
Abstract
Background:
Population-based studies that examine the associations between hyperthyroidism and cancer risk have yielded inconsistent results. It remains unclear whether the risks of different cancers increase in patients with Graves’ disease (GD) who received antithyroid drugs (ATDs) as initial treatment. We aimed to determine whether cancer risk increases in patients with GD, compared with controls.
Methods:
This nationwide retrospective cohort study utilized data from the National Health Information Database of South Korea. We included 29,502 patients aged >20 years with GD, who received ATDs as initial treatment, and 57,173 age- and sex-matched controls. The primary outcome was the incidence of various types of cancers. Hazard ratios (HRs) with confidence intervals (CIs) for cancer risk were estimated using Cox proportional hazards models. We also analyzed HR by follow-up period since the diagnosis of GD, accounting for surveillance effect.
Results:
The risk of biliary tract and pancreatic cancers (HR: 1.41, CI: 1.24–1.60), thyroid cancer (HR: 15.51, CI: 12.29–19.57), prostate cancer (HR: 1.48, CI: 1.28–1.71), and ovarian cancer (HR: 1.31, CI: 1.13–1.52) was elevated in the GD group than in the control group even after the first year of follow-up was excluded. The increased risk of these cancers persisted after a follow-up period of more than 5 years. The risk of thyroid cancer in patients with GD was higher during the initial follow-up period (1 to <2 years) (HR: 19.35, CI: 7.66–48.87) compared with that in the follow-up period exceeding 2 years. The cancer risk estimates remained significant after excluding patients with GD who underwent subsequent radioactive iodine therapy.
Conclusion:
In this large-scale population-based study, GD was associated with increased risks of biliary tract and pancreatic, prostate, ovarian, and thyroid cancers. The increased risk of thyroid cancer, particularly during the initial follow-up period, may be a surveillance effect.
Introduction
Graves’ disease (GD) is an autoimmune thyroid disease, accounting for the most common underlying disease of hyperthyroidism in iodine-sufficient populations. 1 The initial treatment options for GD consist of antithyroid drugs (ATDs), radioactive iodine (RAI) therapy, and thyroid surgery. 2 Historically, initial ATD treatment has been preferred in European and East Asian countries, 3 but RAI has been preferred in the United States. 4 However, ATDs currently constitute the most common initial treatment for GD worldwide, 5 with the recent decrease in the use of RAI in the United States. 6
Thyroid hormones play major roles in various physiological processes including growth, differentiation, development, and metabolism. 7 They also modulate the various pathways implicated in tumorigenesis. In vitro and in vivo experiments have revealed effects of thyroid hormones on cancer cell proliferation. These hormones influence the oncogenic PI3K pathway, angiogenesis, and immunoreactivity. 8 –13 Given the biologically plausible roles of thyroid hormones in tumorigenesis, previous population-based studies have sought associations between hyperthyroidism and cancer development. 14 –30 Some such studies have reported increased risks of breast, 14,16,22,23,30 lung, 14,18,30 prostate, 17,18,30 gastrointestinal tract, 20 ovarian, 24 and thyroid cancers 15,16,19,25 in patients with hyperthyroidism but the results have been inconsistent. 21,26 –29 These studies also had certain limitations in that they examined the cancer risks of only a few specific organs and did not comprehensively adjust for confounding factors including smoking and alcohol consumption status, obesity, or comorbidities. 15,16,18 –20,22,23,25 In addition, earlier studies have investigated cancer risks in patients who were primarily treated with RAI, excluding those treated with ATDs, 31 –33 which are the preferred treatments for GD worldwide. Thus, a comprehensive evaluation of the cancer risk in patients with GD who receive ATDs as primary treatment is required. This large-scale, retrospective cohort study aimed to investigate the risks of various cancers in patients with GD receiving ATDs as first-line treatment, compared with controls.
Methods
This study received approval from the Institutional Review Board of
Data source
This study was based on the data recorded from 2003 to 2022 in the National Health Information Database (NHID) of South Korea. The NHID is a public database of the National Health Insurance Service (NHIS) of South Korea, that includes sociodemographic data, the responses to lifestyle questionnaires, national health screening examination information, diagnosis based on the International Classification of Disease (ICD) codes and information on any treatment provided to the entire Korean population. 34 Our cohort was established after considering all medical records in this nationally representative NHIS database.
