
Abstract
Background:
Brain metastases (BM) are the most common intracranial neoplasms in adults and are a significant cause of morbidity and mortality. The brain is an unusual site for distant metastases of thyroid cancer; indeed, the most common sites are lungs and bones. In this narrative review, we discuss about the clinical characteristics, diagnosis, and treatment options for patients with BM from differentiated thyroid cancer (DTC).
Summary:
BM can be discovered before initial therapy due to symptoms, but in most patients, BM is diagnosed during follow-up because of imaging performed before starting tyrosine kinase inhibitors (TKI) or due to the onset of neurological symptoms. Older male patients with follicular thyroid cancer (FTC), poorly differentiated thyroid cancer (PDTC), and distant metastases may have an increased risk of developing BM. The gold standard for detection of BM is magnetic resonance imaging with contrast agent administration, which is superior to contrast-enhanced computed tomography. The treatment strategies for patients with BM from DTC remain controversial. Patients with poor performance status are candidates for palliative and supportive care. Neurosurgery is usually reserved for cases where symptoms persist despite medical treatment, especially in patients with favorable prognostic factors and larger lesions. It should also be considered for patients with a single BM in a surgically accessible location, particularly if the primary disease is controlled without other systemic metastases. Additionally, stereotactic radiosurgery (SRS) may be the preferred option for treating small lesions, especially those in inaccessible areas of the brain or when surgery is not advisable. Whole brain radiotherapy is less frequently used in treating these patients due to its potential side effects and the debated effectiveness. Therefore, it is typically reserved for cases involving multiple BM that are too large for SRS. TKIs are effective in patients with progressive radioiodine-refractory thyroid cancer and multiple metastases.
Conclusions:
Although routine screening for BM is not recommended, older male patients with FTC or PDTC and distant metastases may be at higher risk and should be carefully evaluated for BM. According to current data, patients who are suitable for neurosurgery seem to have the highest survival benefit, while SRS may be appropriate for selected patient.
Introduction
Distant metastases occur in <10% of patients with differentiated thyroid cancer (DTC) but represent the primary cause of DTC-related death, with an overall survival (OS) rate from the detection of distant metastasis of 42% at 10 years, 33% at 15 years, and 29% at 20 years. 1 Metastases from papillary thyroid cancer (PTC) involve most frequently cervical lymph nodes, while follicular thyroid cancer (FTC), oncocytic thyroid carcinoma (OTC; previously known as Hurtle cell carcinoma [HCC]), and poorly differentiated thyroid cancer (PDTC) tend to metastasize to distant sites. 2 The most common sites are lungs and bones, involved in 49% and 25% of cases, respectively. 1 Other sites of distant metastases are rare, or relatively rare, and involve the brain, liver, adrenal glands, kidneys, pancreas, stomach, and submandibular glands. 3 –5 Among these rare metastatic sites, the most frequent locations are brain, skin, and liver. 6,7 Population-wide, brain metastases (BM) are the most common intracranial neoplasms in adults and are a significant cause of morbidity and mortality. 8 Population-based studies show incidence rates of BM ranging from 8.3 to 14.3 per 100,000 person years. 9 The type of cancer that most frequently metastasizes to the brain is lung cancer (19.9%), followed by melanoma (6.9%), renal cancer (6.5%), breast cancer (5.1%), and colorectal cancer (1.8%). 8 As previous stated, the brain is an unusual site for distant metastases of thyroid cancer (TC), and BM typically occur in older patients with more advanced disease. 10 Therefore, routine screening for BM in all patients with TC is not widely recommended. 11 The choice of treatment in patients with BM of DTC remains still controversial. The 2015 American Thyroid Association (ATA) guidelines on DTC recommend surgical resection and stereotactic external beam radiotherapy (EBRT), while radioiodine (RAI) therapy can be considered in BM able to concentrate RAI. 12 In this review, we discuss clinical characteristics, diagnosis, and treatment options for patients with BM from DTC.
Clinical characteristics
BM from TC occur in ∼0.9–1.5% of all patients with DTC and in 4.5–18% of patients with DTC with other distant metastases. 10,13 BM can be diagnosed either because of symptoms or during imaging performed for treatment.
