
Abstract
Background:
Isthmic thyroid nodules are more likely to be malignant and isthmic differentiated thyroid cancer demonstrates less favorable behavior compared with lobar locations. The goal of this study was to assess molecular differences of thyroid nodules and carcinomas from the isthmus relative to the lobes.
Methods:
The Afirma thyroid nodule database (n = 177,227) was assessed for cytologic and molecular differences between isthmus and lobar nodules in this observational cohort study. Genome-wide differential expression analysis was conducted to decipher transcriptomic differences. Histopathology reports (n = 583) of papillary thyroid cancer (PTC) (n = 389) and infiltrative follicular subtype of PTC (IF-PTC) (n = 194) from Afirma discovery cohorts and from thyroid cancer patients managed at an integrative endocrine surgery community care practice were analyzed for molecular differences between isthmic and lobar cancers.
Results:
In the Afirma database, 8527 (4.8%) isthmus nodules were identified. Bethesda V–VI nodules were almost twice as prevalent from the isthmus as compared with the lobes (8.2% vs. 4.3%, p < 0.0001). Isthmus nodules had twice the frequency of BRAFp.V600E (21% vs. 10.6%, p < 0.0001), an increased frequency of ALK/NTRK/RET fusions (4.6% vs. 2.5%, p < 0.0001) and SPOP variants (1.5% vs. 0.8%, p < 0.0001), and a lower frequency of NRAS mutations (7.8% vs. 13.2%, p < 0.0001), and PAX8::PPARy fusions (1.1% vs. 2.3%, p < 0.0001) than lobar nodules. Transcriptome analysis of molecular signatures and genome-wide analysis showed that isthmus nodules have higher BRAF-like scores, ERK activity, follicular mesenchymal transition scores (FMT), and lower inflammation activity scores. Pathway enrichment analysis revealed genes downregulated in isthmus tumors are enriched in immune response regulation. IF-PTC from the isthmus (n = 13) were more BRAF-like and had increased ERK and FMT scores compared with those from the lobes (n = 181) (p < 0.01 for all).
Conclusions:
These data suggest isthmic nodules are more likely to have malignant cytology and increased rates of higher risk molecular alterations compared with lobar nodules. IF-PTC from the isthmus is molecularly different compared with IF-PTC from the lobes. More data are needed to know if a change in surgical therapy is warranted in isthmic thyroid cancers relative to lobar cancers and if this molecular data should influence isthmic thyroid cancer management and monitoring.
Introduction
The thyroid isthmus is normally a thin piece of tissue that lies anterior to the trachea and connects the two lobes of the thyroid. Thyroid nodules are very common with over 60% of the population having one or more by the seventh and eigth decades of life. 1 Isthmic thyroid nodules are detected about eight times less frequently than nodules in the lobes. 2 However, recent studies have shown that the risk of malignancy arising from isthmic thyroid nodules is greater than lobar nodules. 2,3 In addition, isthmic thyroid cancers have been shown to exhibit more aggressive behavior compared to lobar thyroid cancers, including higher rates of extrathyroidal extension, capsular invasion, and lymph node metastasis. 4,5 Though the anatomical location, thin tissue approximating the thyroid capsule, and unique lymphatic drainage 6 –8 have been noted as reasons for worse pathological features, molecular differences were shown in isthmic papillary thyroid carcinoma (PTC) with higher ERK and lower thyroid differentiation scores (TDSs) compared with lobar PTC. 9
Approximately 20–25% of thyroid nodule aspirates result in The Bethesda System for Reporting Thyroid Cytopathology Bethesda (B) III or IV cytology (together, indeterminate thyroid nodules [ITN]). 10 The risk of malignancy of ITN ranges from 13–34% depending on the institution and the categorization of noninvasive follicular thyroid neoplasm with papillary-like nuclear features) as benign or malignant. 11 To help address the clinical challenge of ITN, the Afirma Gene Expression Classifier (GEC) was developed and eventually replaced by the Afirma Genomic Sequencing Classifier (GSC) after clinical and analytical validation. 12,13 The Afirma GSC uses exome-enriched RNA sequencing (RNAseq) such that each sample is sequenced for 26,268 genes, providing data on gene and exon expression, mitochondrial expression, loss of heterozygosity, and detection of expressed gene variants and fusions. 14 Therefore, Afirma testing can clinically provide both diagnostic (in ITN) and prognostic information in BIII–VI thyroid nodule 15 and be analyzed for gene expression signatures and biological pathways as a research tool.