Study population
Data from patients with GD diagnosed between January 2005 and December 2012 were extracted from the NHID. We defined patients with GD as those who had received ATDs for over 60 days, with ICD codes E050 or E058. This definition aligns with that used in previous epidemiological studies of GD in Korea. 35,36
A 2-year washout period (January 2003 to December 2004) was applied to exclude any previous history of GD or treatment for GD; thus, we identified newly diagnosed cases of GD. The exclusion criteria during the entire study period were as follows: patients aged <20 years or ≥80 years; those with thyroiditis, hypothyroidism, or any other thyroid disorder (E01–4, E051–4, E06); those for whom demographic data were missing; those with any history of cancer (‘C’ codes) before the GD index date; and those on continuous ATDs therapy for <60 days as primary treatment.
The control cohort was also extracted from the NHID using a random number generator. For each patient with GD, two GD-free individuals with available national health screening examination data were randomly selected and matched by age, sex, and index year. To prevent bias from difference in follow-up periods when tracking cancer occurrences, we matched the follow-up periods (index years) of both groups. We applied the identical exclusion criteria to the control cohort before matching them to the GD cohort.
Definitions of outcomes and covariates
Various cancer types were identified based on the diagnostic codes assigned by medical doctors that reflected the possible outcomes. A cancer ‘C’ code greatly affects the insurance cover and available health care benefits; the code is assigned after careful consideration, and the assignment is reliable. The primary outcomes were as follows: esophageal cancer (C15); stomach cancer (C16); lung cancer (C33–4); liver cancer (C22); biliary tract and pancreatic cancers (C24–5); renal cancer (C64, C67); thyroid cancer (C73); colorectal cancer (C19–21); hematological cancers including lymphoma, myeloma, and leukemia (C81–6, C90–5); prostate cancer (C61); breast cancer (C50); and ovarian, uterine, or cervical cancer (C51–8).
The common covariates for all cancers, including demographic and lifestyle data, and basic comorbidities, were considered. These included age (20–44 or 45–79 years), sex, income (lower, middle lower, middle upper, or upper), smoking status (none, ex, or current), alcohol consumption (none, mild-to-moderate, or heavy), the Charlson comorbidity index (0, 1, or ≥2), physical activity status (none, mild, or moderate), body mass index, systolic blood pressure, fasting glucose level, total cholesterol level, and RAI treatment. Anthropometric measurements and laboratory data were based on the national health screening examination data from the NHID and were obtained within 2 years of index date. The covariates were used to construct the final regression model. Follow-up was censored at the end of the study (December 31, 2022).
Statistical analysis
All data manipulation and statistical analyses were performed by a single independent analyst (J.Y.L) who had undergone specialized training by the Health Insurance Review and Assessment Institute focusing on the handling of big data. 37 Continuous variables were compared between the groups using the Wilcoxon rank sum test, and the proportions of all group variables were compared employing the chi-square test. The stratified log-rank test was used to compare the incidence rates of all cancers between the GD and control groups. Cox proportional hazards regression models were used to compute adjusted hazard ratios (HRs) when comparing the GD and control groups. Stratified analyses were performed according to younger/older age (<45 years, ≥45 years) and sex (male or female). In the sub-analyses, comparisons between patients with GD who did not undergo RAI therapy and control group were conducted to support the principal results. The risk of cancer was further analyzed by the duration of ATDs (<2 years, ≥2 years) to assess the possible association between exposure of ATDs and risk of cancer in GD cohort.
The primary outcomes were subjected to sensitivity testing based on the follow-up period since the diagnosis of GD (≥1 year, 1 to <2 years, 2 to <5 years, and ≥5 years) to account for the possibility of surveillance effect. All statistical analyses were conducted using SAS Enterprise Guide version 6.1 software (SAS Inc., Cary, NC, USA). p-Values of <0.05 were considered statistically significant.