While BM from DTC are typically associated with older patients (>55 years), studies indicate that they can also occur in younger individuals. 11,14 –20 Regarding sex, most studies show a higher frequency of BM in females compared with males, which can be attributed to the higher incidence of DTC in females. 11,14 –17,20 In terms of histological subtypes, most studies report more cases of BM in patients with PTC than in those with FTC and PDTC. 16 –18,21 However, when considering the underlying prevalence of PTC and FTC, the actual risk of developing BM may be higher in male patients with FTC and PDTC. 7,15 Li et al. 7 described data from the Surveillance, Epidemiology, and End Results database and observed a 10-fold higher frequency of BM in patients with FTC (14/2946, 0.48%) compared with patients with PTC (28/56522, 0.05%). Additionally, the frequency of BM was even higher in patients with PDTC (11/798, 1.55%). In the study by Hong et al., which involved 4683 patients, the prevalence of BM was 4.1% in patients with PDTC, 0.92% in patients with FTC, and 0.18% in patients with PTC. 15 Furthermore, the majority of the patients with BM also had metastases at other sites, particularly in the lungs and bones. 11,14,16 –18
In a previous study carried out in a group of 83 patients with DTC with distant metastases, Van Velsen et al. showed that in 50 patients (60%), the distant metastases were discovered immediately after RAI therapy via the post-therapy whole body scan. Conversely, in the other 33 patients (40%), distant metastatic disease was detected before RAI therapy. Among these 33 patients, the metastases were identified due to symptoms such as pain (30%) during preoperative staging due to a significant tumor burden in the neck (27%), or incidentally on a computed tomography (CT) scan or 18F-fluoro-2-deoxy-D-glucose (FDG)-positron emission tomography (PET) conducted for other reasons (21%). 22 Similarly, BM can be discovered before initial therapy because of symptoms or during additional imaging performed because of extensive disease, but in the majority of the patients, BM were diagnosed during follow-up, 11,15 –18,21 either without symptoms (e.g., because of a brain magnetic resonance imaging [MRI] performed before starting tyrosine kinase inhibitor [TKI]) or due to symptoms. Median time from DTC diagnosis to diagnosis of BM ranges from 11 to 76 months. 11,14 –19,21 However, BM can be diagnosed up to 40 years after initial diagnosis. 11,16
BM can be asymptomatic, but more often symptoms of BM include (focal) neurological deficits, signs of increased intracranial pressure, neuropsychological symptoms, and seizures. 11,19 When these symptoms occur, the treating physician should be alert of the possibility of BM and perform additional investigations with either CT or MRI; the latter is preferred due to its higher sensitivity and specificity. 14
In summary, older male patients with FTC, PDTC, and distant metastases may have an increased risk of BM; most patients experience BM during follow-up and present neurological symptoms.
Diagnosis
When a patient with cancer presents with new onset neurological symptoms or signs of raised intracranial pressure (e.g., seizure and new onset neurological deficits), it is crucial to initiate neurological evaluation, which should encompass neuroimaging. 23 This diagnostic process aims to differentiate between BM and other potential causes of neurological complications, particularly adverse effects resulting from cancer treatments. 23 As previously mentioned, the gold standard for the diagnosis of BM is an MRI without and with contrast agent administration, which is superior to contrast-enhanced CT. 24 –27 Cranial CT is significantly less sensitive than MRI in detecting BM and should be reserved for patients who cannot undergo MRI due to contraindications. 23 PET using FDG is widely used for evaluating patients with known or suspected malignant tumors, but its role for detecting BM is still controversial due the high FDG uptake in the normal brain that limits its sensitivity. 28,29
The current European Association of Neuro-Oncology/European Society for Medical Oncology guidelines 23 recommend screening for BM for patients with lung cancer, with stage IV melanoma and, potentially, also for patients with metastatic breast cancer epidermal growth factor receptor 2 (HER2)-positive and triple-negative. In patients with DTC, routine screening for BM is not recommended due to the low incidence. The majority of patients with DTC in whom BM were discovered had symptoms, 11,14,15,17 –21 but because no screening for BM is usually performed in patients with DTC, it is possible that asymptomatic patients are underestimated in the literature.
The study by Kim et al. investigated the clinical–radiological features of 35 patients with BM (26 of whom had DTC). It was observed that edema was present in 74% of patients, heterogeneous enhancement at MRI in 63%, and hemorrhage in 60% of patients. For the latter, the strongest predictor for BM hemorrhage was larger tumor size. 30
In most cases, the diagnosis of BM from DTC was made by MRI. 16,31 –33 However, in the study of Saito et al., 17 BM were mostly discovered by CT and, in the study of Wu et al., 18 mostly were discovered by RAI scan.
