomes for groups (a) and (b) were analyzed independently with separate forest plots and effect measures. Thereafter, effect measures from (a) and (b) were compared. Meta-analysis of data was done in Review manager (RevManV5.4.1). OR and 95% confidence interval (95% CI) for each study were calculated. For recurrence data, OR and hazard ratio (HR) were used. As the measure of heterogeneity, I 2 across most studies was >50% (moderate), a random-effects model was chosen. Funnel plots were used to assess for publication bias.
Literature search
We identified 449 relevant studies since 2010 by searching PubMed, Embase, and Web of Science (Fig. 1). A total of 150 studies were excluded as they were identified as duplicate studies. Two hundred ninety-nine studies were screened, and 131 were excluded after screening the title and abstract. Full-text screening was conducted on 168 studies, and 121 studies were excluded because they did not fulfill the criteria of LT definition (US and antibodies only), had discordant designs, comparators, or patient populations, were unavailable in full text, or lacked subset data. Data were finally extracted from 47 studies.
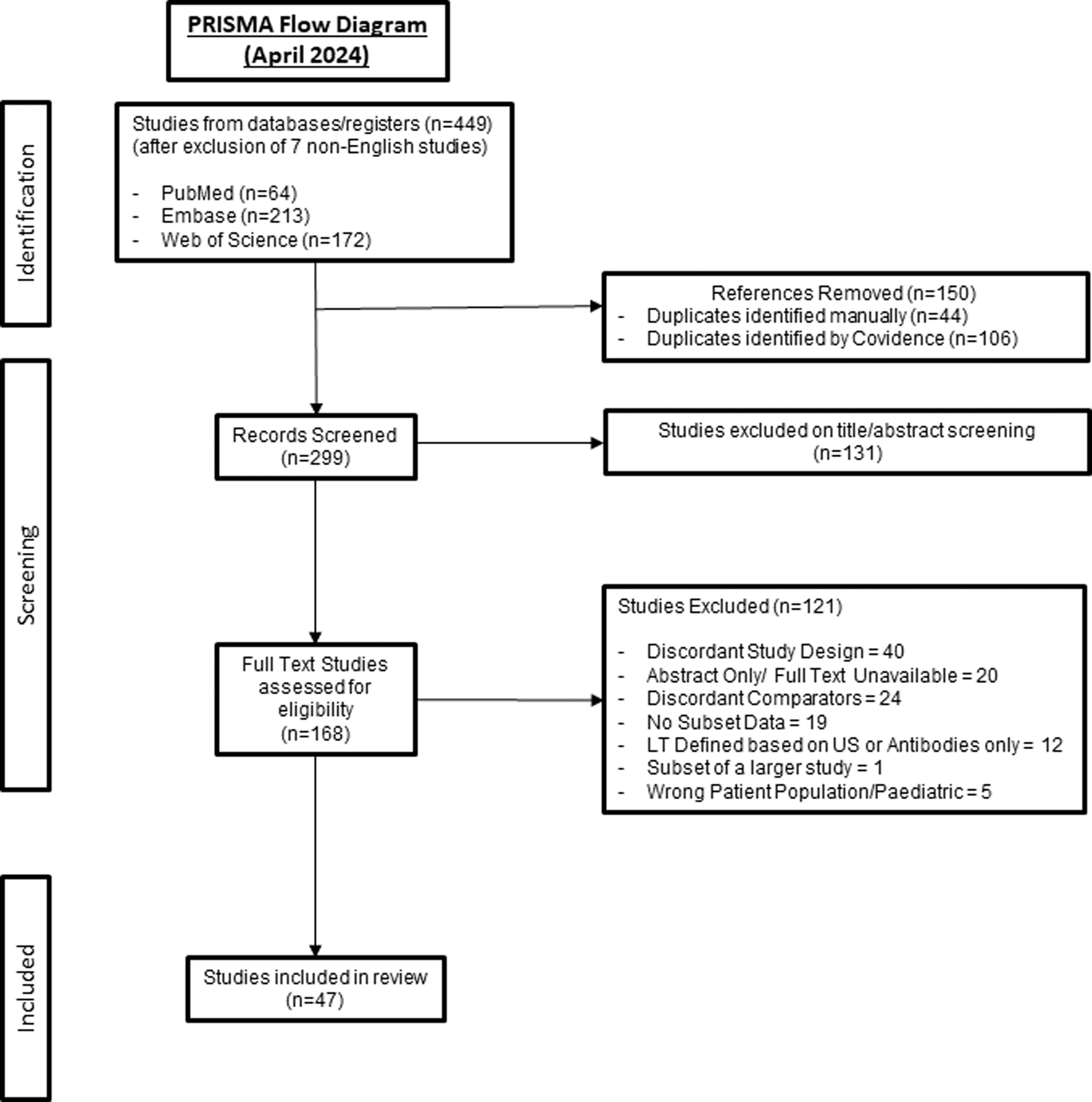
PRISA flow diagram.
