
Abstract
Objectives:
Graves’ disease (GD) is the most common cause of hyperthyroidism. Antithyroid drugs (ATDs) are the first-line treatment, but when discontinued, >50% of patients experience relapses. Conventional definitive treatment options include surgery and radioiodine therapy (RAI), each with its own disadvantages. Radiofrequency ablation (RFA) achieved promising short-term remission rates in a previous pilot study. The current study reports our experience of using RFA to treat relapsed GD in the largest cohort of patients with a longer follow-up period.
Methods:
This single-arm prospective study recruited consecutive patients aged ≥18 with persistent/relapsed GD requiring ATD from two tertiary endocrine surgery centers. Those with compressive goiter, suspected thyroid malignancy, moderate-to-severe Graves’ ophthalmopathy, preference for surgery/RAI, or pregnancy were excluded. Eligible patients received ultrasound-guided RFA to the entire bulk of the thyroid gland. ATDs were discontinued afterward, and thyroid function tests were monitored bimonthly. The primary outcome was the disease remission rate at 24 months follow-up after single-session RFA, defined as being biochemically euthyroid or hypothyroid without ATD. Secondary outcomes were complication rates.
Results:
Of the 100 patients considered, 30 (30.0%) patients were eligible and received RFA. Most were female patients (93.3%). The median total thyroid volume was 23 mL (15.9–34.5). All completed 24 months follow-up. After single-session RFA, disease remission rates were 60.0% at 12 months and 56.7% at 24 months. Among the 13 patients with relapse after RFA, 9 (69%) required a lower ATD dose than before RFA; 2 received surgery without complications. Total thyroid volume was the only significant factor associated with relapse after RFA (odds ratio 1.054, confidence interval 1.012–1.099, p = 0.012). At 24 months, RFA led to disease remission in 100% of the 9 patients with a total thyroid volume <20 mL and 35% of patients with a total thyroid volume ≥20 mL (p = 0.007). There was no vocal cord palsy, skin burn, hematoma, or thyroid storm after RFA.
Conclusions:
In a highly selected group of patients with relapsed GD and predominantly small thyroid glands, single-session RFA may achieve disease remission. Smaller total thyroid volume may be a favorable factor associated with disease remission after RFA. The results of this study need to be confirmed with a long-term clinical trial.
Clinical Trial Registration: This study is registered at www.clinicaltrial.gov with identifier NCT06418919.
Introduction
Graves’ disease (GD) is an autoimmune thyroid disorder that arises from the presence of stimulating auto-antibodies to thyrotropin on thyroid follicular cells. GD is the most prevalent cause of hyperthyroidism, with a lifetime incidence of ∼3% in females and 0.5% in males. 1 Antithyroid drugs (ATDs) are commonly the preferred initial treatment for GD in many parts of the world. Surgical or radioiodine therapy (RAI) is usually reserved for patients who had persistent hyperthyroidism requiring ATD for >18–24 months, with significant Graves’ ophthalmopathy (GO) or with compressive symptoms. 2,3 Understandably, a significant percentage of patients with persistent or relapsed GD are reluctant to undergo surgery or RAI because of apprehensions about surgical risks or radiation exposure. 1 Radiofrequency ablation (RFA) is an image-guided thermal ablation technique that is increasingly used in a variety of thyroid conditions, both benign and malignant. As previous studies have demonstrated that thermal ablation by high-intensity focused ultrasound (HIFU) can also reduce the functional capacity of the thyroid gland when applied to both lobes, 4,5 this inspired our hypothesis that bilateral RFA could also be a nonsurgical, effective treatment for inducing disease remission in patients with persistent or relapsed GD. The short-term efficacy following bilateral RFA was reported in a previous pilot study. 6 In the current study, we present the experience from the largest cohort of patients who had predominantly small glands, with completion of 24 months of follow-up.
Methods
Patients
This prospective, single-arm study followed the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (UW 22–504). It is registered at www.clinicaltrial.gov with identifier NCT06418919. Patients were recruited after providing written informed consent. From March 2020 to December 2021, consecutive adult patients aged 18 years or over with persistent or relapsed GD were considered. Patients from the previous pilot study were also included for analysis. 6 The inclusion criteria have been described before 6 and included the following: first, the diagnosis of GD had to fulfil the standard clinical criteria for GD, which included an elevated serum free thyroxine (fT4), suppressed thyrotropin (TSH) level, positive TSH receptor (TSHR) antibody, and a clinically detectable diffuse goiter. Second, patients had to rely on ATD to maintain a biochemically euthyroid status for ≥18 months, or they had a relapse of GD following previous ATD treatment. Third, patients consented to RFA and had no strong wish to undergo surgery or RAI as a definitive treatment for their persistent or relapsed GD. The exclusion criteria were the presence of clear and immediate surgical indications (e.g., compressive goiter, suspected or documented thyroid malignancy, or moderate-to-severe GO); plans for pregnancy within 6 months; currently pregnant or lactating; or had any medical conditions that would make them too ill to undergo thermal ablation.
