
Abstract
Background:
We assessed the prevalence of complications from percutaneous ethanol injection (PEI) for benign and cystic thyroid nodules (CTNs) and their management.
Methods:
We conducted a systematic review with meta-analysis of data from published observational studies on PEI of CTNs. We also included unpublished retrospectively collected data on complications after PEI from all consecutive patients with cytologically benign CTNs who underwent PEI at the Unit of Endocrinology and Metabolic Diseases, AOU University of Campania Luigi Vanvitelli (Naples, Italy) between June 1, 2021, and March 31, 2024. A random effects meta-analysis was performed on the prevalence rate data. Pooled prevalence data were presented with confidence intervals (CIs). The I 2 statistic index was used to quantify the heterogeneity. The details of the complications and the management were qualitatively described.
Results:
The literature search yielded 1189 studies, of which 48 studies were included in the systematic review and meta-analysis, in addition to our institutional experience (3670 CTNs in total). The overall quality of each included study was judged as fair. The prevalence of “Overall” complications of PEI was 32% ([CI 25–40%], I 2 92.7%, 967 of 3195 thyroid nodules [TNs]). The prevalence of “Minor” complications of PEI was 32% ([CI 25–40%], I 2 92.7%, 952 of 3195 TNs). The prevalence of “Major” complications of PEI was 2% ([CI 1–2%], I 2 0%, 22 of 3670 TNs). Sensitivity analyses did not modify the results. The pooled prevalence rate of local pain was 21% (CI [16–27] I 2 90.3). Local pain was typically transient and mild, sometimes moderate, and requiring analgesics for few days. The pooled prevalence rate of dysphonia was 1% (CI [1–2], I 2 0). Dysphonia was transient and could last from several hours to 12 months after PEI.
Conclusions:
Complications of PEI for benign and CTNs are relatively common, but most are minor and usually transient, not requiring treatment. Dysphonia was a major complication, but it was uncommon and transient. PEI for CTNs could be considered a generally safe technique.
Introduction
Ultrasound (US)-guided minimally invasive treatments (MITs) (including ethanol ablation and thermal ablations) represent an alternative to surgery or even the first-line therapy for benign and locally symptomatic thyroid nodules (TNs). 1 –3 In this setting, percutaneous ethanol injection (PEI) is regarded as the best treatment for relapsing and symptomatic, benign cystic, or predominantly cystic thyroid nodules (CTNs). 1 –3 PEI is associated with high volume reduction rates that range from 80% to 100% and from 65% to 85.4% in purely CTNs and predominantly CTNs (PCTNs), respectively. 4,5 The high efficacy of PEI in reducing thyroid nodule volume persists over time. 4,5 Expert guideline and consensus panels have considered PEI to be a safe technique for TNs, as major complications have rarely been reported and side effects are deemed to be generally well manageable. 1 –3 However, although there is a large amount of data on the efficacy of PEI, 4,5 the safety data have not been extensively, rigorously reviewed. The technique of ethanol ablation has been used for decades, and there are few narrative reviews on the topic of complications. 6 –8 However, the actual prevalence of minor and major complications of PEI and the best management of the complications are not well defined.
Given the therapeutic importance of this issue for physicians performing thyroid ablation worldwide, 9 the aim of this study was to assess the prevalence of complications of PEI in CTNs and PCTNs and their management through a systematic review and meta-analysis of the literature, including data from the authors’ institution.
Methods
Detailed methods of the systematic review
The primary outcome was the prevalence of complications of PEI under real-time US guidance for cytologically benign CTNs and PCTNs (meta-analysis). The secondary outcome was to assess the features and management of these complications (i.e., mechanisms of occurrence, severity, duration, therapy) (systematic review). We conducted a systematic review with meta-analysis of data from published observational studies on PEI of CTNs. We also included unpublished retrospectively collected data on complications after PEI from a cohort of CTNs who underwent PEI at the Unit of Endocrinology and Metabolic Diseases, AOU University of Campania “Luigi Vanvitelli (Naples, Italy). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines 10 were followed in reporting this systematic review and meta-analysis. The current systematic review and meta-analysis was not registered.