Baseline characteristics
Forty-seven studies were included, comprising 33,175 patients, with a female predominance of 77.7%. Data from Hong et al. were reported separately due to two time periods: (a) 1995 to 2003 and (b) 2009 to 2012. 13 Of the 35 studies reporting the age of patients, on average, 57.8% were young (< 45/< 55 years). Microcarcinomas accounted for 59.9% in 34 studies that reported on size. Four studies 14 –17 exclusively focused on papillary thyroid microcarcinomas. Among the 47 studies, 37 studies reported 38.9% ETE, 39 studies reported 33.9% multifocality, and 30 studies reported 47.7% central neck nodal disease (CNND). Overall, 69.6% had PTC-BRAF and 27.3% had PTC with LT present. Characteristics of the included studies are described in Table 1 and Supplementary Table S1 in the Supplement.
Baseline Characteristics of Studies
ETE, extra-thyroidal extension; LT, lymphocytic thyroiditis.
Quality of the included studies
Using the QUIPS risk of bias assessment instrument, 46%, 33%, and 21% of studies were rated as low, moderate, and high risk of bias, respectively, and the Risk of Bias Visualization (ROBVIS) Tool was used for visual representation (Fig. 2). 18 The most frequent high risk of bias was detected in cohort studies with limited reporting of loss to follow-up of recurrence data (details in Supplement). Given the retrospective, observational cross sectional nature of most articles in this meta-analysis, exposures of interest (BRAF/LT status) were not measured prior to the outcomes of interest. Similarly, such study designs often lacked blinding amongst assessors, as well as any sample size justification and power descriptions. Sensitivity analysis excluding studies with a high risk of bias is shown in Supplementary Table S2.
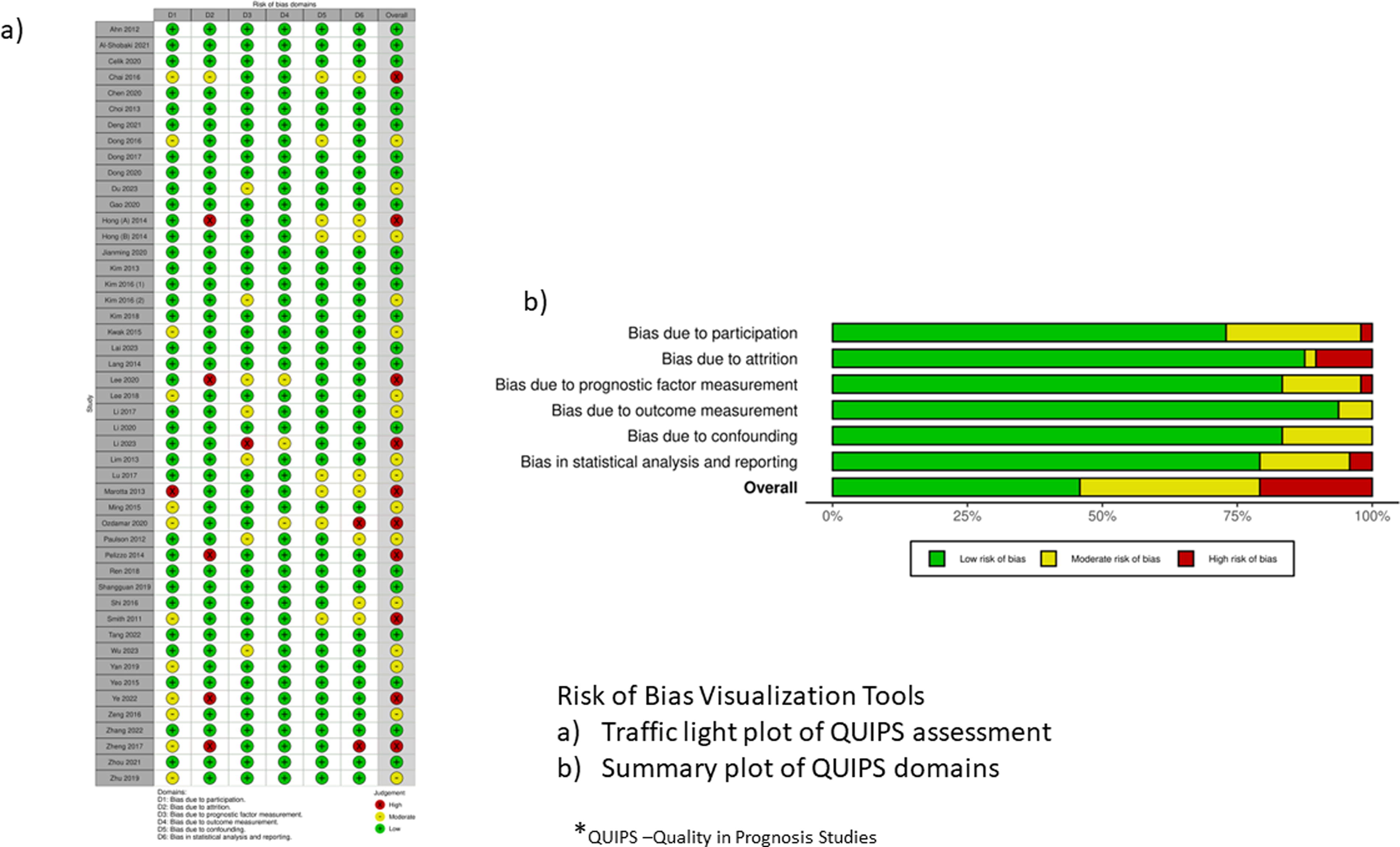
Risk of bias with using ROBVIS tool:
Prevalence of PTC with BRAF mutation in the presence of LT
We assessed the prevalence of PTC-BRAF in the presence of LT in 39 studies that had relevant data. 9 –11,13 –15,17,19 –48 There were 5,134 patients with PTC-BRAF in the presence of LT and 16, 684 patients with PTC-BRAF in the absence of LT, in a total cohort of 28,143. The odds of PTC-BRAF were significantly lower in the presence of LT compared to its absence (pooled OR = 0.53, 95% CI: 0.48–0.58, p < 0.00001) (Fig. 3). Moderate heterogeneity (I 2 = 42%) across studies in the random-effects model was observed. The funnel plot demonstrated asymmetry, which may be attributed to the heterogeneity of the studies and publication bias, with a lack of smaller studies showing a negative effect.
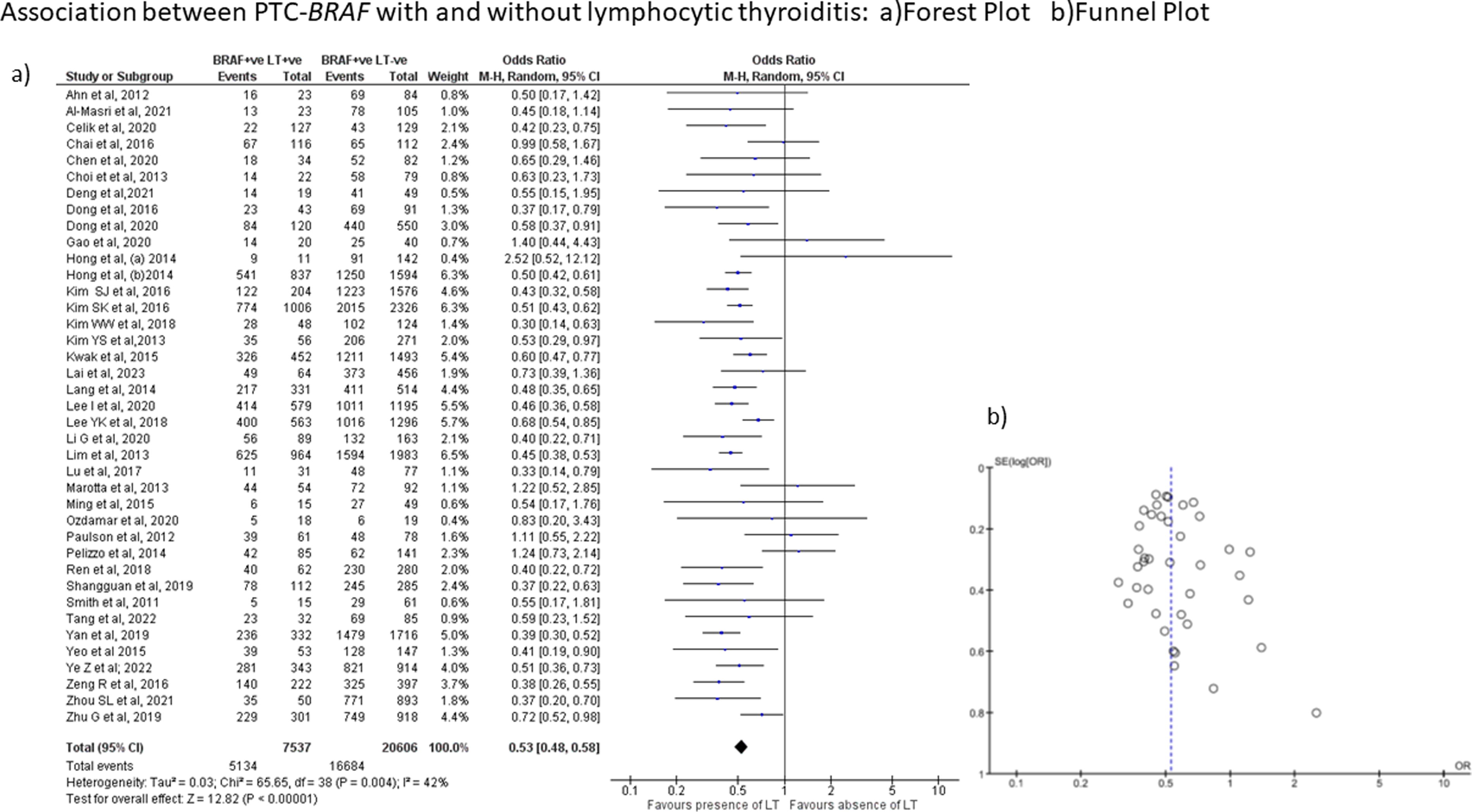
Prevalence of PTC-BRAF with and without Lymphocytic Thyroiditis (LT):
Pathological features
Further analysis was performed on adverse pathological features for aim (b). Many clinicopathological features had < 10 studies with asymmetry in the funnel chart and moderate to high heterogeneity.