Pre-treatment preparation and evaluation
All patients were rendered biochemically euthyroid with ATD before RFA. Baseline serum TSH, FT4, antithyroglobulin antibodies, antithyroid-peroxidase antibodies, anti- TSHR antibody levels, as well as platelet count and clotting profile were checked on the date and just before the procedure. The same ultrasound (USG) machine (Samsung HS60) and transducer (Samsung LN5-12) were used for evaluation and treatment. The dimensions of each thyroid lobe (width [W], depth [D], and length [L]) were measured, and the volume of each thyroid lobe (V) was calculated using the formula V = W × D × L × 0.523. 7 Total thyroid volume was calculated by the sum of the volume of both lobes. 8 If thyroid nodules were present, USG-guided fine-needle biopsy with cytology (FNAC) would be performed to prove their benign nature before RFA. Vocal cord mobility was assessed by trans-laryngeal ultrasonography (LUSG) before, during, and after ablation and also by flexible laryngoscopy on day 7 after ablation. 9 On LUSG, vocal cord palsy (VCP) was defined as any reduction in one of the three vocal cord landmarks: the true vocal cord, the false vocal fold, or the arytenoid cartilage.
RFA procedure
This has been described before. 6 All RFA procedures were performed by the same surgical team consisting of two highly experienced endocrine surgeons, each having performed >100 thyroid RFA procedures. The same RF generator (STARmed VIVA RF generator) and electrode (star RF Electrode—Fixed, 18G 70 mm, 10 mm active tip length) were used. Before ablation, intravenous boluses of midazolam (Cheplapharm) (1–3 mg) and pethidine (Martindale Pharmaceuticals) (10–30 mg) were given. 10 Perithyroidal local anesthesia with 1% lignocaine was given. Under USG guidance, the RFA electrode was inserted into each thyroid lobe. The procedure aimed to ablate all of the vascularized thyroid parenchyma, that is., the right lobe, left lobe, and the isthmus if its thickness was >0.5 cm. Ablation with 50–60 W of power under USG guidance was performed using the trans-isthmic approach and moving-shot technique. 11,12 The formation of microbubbles would indicate successful ablation of the area concerned. Ablation close to the “danger triangle” of the tracheal esophageal groove was avoided. 11
Throughout the procedure, the patient’s vital signs, including heart rate, blood pressure, respiration rate, and peripheral oxygenation, were continuously monitored. Any adverse events that took place during and after the RFA procedure were carefully documented. The patients were closely observed for a duration of 4–6 hours and were discharged once they had consumed food and reported no complaints of nausea or vomiting.
Post-ablation follow-up
Patients were advised that they might experience palpitations or worsening of other thyrotoxic symptoms during the initial 2-week period. ATDs were immediately discontinued following RFA. Patients were instructed to take propranolol, a beta-blocker, in the event they experienced palpitations. Thyroid function was monitored at 2 weeks, 4 weeks, and thereby every 2 months, when patients also received thyroid USG assessment. GO was assessed every 6 months.
Study outcome
The primary objective of this study was to assess the rate of disease remission at 24 months after RFA. Disease remission was defined as achieving either a biochemically euthyroid state (FT4 levels between 12 and 23 pmol/L) or a hypothyroid state (FT4 levels below 12 pmol/L) without the need for ATDs. Relapse was defined as either a biochemically hyperthyroid state (FT4 levels above 23 pmol/L) or the requirement of ATD to maintain a euthyroid state. Partial response was defined as the ability to maintain a biochemically euthyroid state with a lower dose of ATD compared to baseline. Complications, including VCP, hematoma, skin complications, thyroid storm, and changes in GO activity following RFA, were documented.
Biochemical results
All tests on serum TSH, FT4, and antithyroid antibodies levels were performed at our institution’s laboratory. The normal reference values for TSH were 0.35–4.78 mIU/L, while FT4 ranged from 12 to 23 pmol/L. Serum antithyroglobulin and antithyroid peroxidase antibodies were determined using radioimmunoassay (Bio Code), and any values >99 IU/mL were considered positive. For anti-TSHR antibodies, any values ≥1 IU/L were considered positive.
Statistical analysis
Statistical analysis was performed using software (SPSS version 28, IBM). Missing data, if any, were removed from the analysis. Data were expressed as mean ± standard deviation or median with interquartile range (IQR), as appropriate. Datasets were compared using the Student’s two-tailed t-test for variables with a normal distribution and the Mann–Whitney U test for nonparametric data. Comparison of categorical variables was performed using the χ2 test. Kaplan–Meier analysis and the log-rank test were performed to analyze remission rates, and Cox regression analysis was used to identify factors associated with relapse. The threshold for a statistically significant difference was considered to be a p-value of <0.05.