Treatment options
The management of patients with BM from DTC still remains controversial since current therapeutic strategies are based on case reports, and retrospective research with a very limited number of patients and, often, heterogeneous study populations, for example, including patients with DTC, medullary thyroid cancer (MTC), and anaplastic thyroid cancer (ATC) together.
Until now, there is not clear evidence for neurosurgery, RAI therapy, TKIs, stereotactic radiosurgery (SRS), whole-brain RT (WBRT), or chemotherapy.
As previously mentioned, the current ATA guidelines 12 recommend that neurosurgery and SRS are the mainstays for the treatment of BM, while RAI therapy can be used if the lesions are able to concentrate RAI. However, this is a weak recommendation based on low-quality evidence. Overall, it is essential to tailor treatment approaches to the patient’s clinical condition. Given the generally poor prognosis, it is important to avoid unnecessary aggressive treatments. Patients with poor performance status are candidates for palliative and supportive care. More intensive local treatments can be advantageous for patients with good neurological status, controlled primary disease, and no systemic disease. 34
Local intensive treatments such as neurosurgery or SRS are recommended for patients with a life expectancy of at least three months and a good performance status. 35 Indeed, the most important prognostic factor for choosing more aggressive treatments was a performance status of ≤2 (according to the Eastern Cooperative Oncology Group [ECOG]). 16,18,21,31,36 Surgery is typically the preferred treatment for patients with a single tumor larger than 3 cm in diameter accompanied by significant edema and mass effect, and it is recommended in patients with BM measuring >4 cm. In contrast, SRS is more suitable for smaller lesions that do not exhibit marked edema or mass effect, as well as for lesions located deep within the brain. 37 –40 Guidelines from the American Society of Clinical Oncology (ASCO), the Society for Neuro-Oncology, and the American Society for Radiation Oncology (ASTRO) consistently indicate surgical resection as the first-line treatment for large BM with mass effect, while SRS alone should be offered to patients with one to four BM, especially smaller than 4 cm. 41 SRS is generally not performed on patients with larger BM because (i) delivering a high dose of radiation precisely to the target area while sparing surrounding healthy tissue becomes challenging, and incomplete treatment may result from a dose distribution that does not adequately cover the entire tumor; (ii) larger BM require higher doses of radiation, increasing the risk of radiation-induced damage to the surrounding brain tissue; and iii) symptoms due to mass effect and increased intracranial pressure require immediate relief and reduction in tumor burden, which only surgery can quickly achieve. 42 The optimal treatment for patients with five or more BM remains controversial due to the lack of published prospectively randomized data. 42 ASTRO guidelines conditionally recommend SRS for patients with 5–10 BM who have a performance status of ECOG ≤2. Conversely, for patients with a favorable prognosis but not eligible for neurosurgery or SRS (e.g., performance status ECOG 3–4), WBRT is considered the first line of treatment. 42 Despite these recommendations, no study has demonstrated that SRS warrants improved survival compared with WBRT in patients with 5–10 BM, but SRS has shown a lower rate of posttreatment adverse effects. 43 –45
Neurosurgery
The purpose of neurosurgery is to debulk BM, relieve vasogenic edema, and achieve local control of lesions, therewith improving neurological symptoms and overall patient survival. 46 –48 Neurosurgery is typically performed in BM-associated symptoms resistant to medical treatment, particularly in patients with good prognostic factors and larger lesions, and should be considered for patients with a single BM in a surgically accessible location, especially in controlled disease at the primary site without other systemic metastases. 34,49 –51 Patients with multiple BM and/or uncontrolled systemic disease are less likely to benefit from surgery unless the remaining disease is controllable via other measures. 41 Despite the aforementioned potential benefit, neurosurgery carries risks of adverse events, including some of the most common: hematoma, cerebrospinal fluid leak, cerebral infarction, hydrocephalus, and deep venous thrombosis. 52
Numerous studies have identified neurosurgery as an independent factor associated with improved outcomes in patients with BM from DTC. 10,15,53 In their multivariable Cox regression analysis, Hong et al. 15 included variables such as histological type, metastatic site, and surgical resection, observing that surgical resection independently contributed to better survival (hazard ratio (HR) = 0.13, [confidence interval: 0.02–0.92]; p = 0.042). Similarly, Chen et al., 47 incorporating factors such as metastatic sites (lung and bone) and types of intervention (RAI, neurosurgery, SRS, WBRT) in their multivariable model, demonstrated that neurosurgery was an independent prognostic factor for solitary intracranial metastases of DTC (p = 0.014).