The purpose of this study was to interrogate the Afirma thyroid nodule database (AfirmaDB) to assess the cytological and molecular differences between thyroid nodules of the isthmus and lobes. In addition, a cohort of thyroid cancers that underwent Afirma testing were analyzed to assess for histological, molecular, clinicopathologic outcome differences between isthmic and lobar thyroid carcinoma.
Materials and Methods
Thyroid nodule evaluation
Analysis of 177,227 consecutive thyroid nodules with clinical Afirma GSC results from 2017 to 2022 with BIII–VI cytology by location (as indicted on the test request form, isthmus vs. non-isthmus [lobar]), cytology category (BIII–IV vs. BV–VI), sex, age, and Genomic Sequencing Classifier-Suspicious (GSC-S) rate was performed in this observational cohort study (Fig. 1 and Table 1). Most nodules referred had BIII and BIV cytology and were analyzed to assess if these nodules were molecularly benign and could avoid unnecessary surgery. 16 Cytology was read either at a local pathology practice or, when preferred, at Thyroid Cytopathology Partners (Austin, TX). There was no formal centralized cytopathology review. The relative frequencies of genomic alterations (variants and fusions) from the Afirma Xpression Atlas 17 were evaluated by nodule location across different subgroups (ITN GSC-S and BV–VI combined, ITN GSC-S and BV–VI alone) and without knowledge of the final histopathology when applicable.
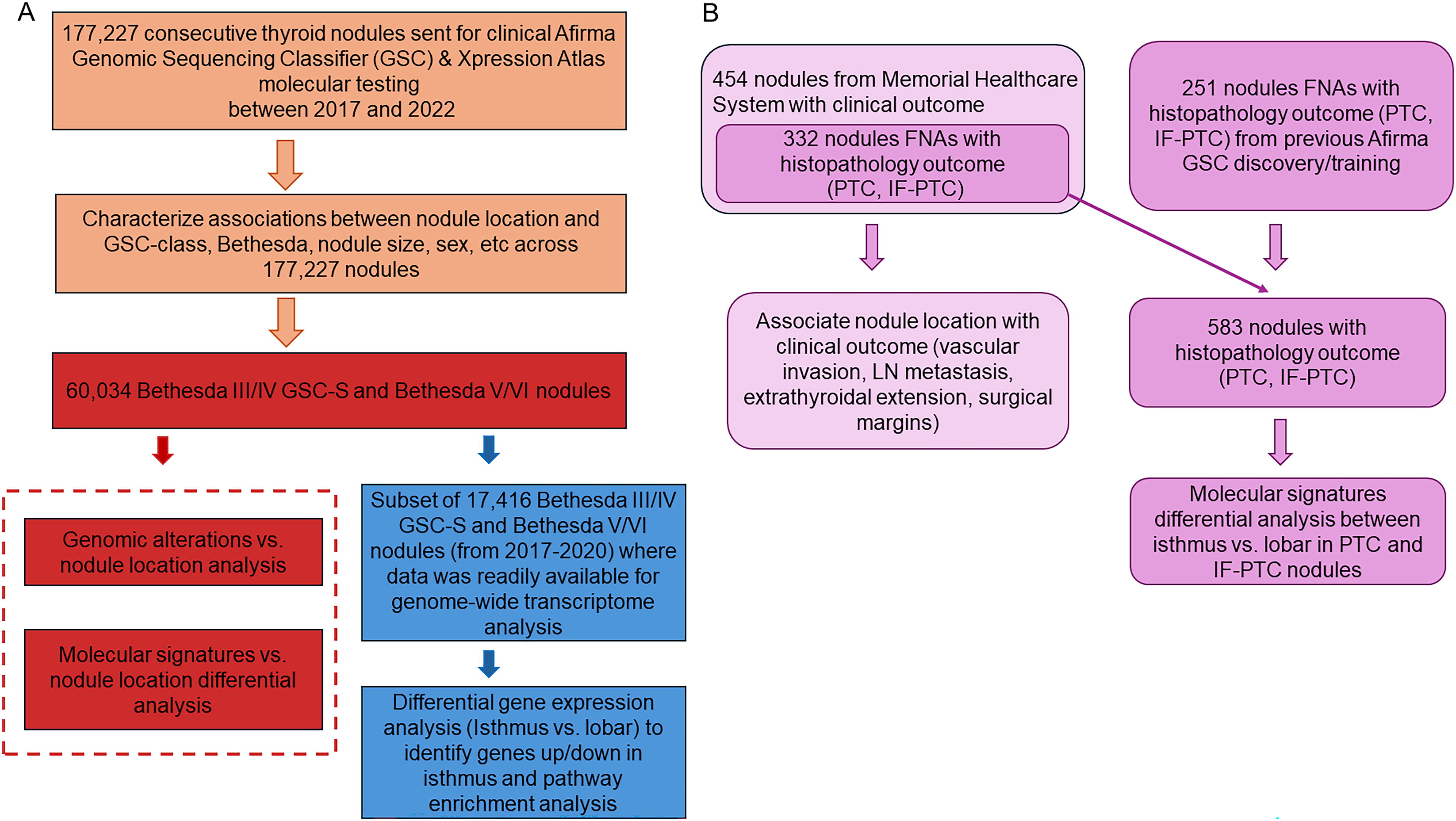
Flowchart of cohorts used, and analyses conducted.
Characteristics of Samples from AfirmaDB with Nodule Location
(x, y) includes the nodules ≥x and <y cm.
within bethesda III/IV.
GSC, genomic sequencing classifier; IQR, inter quantile range.
Thyroid carcinoma evaluation
Local histopathology reports from differentiated thyroid carcinoma (DTC) (infiltrative follicular subtype of papillary thyroid carcinoma ([IF-PTC]) = 194, PTC = 389) from Afirma GSC discovery/training cohorts 13 (n = 251 collected from 2013 to 2016) and from thyroid cancer patients managed at an integrative endocrine surgery community care practice (Memorial Healthcare System, n = 332 collected from August 2017 to July 2022) that all underwent Afirma GSC exome-enriched RNAseq analysis were assessed for cytological differences and gene expression signatures based on cancer location. 