
Abstract
Background:
Patients diagnosed with low-risk papillary thyroid microcarcinoma (PTMC) face the decision between thyroid lobectomy and active surveillance (AS). This study aimed to investigate the factors influencing treatment decisions in low-risk PTMC and to compare the quality of life (QoL) according to the treatment plan.
Methods:
The multicenter prospective cohort study comparing AS and thyroid lobectomy was conducted. Clinical characteristics were compared between the AS and Lobectomy groups. QoL questionnaires were administered every 6 months in the initial year and annually thereafter.
Results:
A total of 927 patients (453 in the AS group and 474 in the Lobectomy group) with low-risk PTMC were included in this study. The mean age was 47.4 ± 12.2 years, and 72.2% of the patients were women. Older age (odd ratio [OR] 1.04, confidence interval [CI] 1.02–1.05, p < 0.001), smaller tumor size (OR 0.78, CI 0.69–0.87, p < 0.001), family history of thyroid cancer (OR 1.48, CI 1.03–2.12, p = 0.035), prior awareness of AS (OR 1.53, CI 1.16–2.02, p = 0.003), and higher income (OR 1.79, CI 1.13–2.83, p = 0.013) were significantly associated with a higher likelihood of choosing AS. The median follow-up was 27.3 months (23.9–43.9) in the AS group and 28.7 months (20.4–44.5) in the Lobectomy group. During the follow-up period, the AS group showed significantly better QoL scores compared with the Lobectomy group (β 0.17, CI 0.02–0.33, p = 0.029). Although baseline QoL scores favored the AS group significantly (7.1 ± 1.2 vs. 6.7 ± 1.2, p < 0.001), no significant difference was observed after 12 months (7.2 ± 1.2 vs. 7.1 ± 1.2, p = 0.592).
Conclusions:
This study demonstrated that age, tumor size, family history of thyroid cancer, awareness of AS, and income were associated with patients’ treatment choices. Although the overall QoL scores were significantly higher in the AS group, the QoL became similar between the two groups after 12 months.
Clinical Trial Registration:
KCT0004935.
Introduction
Active surveillance (AS) is a viable option for papillary thyroid microcarcinoma (PTMC) measuring 1 cm or smaller without high-risk features including extra-thyroidal extension and clinical lymph node (LN) metastasis. 1 The American Thyroid Association’s guideline states that both surgery, especially thyroid lobectomy, and AS can be considered for low-risk PTMC. 1 Therefore, the choice of treatment is made through a collaborative decision-making process between the physician and the patient, where comprehensive information regarding the pros and cons of both immediate surgery and AS should be provided to patient. 2,3 Previous studies have reported that age, tumor size, quality of life (QoL), and consulting physician can influence on the decision of treatment plan. 4,5 Recently, Sawka et al. reported that lower educational level was associated with the choice of AS, 6 indicating a need to explore further how socioeconomic status factors such as education and income impact treatment choices.
The patient-reported outcomes (PRO) are particularly critical when deciding on a treatment plan for low-risk PTMC. The significance arises because the differences in the clinical outcomes between immediate surgery and AS are minimal due to the indolent nature of PTMC. According to a recent report from Miyauchi et al., the long-term oncological outcomes of patients with PTMC were slightly different between patients undergoing AS and immediate surgery: a 1.1% occurrence of LN metastasis in the AS group compared with a 0.4% LN recurrence in the immediate surgery group at 10 years. 7 Distant metastases were reported in one patient from each group; however, all patients survived without thyroid cancer-specific deaths. 7
A few studies have compared PRO or QoL between AS and immediate surgery in low-risk PTMCs. Cross-sectional studies have found better QoL in the AS group than in the surgery group, attributed to fewer surgery-related complaints, such as neuromuscular, throat/mouth, voice, and scar problem. 8,9 There are two prospective longitudinal cohort studies regarding QoL. Moon et al. reported that AS group showed a significantly better QoL compared with the surgery group during the median 24.4 months follow-up period. 5 Liu et al. reported that the AS group initially reported significantly better QoL concerning voice, throat/mouth, and scar problems, these differences, except for scar problems, leveled off after 12 months. 10 These findings underscore the need for more comprehensive, long-term longitudinal studies to analyze various factors influencing QoL.