Current data on the survival benefit of neurosurgery are inconsistent. Some studies have documented a nonstatistically significant trend toward longer survival in patients who underwent neurosurgery. For instance, Gomes-Lima et al. 16 observed that 10 out of 24 patients who underwent neurosurgery had a median survival time of 27.3 months compared with 6.8 months for those who did not undergo surgery. In the study by Lee et al., 21 the median survival time was 33 months for those who underwent surgical resection (n = 6), whereas it was 1 month for those who had no surgical treatment (n = 4). Similar findings were reported by McWilliams et al., 54 who observed a longer survival after surgical resection of BM (20.8 months vs. 2.7 months for patients without surgery). Overall, these findings may be due to a limited number of patients or the inclusion of histological types other than DTC. In contrast, some studies have demonstrated a clear benefit of neurosurgery. In the study of Choi et al., 31 a better median OS was achieved in patients who underwent neurosurgery or SRS (30.7 compared with 5 months). In the study by Chiu et al., 10 patients who underwent surgical excision had a median disease-specific survival of 22 months, in contrast to 3 months for those who did not have surgery. Focusing specifically on patients with a single brain metastasis, the median survival was 25.2 months for those who had surgery, compared with 2.4 months for those who did not (Table 1). The same was true for the study of Wu et al., 18 Osborne et al., 56 and Yoo et al. 33 (Table 1). In the latter study, neurosurgery showed a statistically significant survival benefit in the subgroup of patients with ≤3 BM. This finding is in line with other studies. Indeed, a greater number of BM had an impact on prognosis 57 : most studies found that patients with ≤3 BM had a higher median OS than patients with >3 BM. 17,31,33,56
Selected Studies on the Clinical Features at Diagnosis and Outcome After Therapies in Patients with Brain Metastases from Thyroid Cancer
Study quality evaluated by the National Heart, Lung, and Blood Institute of the National Institutes of Health for quality assessment for case series study.
p value <0.05 compared with the no treatment group.
BM, brain metastases; F to M, female to male; FTC, follicular thyroid cancer; NA, not available; OS, overall survival; OTC, oncocytic thyroid carcinoma; PDTC, poorly differentiated thyroid cancer; PTC, papillary thyroid cancer; SRS, stereotactic radiosurgery; TC, thyroid cancer; TKI, tyrosine kinase inhibitors; WBRT, whole-brain radiotherapy.
Radiotherapy
SRS is a focused ablative radiation treatment capable of delivering a high dose of radiation in a single fraction to a precisely defined target. 55 This focused and ablative approach emulates the impact of surgical resection but in a minimally invasive way. It is indicated for small-sized BM (≤2 cm) and serves as an alternative when surgery is not feasible. For example, this includes lesions situated in critical or challenging areas of the brain that cannot be surgically removed, or in patients deemed unsuitable for surgery due to underlying health conditions. 55,58 –60
Compared with WBRT that use larger radiation fields, SRS showed a better cognitive function preservation rate. 61,62 In a randomized clinical trial 61 (including patients with cancer from primary sites other than the thyroid), cognitive deterioration at 3 months after treatment was observed in 64% of patients treated with SRS alone, compared with 92% when SRS was combined with WBRT (p < 0.001). Moreover, patients treated with SRS alone exhibited better quality of life, including overall quality of life and functional well-being. Similarly, the authors of a multicenter, randomized, controlled, phase 3 trial 62 (including patients with cancer from primary sites other than the thyroid) documented that patients treated with SRS developed cognitive deterioration at 6 months less frequently than those who received WBRT (52% vs. 85%, respectively, p < 0.001). Preservation of cognitive function can be of particular importance for patients having cancers with a relative favorable prognosis, such as a TC. 63 The use of SRS in patients with BM from DTC showed an excellent safety profile (among the most common adverse effect: headaches, seizures, cognitive deficits, nausea and vomiting, and transient sensory symptoms). 