Results
Over the study period, 100 consecutive patients with persistent/relapsed GD were referred to our unit for management (Fig. 1). Seventy patients were excluded from the study and underwent surgery because of severe compressive symptoms (n = 33), severe GO (n = 3), plans for pregnancy within 6 months (n = 9), concomitant thyroid malignancy or indeterminate thyroid nodules on fine-needle aspiration cytology (n = 7), and refusal to participate or a preference to undergo surgery directly (n = 18). After these exclusions, 30 (30.0%) patients were eligible and underwent RFA treatment, all of whom completed 24 months of follow-up. The baseline characteristics of our patients are shown in Table 1. The cohort comprised mainly female patients (93.3%), with a median age of 36 years (IQR 29–45). The median follow-up time was 31 months (IQR 28–39). The median disease duration was 108 months (IQR 60–132), and the median duration of ATD use before RFA was 49 months (IQR 25–62). All patients were confirmed to have elevated anti-TSHR before RFA (median 3.3 [1.5–6.4]), and all required ATD to maintain a euthyroid state. Most patients were on carbimazole (90.0%) before RFA. Only one patient (3.3%) was on block-and-replace therapy. Except for one patient who had undergone partial thyroidectomy 10 years ago, none of the remaining patients had previous thyroid surgery. All patients suffered relapsed GD after discontinuation of ATD and were rendered biochemically and clinically euthyroid with ATD before RFA. The median total thyroid volume was 23.0 mL (IQR 15.9–34.5).
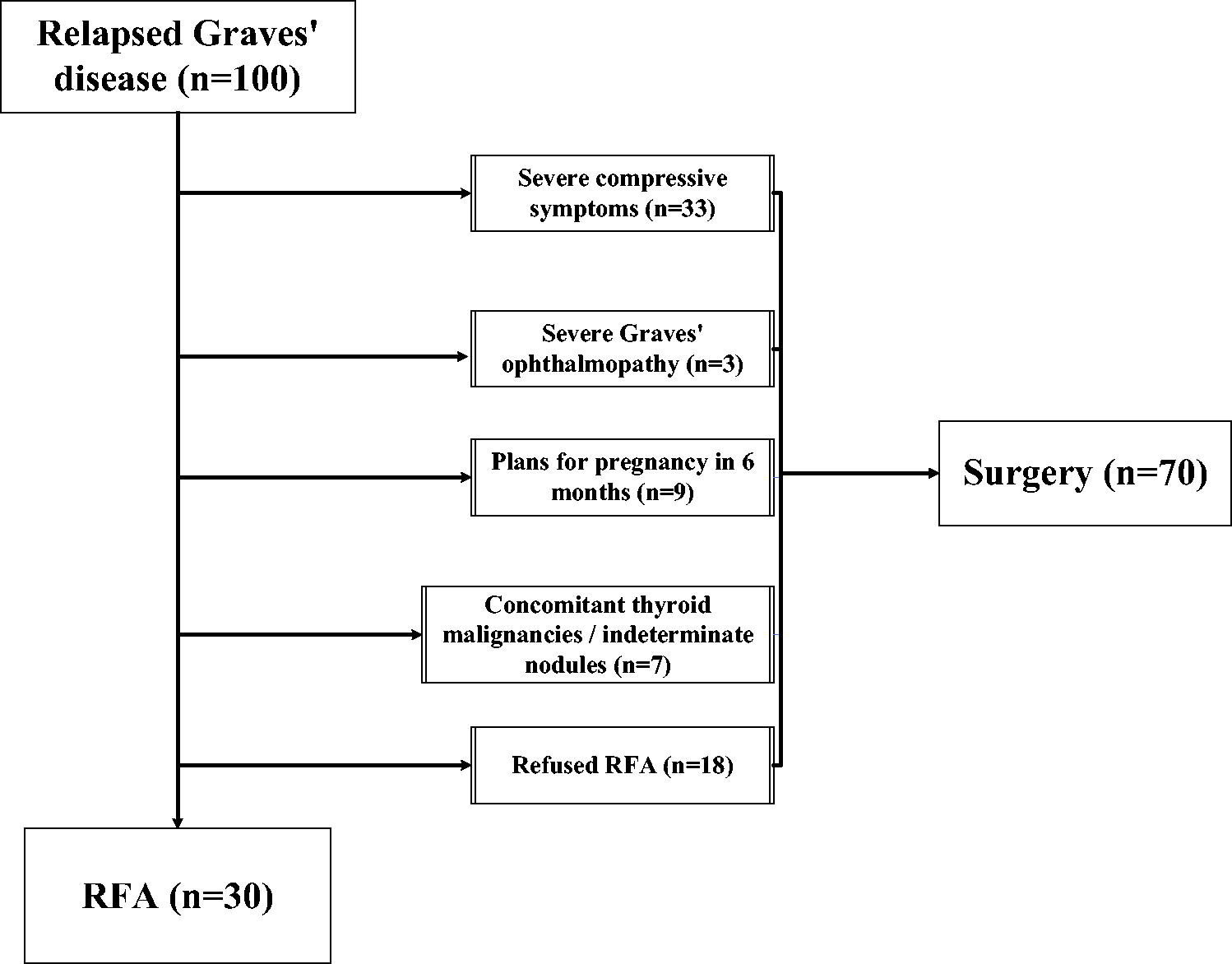
Flow diagram showing patient recruitment pathway.
Baseline Characteristics (n = 30) of Patients Undergoing Single-Session Radiofrequency Ablation for Persistent/Relapsed Graves’ Disease
ATD, antithyroid drugs; anti-TSHR, anti-thyrotropin receptor; CAS, clinical activity score; FT4, free thyroxine; GO, Graves’ ophthalmopathy, IQR, interquartile range; RFA, radiofrequency ablation; TSH, thyrotropin.