Results
Baseline characteristics
In total, 29,502 patients with GD and 57,173 age-, sex-, and index year-matched controls were included during the enrollment period (Fig. 1). Baseline characteristics of the subjects are shown in Table 1. The mean age of the subjects in both groups was 45.8 ± 11.9 years. The mean follow-up period for the entire cohort was 12.4 years.
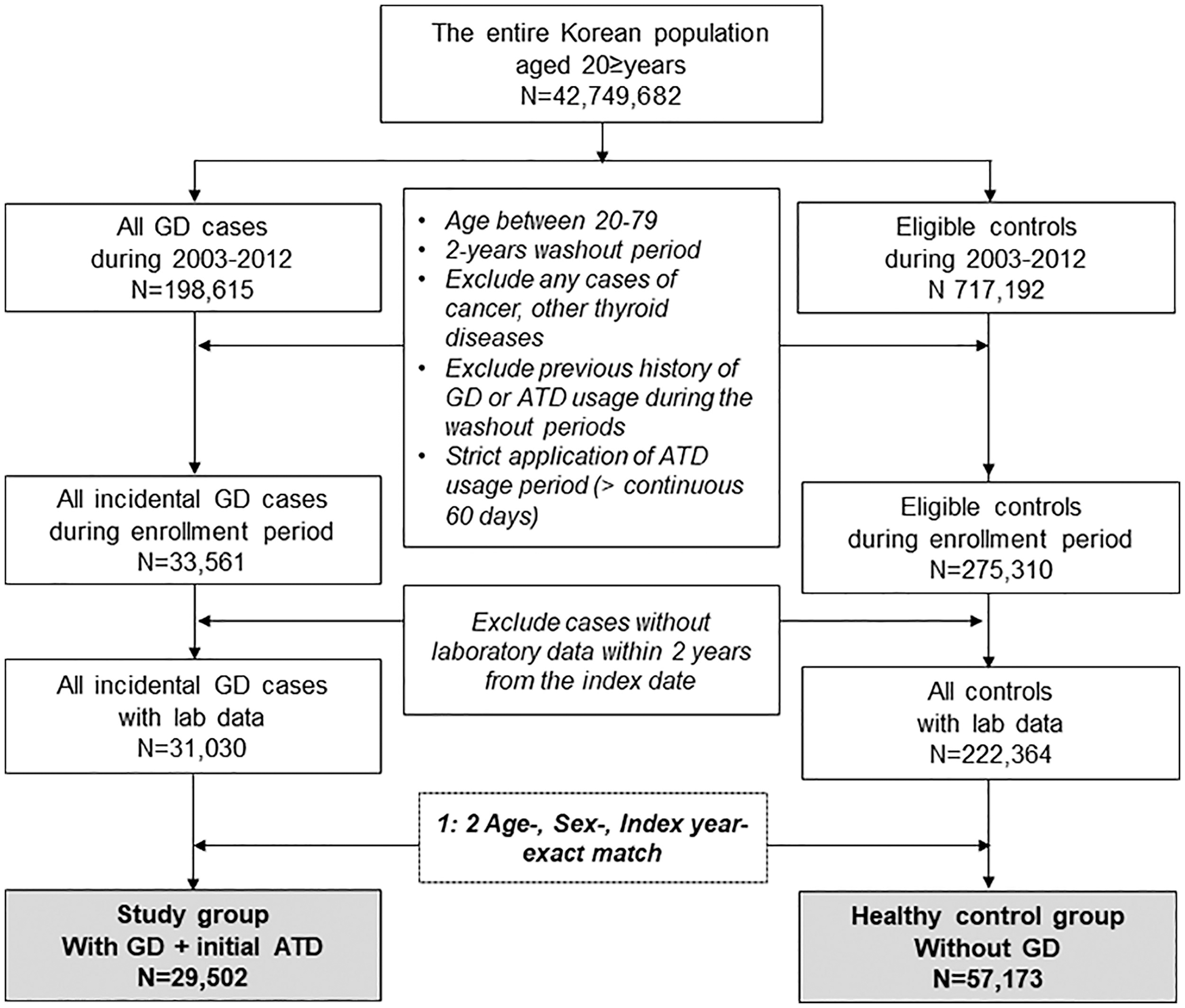
Identifying process and selection of the study cohort. GD, Graves’ disease; ATD, antithyroid drugs.