Thus, we aimed to compare PRO using QoL questionnaires in patients with low-risk PTMC undergoing either immediate thyroid lobectomy or AS. This study included participants from a Korean multicenter prospective cohort study comparing clinical outcomes of AS with those of an immediate thyroid lobectomy in PTMC. 11 We analyzed various demographic factors, such as education and income levels, to understand their influence on treatment decisions. Additionally, we examined the long-term changes in patients’ QoL based on their selected treatment plan.
Materials and Methods
Study population
This study was conducted as part of the ongoing Korean Multicenter Prospective cohort study of Active Surveillance or Surgery (KoMPASS), which aims to enroll 2000 participants and has been continuously recruiting patients since August 2020. KoMPASS study is a prospective observational cohort study to compare clinical outcomes between AS and immediate thyroid lobectomy for low-risk PTMC involving 11 hospitals in Korea. This study included patients aged 19–80 with thyroid nodules measuring 6–10 mm diagnosed as either malignancy (Bethesda category VI) or suspicious for malignancy (Bethesda category V) through fine-needle aspiration or core-needle biopsy. Patients with a suspicion of a cervical LN metastasis and/or a suspicion of distal metastasis, with clinical symptoms/signs of extra-thyroidal extension of the tumor, or showing invasion to recurrent laryngeal nerve, and patients with multiple thyroid nodules or another thyroid disease requiring a total thyroidectomy were excluded. Low-risk PTMCs that can be treated by thyroid lobectomy are considered eligible. The physician explained the advantages and disadvantages of AS and surgery to patients with low-risk PTMC using printed materials that included a detailed description of the clinical outcomes of low-risk PTMC and the pros and cons of AS and lobectomy. After a thorough explanation and careful consideration, patients chose their treatment plan based on their preference. After deciding on the treatment plan, the study was explained to the patients, and informed consent was obtained. The detailed protocol for the study was described previously. 11 The primary outcome of the KoMPASS study is progression-free survival in patients with low-risk PTMC, but one of the secondary outcomes is patients’ QoL. This study is an interim analysis of QoL in the ongoing KoMPASS study.
From August 2020 to August 2023, a total of 1033 patients were screened, and 1017 were enrolled in the study. After excluding 10 patients who underwent surgical procedures other than thyroid lobectomy, such as total thyroidectomy or isthmectomy, and 80 patients who did not complete the QoL survey, 927 patients remained. These included 453 in the AS group and 474 in the Lobectomy group. These participants were finally included in the study analysis (Supplementary Fig. S1). The study protocol was approved by the institutional review boards of 11 centers including Asan Medical Center (2019-1541), Seoul National University Bundang Hospital (B-1912/583-304), Seoul St. Mary’s Hospital (XC20ONDE-0053K), the National Cancer Center (NCC2020-0123), Gangnam Severance Hospital (3-2020-0077), Seoul National University Hospital (1911-149-1083), Samsung Medical Center (2019-11-140), Eunpyeong St. Mary’s Hospital (XC20ONDE0053P), Pusan National University Hospital (2004-03-089), Chonnam National University Hwasun Hospital (CNUHH-2020-086), and Chungnam National University Hospital (2019-11-054). The study protocol was registered at the Clinical Research Information Service of the Korea Centers for Disease Control and Prevention (KCT0004935).
QoL survey
To assess QoL in patients with low-risk PTMC, a Korean version of the self-reported thyroid-specific QoL questionnaire for patients with thyroid cancer (KT-QoL) was used. This questionnaire was originally developed by Dow et al., 12,13 translated into Korean, and subsequently validated. 14 The questionnaire encompassed aspects of physical, psychological, social, and spiritual QoL. The questionnaire consists of 15, 16, 14, and 7 questions for each section, and the responses to each question are scored on a scale from 0 (worst) to 10 (best outcome). The overall KT-QoL score was calculated as the average score of all responses to the questions. The KT-QoL survey was administered every 6 months during the first year and annually thereafter by trained clinical research coordinators.