Treatment parameters are shown in Table 2. All patients received bilateral lobe thyroid ablation, except for one patient who received ablation to a right thyroid remnant following partial thyroidectomy 20 years ago. The median total energy applied per unit volume was 2046 Joules/mL (IQR 1557–2533). The median total ablation time was 1241 seconds (IQR 916–1450), which is ∼20 minutes. All patients were discharged the same day, ∼6 hours after ablation. There were no major complications, such as VCP, skin burn, hematoma formation, thyroid storm, or acute thyrotoxic symptoms that required treatment. At 24 months, there was no worsening of preexisting or new development of GO.
Treatment Parameters (n = 30)
Disease Status Following Single-Session Radiofrequency Ablation of Graves’ Disease (n = 30) at 24 Months
Serum FT4 level within the normal range without daily ATD maintenance.
Serum FT4 level below the normal range without daily ATD maintenance.
Relative to daily maintenance dose before RFA.
GD, Graves’ disease.
Disease remission rates at 24 months after single-session RFA
Figure 2 shows the Kaplan–Meier curve of complete remission rates over time, which were 60.0% at 12 months, 60.0% at 18 months, and 56.7% at 24 months. All except one relapse occurred within the first 12 months (92.3%). One relapse occurred at 24 months. Seventeen patients (56.7%) were in disease remission at 24 months (Fig. 3). Among them, 15 were biochemically euthyroid, all with normal FT4 and TSH. Two patients (6.7%) were biochemically hypothyroid and required thyroxine replacement. Nine patients (30%) required a lower maintenance ATD dose (i.e., partial response) and four required the same dose (Table 3).
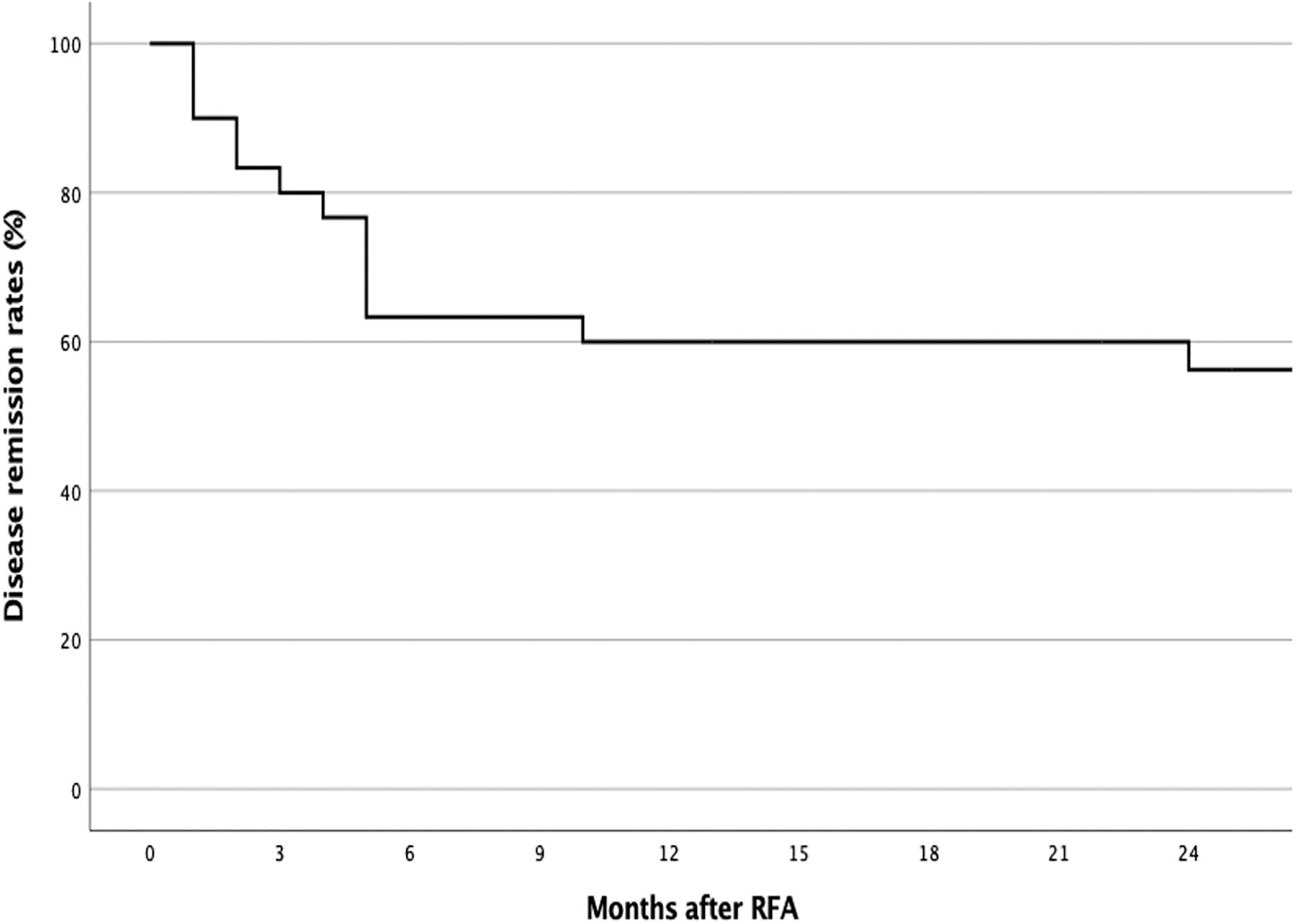
Kaplan–Meier analysis of the rate of disease remission after bilateral thyroid lobe radiofrequency ablation (n = 30). The disease remission rate was 60.0% at 12 months and 18 months and 56.7% at 24 months.