Search strategy
Two investigators (L.S. and P.F.) independently conducted a comprehensive literature search in the online databases of MEDLINE (PubMed), Scopus, and Web of Science using the following search terms and their combinations: ‘‘Ethanol’’ (or “Alcohol”), “Thyroid” (or “Thyroid nodule”). A commencement date limit was not used, and the last search was conducted on July 01, 2024. Only articles with English main text were considered for inclusion. The search strategy was refined to evaluate all references of the screened studies to identify additional relevant studies. The search was restricted to human studies.
Eligibility criteria and study selection
Records identified by our search strategy were screened using “the report of complications of PEI under real-time US guidance for cytologically benign CTNs and PCTNs” as the major criterion of inclusion. We excluded patient cohort cases where PEI was combined with other MITs. Articles examining the use of PEI for hot nodules, metastatic lymph nodes, locoregional recurrence of papillary thyroid cancer patients, parathyroid, or thyroglossal duct cysts were excluded. Only published research articles were considered for inclusion (i.e., experimental studies, observational studies, and case series). We excluded the following types of articles: (i) case reports, reviews, editorials, letters, commentaries, guidelines, and meeting abstracts; (ii) small studies with <10 patients; and (iii) research articles, including nodules treated with other chemical agents (i.e., polidocanol, saline, tetradecyl sulfate) or with missing ultrasound features (cystic or noncystic). Two researchers (L.S. and P.F.), applying the above criteria, independently reviewed titles and abstracts of the screened articles. Then, all authors independently reviewed the main text of the eligible articles to define their inclusion. Disagreements were resolved by consensus among all the reviewers.
Data extraction
For the included studies, the following data were coded and extracted independently and in duplicate by two investigators (L.S. and P.F.), in a piloted form: (i) author, publication year, country, study design; (ii) number of nodules (CTNs and PCTNs) undergoing PEI with sex and age of patients; (iii) nodule volume; (iv) number of sessions per nodule; (v) number of punctures per session of PEI; (vi) needle diameter; (vii) local anesthesia at the needle-puncture site and/or peri-thyroidal area; (viii) approach for needle entry during US guidance; (ix) anticoagulation and/or antiplatelet therapy discontinuation; (x) grade of ethanol and amount of injected ethanol for each session of PEI; (xi) ethanol reaspiration; and (xii) number and details of complications.
Measures
For the included studies, complications were subdivided into “Minor” (local pain; transient burning sense; neck hematoma; set of symptoms [one or more in a single patient], including dizziness/drunkenness and/or flushing and/or increased heartbeat and/or nausea and/or headache; fever; vasovagal reaction [VVR] with hypotension) and “Major” (dysphonia with or without dysphagia, arrhythmia, nodule infection, Horner’s syndrome, thyrotoxicosis or hypothyroidism, esophageal injury, tracheal injury, skin burning) complications, also according to the Society of Interventional Radiology guidelines. 11
Risk of bias assessment
The risk of bias of the included studies was assessed independently by two investigators (L.S. and N.D.M.) through the National Heart, Lung, and Blood Institute Quality Assessment Tool (https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools). 12
Statistical analysis
Outcomes were assessed on a patient basis for each study. A proportion meta-analysis was performed with the DerSimonian and Laird method (random-effects model), 13 where pooled data are weighted averages relative to the sample size of the single studies. Pooled data were presented with confidence intervals (CI) and displayed in a forest plot. I 2 statistic index was used to quantify the between-study heterogeneity as follows: <25%, no heterogeneity; 25–50%, mild heterogeneity; 50–75%, moderate heterogeneity; and >75%, high heterogeneity. Trim and fill analysis and Egger’s linear regression test were used to evaluate for publication bias. Meta-regression and subgroup analyses were performed to explore the heterogeneity of results. The results of the meta-regression coefficient with the corresponding p value were reported. The sign of the regression coefficient indicated the “direction” of the relationship, while its value indicated the “degree” of the relationship. Analysis of variance test was carried out to evaluate the differences between the means of two or more data subgroups. A two-sided p value of <0.05 was regarded as significant for all analyses. Statistical analysis was performed using ProMeta 3.0 (Internovi, Cesena FC, Italy).