13 Memorial Healthcare submitted thyroid nodule biopsy specimens with BIII–VI cytology (with local cytopathology reads) for Afirma testing in an actively managed cohort, from which molecular findings were correlated to final histopathology (Fig. 1).
Biological pathways enrichment analysis
For molecular difference assessment, 54 gene expression signatures were evaluated. These include activity scores of 50 hallmarks of cancer pathways, 18 BRAF-like to RAS-like molecular score (BRS), ERK signaling, TDS and follicular to mesenchymal transition score (FMT). For pathway enrichment analysis, transcriptome-wide differential expression analysis using 26,268 genes was conducted to identify genes upregulated and downregulated in isthmus nodules by using Wilcoxon rank sum statistical test. g:Profiler online tool (https://biit.cs.ut.ee/gprofiler/gost) was used to identify biological pathways enriched in upregulated and downregulated genes in isthmus nodules. 19 EnrichmentMap and Cytoscape tools were used to take g:Profiler output and build a network of related, significantly enriched pathways. 20,21 Finally, to gain more insights into the immune content of the sequenced samples, we used ESTIMATE algorithm that uses deconvolution of bulk gene expression data to output estimated levels of infiltrating immune cells. 22
Institutional review board approval
The Afirma GSC discovery cohort pathology reports were from subjects recruited for the Afirma GEC and subsequent GSC training and validation studies with approval of institutional-specific review boards, Chesapeake IRB (now Advarra IRB, Columbia, MD), and Copernicus Group Independent Review Board (now WCG IRB, Princeton, NJ). 13 Patients recruited to the Afirma GEC validation study provided written informed consent. 12 Memorial health patient data, including cytology and histopathology reports, was collected under WCG IRB protocol # DHF 005-044.