Central neck nodal disease (CNND)
Ten studies with 7,425 patients, among which 5,828 were PTC-BRAF patients and 1,567 were PTC without BRAF. 16,23,27,31,46,47,49 –52 In PTC-BRAF patients, 3,143 had CNND with a pooled OR of 1.54 (95% CI: 1.16–2.04; p = 0.003, I 2 = 74%, REM), compared to wild-type PTC [Fig. 4A(a)]. In the same studies, we evaluated the presence of CNND in PTC with LT, irrespective of BRAF status. 954 PTC with LT patients had CNND with a pooled OR of 0.64 (95% CI: 0.51–0.81; p = 0.0002, I 2 = 67%, REM), compared to PTC without LT [Figure 4A(b)]. The funnel plot [Fig. 4A(a)] showed reasonable symmetry with a low level of publication bias. However, smaller studies in the funnel plot [Figure 4A(b)] are lacking.
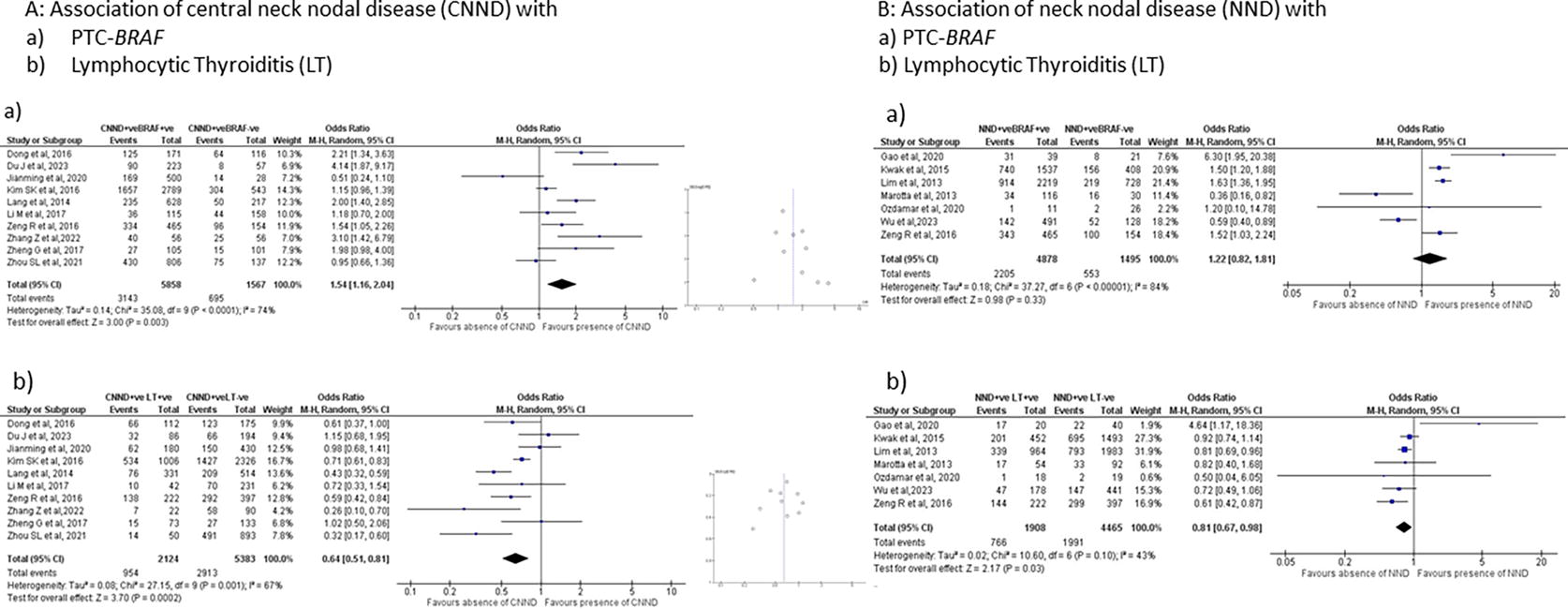
Figure 4A: Association of central neck nodal disease with
Neck nodal disease (NND)
Presence of NND was determined to assess if the above relationship was maintained. Seven studies 9,10,25,35,46,53,54 with 2,205 out of 4,878 PTC-BRAF patients had NND compared to 553 out of 1,495 wild-type PTC, with a pooled OR of 1.22 (95% CI: 0.82–1.81; p = 0.33, I 2 = 84%, REM), which was not significant [Figure 4B(a)]. On the other hand, in the same studies, the presence of LT irrespective of BRAF status, was negatively associated with NND with a pooled OR of 0.81 (95% CI: 0.67–0.98; p = 0.03, I 2 = 43%, REM) [Figure 4B(b)]. Given the small number of studies, it was difficult to draw conclusions on publication bias, and a funnel plot has not been displayed.