Detailed methods of the institutional retrospective study
This retrospective study was approved by the Institutional Review Board of University of Campania “Luigi Vanvitelli” (Naples, Italy) (Campania 2, 2024 0039/i). We included data from all consecutive patients who had cytologically benign CTNs and PCTNs and underwent PEI at the authors’ institution between June 1, 2021, and March 31, 2024. From our anonymous and electronic database, we extracted details on PEI complications with their management of PEI for CTNs and PCTNs. At our center, PEI was performed by the same experienced operator (L.S., with six years of clinical experience in performing PEI) who prospectively and accurately collected details. Moreover, all patients were in contact with the operator for at least six months after PEI. During this time, we did not have dropouts, and the reported data for each case were sufficiently comprehensive to answer to the study endpoints. PEI procedure consisted in one to two punctures for sessions, through a needle of 23 Gauge. During US guidance a lateral approach was used, and local anesthesia was not adopted. Anticoagulation therapy was discontinued 10 days before PEI, while antiplatelet therapy was not discontinued. Ninety-six percent ethanol was injected before or after cyst content evacuation in the amount of 20% of the initial nodule volume (≤10 mL), without early ethanol reaspiration. Data were reported descriptively.
Results
Institutional experience
Sixty-eight benign nodules (37 CTNs and 31 PCTNs, mean volume 16.3 ± 14.1 mL) from 68 patients (39 females and 29 males, mean age 50.0 ± 16.2 years) were treated with PEI (one session in 40 nodules and two sessions in 28 nodules during a mean follow-up of 12 months). We had 41 complications (60.3%, in 41 patients), subdivided into 40 minor complications (20 cases of transient burning sense, 11 cases of local pain, four cases of neck hematoma, three cases of set of symptoms, 2 cases of VVR with hypotension) and one major complication (one case of dysphonia). Local transient burning sense occurred during and/or after ethanol injection, resolving in few seconds or minutes. Local pain was mild, with need of nonsteroidal anti-inflammatory drugs for few days in two patients. Neck hematoma was managed with ice pack application, compression bandage, and glucocorticoids (prednisone 0.5 mg/kg daily) for a few days. VVR with hypotension spontaneously resolved in a few minutes. The set of symptoms, including one or more among dizziness/drunkenness and/or flushing and/or increased heartbeat and/or nausea and/or headache, appeared soon after ethanol injection and spontaneously solved in few minutes. Dysphonia (and dysphagia that lasted two weeks) occurred in one patient beginning few seconds after ethanol injection. Dysphonia was treated with 30 days of prednisone oral therapy, then 1 month of voice therapy, and the voice returned to normal after another 15 days.
Results of the literature search
The literature search initially yielded 1189 studies. All the studies were assessed, and the reasons for exclusion are shown in Figure 1 and Supplementary Table S1. Forty-eight observational retrospective studies, 14 –61 plus our institutional experience, were eligible for the meta-analysis. Data were included from 3670 thyroid benign and cystic nodules subject to PEI from adult patients (≥18 years of age). Table 1 summarizes the general characteristics of the included studies. Seven studies were published between 1990 and 2000, 55 –61 10 studies between 2000 and 2010, 45 –54 17 between 2010 and 2020, 28 –44 and 15 between 2020 to date (including our experience). 14 –27 Twenty three studies were from Asia, 14,16,19,24,28,32 –34,36 –44,46 –49,54,61 21 studies were from Europe, 15,18,20 –22,25 –27,31,35,45,50 –53,55 –60 3 studies from America, 17,23,29 and 2 from Turkey. 21,30 Of 2757 TNs, of which we know how they were subdivided into CTNs and PCTNs, 53.4% were represented by CTNs. The volume of TNs greatly varied across the studies.