Statistical analysis
All statistical analyses were conducted in R 3.2. Wilcoxon rank sum test was used to assess differences of continuous variables (gene expression, pathway scores, BRAF-like score, ERK, FMT) between nodule locations and for genome-wide differential expression analysis. The chi-square test was used to assess significant associations between cytology groups, genomic alterations, and nodule location. Logistic regression was used to calculate odd ratios (ORs) of cancer pathways scores and their association with isthmus nodules. Multiple esting p value correction was done using Benjamini-Hochberg procedure.
Results
A total of 177,227 nodules were evaluated with 8527 from the isthmus (4.8%) (Table 1). The median age was slightly higher in patients with lobar nodules (57.7 vs. 59 years old, p < 0.001). More female patients were found with isthmus nodules compared with lobar nodules (80% vs. 77.4%, p < 0.001). Isthmus nodules were twice as likely to have BV–VI cytology compared with lobar nodules (8.2% vs. 4.3%, p < 0.001). There was no significant difference in the GSC-S call rate of isthmus versus lobar nodules for ITN (30.5% vs. 30.8%, p = 0.52) (Table 1).
Genomic analysis within ITN GSC-S or BV–VI nodules showed that isthmus nodules were more enriched with molecular variants and fusions at high-risk for malignancy like BRAFp.V600E (21% vs. 10.6%, p < 0.0001) and ALK/NTRK/RET fusions (4.5% vs. 2.5%, p < 0.0001) (Table 2). Additionally, SPOP variants were statistically more frequent in the isthmus (1.5% vs. 0.75%, p < 0.0001). Moderate risk for malignancy variants that were overrepresented in the lobes relative to the isthmus were: NRAS (13.2% vs. 7.9%, p < 0.0001), HRAS (8.3% vs. 4.6%, p < 0.0001), and PAX8::PPARy fusions (2.3% vs. 1.1%, p < 0.0001). In addition, RET variants were overrepresented in the lobes relative to the isthmus (0.53% vs. 0.06%, p = 0.001). Genomic analysis of ITN GSC-S nodules alone showed a similar trend of overrepresentations of BRAFp.V600E, ALK/NTRK/RET fusions, and SPOP variants in isthmus nodules (Table 2).
Key Genomic Alterations Found in Isthmus and Lobar Nodules in AfirmaDB Samples excluding GSC-Benign
p values adjusted for multiple testing using Benjamin-Hochberg method.
GSC-S, Genomic sequencing classifier-suspicious; IF-PTC, infiltrative follicular subtype of PTC; PTC, papillary thyroid cancer.
To further gain molecular insights into the differences between isthmus and lobar nodules, we evaluated 54 gene expression-based signatures that are thyroid specific BRS, ERK activity, FMT, TDS, and pan-cancer (Molecular Signatures Database hallmarks of cancer pathways) (Fig. 2). Within ITN GSC-S and B V–VI subgroups, isthmus nodules had significantly higher BRS score, ERK activity, and FMT scores (p < 0.0001 for all). Differential analysis of cancer hallmark pathways scores showed that isthmus nodules have higher scores of epithelial-mesenchymal transition (EMT), coagulation, apical junctions, angiogenesis, estrogen receptor, and TGF-beta signaling. However, they had lower activity of PI3K-AKT signaling, heme metabolism and inflammation immune related signatures (Fig. 2). The same trend was observed for the 54 signatures when limiting the analysis to ITN GSC-S samples or BRAF-negative ITN GSC-S and BV-VI samples (Supplementary Figures S1 and S2).

Molecular differences between isthmus and lobar nodules.
Transcriptome-wide differential expression analysis showed that 1619 genes were found upregulated in lobar, and 1329 genes were upregulated in isthmus nodules within ITN GSC-S and BV/VI samples (Fig. 3). To gain functional insights into these genes, we conducted gene set enrichment analysis using g:Profiler online tool to identify biological pathways enriched in upregulated genes in isthmus and lobar nodules. 19 EnrichmentMap 20 and Cytoscape tools 21 were used to build and visualize a network of significantly enriched pathways. Upregulated genes in isthmus nodules were enriched with cell migration, blood vessel development, and angiogenesis gene sets, and rRNA processing (Fig. 3, Supplementary Table S1). Upregulated genes in lobar nodules were enriched with immune system response, immune cell activation, cytokine signaling, antigen receptor-mediated signaling, and inflammatory response pathways (Fig. 3, Supplementary Table S1). To further gain insights into the immune content, we applied the ESTIMATE algorithm, which showed that isthmus nodules have lower immune content relative to lobar nodules (OR: 0.74, p < 0.001). 22 Enrichment analysis and ESTIMATE results provide strong evidence of the immune coldness of isthmus tumors.