Clinical data
At the time of enrolling patients in the study, demographic characteristics such as age, sex, education level, income level, family history of thyroid cancer, and prior awareness of AS were collected through questionnaires and interviews. To determine prior knowledge of AS, patients were asked, “Have you ever heard of or searched for AS for PTMC?” with response options of “yes” or “no.” Height and weight were measured, and the body mass index (BMI) was calculated as weight (kg)/height (m2). Information about thyroid cancer, including tumor size and biopsy results (Bethesda category V or VI), was obtained from medical records. Serum thyrotropin (TSH) levels, as measured using an immunoradiometric assay (Beckman Coulter [Marseille, France], Simens [Berlin, Germany], Shinjin Medics Inc. [Goyang-si, Republic of Korea], Roche Diagnostics [Monza Italy and West Sussex, UK], and BRAHMS [Berlin, Germany]) by each hospital, were also collected.
Statistical analysis
Data were presented as mean ± standard deviation (SD). To compare baseline characteristics between AS and Lobectomy groups, continuous variables were compared using the Students’ t-test and categorical variables were compared using the Chi-squared test. To investigate the factors influencing the choice of treatment plan, a logistic regression analysis was performed on age, sex, BMI, tumor size, Bethesda category, TSH, family history of thyroid cancer, prior awareness of AS, education, and income. Multivariable logistic regression analysis was performed for age, tumor size, family history of thyroid cancer, prior awareness of AS, and income, all of which showed significant results in univariable logistic regression analysis. The QoL scores at each visit were compared using the Students’ t-test or Wilcoxon test. To investigate the factors associated with QoL, the generalized estimating equation (GEE) analyses were performed on treatment choice, age, sex, BMI, tumor size, Bethesda category, TSH, family history of thyroid cancer, prior awareness of AS, education, and income. Multivariable GEE analysis was performed for treatment choice, age, sex, Bethesda category, and income, which showed significant results in univariable analysis. All statistical analyses were conducted using the SAS software version 9.4 (SAS Institute Inc, Cary, NC, USA) and SPSS software version 27 (IBM Corp., Armonk, NY, USA).
Results
Clinical characteristics of AS and Lobectomy group
A total of 927 patients with low-risk PTMC were included in this study, with 453 (48.9%) in the AS group and 474 (51.1%) in the Lobectomy group. The mean age was 47.4 ± 12.2 years, and 72.2% of the patients were women. Baseline characteristics between the two groups were compared (Table 1). The AS group was significantly older than the Lobectomy group (49.8 ± 12.0 years vs. 45.0 ± 11.9 years, p < 0.001), had smaller tumor size (7.3 ± 1.1 mm vs. 7.6 ± 1.2 mm, p < 0.001), and higher income (p = 0.011) (Table 1). The AS group had a higher prevalence of a family history of thyroid cancer (19.2% vs. 14.3%, p = 0.047) and a higher rate of prior awareness of AS (64.0% vs. 55.7%, p = 0.010). Serum TSH level was comparable between groups (2.06 ± 2.50 μIU/mL vs. 2.13 ± 1.39 μIU/mL, p = 0.611): levothyroxine was prescribed to eight (1.8%) patients in the AS group and eight (1.7%) patients in the Lobectomy group.
Baseline Characteristics of Active Surveillance and Lobectomy Groups
AS, active surveillance; BMI, body mass index; IQR, interquartile range; SD, standard deviation.
In the Lobectomy group, the majority (80.8%) underwent a conventional open thyroid lobectomy, while 19.2% underwent robotic surgery. After surgery, eight patients experienced temporal voice changes, but they recovered and there were no permanent voice changes. There were no cases of transient/permanent hypoparathyroidism. In the AS group, 52 (11.5%) patients decided to do delayed surgery during the 2-year follow-up period (Supplementary Fig. S1).
In this study, 485 patients (252 in the AS group and 233 in the Lobectomy group) were followed for more than 2 years. At the 2-year follow-up, 23 (7.1%) patients in the AS group and 114 (48.9%) patients in the Lobectomy group were taking levothyroxine. Levothyroxine was prescribed based on the physician’s judgment or preference, even when thyroid function was normal. However, TSH levels were significantly lower in the AS group than in the Lobectomy group (1.96 ± 1.59 μIU/mL vs. 2.62 ± 1.78 μIU/mL, p < 0.001).