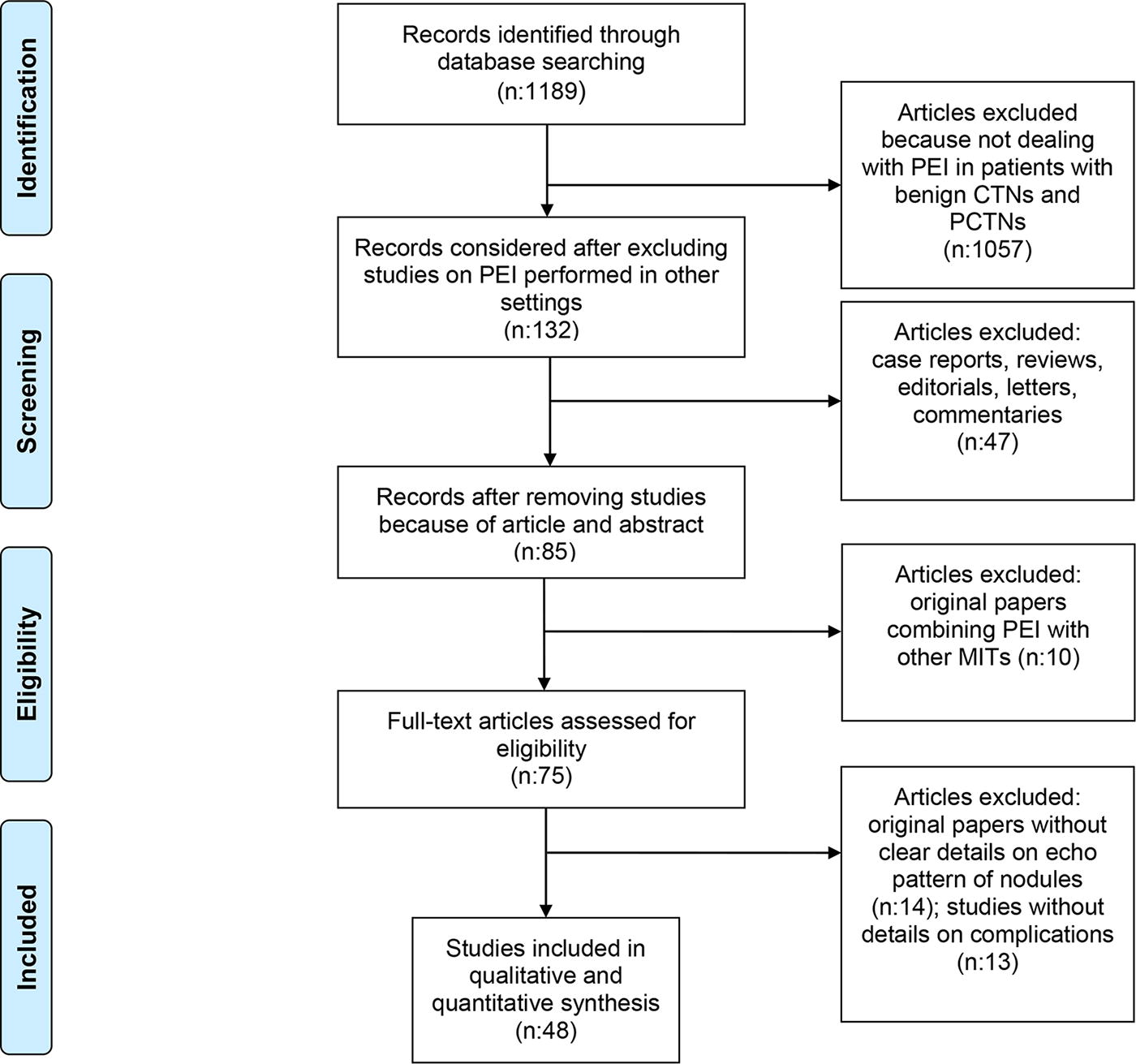
Flowchart of the study selection process. PEI, percutaneous ethanol injection; CTNs, cystic thyroid nodules; PCTNs, predominantly cystic thyroid nodules; MITs, minimally invasive treatments.
Summary of the General Characteristics of the Included Studies
Blanks are missing data.
TN, thyroid nodule; CTNs, cystic thyroid nodules; PCTNs, predominantly cystic thyroid nodules; PEI, percutaneous ethanol injection; US, ultrasound.
In 23 studies (46.9%), 14,17 –19,21 –25,28,32 –34,36 –40,42,44,49,58,61 the reported data, including those related to complications, referred to single-session PEI, whereas in the remaining studies, nodules could undergo more than one session of PEI. In all the included studies, except for the study by Kim DW 49 and our cohort where patients could undergo two punctures, the skin of patients was punctured one time to make both liquid aspiration and ethanol injection. The needle gauge sizes varied greatly depending on the study. In 30 studies (61.2%), local anesthesia at the needle-puncture site and/or peri-thyroidal area was not adopted. 15,19,20,23,26,27,30,32,33,36,38,39,42,44,46,50,52 –61 The approach for needle entry during US guidance (trans-isthmic or lateral approach) was reported in only 14 studies (28.6%). 14,17 –19,24,28,33,37,40 –43,50 Details on the anticoagulation and/or antiplatelet therapy discontinuation were reported in only four studies (8.2%) (including our experience). 15,21,26 The grades of ethanol for PEI varied from 95% to 100% across the studies. The amount of the injected ethanol for each session of PEI significantly varied across the studies. In 15 studies (30.6%), 14,19,24,28,29,32 –34,37,40 –43,48,49,59 injected ethanol was reaspirated as the last step of the PEI procedure.