Baseline Characteristics of Cohort in Each Study Group
CCI, Charlson comorbidity index; BMI, body mass index; BP, blood pressure.
Not available due to nonresponder during questionnaire.
Risk of cancer in patients with GD versus controls
During the follow-up period, 4880 (16.5%) cancer cases were reported in the GD group, and 5566 (9.7%) cancer cases were reported in the control group. In the GD group, there were 610 new liver cancers, 582 biliary tract and pancreatic cancers, 957 thyroid cancers, 416 prostate cancers, and 404 ovarian cancers (Table 2). The incidence rate per 100,000 person-years was 168.46 for liver cancer, 159.89 for biliary tract and pancreatic cancers, 265.02 for thyroid cancer, 281.75 for prostate cancer, and 188.86 for ovarian cancer in the GD group compared with 123.73, 95.61, 12.69, 177.42, and 140.01, respectively, in the control group. In multivariate Cox regression analysis, the risks of these cancers were significantly higher in the GD group.
Cancer Risk in Patients with Graves’ Disease Compared with Age- and Sex-Matched Controls in Whole Cohort
Adjusted by age, sex, income, smoking, alcohol, CCI, physical activity, body mass index, BP, glucose level, and cholesterol level.
Number of events.
Incidence rate was calculated per 100,000 persons.
No., number; IR, incidence rate; PY, person-year; HR, hazard ratio; CI, confidence interval.
In the sex-stratified analysis, the risk estimates were generally similar to those of the entire population and the increased risk remained significant for both sexes (Table 3). The risk of liver and biliary tract and pancreatic cancers associated with GD was higher among females, whereas the risk of thyroid cancer associated with GD was higher among males.
Cancer Risk in Patients with Graves’ Disease and Controls According to Sex
Control cohort was reference group.
Number of events.
Incidence rate was calculated per 100,000 persons.
GD, Graves’ disease.
Stratified analysis by age
Risk of cancer stratified by age group is presented in Supplementary Table S1. The risk of liver, biliary tract and pancreatic, thyroid, and prostate cancers associated with GD was increased in both age groups (<45 years, ≥45 years). However, the association between GD and ovarian cancer was significant only in the younger age group.
Sensitivity testing and sub-analysis
For cancers that were significant in primary analysis, we assessed the risks of developing those cancers based on the follow-up period since the diagnosis of GD (≥1 year, 1 to <2 years, 2 to <5 years, and ≥5 years) (Table 4). After excluding the first year of follow-up, GD-associated risk of biliary tract and pancreatic cancer (HR: 1.41, confidence interval [CI]: 1.24–1.60), thyroid cancer (HR: 15.51, CI: 12.29–19.57), prostate cancer (HR: 1.48, CI: 1.28–1.71) and ovarian cancer (HR: 1.31, CI: 1.13–1.52) remained significant, but the risk of liver cancer did not reach statistical significance. The HR for thyroid cancer was 19.35 (CI: 7.66–48.87) during the early follow-up period (1 to <2 years), but 14.38 (CI: 9.18–22.52) during 2 to <5 years period, and 15.86 (11.93–21.07) after ≥5 years. The increased risk for biliary tract and pancreatic, prostate, and ovarian cancers associated with GD persisted after >5 years of follow-up.
Cancer Risk in Patients with Graves’ Disease and Controls According to Follow-up Period Since the Diagnosis of Graves’ Disease
No., number of events; IR, incidence rate per 100,000 person-years.
In the analysis that excluded all cases who received RAI (n = 1214), the results were very similar to the primary analysis (Supplementary Table S2). The risks of liver cancer (HR: 1.27, CI: 1.13–1.41), biliary tract and pancreatic cancer (HR 1.49, CI: 1.32–1.67), prostate cancer (HR 1.55, CI: 1.35–1.78), and ovarian cancer (HR: 1.22, CI: 1.07–1.41) were significantly higher in the GD group than in the control group. The risk of thyroid cancer was slightly higher in analyses that excluded RAI (HR: 20.83, CI: 16.47–26.34) compared with the overall analysis (HR: 18.45, CI: 14.76–23.08).
