
Abstract

Subacute thyroiditis (SAT) is a self-limiting inflammatory thyroid disorder often triggered by viral infections. Nonsteroidal anti-inflammatory drugs (NSAIDs) or corticosteroids (CS) are standard treatments, but managing SAT can be challenging due to its potential for recurrence during dose tapering or week(s) after continuation of therapy. Recurrence rates are around 12%, with higher incidences in patients treated with CSs compared to those treated with NSAIDs. 1 High-dose CS, rapid tapering, and shorter CS treatment durations increase relapse risk. 2,3 Steroid dependency presents a therapeutic challenge due to the well-known adverse effects of prolonged steroid use and may finally lead to hypothyroidism or require thyroidectomy. Steroid dependency, characterized by relapse upon tapering or discontinuation of CS, presents a therapeutic challenge due to the adverse effects of long-term use and can potentially result in hypothyroidism or the need for thyroidectomy.
Colchicine, an anti-inflammatory agent commonly used in treating gout and familial Mediterranean fever, has shown efficacy in various inflammatory conditions. However, its potential in SAT is although reported is underexplored. 4 Hereby we present a case series of five steroid-dependent SAT patients successfully managed with a colchicine-supported protocol.
We retrospectively reviewed five cases of steroid-dependent SAT who were treated with a combination of CS and colchicine. Recurrence/relapse was determined based on clinical, laboratory, and ultrasonographic (US) features. Patients were initiated on CS treatment at a dose of either 32 or 24 mg/day methylprednisolone (MPS) depending on the severity of the clinical presentation for at least 10 days, followed by tapering off the dose in 6–12 weeks if they are symptom free. Steroid dependency was defined as the need to restart CS due to relapse during tapering off or the week(s) after discontinuation. Our regimen was to introduce colchicine (0.5 mg bid) at the CS dose where relapse occurred and gradually taper and eventually discontinue treatment. Suggested “treatment discontinuation protocol” (TDP) is as follows: CS were reduced to 4 mg/day MPS and continued for four weeks, and to prevent the rebound, colchicine (0.5 mg bid) was continued for an additional four weeks after CS discontinuation and then stopped. Informed consent was obtained from all patients for the off-label use of colchicine and the publication of their medical information.
Case Presentations
Hereby we present five cases of steroid-dependent SAT, initially treated with 24–32 mg/day of MPS, but required 2–5 CS courses due to relapses. Patients were successfully treated by adding colchicine 0.5 mg bid to their CS regimens. The disease course and treatment regimens for these cases are described in Figure 1. None of the described patients experienced any side effects associated with colchicine. All cases typically showed an initial overt thyrotoxicosis and finally euthyroid after a temporary hypothyroid phase.
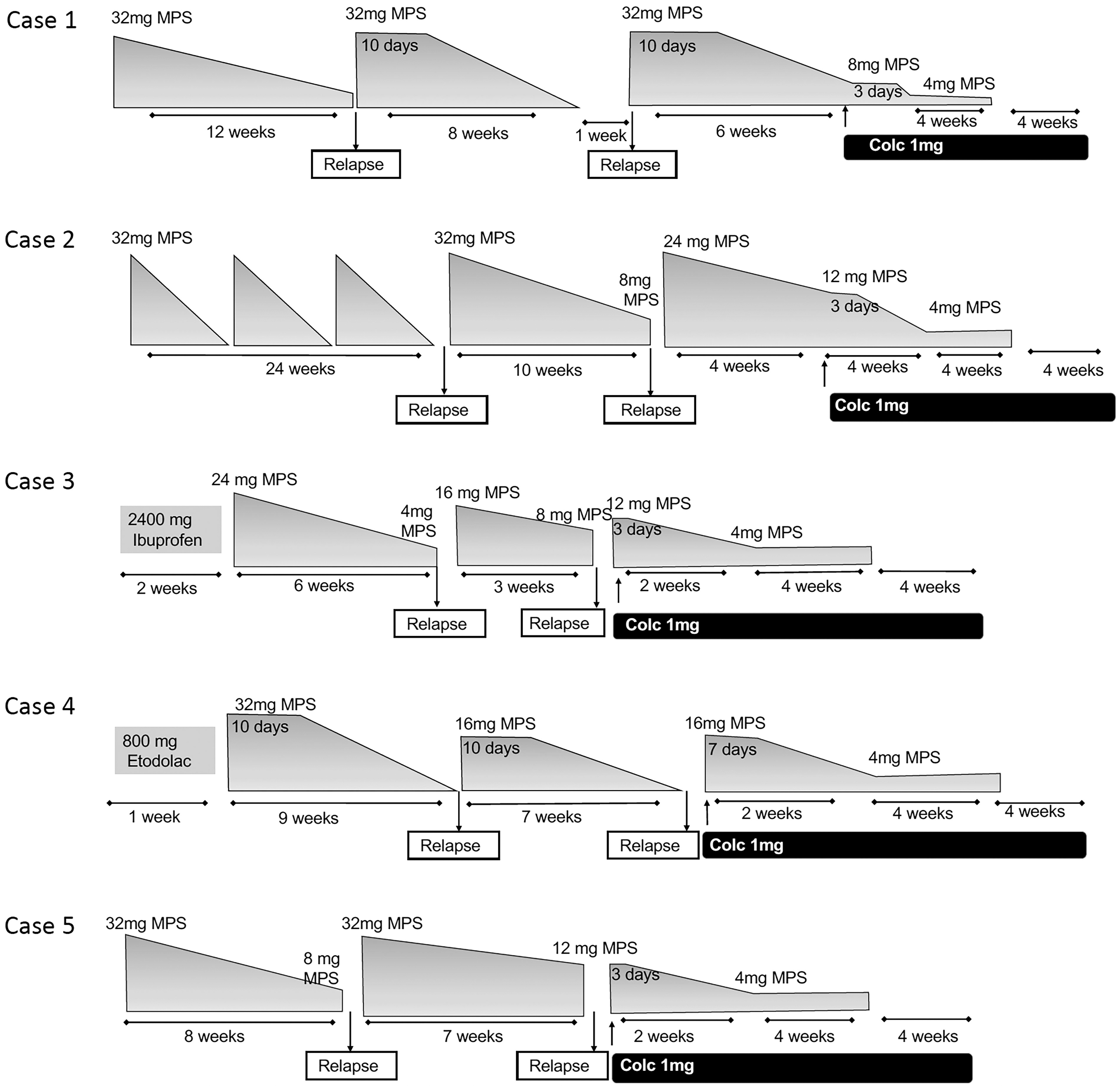
The disease course and treatment regimens of cases.