64 In the studies of Bunevicius et al. 63 and Byun et al., 65 none of the patients with TC, respectively, 42 (papillary or follicular) and 19 (differentiated, medullary, or anaplastic), experienced adverse radiation events. Several studies have showed a clinical benefit, but only a few of these have demonstrated a significant improvement in OS. 16,66 A study of 24 patients showed that the median OS was longer in patients who underwent SRS than for those who did not (52.5 vs 6.7 months). 16 Another study with 23 patients with TC, in which pathology was available only for 12 of them, showed that patients receiving SRS had a median OS of 37.4 months as compared with 12.3 months for those treated without SRS. 66 Overall, SRS showed a high local control of BM. In the study of Kim et al., 67 the authors reported a local control rate of 96% (25 of 26 BM), with a median OS of 33 months after SRS; however, in this study, only 7 patients had DTC. More robust data were reported by Bunevicius et al. 63 : in 42 patients with DTC, local control was documented in 96% of the BM treated with SRS. Only one study compared patients treated with SRS or WBRT, and, although the series also included patients with ATC, patients with BM treated with SRS had a longer median OS than patients who received WBRT (10.7 months vs. 1.8 months). 57
WBRT has traditionally been the gold standard in the treatment of patients with BM. However, recent clinical trials have shown that although it may reduce the incidence of local recurrences, WBRT does not significantly improve OS or quality of life in oncological patients with BM. 68 –72 Moreover, patients treated with WBRT usually show a high incidence of radiation-induced dementia (52% for patients treated with SRS plus WBRT and 24% for patients treated with SRS alone) due to irradiation of healthy brain tissue that may occur from 6 to 12 months after therapy. Other radiation-induced events include fatigue, alopecia, dermatitis, and optic neuropathy. 73,74 Due to these potential side effects combined with the controversial efficacy, WBRT should be indicated for the treatment of patients with multiple BM and too large in size for SRS. 16,51,68,73,75 –77 Specifically, WBRT was not associated with improved OS in patients with BM from DTC. 10,16,18,54,56 In the retrospective study of Gomes-Lima et al., 16 10 patients received WBRT with no difference in survival compared with patients not receiving this therapy (21.3 vs. 19.1 months); the same applies to the studies of Wu et al. 18 in which the median OS was of 33.0 months for 12 patients treated with radiotherapy (compared with 26.0 months in untreated patients) and of 19.0 months in the study of Osborne et al. 56 in which 63 patients underwent to WBRT (compared with 11.0 months in 14 untreated patients).
Overall, SRS has been shown to be a minimally invasive and safe treatment modality, associated with a low risk of toxicity and able to ensure high local control of BM, and should be considered for patients who are not eligible for surgery due to comorbidity or with advanced intracranial disease. Although the use of WBRT for BM has decreased with the advent of SRS and targeted therapies, modern techniques have enhanced its tolerability. To mitigate neurocognitive deficits, particularly those affecting episodic and verbal memory due to hippocampal irradiation, strategies such as the use of memantine (a neurocognitive protective agent) and hippocampus-avoidance WBRT are increasingly adopted. 78 However, caution is warranted before drawing firm conclusions, as studies on WBRT often involve small sample sizes, and underpowered comparisons are a common limitation in this field.
Systemic therapy
According to current ATA guidelines, 12 TKIs should be considered for patients with radioiodine–refractory (RAI-R) DTC who have metastatic, rapidly progressive, symptomatic, and/or imminently threatening disease that cannot be controlled locally by other methods. Lenvatinib and sorafenib are multikinase inhibitors that were approved by the European Medicines Agency and Food and Drug Administration (FDA) for the treatment of progressive RAI-R TC based on large phase III studies that showed a significant improvement in PFS with these drugs compared with placebo. 79,80 Another TKI, cabozantinib, demonstrated a prolonged PFS in patients with progressive RAI-R DTC who had previously received a vascular endothelial growth factor (VEGF) inhibition therapy, with a significant risk of disease progression or death. 81
Despite the frequent use of these drugs in patients with RAI-R metastatic DTC, their use in patients with BM from DTC remains still very controversial due to insufficient data.