Size: PTC >1 cm
Apart from lymph node disease, we assessed other pathological features including size, extrathyroidal extension, American Joint Committee on Cancer (AJCC) stage, and multifocality. Six studies 27,30,35,46,47,55 with 8,612 patients had data on PTC > 1 cm vs PTC ≤ 1 cm (Fig. 5A). In PTC-BRAF patients, 2,888 out of 6,875 patients had PTC > 1 cm with a pooled OR of 1.14 (95% CI: 0.82–1.58; p = 0.45, I 2 = 85%, REM). In comparison, for PTC and LT, irrespective of BRAF status, 882 out of 2,346 had PTC >1 cm, with a pooled OR of 0.83 (95% CI: 0.73–0.95; p = 0.007, I2 = 21%, REM). Again, with fewer than 10 studies, conclusion on publication bias cannot be made.
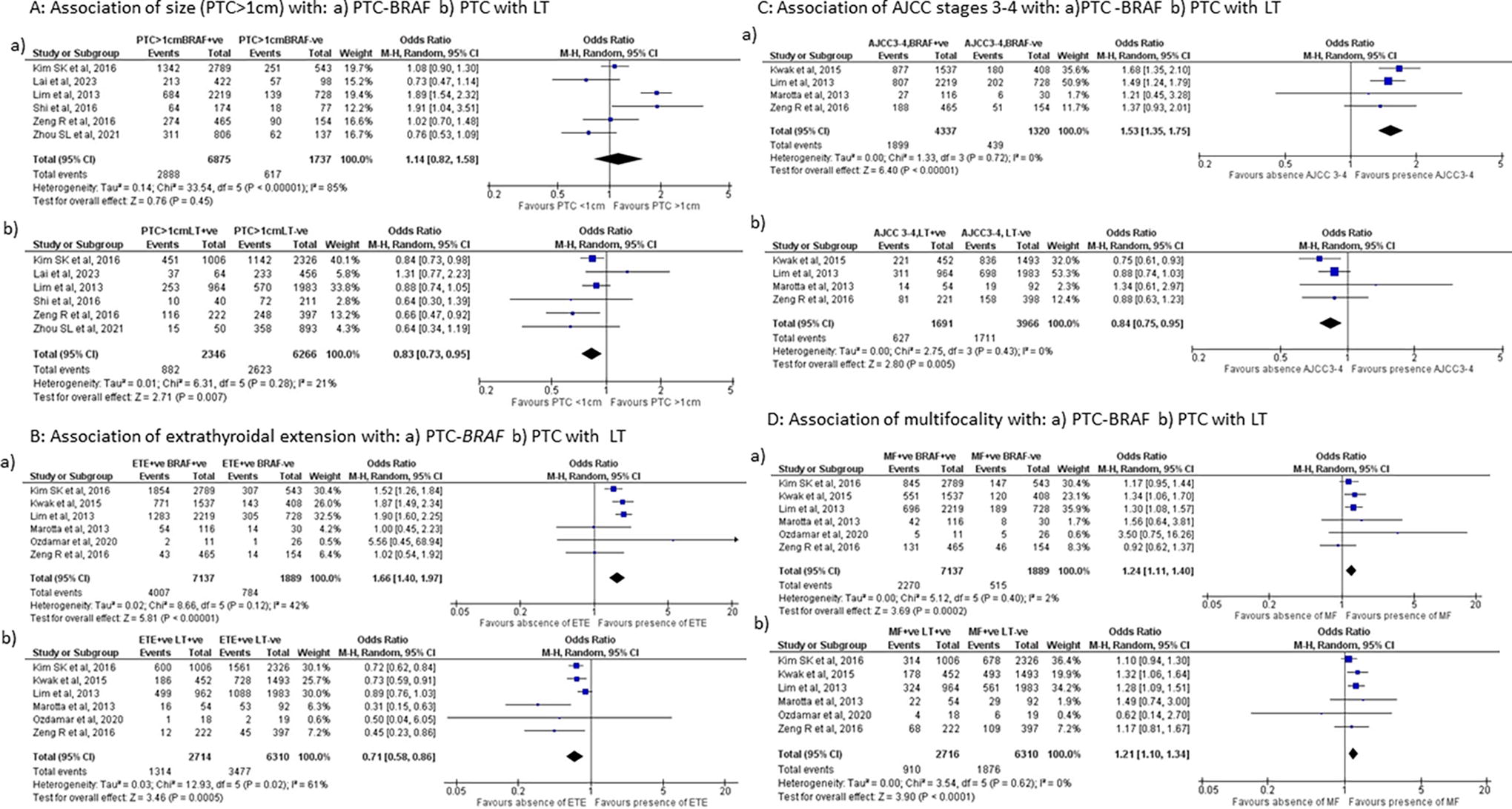
Figure 5A: Association of size (PTC > 1 cm) with:
Extrathyroidal extension
Six studies 9,10,27,35,46,53 reported on ETE in PTC -BRAF patients and PTC with LT (Fig. 5B). ETE was significantly positively associated with the presence of BRAF, irrespective of LT status, with a pooled OR of 1.66 (95% CI: 1.40–1.97; p < 0.0001, I 2 = 42%, REM). In the same cohort of patients, ETE was significantly negatively associated with a pooled OR of 0.71 (95% CI: 0.58–0.86, p = 0.0005, I 2 = 61%, REM), compared to PTC without LT.
AJCC stage 3–4
Four studies. 9,10,35,46 reported the AJCC stages (AJCC Cancer Staging Manual, seventh edition (2010) 56 of PTC patients with BRAF and LT status (Fig. 5C). In PTC-BRAF, 1,899 out of 4,337 patients had higher AJCC stage 3–4, with a pooled OR of 1.53 (95% CI: 1.35–1.75; p < 0.00001, I 2 = 0%, REM), irrespective of LT status. In the same cohort of patients, AJCC stage 3–4 were present in 627 out of 1,691 PTC with LT, with a pooled OR of 0.83 (95% CI: 0.74–0.94, p = 0.003, I 2 = 0%, REM), irrespective of BRAF status.
Multifocality
Apart from lymph node disease, size, extrathyroidal extension, and stage of disease, we evaluated multifocality. Six studies 9,10,27,35,46,53 had adequate data on multifocality of PTC patients with BRAF and LT status (Fig. 5D). In PTC-BRAF, the odds of multifocal carcinomas were higher, with a pooled OR of 1.24 (95% CI: 1.10–1.40; p = 0.0002, I 2 = 2%, REM). In the same cohort of patients, the odds of multifocality were similarly increased in PTC with LT, with a pooled OR of 1.21 (95% CI: 1.10–1.34, p < 0.00001, I 2 = 0%, REM), irrespective of BRAF status. Unlike other pathological features, the risk of multifocality was similar in PTC with LT and PTC-BRAF.
Recurrence
Recurrence data were presented as cross-sectional data with a mean follow-up ranging from 24 to 120 months in nine studies 10,13,20,21,38,43,45,53,57 (Fig. 6A). Recurrence occurred in PTC-BRAF with a pooled OR of 1.12 (95% CI: 0.66–1.90, p = 0.67, I 2 = 57%, REM), failing to reach significance. However, unlike other pathological factors described above, only four studies. 10,32,53,57 had concurrent recurrence data for PTC with LT. PTC recurrence was not affected by LT, with a pooled OR of 0.60 (95% CI: 0.28–1.30, p = 0.20, I 2 = 37%, REM).