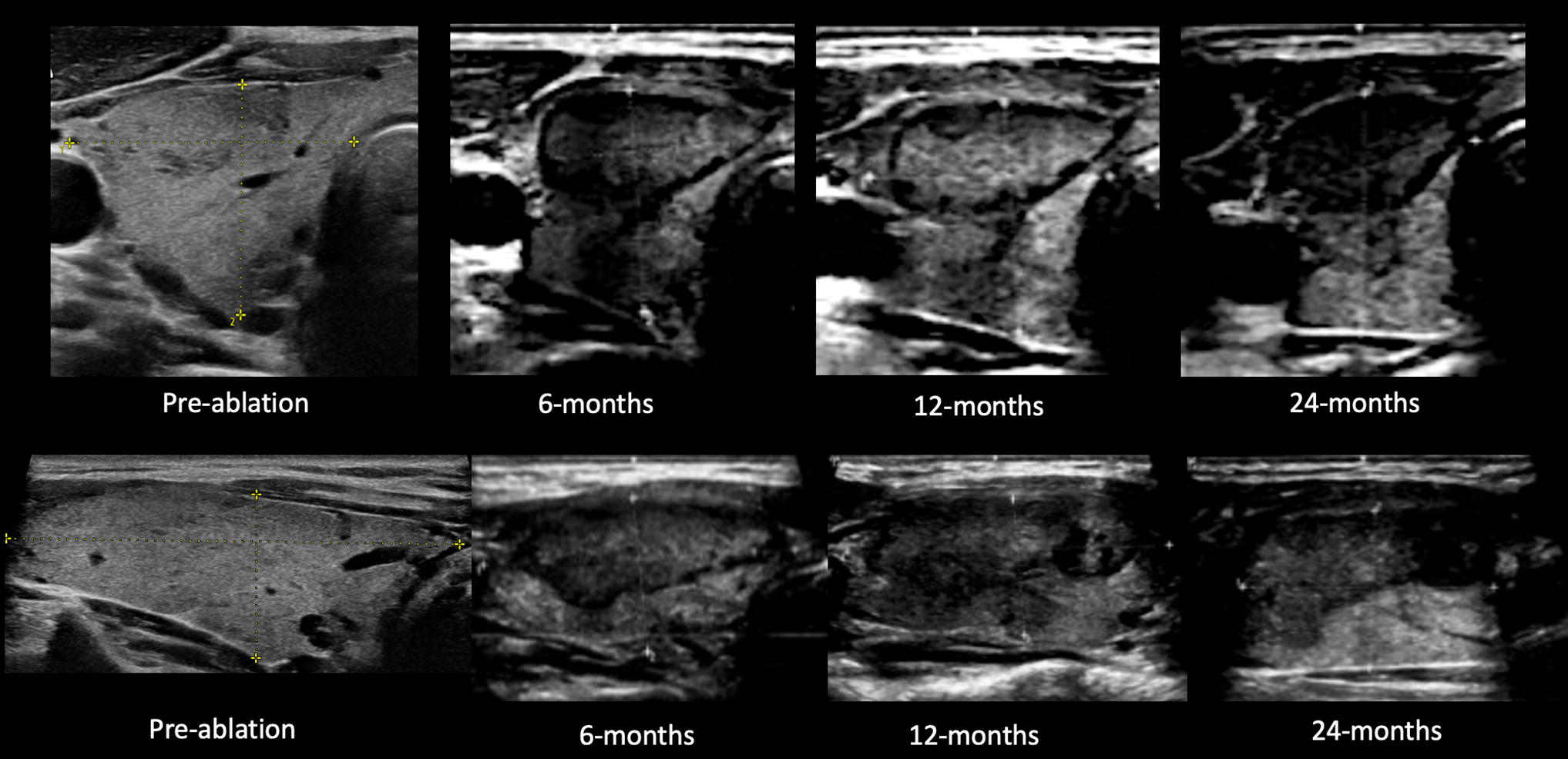
Ultrasound images of the right thyroid lobe of a 36-year-old lady who underwent single-session radiofrequency ablation and remained in remission and euthyroid at 24 months. Top row: transverse view; bottom row: longitudinal view. Note the hypoechoic ablation zones in the post-ablation images.
