
Abstract

Ultrasound-guided thermal ablation is increasingly used and widely accepted as an effective and safe alternative to surgery for the treatment of thyroid nodules, including treatment of benign and selected cases of malignant thyroid lesions. 1,2 Consequently, Radiologists and other thyroid specialists will increasingly need to evaluate ultrasounds of patients treated with thermal ablation. Thus, Radiologists and other thyroid specialists will need to be prepared to correctly report the imaging findings of such cases.
Ultrasound represents the most widely used imaging modality for the study of the thyroid gland and characterization of thyroid nodules. One of its main limitations is the subjectivity of assessment of some ultrasound features. 3 In particular, ultrasound is known to be characterized by a relatively low diagnostic sensitivity for some particular ultrasound features, and specially, in estimating the malignant potential of focal lesions (27%–63%). 4
The EU-TIRADS classification was introduced in 2017 by the European Thyroid Association to offer a standardization for thyroid nodules reporting and stratification according to the risk of malignancy and requirement for fine needle aspiration (FNA). EU-TIRADS classification proposes the use of a combination of ultrasound features, such as nodule composition, echogenicity, margins, shape, and presence of calcifications to establish the potential risk of malignancy of a nodule and drive the subsequent need for cytological assessment. 4 This classification is intended to have a high sensitivity, exclude low-risk lesions from FNA and minimize the proportion of false-negative lesions. However, it is also important to obtain the highest possible level of specificity, in order to eliminate over-diagnosing and treating patients who do not actually need it. 4
TIRADS classification systems are an extremely useful tool and are increasingly applied in the clinical practice. However, is it possible to apply TIRADS classification to nodules following thermal ablation? Post-ablation nodules may exhibit altered ultrasound features, sometimes resembling malignancy (Fig. 1). 5 This has consequences for the follow-up of patients treated by thermal ablation, especially in the case of allegedly benign nodules with a suboptimal response to treatment and in case of thyroid carcinomas treated with thermal ablation.
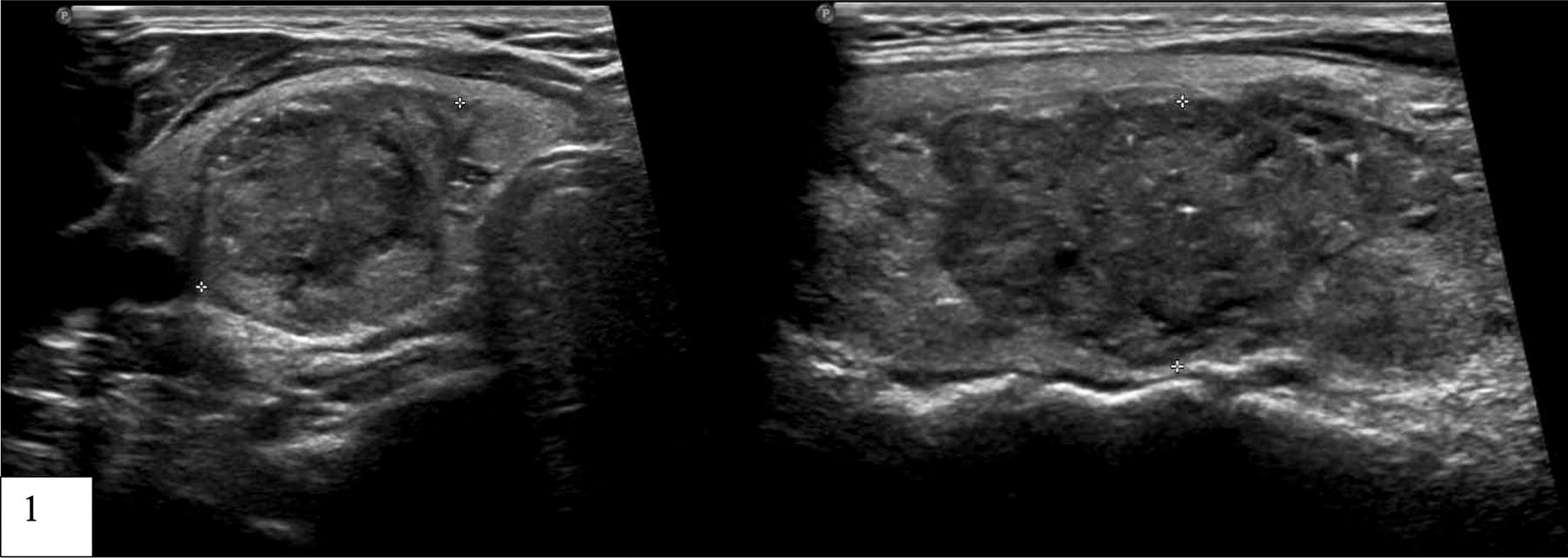
Ultrasound appearance of a nodule treated with thermal ablation. The nodule present solid, hypoechoic appearance, non-oval/round shape, irregular margins, and presence of punctate echogenic foci, presenting as suspicious for malignancy.
Distinguishing treated nodules from potentially malignant ones poses challenges for radiologists, potentially leading to unnecessary FNAs and patient anxiety. Wu et al. reported that after radiofrequency ablation the number of nodules with highly suspicious ultrasound features significantly increased, reaching a 70,1% of cases classified in category 4 or 5. 5 This represents a major challenge for Radiologists and thyroid specialists having to report on these cases, and for clinicians having to decide whether or not perform a fine needle aspiration biopsy on the basis of the present rules. This may also increase the anxiety of treated patients who receive radiological reports with description of highly suspicious features.
To address this, there’s a need for awareness and further research into the ultrasound appearance of ablated thyroid nodules. Establishing a subclassification within TIRADS classification systems for thyroid nodules treated with thermal ablation could aid clinicians in accurately assessing these cases, acknowledging their distinct characteristics and risk profiles.
Footnotes
Authors’ Contributions
T.D.: Conceptualization, writing—original draft, approval of final article. G.M.: review and editing and approval of final article.
Author Disclosure Statement
Teresa Dionísio—no conflicts to disclose. Giovanni Mauri—no conflicts to disclose.
Funding Information
No funding information to declare.