In the analysis of HR based on the duration of treatment with ATDs, the risk of cancer was generally similar between patients who were treated for <2 years and those treated for ≥2 years in the GD group (Supplementary Table S3).
Discussion
In this nationwide, population-based, retrospective cohort study, we demonstrated elevated risks of biliary tract and pancreatic, thyroid, prostate, and ovarian cancers in patients with GD compared with controls. The increased cancer risk was also significant in most subgroup analyses by age and follow-up duration and remained significant even after excluding patients who received subsequent RAI.
Previous population-based studies have investigated the associations between hyperthyroidism and cancer risk, but the results have been inconsistent. 14 –30,38 Possible reasons for these inconsistencies include differences in the definition of hyperthyroidism, characteristics of study participants, adjustments for various confounding factors, and types of cancers evaluated. In several prospective cohort studies based on measurement of thyroid hormones, hyperthyroid state was at overall higher risk of solid cancer, 18 lung cancer, 18 breast cancer, 23 and prostate cancer, 17,18 compared with those in a euthyroid state. In a Rotterdam prospective cohort study, a positive relationship was observed between free thyroxine levels and the risk of overall solid cancers, as well as lung and breast cancer. 14 These studies propose a causal link between hyperthyroidism and cancer risk. In questionnaire-based studies, self-reported hyperthyroidism was associated with mortality of breast cancer 38 or risk of ovarian cancer. 24 However, other studies found no significant association between hyperthyroidism and risk of breast 21 or liver cancer. 27 Similar to our study, previous register-based studies have shown an increased risk of solid cancer, 30 thyroid cancer, 15,16,19,25 breast cancer, 16,22,30 and gastrointestinal tract cancer 20 in patients with hyperthyroidism. Nonetheless, some found no such association between hyperthyroidism and thyroid cancer 28 or breast cancer, 29 and others even observed a decreased risk of colorectal cancer in patients with hyperthyroidism. 26 However, aforementioned studies have limitations, such as including only selected populations 14,15,21,23,28 (predominantly middle aged to older or postmenopausal patients or only hospitalized patients), focusing on specific organ, 20,21,23,25,27,28 using sample cohort data, 19 and inadequate adjustment for confounding factors and comorbidities. 15,16,18,20,22,25 The present study investigated the various types of cancer in patients with GD among an entire population using a long cohort design and comprehensively considered related factors.
The increased risk of cancer during the early follow-up period of GD likely reflects surveillance effect, while long-term elevated risks may indicate causal association between GD and cancer. In our study, the risk of liver cancer increased in patients with GD during the entire follow-up period, but the association was not significant after excluding the first year of follow-up. Diagnostic workup for accompanying symptoms such as weight loss and abnormal liver function test, as well as for side effects of ATDs may be attributable to the increased detection of liver cancer during the early follow-up period. However, the increased risk of biliary tract and pancreatic, prostate, and ovarian cancers remained significant even after excluding the first year of follow-up and continued to be significant for >5 years of follow-up period. These findings suggest that the association between GD and cancers cannot be solely attributed to the surveillance effect.
Notably, a strong increase in the risk of thyroid cancer was observed in patients with GD compared with that of other cancers, particularly during the early follow-up period similar to findings from previous register-based studies. 15,16,25 Our findings regarding risk of thyroid cancer should be interpreted with caution, considering the epidemiological features related to overdiagnosis of thyroid cancer. In Korea, a national screening program for other common malignancies implemented in the early 2000s has contributed to increased opportunistic examinations for thyroid cancer. 39 Thus, the increase in thyroid cancer incidence in many countries, including Korea, may be attributable to the increased use of ultrasound and imaging tools, enhancing the detection of indolent tumors. 40 For patients with GD, intensive examinations of the thyroid gland are likely performed given the thyroid-related symptoms and goiter, particularly in the early stages of disease. This heightened scrutiny may have contributed to a surge in the incidence of thyroid cancer in patients with GD.