Genome-wide differential expression analysis and Enrichmentmap of biological pathways enriched in genes upregulated in isthmus or lobar nodules. Within ITN GSC-S or Bethesda V/VI nodules, gene expression in isthmus nodules (n = 935) was compared with lobar nodules (n = 16,481) showing 1329 gene upregulated in isthmus and 1619 upregulated in lobar (adjusted p value <0.0001). Gprofiler online tool was used to identify enriched biological pathways and gene sets. Enrichmentmap and cytoscape were used to build network of pathways, where every node represents a significantly enriched pathway (p < 0.000001) and each edge represent gene overlapping between pathways. Groups of related pathways were annotated by the common pathway theme. ITN, indeterminate thyroid nodules.
Finally, we characterized the molecular differences between thyroid isthmus and lobar carcinomas by histological subtype (PTC [isthmus = 37, lobe = 352] and IF-PTC [isthmus = 13, lobe = 181]). (Table 3). Isthmic IF-PTC had higher scores of BRS, ERK, and FMT activity relative to the lobar IF-PTCs (Fig. 4). Isthmic PTC, on the contrary, did not differ from lobar PTC, except for FMT. Isthmic PTC had higher ERK, FMT, and BRS scores relative to isthmic IF-PTC (p < 0.006 for all). Within thyroid cancers that had indeterminate cytology, there was no difference between isthmic versus lobar IF-PTC nor between isthmic versus lobar PTC (Supplementary Figure S3). In terms of clinical outcomes, a cohort of 454 samples from Memorial Healthcare System (Fig. 1) with 41 isthmus nodules was analyzed. These included 9 isthmic IF-PTC and 30 isthmic PTC as well as 2 other isthmus tumor types (1 oncocytic cell carcinoma, 1 follicular thyroid carcinoma). From the 41 isthmus cancers, 32 (77%) tumors were ATA low risk, 7 (18%) were ATA intermediate risk, and 2 (5%) were ATA high risk. There was no difference in the rates of vascular or capsular invasion, extrathyroidal extension, positive surgical margins, or lymph node metastases by cancer location.
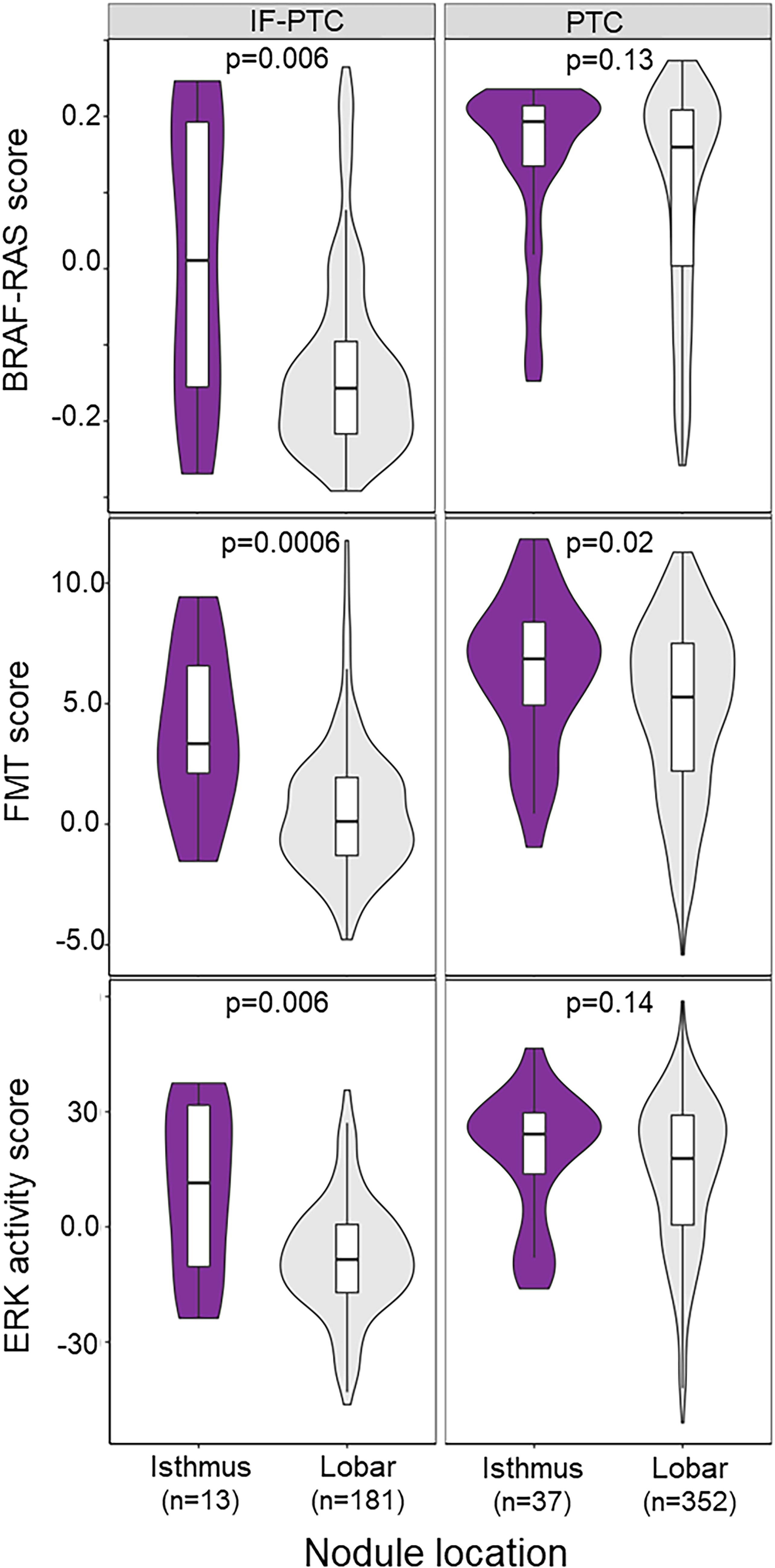