Factors associated with relapse after single-session RFA
Table 4 compares the baseline characteristics and treatment parameters of patients who remained in remission (Group I) versus those who relapsed (Group II) after single-session RFA. Group I patients had older age (p = 0.044) and smaller total thyroid volume (p = 0.022). Table 5 shows results from univariate Cox regression analysis for factors associated with relapse. Upon multivariate Cox regression analysis, total thyroid volume was the only factor significantly associated with relapse (p = 0.012). Figure 4 shows the Kaplan–Meier analysis comparing disease remission rates between patients with total thyroid volume <20 mL (n = 9) and ≥20 mL (n = 21). At 24 months, all 9 patients with total thyroid volume <20 mL had 100% disease remission, whereas for the remaining 21 patients with total thyroid volume ≥20 mL, the disease remission rate was 35.1% (p = 0.007). The largest gland among the 17 patients in remission had a total thyroid volume of 45 mL.
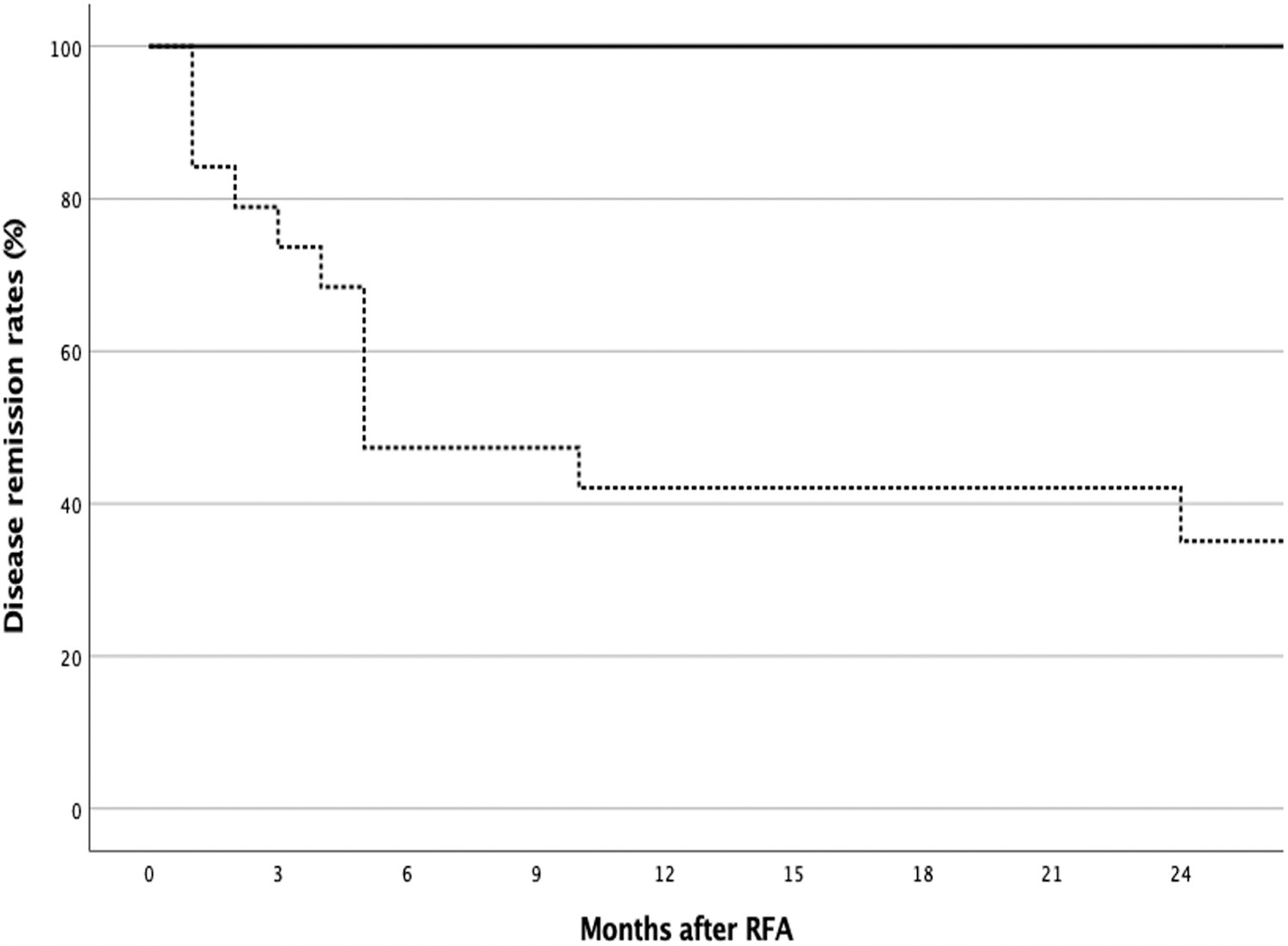
Kaplan–Meier analysis with log-rank test comparing the remission rates between patients with total thyroid volume <20 mL (solid line, n = 9) and ≥20 mL (dotted line, n = 21) (p = 0.007). At 24 months, disease remission rate was 100% for volume <20 mL and 35.1% for volume ≥20 mL.
Comparison of Patient Characteristics and Treatment Parameters Between Those Who Remained in Remission (Group I) and Those Who Relapsed (Group II) After Single-Session Radiofrequency Ablation for Persistent/Relapsed Graves’ Disease at 24 Months
BMI, body mass index.