In the case report of Shen et al., 82 a patient with RAI-R metastatic (brain and lung) and progressive FTC was treated with sorafenib for 14 months because the patient was not a good candidate for surgery and had a poor response to SRS. After 1 year, a partial response of BM was achieved. In the case report of Krajewska et al., 83 a patient with RAI-R PTC having bone, lung, and BM was first treated with neurosurgery, WBRT, and thalidomide. Then, the latter was discontinued due to disease progression and, subsequently, was treated with sorafenib for 16 weeks resulting into stable disease. In another study, the use of lenvatinib in three patients allowed a stabilization of BM for 2, 4, and 5 years, respectively. 11 Although very limited, these data can suggest the ability of these drugs to act at the level of the central nervous system.
Larotrectinib is a highly selective inhibitor of tropomyosin-receptor kinase A (TRKA), tropomyosin-receptor kinase B (TRKB), and tropomyosin-receptor kinase C (TRKC) and was approved for the treatment of solid tumor harboring neurotrophic tyrosine receptor kinase (NTRK) fusion. Beyond TC, there are very solid data on central nervous system (CNS) activity and efficacy of NTRK inhibitors, for example, patients with lung cancer, sarcoma, breast cancer with metastatic intracranial disease, and for primary CNS tumors. 84 –89 Preliminary data about the efficacy of larotrectinib seem to demonstrate that it is able to cross the blood–brain barrier (BBB) and be effective for the treatment of CNS metastases from TC. 90,91 Pitoia 92 reported a case of a woman with a multi-metastatic advanced RAI-R PTC who progressed after sorafenib and lenvatinib treatment and then received larotrectinib after the detection of NTRK gene fusion; during larotrectinib treatment, radiological imaging showed a complete response and all target lesions disappeared.
Selpercatinib, a novel adenosine triphosphate (ATP)-competitive, highly selective small-molecule Rearranged during Transfection (RET) kinase inhibitor, demonstrated durable efficacy in RET-mutant MTC and previously treated RET fusion-positive nonmedullary TC. Among patients with nonmedullary TC, six were affected by BM, suggesting that, similar to larotrectinib, selpercatinib can penetrate the BBB and potentially be effective in treating patients with BM. 93 More robust data on the efficacy of selpercatinib for the treatment of BM come from studies on non-small cell lung cancer. These studies confirmed that selpercatinib has robust and durable intracranial efficacy in patients with RET fusion-positive cancers. 94 –96
The BRAFV600E mutation is the most prevalent oncogenic mutation in PTC, occurring in around 60% of patients. 97 Similarly, BRAFV600E is the most frequently observed actionable mutation in ATCs, occurring in 50–70% of cases. 98,99 In May 2018, the FDA approved the combination of BRAF/MEK inhibitors, dabrafenib, and trametinib, for patients with ATC with the BRAFV600E mutation. 98 Retrospective and prospective studies of single-agent BRAF inhibitors such as dabrafenib and vemurafenib in BRAFV600E -mutated PTC showed safety and clinical benefit, although the effect on the CNS remains unknown as there is a lack of reports on the use of these drugs in patients with BM from DTC. 81,100 Available data on the use of BRAF/MEK inhibitor combination against BM from melanoma support the efficacy of these drugs also for the treatment of BM in patients with TC. 101 –103
Only one retrospective series showed that patients with BM treated with TKI had a higher survival compared with untreated patients (27.2 vs. 4.7 months) and that TKI reduced the odds of death by ∼73%. 16
Historically, for patients with metastatic DTC that progresses despite the standard therapy, the role of chemotherapy has been limited because a poor or no response is common, causing limited effectiveness. The limited benefit of chemotherapy has been attributed to the low proliferation rate of DTC as compared with other tumors. 104 A systematic review showed that none of the studies analyzed in the research, that assessed monotherapy alone, achieved a complete response, while the complete response rate was 3.2% for combination chemotherapy. 105 For patients with BM, Chiu et al. 10 found that chemotherapy did not increase disease-specific survival. McWilliams et al. 54 described three patients treated with doxorubicin-based chemotherapy, but none of the patients achieved an objective response in either their brain lesion or extracranial disease. In the study of Samuel et al., 106 the use of chemotherapy with adriamycin, methotrexate, and cyclophosphamide did not lead to an improvement in survival. Lastly, Krajewska et al. 83 found no evidence supporting the use of thalidomide in patients with brain metastasis from DTC.