Study quality assessment
Supplementary Table S2 summarizes the quality assessment of the 48 included studies.
The overall quality of each included study was judged as fair. Specifically, the risk of bias for each study could be judged as low in 8 of 14 items. By contrast, all studies did not report any power or sample size justification. Participation rate of eligible persons was not mentioned in any of the included studies. In all studies, the risk of bias on blinding of outcome assessors and confounding variables were regarded as high.
Complications
Prevalence rates
In the pooled analysis, prevalence rate of “Overall” complications of PEI was 32% ([CI 25–40%], I 2 92.7%, 967 of 3195 TNs) (Supplementary Fig. S1). The pooled prevalence rate of “Minor” complications of PEI was 32% ([CI 25–40%], I 2 92.7%, 952 of 3195 TNs) (Supplementary Fig. S2). The pooled prevalence rate of “Major” complications of PEI was 2% ([CI 1–2%], I 2 0%, 22 of 3670 TNs) (Supplementary Fig. S3). Table 2 shows the pooled analyses. Table 3 summarizes the characteristics of the respective complications.
Results of the Meta-Analysis (Pooled Prevalences of Complications of PEI)
p value using Egger’s test.
Summary of the Main Characteristics of Complications
Blanks are missing data.
TN, thyroid nodule; CI, confidence interval.
TBS, transient burning sense; NSAIDs, nonsteroidal anti-inflammatory drugs; SAIDs, steroidal anti-inflammatory drugs; VVR, vasovagal reaction; PEI, percutaneous ethanol injection; EA, ethanol ablation.
Local pain
The pooled prevalence rate of local pain was 21% (CI [16–27], I2 90.3, 663 cases of 3195 TNs). Pain was localized at the site of the ablated nodule, sometimes radiating to the ear or to the jaw. 55 Pain was associated with needle puncture and removal, and with ethanol retention and spread into the subcutaneous tissue. 28,54 Local pain was typically transient (minutes/few hours or few days after PEI) and mild, sometimes moderate and requiring analgesics (mainly nonsteroidal) for few days. 50 Only in one case EA was terminated early in one patient because of severe pain. 33
Transient burning sense
The pooled prevalence rate of transient burning sensation was 2% (CI [1–5], I2 89.3, 187 cases of 3195 TNs). Transient burning sense occurred at the injection site within a few seconds and resolving in few seconds or minutes (for a maximum of one hour). 39,47 Transient burning sensation did not require any medication.
Dizziness/drunkenness, and/or flushing, and/or increased heartbeat and/or nausea, and/or headache
The pooled prevalence rate of dizziness/drunkenness, and/or flushing, and/or increased heartbeat and/or nausea, and/or headache was 2% (CI [1–3], I2 47.0, 28 cases of 3195 TNs). One or more of these symptoms occurred during or several minutes after the procedure and spontaneously solved in few minutes or 1 hour. 36 These symptoms did not require any treatment.
Neck hematoma
The pooled prevalence rate of neck hematoma was 2% (CI [1–3], I2 49.1, 26 cases of 3195 TNs). Neck hematoma presented as a swelling of the neck at the injection site within a few seconds or minutes, or less often, some days after PEI. 18 This was the consequence of an intra-cystic or extrathyroidal (i.e., intramuscular or subcutaneous) hemorrhage. Neck hematoma typically recovered within a week, 24 after treatment with ice pack application, compression bandage, and steroid analgesics for few days.