Univariate Cox Regression Analysis of Factors Associated with relapse After Single-Session RFA for Persistent/Relapsed Graves’ Disease
Bold and italicized values represent statistically significant results.
Reading taken from 24 months for those in remission and at time of relapse for patients who suffered a relapse.
anti-Tg, anti-thyroglobulin antibody; anti-TPO, anti-thyroid peroxidase antibody
Definitive treatment for relapses after single-session RFA
Two patients with relapse after single-session RFA underwent open total thyroidectomy as definitive treatment. Intraoperatively, adhesions of the thyroid capsule with the strap muscles were noted at the isthmic region, where the RFA electrode had previously passed through. No adhesions around the recurrent laryngeal nerves and carotid sheath were noted during dissection. Both patients had smooth recoveries from surgery without VCP or hypoparathyroidism. The gross appearance and histopathological findings from one patient are shown in Supplementary Figures S1 and Figure S2, respectively. Six patients with early relapse after single-session RFA underwent a second session of RFA within 6 months of the first RFA. At a median follow-up of 17 months (IQR 7–23) after the second RFA, three remained in remission (50%) and three had relapse and were restarted on ATD. The remaining five patients who did not receive surgery or re-ablation were resumed on ATD. None of the patients received RAI.
Discussion
To the best of our knowledge, this study reports results from the largest cohort of patients with the longest follow-up time after whole-gland RFA for the treatment of relapsed GD. With all patients completing 24 months follow-up and a median follow-up of 31 months, the disease remission rate was 60.0% at 12 months and 56.7% at 24 months. Upon multivariate analysis, a larger total thyroid volume was the only significant factor associated with relapse. A 100% disease remission at 24 months could be achieved if the total thyroid volume is <20 mL versus only a 35.1% disease remission for those with a total thyroid volume ≥20 mL. (Fig. 4) These findings highlight the importance of careful case selection (smaller glands) for the best results from RFA. One hypothesis for this observation is that, as areas near the danger triangle and great vessels were less well-ablated for safety reasons, the viable remnant for larger glands would proportionately be larger, contributing to relapse. In addition, similar to large nodules that typically require additional RFA sessions for satisfactory results, 13,14 the deep portions of larger glands were more difficult to treat because of the larger amount of microbubbles generated from large-area ablation. The fact that 50% of patients who underwent an additional session of RFA remained in remission may further strengthen these hypotheses. Shrinkage of the gland from the first session, and dispersion of microbubbles and hence improved visualization of unablated zones, may facilitate effective ablation in the second session. Nevertheless, whether durable remission could be achieved in patients with two-session RFA would require longer-term evidence.
It is important to note that, according to the literature, the mean total thyroid volume in patients with GD ranged from 24.8 to 40.2 mL. 15 –19 Therefore, although the largest gland that was rendered into remission by RFA was 45 mL in volume, which was slightly more than the average size of a gland that causes GD, the majority of our patients actually had smaller glands (median 23 mL). Our results showed that smaller glands (<20 mL) responded better than larger glands. Although age was not found to be a significant factor associated with remission, the responders were also older than the non-responders (40 ± 10 vs. 33 ± 9). These overall results suggest that good candidates for RFA are patients with small glands and the age range of 30–50 years.
Our study provided insight into the disease course following RFA. All but one relapse occurred before 12 months, suggesting a more stable disease course 1 year after ablation. However, the occurrence of one relapse at 24 months would indicate that there is a need for continued surveillance even at a later stage of the disease. Another unique aspect of our study is the histopathological findings obtained from surgery for relapse after RFA (Supplementary Fig. S1 and Fig. S2). Under the microscope, it was evident that RFA induced tissue necrosis within thyroid parenchyma characteristic of GD. There were no viable cells within the ablation zone, which only exhibited residual colloid admixed with fibrin. The effect of RFA seemed to be limited to the ablation zone, as there were no changes atypical of GD outside the fibrous capsule surrounding the ablation zone. It is important to know whether the lack of changes or resolution from GD features on histology is unique to patients with relapse or is universal to all GD patients who received RFA. In the latter situation, the volume of hyperfunctioning tissue reduced by RFA and the volume of viable tissue remaining would determine whether the patient goes into a euthyroid remission state, a hypothyroid remission state, or relapse. The concept of reducing pathological thyroid tissues to treat GD has been examined previously with various methods, such as HIFU 4,5 and thyroid arterial embolization, 20 –22 with encouraging results. From our study, RFA appears to be another viable option using this concept. The nine patients (30%) with a partial response to RFA may suggest the potential role of a second RFA to further reduce viable hyperfunctioning gland tissue and hence achieve GD control.
It is valuable to note that surgery could be safely performed even if there is a relapse after RFA. Adhesions were mainly found at the thyroid isthmus, and critical areas near the recurrent laryngeal nerve and carotid sheath were spared from adhesions. This is because, using the trans-isthmic approach during RFA, one would have avoided ablation close to these vital structures.