Case 1
A 48-year-old woman with a history of COVID-19 and concomitant SAT presented with typical symptoms. Erythrocyte sedimentation rate (ESR) was 60 mm/h, and C-reactive protein (CRP) was 36 (0–5) mg/L, and US revealed patchy hypoechoic areas in both lobes. The patient had to receive a 32 mg/day MPS regimen thrice due to relapses. Colchicine was added at the 26th week, and the treatment was successfully completed with TDP. No recurrence was observed after 38 months (Fig. 1, Case 1).
Case 2
A 31-year-old female patient with neck pain and myalgia was diagnosed with relapsing SAT and received four MPS courses over 34 weeks due to relapses. At presentation, ESR was 40 mm/h, and CRP was 22 mg/L. US showed patchy hypoechoic areas in both lobes. At the last course MPS was increased to 24 mg/day and then tapered to 12 mg/day over four weeks, while colchicine was also added. CS dose was tapered again and successfully discontinued in 12 weeks with TDP. No recurrence was observed after 24 months (Fig. 1, Case 2).
Case 3
A 43-year-old woman presented with neck pain and palpitations. Examination revealed thyroid tenderness and elevated APR (ESR: 35 mm/h, CRP: 20 mg/L); US revealed patchy hypoechogenic areas found in the left lobe. After NSAID (ibuprofen 2400 mg/day) treatment failed, MPS was initiated at 24 mg/day, but patient required dose adjustments due to several recurrences. Finally, colchicine was added, and treatment was successfully completed with TDP. No recurrence was observed after five months of follow-up (Fig. 1, Case 3).
Case 4
A 42-year-old woman with a history of significant anterior neck pain and fatigue, which did not respond to Etodolac 800 mg/day. Past medical history revealed multiple relapses under MPS, over 17 weeks. Upon admission, a swollen and tender left thyroid lobe and patchy SAT areas were observed on ultrasound, along with elevated APR (ESR: 30 mm/h, CRP: 18 mg/L). Lastly, treatment with 16 mg/day MPS and colchicine was successful, tapering CS off in six weeks according to TDP. The patient was symptom-free after five months (Fig. 1, Case 4).
Case 5
A 31-year-old woman with a history of 15 weeks of fatigue and radiating jaw pain initially responded to 32 mg/day MPS, but relapses occurred during dose reduction, and she could not reduce CS below 8 mg/day due to relapses. At admission, she was cushingoid, had neck tenderness, elevated APR (ESR: 28 mm/h, CRP: 12 mg/L), and US showed right lobe and isthmic enlargement and patchy infiltration. We started 0.5 mg bid colchicine and 12 mg/day MPS. CS therapy was successfully stopped with TDP, and she remained relapse-free at the fifth month of follow-up (Fig. 1, Case 5).
Discussion
This case series suggests that colchicine may be a valuable adjunct in managing steroid-dependent SAT, helping to prevent relapses and reduce prolonged CS exposure. Colchicine’s effects, including inhibition of neutrophil activation and its antifibrotic properties, 5 may contribute to controlling inflammation. In this series, all relapsing patients could successfully discontinue CS, and no recurrence was observed after cessation of colchicine.
We are aware of a single article, regarding use of colchicine in the treatment of SAT, consisting of three cases. 4 In this case report, the authors noted that they observed the control of SAT symptoms with the use of colchicine in a patient concurrently diagnosed with acute gout arthritis. Based on this observation, they added colchicine to the treatment regimen and successfully concluded CS therapy. 4 Similar to the case report mentioned, in our series, the combination of colchicine with CS therapy in “steroid-dependent SAT” cases facilitated the reduction and discontinuation of CS.
This report is a retrospective case series containing preliminary observations suggesting that colchicine might be beneficial when stopping steroid treatment is challenging. However, this report has limitations since it is a retrospective case series, and the patients were not followed according to a standardized treatment protocol, resulting in heterogeneity among cases. Follow-up after discontinuation of colchicine varied, from 5 to 38 months, which we believe is a reasonable period since the recurrences usually occur week(s) after CS withdrawal, but long-term follow-up data are needed to assess long-term recurrences.
The promising results observed in our cases warrant further research. If confirmed by a randomized controlled study with a larger patient cohort and longer follow-up, colchicine could become a valuable tool in reducing steroid dependency and preventing relapse in SAT patients.
Footnotes
Authors’ Contributions
All the authors of the article fulfill the criteria for authorship. A.B.B: Conception and design of the work, collecting data, analysis and interpretation of data and article writing; M.F.E.: Conception and design of the work, finding funds, collecting data, article writing, and revising the article.
Author Disclosure Statement
None of the authors have any potential conflicts of interest associated with this research.
Funding Information
No funding was received for this article.