The potential relationship between breast cancer and thyroid dysfunction has long been investigated. Although in vitro studies have shown that thyroid hormones stimulate breast cancer cells via nuclear receptor αvβ3 and interaction with estradiol. 1,41 The results of population-based studies and meta-analyses remain controversial. 16,17,21 –23,42,43 In a 2022 meta-analysis, hyperthyroidism was associated with 1.2-fold higher risk of breast cancer, with the risk being greater in postmenopausal women. 42 However, the included studies in the meta-analysis were heterogenous in terms of measure of risk estimate, treatment modality, number of patients, and the extent of adjusting clinical variables. Our study does not support an association between GD and breast cancer, regardless of age group (<45 years and ≥45 years). Further studies are needed that integrate both pathophysiological and clinical data, such as the use of female hormones, to establish a causal relationship between these diseases.
Regarding cancer risk according to treatment modalities in GD, previous studies have reported an elevated risk of cancer incidence and/or mortality in patients who were treated with RAI, 31,33 but not all studies have found a significant association. 44 Recent meta-analyses have shown that there was no increase in solid cancer mortality in patients across various treatment groups. 45 In patients treated with RAI, a dose–response relationship was observed, but the risk increased only at higher cumulative doses. 45 In this study, cancer risk estimates remained significant even after excluding patients who received subsequent RAI. In addition, cancer risks were generally comparable between those treated with ATDs for >2 years and those treated for <2 years. Taken together, the increased cancer risk in patients with GD is more likely due to the underlying disease rather than an effect of treatment modality.
This study has several strengths lacking in previous studies. First, we included patients with GD aged >20 years who received ATDs as primary treatment. This cohort is representative of patients with GD encountered in current real-world practice. Second, we derived the risks of various cancers in patients with GD unlike previous studies focusing on specific organs. Third, the various stratified analyses ensured the validity of data and reduced the risk of reverse causality. However, our work had several limitations. First, individual data on thyroid hormone tests were lacking; it was not possible to analyze the associations between changes in thyroid function and cancer incidence. Second, reproductive factors such as menopause or fertility status were not adjusted, although we attempted to overcome this limitation by performing an age-stratified analysis (<45 years, ≥45 years) to explore whether the risk varied by menopausal status. The possibility that unmeasured confounders were in play cannot be entirely ruled out, as is true of most observational studies. Third, we performed sensitivity analysis by follow-up period to account for surveillance effect and demonstrated long-term cancer risk; however, further studies that differentiate incidentally detected indolent and more advanced cancers, including molecular profiles and tumor stage, are required to confirm our findings. Finally, this study was performed primarily on a Korean population, our results may have limited generalizability to other population with different genetic susceptibility and environmental factors such as iodine intake.
In conclusion, patients with GD who received ATDs as initial treatment exhibited elevated risks of biliary tract and pancreatic, prostate, ovarian, and thyroid cancers. The increased risk remained significant after excluding the first year of follow-up and continued to be significant 5 years after the diagnosis of GD. The increased risk of thyroid cancer, particularly during the initial follow-up period, may reflect a surveillance effect.
Footnotes
Authors’ Contributions
J.Y.L.: Conceptualization, methodology, formal analysis, interpretation of data, and writing (original draft, review, editing). M.K.L.: Methodology, interpretation of data, and writing (review, editing). J.H.L.: Methodology, interpretation of data, and writing (review, editing). K.K.: Methodology, interpretation of data, and writing (review, editing). K.B.: Conceptualization, interpretation of data, and writing (review, editing). S.Y.S.: Conceptualization, data acquisition, methodology, interpretation of data, and writing (original draft, review, editing).
Role of the Funder
The funder was not involved in the design and conduct of the study.
Data Sharing Statement
Sharing the data underlying this study is restricted for authors because Korean National Health Insurance Service (NHIS) owns the data. Researchers can request access on the NHIS website (https://nhiss.nhis.or.kr). Further details about this process and a provision guide are available at (![]() ).
).
Author Disclosure Statement
The authors have declared no conflicts of interest.
Funding Information
J.Y.L. was supported by faculty grant from
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3