Radioiodine therapy
Since the 1940s, the treatment for metastatic DTC has relied on the administration of 131I. 107,108 However, large retrospective studies have demonstrated that over time, two-thirds of metastatic patients become refractory to 131I treatment. In such cases, alternative treatment modalities are required. 1,109 Based on currently available data, radioiodine uptake by BM is variable, with a reported range of 0–45% of cases. 10,15 –17,54,56,106,110 –112 Therefore, studies showing that RAI may improve OS in patients with DTC with BM are lacking. However, in a retrospective series in which three patients with BM were treated with 131I, two of them showed a considerable improvement in their neurological symptoms and signs. 106 131I administration was associated with important side effects such as hemorrhage in the brain lesion, (worsening of) focal neurological deficit, severe headaches, motor weakness, and seizures due to radiation-induced cerebral edema. 10,113,114 In a retrospective study of Chiu et al., 10 neurological complications occurred in two of three patients treated with 131I; Datz 114 reported a case of a patient treated with 200 mCi of 131I that, 12 hours after institution of therapy, developed seizures, slurred speech, and muscle weakness. Before 131I administration for BM, it is recommended to prepare patients with recombinant human thyrotropin (rhTSH) to minimize the possibility of growth of BM and the possibility of adverse event. 10,114 Overall, rhTSH was generally well tolerated; however, in a subset of patients with CNS, spinal, or bone metastases, administration of rhTSH was observed to induce tumor growth, leading to compression of critical anatomical structures and subsequent neurological, respiratory, or other clinical complications. 115 For this reason, glucocorticoid premedication (dexamethasone, prednisone, or hydrocortisone) is recommended in patients with known or suspected metastatic lesions in confined spaces that are exposed to increases in TSH (by either withdrawal of thyroid hormone therapy or administration of rhTSH). 115 –118 In the study of Pellegriti et al., 116 all patients with distant metastases (bone or CNS) were treated with corticosteroids to prevent acute effects caused by peritumoral edema after 131I uptake. Specifically, 4–8 mg of dexamethasone was administered intramuscularly per day for 5 days before 131I administration and 2–4 mg per day during the following week. A different protocol has been described by Luster et al., 118 who treated patients with documented or clinically suspected brain or spinal cord metastases with 8 mg dexamethasone orally, twice daily or 80 mg prednisone orally, daily.
Conclusions
The brain is a rare site of metastases in patients with DTC. The diagnosis is often made incidentally or because of imaging performed before starting TKI treatment and is rarely made due to the presence of signs or symptoms. According to ATA guidelines (recommendation 69), imaging to detect BM should be considered in patients with DTC with elevated serum thyroglobulin (Tg) (generally >10 ng/mL) and negative neck and chest imaging, especially if neurological symptoms are present. 12 However, screening for BM can be advised in older male patients with FTC and PDTC who have other distant metastases, especially in bones and lungs. In contrast, in patients affected by ATC in which treatment is considered, current guidelines recommend brain MRI assessing the presence of BM at diagnosis as a part of initial staging and when specific symptoms appear. 98 The most accurate radiological investigation for the diagnosis of BM is MRI with and without contrast agent administration, which is superior to contrast-enhanced CT and the FDG-PET. Neurosurgery is the most extensively studied treatment modality and is associated with a potential survival benefit, followed by SRS. However, studies evaluating these treatment modalities are subject to selection bias, as only patients with better performance status or longer life expectancy undergo more invasive treatments. TKI therapy appears to be quite promising in patients with TC with RAI-R progressive disease and multiple metastases, even though only a few studies investigate its response in terms of survival. RAI therapy seems not to have any benefit, especially given the low iodine uptake in BM, and it could expose the patient to life-threatening side effects. However, despite many available studies being limited by small sample sizes, single-center designs, and a lack of information on clinical, pathological, or molecular risk factors, we have proposed a practical therapeutic approach for managing BM in patients with DTC (Fig. 1). Future research should aim to enhance the therapeutic options for patients with TC BM through well-designed clinical trials, biomarker discovery, exploration of novel therapies, and a focus on minimizing treatment-related side effects.