Factors influencing treatment selection
To investigate the factors influencing patients’ treatment plan choices, a logistic regression analysis was conducted. In both univariable and multivariable logistic regression analysis, older age, smaller tumor size, family history of thyroid cancer, prior awareness of AS, and higher income (≥5400 dollars/month) were significantly associated with a higher likelihood of choosing AS (Table 2).
Logistic Regression Analysis on Factors Affecting Treatment Plan Selection in Patients with Low-Risk Papillary Thyroid Microcarcinoma
The outcome variable is the choice of treatment plan, either surgery or AS. Surgery serves as the reference category when calculating the ORs. An OR >1 indicates a higher likelihood of choosing AS over surgery.
OR, odds ratio.
Longitudinal changes of QoL
KT-QoL survey was conducted every 6 months during the first year and annually. The median follow-up was 27.3 months (interquartile range [IQR] 23.9–43.9) in the AS group and 28.7 months (IQR 20.4–44.5) in the Lobectomy group. At baseline, 905 patients completed the KT-QoL survey, 661 patients at 6 months, 508 patients at 12 months, and 249 patients at 24 months. To investigate factors associated with QoL, GEE analyses were conducted. Univariable GEE analyses revealed that the AS treatment plan, older age, male sex, Bethesda category V, a family history of thyroid cancer, and a higher income were associated with higher KT-QoL scores in overall health (Table 3). In the multivariable GEE model, only the AS treatment plan, older age, male sex, and Bethesda V showed a significant association with better KT-QoL scores (Table 3). Specifically, the AS group exhibited better KT-QoL scores compared with the Lobectomy group, even after adjusting for age and sex (β 0.17, CI 0.02–0.33, p = 0.029). This suggests that the choice between AS and surgery significantly influences the QoL in patients with low-risk PTMC.
Linear Model Generalized Estimated Equation Analyses on Factors Associated with Overall Health KT-QoL Scores in Patients with Low-Risk Papillary Thyroid Microcarcinoma
Higher education is defined as having attained a college degree or higher, while lower education is defined as having completed high school or less.
Highest income means ≥5400 dollars/month, middle income means 2300–5400 dollars/month, and lowest income means <2300 dollars/month.
The AS group included 52 patients who underwent delayed surgery. Those who had delayed surgery in the AS group had significantly lower KT-QoL scores compared with those who continued with AS (β −0.33, CI −0.64 to −0.03, p = 0.031). Compared with the Lobectomy group, there was no significant difference in QoL for those who had delayed surgery (β 0.05, CI −0.25 to −0.35, p = 0.743), but those who continued with AS had significantly higher QoL (β 0.33, CI 0.03–0.64, p = 0.031).
At baseline, the AS group had significantly higher scores than the Lobectomy group for overall KT-QoL scores (7.1 ± 1.2 vs. 6.7 ± 1.2, p < 0.001) and most of the individual KT-QoL items (Fig. 1 and Supplementary Table S1). Over time, there was little change in the KT-QoL of the AS group (Fig. 1 and Supplementary Table S1). In contrast, the Lobectomy group showed an overall increase in KT-QoL scores. After 12 months, there was no significant difference in all QoL dimensions between the AS and Lobectomy groups (Fig. 1). There was no statistical difference in overall KT-QoL scores between the AS group and the Lobectomy group at 12 months (7.2 ± 1.2 vs. 7.1 ± 1.2, p = 0.592) and 24 months (7.3 ± 1.2 vs. 7.1 ± 1.2, p = 0.142). At 24 months, among the KT-QoL items, the AS group had significantly higher scores than the Lobectomy group only in weight gain, dry skin/hair changes, change in self-concept, and efficiency outside of work. However, there were no statistical differences in the other items (Supplementary Table S1). In the Lobectomy group, there was no difference in QoL between patients who underwent open surgery and those who underwent robotic surgery (β 0.34, CI −0.23 to 0.31, p = 0.797).