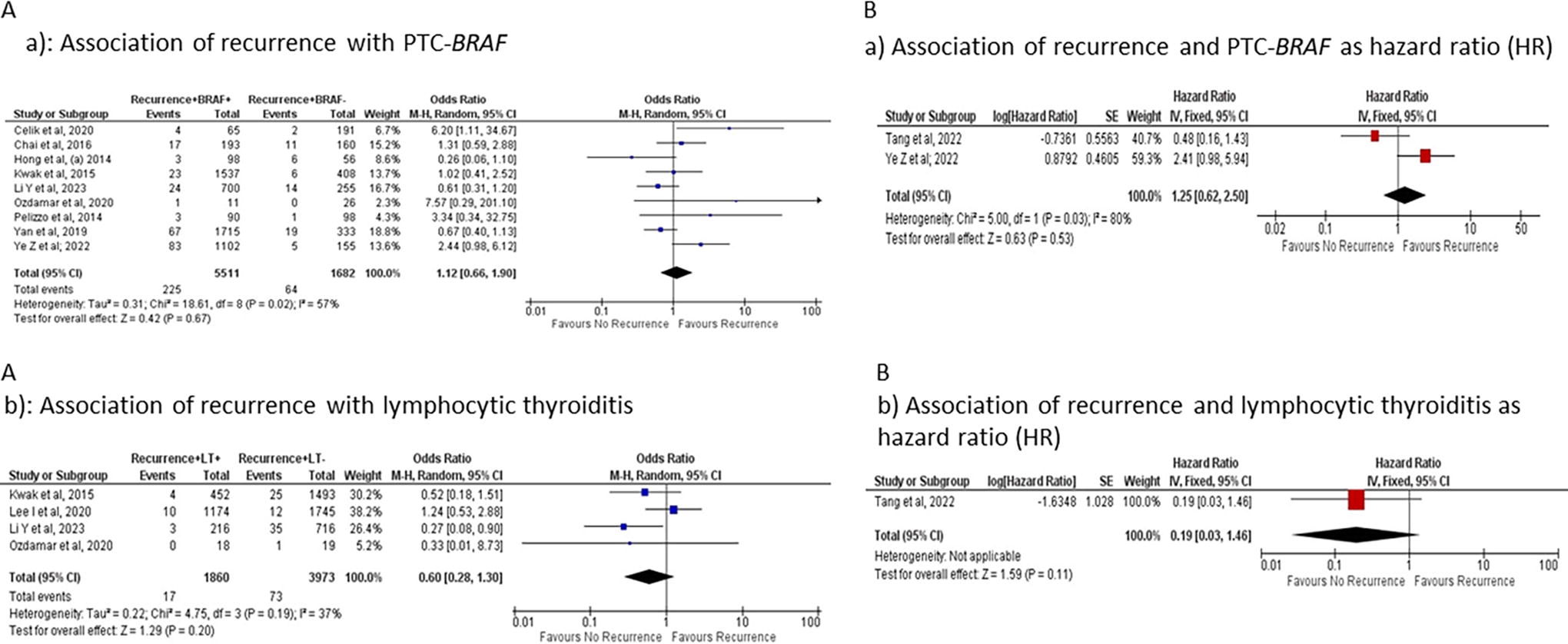
Only two studies. 42,45 presented recurrences as HR with data on univariate analysis having median follow-up periods of 30 and 21 months, respectively (Fig. 6B). In this limited dataset, PTC recurrence was not affected by either BRAF (HR 1.25, 95% CI: 0.62–2.50, p = 0.53) or LT (HR 0.19, 95% CI: 0.03–1.46, p = 0.11). 42
Sensitivity analysis after exclusion of high-risk of bias studies did not show significant changes in prognostic features except in NND, which was no longer significantly associated in PTC with LT (Supplementary Figs. S1, Figs. S2, Figs. S3 and Supplementary Table S2).
Discussion
Our systematic review and meta-analysis found that the prevalence of the BRAF mutation in PTC was 47% lower in the presence of LT than in its absence. It has been well established that the PTC-BRAF mutation is associated with adverse prognostic features. The presence of LT in PTC, irrespective of BRAF status, was significantly associated with better prognostic factors, including fewer cases of CNND, smaller PTC, less ETE, and lower AJCC stage disease (Table 2), compared to the absence of LT. Interestingly, PTC with LT was associated with increased multifocality, similar to PTC with the BRAF mutation. Although there was a trend towards a reduced risk of recurrence in PTC with LT, it was not significant, possibly due to the paucity of data. It is not known if LT has an inherently protective effect or if these associations are mediated via a lower prevalence of the BRAF mutation. The interplay between the immune system and BRAF as a driver mutation needs to be explored.
Summary of Effect Size of Pathological Features in Relation to PTC-BRAF and PTC with Lymphocytic Thyroiditis (LT)
CI, confidence interval; LT, lymphocytic thyroiditis; OR, odds ratio; PTC, papillary thyroid cancer.