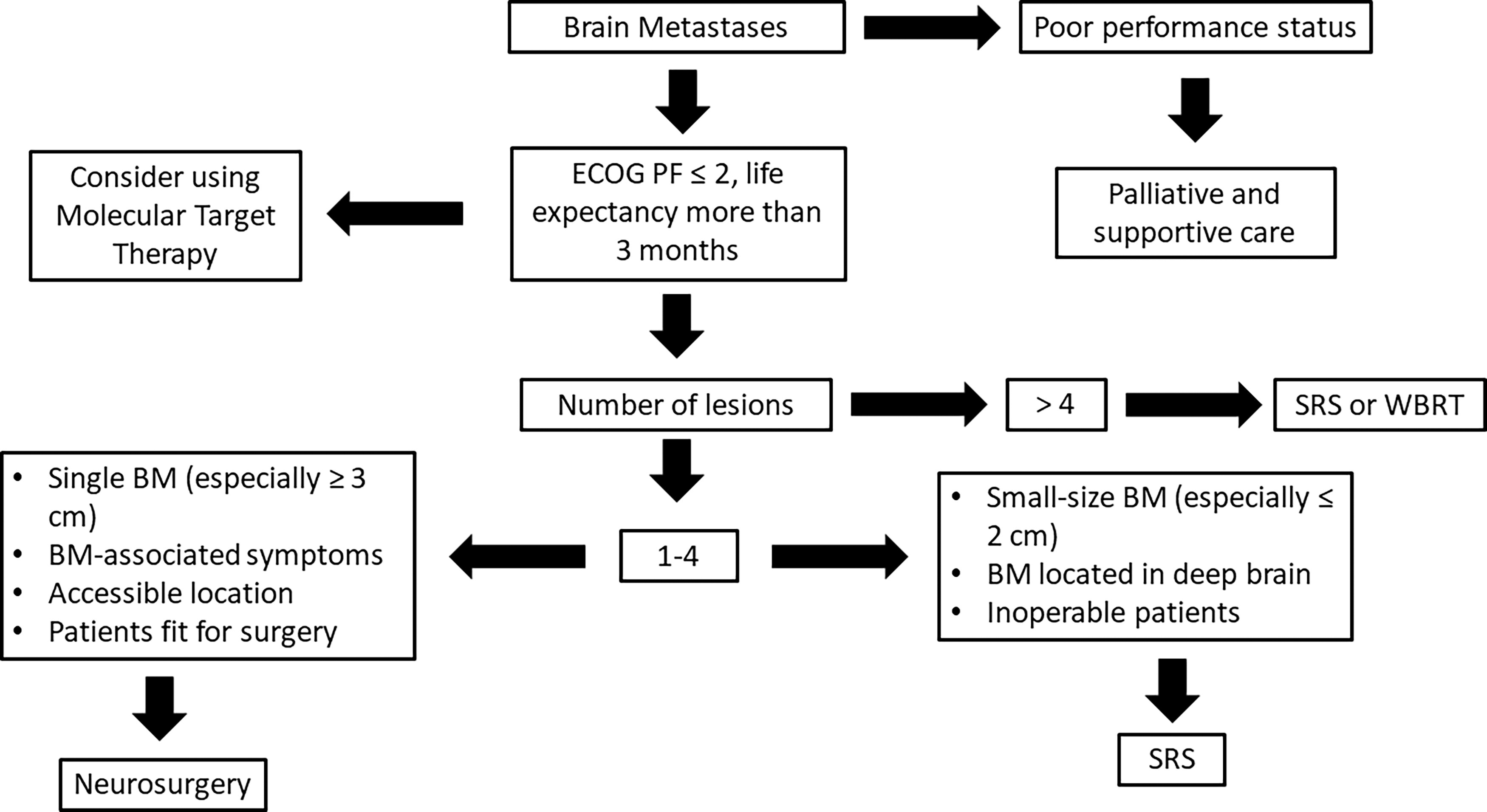
Proposed therapeutic approach of patients with brain metastases in differentiated thyroid cancer. BM, brain metastases; ECOG PS, Eastern Cooperative Oncology Group performance status; SRS, stereotactic radiosurgery; WBRT, whole-brain radiotherapy.
Footnotes
Authors’ Contributions
A.P.: conceptualization and writing—original draft; E.F.S.v.V.: writing—reviewing and editing and supervision; A.B.: writing—reviewing and editing and supervision; F.F.: writing—reviewing and editing and supervision; P.M.: writing—reviewing and editing and supervision.
Author Disclosure Statement
All authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Funding Information
No funding was received for this article.