Violin plots of thyroid molecular signatures scores across nodule locations in IF-PTC or PTC nodules showing that BRAF-RAS score, FMT, ERK scores are higher in isthmic IF-PTC relative to lobar IF-PTC. IF-PTC, infiltrative follicular subtype of PTC; PTC, papillary thyroid cancer.
Characteristics of Samples with Histology Reports Used for Molecular Assessment of Isthmic Nodules
IQR, interquartile range; IF-PTC, infiltrative follicular subtype of PTC; PTC, papillary thyroid cancer.
Discussion
In the present study, we have investigated the cytological and molecular differences between thyroid nodules and cancers arising from the isthmus as compared with the thyroid lobes. We have shown that for thyroid nodules sent for Afirma molecular testing, there is a higher rate of BV–VI cytology in isthmus nodules relative to the lobes. In addition, isthmus nodules harbor higher rates of BRAF-like molecular signatures and other molecular markers associated with aggressive behavior compared with those found in the lobes. Of uncertain significance is the increased frequency of SPOP variants found in isthmic tumors relative to those in the lobes. SPOP has been shown to be relatively enriched in benign thyroid nodules and was demonstrated to be a candidate alteration in “driver negative” thyroid carcinoma. 23,24 Interestingly, in terms of isthmic carcinomas, IF-PTC of the isthmus showed significantly higher levels of BRAF-like, ERK, and FMT expression scores than those of the lobes and were molecularly closer to classical PTC. Classical PTC, however, did not show molecular differences between the isthmus and the lobes except for higher rates of FMT in the isthmus locations.
Thyroid cancer is predominantly an ERK-driven carcinoma with BRAFp.V 600E mutations found in up to 60% of PTC, followed by mutations in the different RAS isoforms (10–15%). 25 BRAF mutations lead to higher ERK activation, which may drive EMT, leading to cancer progression, metastasis, and resistance to radioiodine. 26 Activation of EMT has been shown to play a key role in thyroid cancer progression by promoting capsular invasion, extrathyroidal extension, and both local and distant metastasis. 27 In this study, FMT reflects EMT specifically assessed in thyroid follicular cells.