Fever
The pooled prevalence rate of fever was 1% (CI [1–2], I2 0, 8 cases of 3195 TNs). Fever usually disappeared within one to two days without treatment. 55,56
VVR with hypotension
The pooled prevalence of VVR with hypotension was 1% (CI [1–2], I 2 0, 4 cases of 3195 TNs). Hypotension generally resolved within 30 minutes without treatment. 48
Dysphonia
The pooled prevalence rate of dysphonia (with or without dysphagia) was 1% (CI [1–2], I 2 0, 18 cases of 3670 TNs). This was due to the chemical damage of the homolateral recurrent laryngeal nerve, after leakage of ethanol toward the posterior region and the lower thyroid lobe. 45 The small thickness of cyst wall, the high speed of alcohol injection, the patient swallowing during the alcohol injection, or some pores of the cystic lesion could promote dysphonia. Dysphonia usually appeared soon after the procedure (or rarely 36 hours after PEI). 49 The way of resolution of dysphonia could vary as follows: it spontaneously resolved within 24 hours or 7 days or it could require medical therapy and strict laryngoscopy follow-up. In two cases (one from our institute and one from the study by Raggiunti et al. 45 ) when the patient did not show spontaneous and gradual improvement, glucocorticoids and vocal therapy were adopted to accelerate the full recovery of the normal voice. Dysphonia was transient and could last from several hours to 12 months after PEI. 53
Arrhythmia
The pooled prevalence rate of arrhythmia was 1% (CI [1–1], I 2 0, 2 cases of 3670 TNs). It consisted of the following two cases of transient tachycardia: one requiring hospitalization for 1 day of observation; 24 the other case occurred during a new onset thyrotoxicosis event, lasting one week. 60
Infection
The pooled prevalence rate of cyst infection was 1% (CI [1–1], I 2 0, 1 case of 3670 TNs). This occurred 25 days post-PEI and required incision and drainage of the abscess. 18
Thyrotoxicosis
The pooled prevalence rate of thyrotoxicosis was 1% (CI [1–1], I 2 0, 1 case of 3670 TNs). This occurred in one patient about 30 minutes after PEI and presented as sweating and tachycardia associated with TSH suppression and mild elevation of fT4 and fT3, which gradually normalized after one week without treatment. 60
Exploration of heterogeneity
A meta-regression was performed to evaluate the relationship between prevalence of complications of PEI and sample size, and the latter was divided into small (< 50 cases), medium (>50 cases and <100 cases), and large (>100 cases). As reported in Supplementary Table S3, the sample size did not significantly influence the prevalence of complications (“Overall,” “Major,” and “Minor” complications). Subgroup analysis was conducted to assess the impact of the country where PEI was performed (Asia vs. Europe) on prevalence of complications. Moreover, subgroup analysis served to explore if local anesthesia or alcohol respiration could impact on the prevalence of local pain. The prevalence of complications (“Overall”, “Major”, and “Minor” complications) did not statistically vary depending on the country. The prevalence of local pain did not vary depending on technical features (use of local anesthesia or ethanol respiration) (Supplementary Table S4 and Supplementary Table S5, respectively).
Discussion
A thorough understanding of the potential complications of MITs for benign TNs is needed in considering the safety of these procedures. 9 Before and during the performance of MITs, operators should know how common the potential complications are and how to manage them. Patients should also accurately be informed about complications of PEI for CTNs.
As far as we know, this is the first comprehensive systematic review examining the complications of PEI for benign and CTNs and the management of these complications. We summarized complication details (prevalence and features of management) from a large cohort (more than 3000) of TNs. We observed more studies published from 2010 to date (more than 65% of the included studies) compared with prior years, highlighting the growing literature available on PEI in recent years. Almost all the included studies were from Asia and Europe.
The results of this meta-analysis indicated that the prevalence of “Overall” complications of PEI was relatively high since we found a complication in about one third of the ablated TNs. However, most of the complications of PEI for CTNs and PCTNs were represented by “Minor” complications. The pooled prevalence rates of “Overall” and “Minor” complications were equal, whereas “Major” complications occurred only in 2% of cases. Moreover, local pain covered about two thirds of both “Overall” and “Minor” complications since it was observed in 21% of cases. Pain was typically transient and mild, and analgesics were needed only in a minority of cases. Another relatively common side effect was represented by transient burning sense because it occurred in 187 cases (2% of pooled prevalence). Transient burning sense typically resolved in few seconds or minutes and did not require any treatment. One or more of the symptoms of dizziness/drunkenness, flushing, increased heartbeat, nausea, and headache accounted for 2% of complications, and none of these required any treatment. Neck hematoma also occurred in 2% of cases and typically resolved within a week, after treatment with ice pack application, compression bandage, and steroid analgesics. Among the “Minor complications,” fever and VVR with hypotension were even more rare (1% of prevalence), but still transient and managed without important treatment. We found a high level of heterogeneity for pain and transient burning sense, and this could potentially be due to several factors, including approach for needle entry, amount of ethanol injected, and experience of the operator, but we could not formally examine for this using the limited data available for review in the primary studies.