The negative association between LT and BRAF-induced adverse prognostic features contrasts with data associating LT with increased PTC risk. 57 One possibility is that the antitumor immune response from LT has effective cytotoxicity, resulting in negative selection pressure on BRAF as a driver mutation. Another possibility is that the inflammatory nature of LT is more likely to induce PTC by oncogenes other than BRAF (e.g., RET fusions). 58
LT-associated anti-tumor mechanisms against PTC include elevated major histocompatibility complex (MHC) class I expression with enhanced T cell activation and increased IL-2 production. 59,60 PTC-BRAF has been associated with a decrease in CD8+ T cells, cancer-associated fibroblasts, and upregulation of immune checkpoints, consistent with adverse features seen in PTC-BRAF. 61 Prominent B cell infiltration with a tertiary lymphoid structure (TLS) signature is a recognized features of LT. TLS density has recently been recognized as an antitumor adaptive immune response, and TLS density has a beneficial effect on disease-free survival in some cancers, 62,63 but it has not been adequately explored in thyroid cancer. Immune responses to PTC in the presence of LT may help to identify targets for immunotherapy in advanced thyroid cancer.
Although, in general, PTC has an excellent 5-year survival rate, the morbidity of thyroid cancer related to recurrent disease remains significant. 64 Current risk stratification does not consider LT as a prognostic feature or treatment modifier. Notably, LT is more likely to be associated with thyroglobulin antibodies, which interferes with thyroglobulin assays. 65 More work is needed to understand whether the presence of LT should influence treatment decisions in PTC.
Women with LT were found to be 30% more likely to have coexisting PTC compared to women without LT. 66 PTC occurred at a younger age in the presence of LT compared to its absence. 67 Older age is a risk factor for BRAF mutation in PTC patients, especially in those without LT. 68 It is not clear if sex and age are confounding factors that may account for PTC with LT having a better prognosis.
Previous systematic reviews have shown that LT increases the risk of developing PTC but decreases the risk of adverse clinicopathological features. 6 The meta-analysis by Janicki et al. reviewed evidence on the relationship between PTC-BRAF and concomitant PTC-LT. 69 They also demonstrated that PTC with LT had a significantly lower prevalence of BRAF mutation compared to PTC without LT (OR 0.45, 95% CI: 0.35–0.58) using nine studies. For pathological features, they categorized patients into PT-BRAF with and without thyroiditis (two factors), whereas we categorized them as either PTC-BRAF or PTC with LT (single factor). They showed in 3–5 studies with 1500–3500 total patients that NND and ETE were less likely in PTC-BRAF with thyroiditis. Similar analysis are shown from the studies we included in Supplementary Figures S4 in the Supplement. On the other hand, using a single factor in 4–10 studies with 5500-8500 total patients, we showed that the presence of LT in PTC is associated with better prognostic features, irrespective of BRAF status, adding power with less confounding effects. Comparison of measured effects after exclusion of studies with a high risk of bias showed similar results, supporting the robustness of our data (Supplementary Table S2). Our meta-analysis of recurrence data did not find a significant effect size. Although HR is a superior statistical analysis for recurrence with time-to-event and censoring, studies reporting HR as a univariate analysis are lacking.
The main limitation of this meta-analysis was that most studies were based on retrospective observational cross-sectional data obtained from surgical specimens. As the assessment of exposures of interest (BRAF/LT status) occurred simultaneously with outcomes of interest, selection bias cannot be excluded. Heterogeneity of >40% across many studies and fewer than ten studies for pathological features may also cause publication bias. Although 21% studies showed a high risk of bias, the measured effect size did not change significantly in most pathological features after the exclusion of these studies. A limitation of this meta-analysis is that potential confounders are not accounted for. Most large studies from Korea and China have reported a higher prevalence of the BRAF mutation and also routinely conduct prophylactic central lymph node dissection. It is difficult to know if the findings remain applicable to other populations.
Conclusion
This meta-analysis found that the prevalence of PTC with BRAFV600E was significantly lower in the presence of LT than in its absence. Presence of LT in PTC was associated with better prognostic features compared to the absence of LT, independent of BRAF status. In the same cohort of patients, the odds of several adverse pathological features, including lager tumor size, CNND, extrathyroidal extension, and higher stage disease, were significantly lower in PTC with LT compared to PTC-BRAF, evaluated as independent groups. Further studies are required to determine whether LT inhibits PTC-BRAF, and if so, whether this can be harnessed by immunotherapy in advanced thyroid cancer.
Footnotes
Acknowledgement
The authors acknowledge the statistical consulting service provided by Mr. Jim Matthews from the Sydney Informatics Hub, a core research facility of the University of Sydney.
Authors’ Contributions
R.C.-B., M.G., L.T., and M.B. contributed to conceptualization, supervision of the study, analysis of data and writing (reviewing and editing). K.W. contributed to data curation, data analysis, and validation of data and writing (original draft). S.P. contributed to methodology, data curation, data collection, data analysis, and writing (original draft).
Author Disclosure Statement
All authors have no conflict of interest.
Funding Information
No funding was received for conducting this research and reporting the results.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Table S1
Supplementary Table S2