A recent study by Alqahtani et al. evaluating nodules with BIII cytology redemonstrated a higher risk of malignancy (ROM) for isthmic nodules (66%) compared with those in the lobes (overall 48% ROM). 28 The majority of ITN sent for Afirma testing have BIII cytology, and it is notable there was no significant difference between the benign and suspicious result for Afirma tested ITN at the isthmus versus the lobes. There is no clear explanation for this discordance, though it may be due to a significant difference in the prevalence of cancer in BIII cytology where the Alqahtani study had a 47% ROM as compared with 13–30% expected in the United States. 11
In terms of tumor behavior, Wang et al. showed that isthmic PTC had greater minimal and gross extrathyroidal extension compared with PTC from the lobes. 29 These clinical findings are consistent with the molecular differences of isthmus cancers compared with those arising from the lobes, such as BRAF-like and ERK differences. In the current analysis, there was no significant difference in isthmus versus lobe thyroid cancer histology though this is most likely driven by the low number of isthmus cancers analyzed. This low number limits the ability to determine if the molecular differences described between isthmus and lobar tumors alters the performance of Afirma based on nodule location. The extent of surgical resection for PTCs located in the isthmus has remained a matter of considerable debate. At present, there is no standard surgical approach when treating PTC located predominantly in the isthmus. 30 –32 The molecular findings described in this study suggest clinicians should carefully assess for aggressive clinical features in isthmic tumors, though a lack of documented long term oncologic outcomes with different surgical approaches to isthmic thyroid carcinomas tempers any clear surgical recommendation.
This study expands upon the work of Smith et al., which studied isthmic PTC, by including follicular lesions which are enriched in BIII and IV cytology as well as IF-PTC. In addition, this study analyzes molecular data from preoperative samples via the AfirmaDB, including the Afirma Xpression Atlas, though it is limited by the lack of TERT promoter mutation testing which was not available until more recently. Finally, this work is strengthened by the incorporation of features of the tumor microenvironment and immune scores via the ESTIMATE algorithm that are novel compared with other studies of isthmic thyroid tumors. Consistent with the findings of Wang et al. where PTC had lower stromal and immune scores of PTC as compared with normal thyroid, this work leverages exome-enriched RNA-seq to show the relative immune coldness of isthmus nodules that may be a factor in the reported clinical behavior of isthmus thyroid carcinomas. 33
This study is constrained by an inability to account for potential selection bias for sending isthmus tumors for molecular testing and only performing analysis of the subset of tumors with actionable Afirma or cytology results (GSC-S or BV–VI nodules). The relatively small number of isthmus carcinomas limits the analysis of clinical behavior differences from lobar thyroid cancers though this is consistent with the reported rates of DTC located in the isthmus that range from 1% to 9.2% for all malignant thyroid nodules. 2 In addiiton, long-term oncologic outcomes are not assessed. These hypothesis generating results indicate that future studies comparing progression free and overall survival from larger cohorts would be of interest. In addition, analyses that explore why thyroid isthmus lesions have a different molecular profile compared with lobar lesions will be valuable. In summary, isthmus thyroid nodules and IF-PTC of the isthmus appear to be cytologically and molecularly more aggressive than those of the thyroid lobes. More data are needed to know if a change in surgical therapy is warranted in isthmic thyroid cancers relative to lobar cancers and if this molecular data should influence isthmic thyroid tumor management and monitoring.
Footnotes
Authors’ Contributions
S.J. and T.C.B. conceptualized the study and helped with article preparation and review. A.G. and D.B. provided clinical data and reviewed the article. J.P.K., M.A., and R.T.K. helped with study design and article preparation and review. M.A., R.J., Y.C., Y.H., and J.H. helped with data analysis, article preparation, and review. All authors reviewed the final article, and all gave final approval for publication.
Author Disclosure Statement
M.A., R.J., Y.C., Y.H., J.H., J.P.K., and R.T.K. are employees and equity owners of Veracyte, Inc. S.J., T.C.B., A.G., and D.B. have no disclosures.
Funding Information
There was no external funding source for this project.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1