Among the “Major complications” dysphonia was the most common and relevant side effect. It occurred in 1% of cases (18 cases reported in literature to date); it was transient but potentially lasting until 12 months. In some cases, dysphonia required glucocorticoids and vocal therapy to accelerate the full recovery of the normal voice. Arrhythmia, cyst infection, and thyrotoxicosis were uncommon side effects (1% of prevalence), without permanent sequelae. For prevalences of “Major” complications we found absence of heterogeneity, but the analyses were limited by low event rates.
Through the sensitivity analyses, we finally confirmed that prevalence of complications of PEI (“Overall”, “Major”, and “Minor” complications) did not vary according to country (Asia vs. Europe) or the sample size of the included studies, findings that could imply that complications do not depend on location or the number of PEI procedures. Moreover, we also demonstrated that prevalence of local pain did not vary according to technical features (i.e., use of local anesthesia or ethanol reaspiration).
Our study does have some limitations. We were unable to determine whether the prevalence and/or type of management varied according to the sex, location of TNs (CTNs vs. PCTNs), position of TNs, amount and degree of ethanol injected, or needle size. We could not exclude that our results (mainly the prevalences of “Major” complications) were affected by publication bias. Furthermore, all of the studies included in this systematic review (including our own data) were subject to a retrospective design, with inherent methodologic limitations. The quality of included studies was thus relatively low. Because the current study was not registered in PROSPERO, this could be another limitation. Furthermore, we also could not analyze the prevalence rates of concurrent major and minor complications due to limitations of the available data in the published studies. Finally, because we excluded case reports, we did not consider anecdotal but serious complications of PEI for TNs (i.e., necrosis of the larynx and adjacent skin, Horner’s Syndrome, Graves’ disease without or with Graves’ ophthalmopathy, Plummer adenoma, acute suppurative thyroiditis). 8,62 –65
A major strength of this study is that this is the first comprehensive systematic review and meta-analysis on complications of PEI for cystic TNs and the management of these complications. Compared with previously published narrative reviews, 6 –8 our study may provide more accurate numeric estimates for complication rates and potentially be subject to less bias.
Conclusions
Based on the results of this study, complications of PEI for benign and CTNs are relatively common, but minor and usually transient, not needing relevant therapies. Dysphonia was a major complication, but it was uncommon and transient. Therefore, PEI for CTNs could be considered a safe technique. Our findings could be useful for the drafting of the dedicated form for written informed consent for PEI of CTNs.
Footnotes
Acknowledgments
The authors sincerely thank PNRR-ANTHEM (AdvaNced Technologies for HumancentrEd Medicine) project for oversight of the scientific activity of the researcher Lorenzo Scappaticcio. The authors also thank Dr. Vincenzo Morone, library information specialist at University of Naples Federico II (Naples, Italy), who assisted with the electronic search of literature. The authors greatly thank Doctor Alberto Gorgoni, journalist in Portugal, who patiently revised the vocabulary and grammar of our article.
Authors’ Contributions
L.C. designed the study, drafted it, approved the final version, and agreed for all aspects of the work. P.F. managed data analysis, critically reviewed it, approved the final version, and agreed for all aspects of the work. N.D.M. managed data analysis, critically reviewed it, approved the final version, and agreed for all aspects of the work. R.N. interpreted results, critically reviewed the study, approved the final version, and agreed for all aspects of the work. M.D. interpreted results, critically reviewed the study, approved the final version, and agreed for all aspects of the work. M.I.M. interpreted results, critically reviewed the study, approved the final version, and agreed for all aspects of the work. P.C. interpreted results, critically reviewed the study, approved the final version, and agreed for all aspects of the work. M.D.N. interpreted results, critically reviewed the study, approved the final version, and agreed for all aspects of the work. M.L. interpreted results, critically reviewed the study, approved the final version, and agreed for all aspects of the work. G.D. interpreted results, critically reviewed the study, approved the final version, and agreed for all aspects of the work. G.P. interpreted results, critically reviewed the study, approved the final version, and agreed for all aspects of the work. P.T. interpreted results, critically reviewed the study, approved the final version, and agreed for all aspects of the work. K.E. interpreted results, critically reviewed the study, approved the final version, and agreed for all aspects of the work. G.B. interpreted results, critically reviewed the study, approved the final version, and agreed for all aspects of the work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Fig. S1
Supplementary Fig. S2
Supplementary Fig. S3
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5