We would like to emphasize that we fully acknowledge the merits of conventional treatment, such as surgery, and we do not intend to suggest RFA as a replacement but rather as a potential alternative for well-selected patients. As shown in our study, larger glands respond less well to RFA, and they are probably best treated with surgery. However, in our clinical practice, we do encounter a significant number of patients with relapsed GD who have smaller glands and are reluctant to undergo surgery because of potential issues with scars, lifelong thyroxine replacement, and hypoparathyroidism; wish to avoid general anesthesia; and wish for a quick recovery. The many advantages of RFA, as shown in thyroid nodule ablation, have prompted our efforts to investigate its novel use for GD. First, RFA is considered scarless. A typical RFA treatment for GD requires at most two to four punctures, which become invisible after a few weeks, in our experience. A scar is inevitable for surgery, and it has been shown to impair health-related quality of life after thyroid surgery in numerous studies. 23 Another advantage of RFA is the potentially reduced risk of hypoparathyroidism. In our study, none of our patients suffered from hypoparathyroidism, when compared with the 11.2% rate of permanent hypoparathyroidism (PH) after total thyroidectomy in the community setting. 24 Surgical PH is associated with serious adverse cardiovascular, renal, and psychosocial events, 25 and the avoidance of PH by RFA presents a clear advantage. The entire ambulatory setting of RFA is also attractive to patients who seek a quick recovery from treatment. From our results, we found that a subgroup of patients with smaller glands could both benefit from remission rendered by RFA and avoid the disadvantages of surgery.
When compared with single-session RAI done in our locality and Asia, single-session RFA achieved comparable remission rates at 12 months (60% vs. 63%). 26 –28 RFA carries no radiation and therefore precludes the fear of increased risk of malignancy. 29 RFA does not require isolation afterward, a specific and genuine issue for our locality, which has crowded living conditions. Longer duration of ATD use has been shown to achieve better remission rates (80% after 80 months of ATD) than the conventional duration of 18–24 months. 30 However, noninterruption of ATD for ≥60 months is recommended if long-term ATD is chosen to treat persistent GD. 30 Ensuring full compliance and stringent follow-up could be challenging to both the patient and the doctor. On the contrary, RFA is a one-off procedure. Finally, RFA can be considered an organ-preserving procedure. It has the lowest rate of hypothyroidism (6.7%) when compared with surgery (100%) and RAI (41%). 31 We acknowledge that the long-term rate of hypothyroidism after RFA remains to be elucidated by longer follow-up. Nevertheless, RFA could render half of our patients drug free for at least 2 years, an advantage unique to surgery and long-term ATD. The above advantages of RFA make it an attractive option for well-selected patients who do not find surgery, RAI, or long-term ATD acceptable.
Finally, our study showed that RFA was well tolerated and safe in our cohort. All patients could be discharged on the same day, and none suffered from VCP, skin burn, hematoma, or severe thyrotoxicosis. We find adding sedation beneficial to patient experience and using intraoperative laryngeal ultrasonography to monitor vocal cord function highly reassuring for this bilateral procedure. 9,10
Several limitations should be acknowledged. First, we have a small sample size, and there is a lack of a control group for comparison. Second, this is a highly selected cohort, and only 30.0% of our patients were eligible. However, as we are a tertiary surgical unit, a large number of referrals were based on strong surgical indications, for example, a very large goiter, GO, and suspicion of thyroid malignancy. More patients with smaller glands will likely be eligible in the community setting. Nevertheless, we acknowledge that the stringent exclusion criteria would have reduced the generalizability of the technique. As there is no literature on this novel treatment, we find it more appropriate at this stage to exclude patients with strong indications for surgery. More evidence on safety and efficacy is required before expanding the trial to other patients, for example, those with moderate ophthalmopathy. Third, we acknowledge that whole-gland RFA for relapsed GD is a highly technically demanding procedure requiring a high level of expertise and technique. This may again limit the generalizability of the procedure. At the current stage, where evidence is still accumulating, we suggest the procedure to be done in highly experienced centers that can perform both high-quality thermal ablation and high quality, high-volume thyroid surgery in case of treatment failure by RFA. Fourth, postoperative anti-TSHR was not measured. Changes in anti-TSHR levels may have implications on post-procedural changes in ophthalmopathy and thus would be valuable to study. Fifth, the presence of functional thyroid remnants in euthyroid patients after RFA raises concerns about the risk of relapse in the future. Longer follow-up would be required to examine the durability of single-session RFA and also two-session RFA for treating GD.
Conclusion
Single-session RFA of the thyroid gland led to disease remission in a highly-selected group of patients with relapsed GD. Smaller total thyroid volume may be a favorable factor associated with disease remission after RFA. The durability of RFA treatment and the results of this study need to be confirmed with a long-term clinical trial.
Footnotes
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available, but they are available from the corresponding author upon reasonable request.
Authors’ Contributions
M.H.M.F.: Patient recruitment, data collection, and article writing. Y.L.: Patient recruitment, data collection, and article review. K.K.W.Y.: Pathology review and article review. B.H.H.L.: Patient recruitment, data collection, and article review and editing.
Author Disclosure Statement
The authors have no related conflicts of interest to declare.
Funding Information
The authors received no sponsorship. Equipment was provided by the authors’ institution.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2