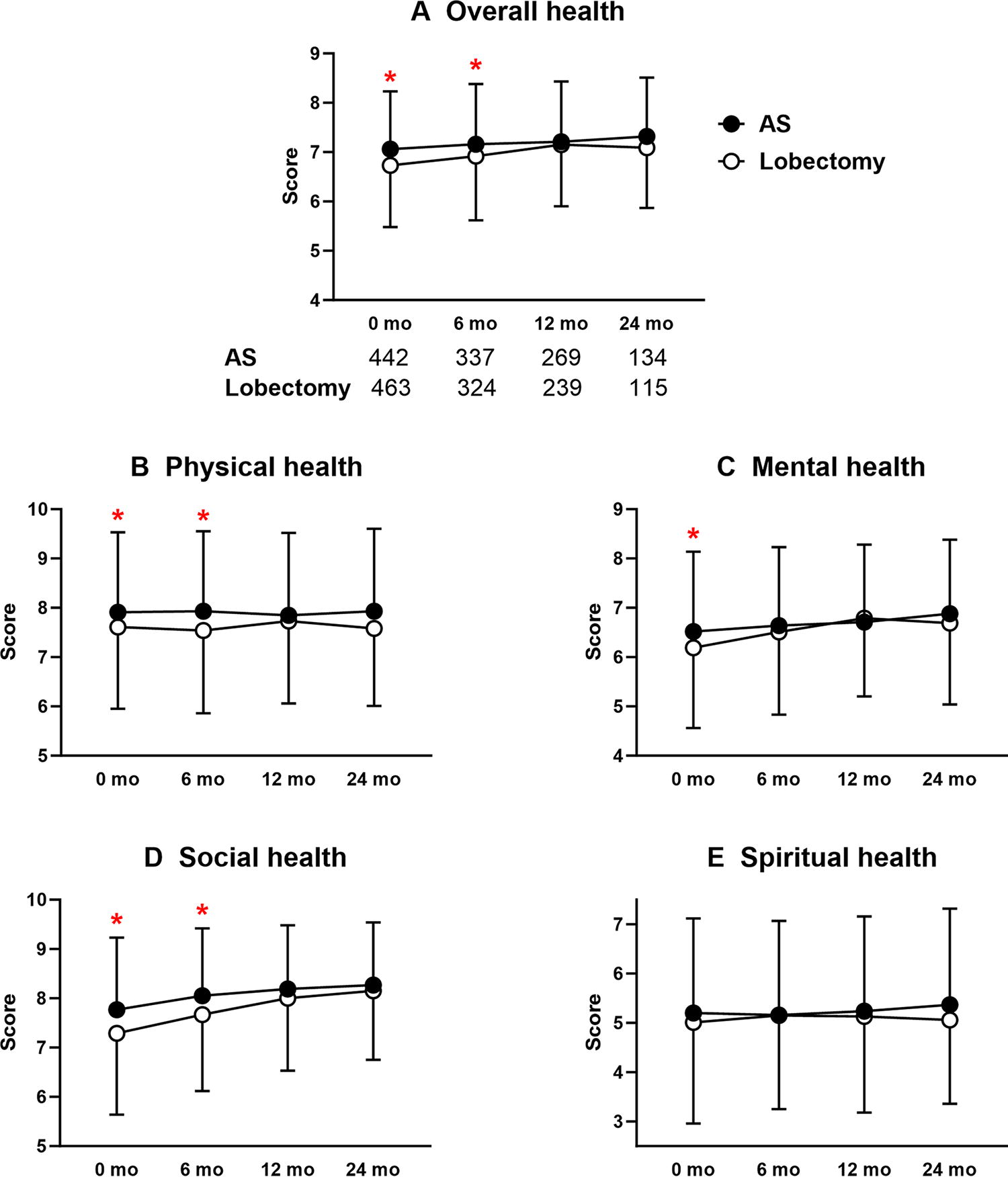
Longitudinal changes of a Korean version of the self-reported thyroid-specific quality of life (KT-QoL) scores in active surveillance (AS) and Lobectomy groups.
Discussion
This study including 927 patients with low-risk PTMC demonstrated that older age, smaller tumor size, family history of thyroid cancer, prior awareness of AS, and higher income level were significantly associated with the choice of AS. QoL assessments showed that the AS group reported initially higher KT-QoL scores in various dimensions, including physical, mental, and social health. Over time, the KT-QoL scores for the AS group remained stable, whereas those for the Lobectomy group increased, resulting in comparable scores between the two groups after 12 months.
In this study, age, tumor size, family history of thyroid cancer, prior awareness of AS, and income level were associated with the decision to choose AS. AS is a feasible option even for patients <60 years. However, given that younger patients tend to experience more disease progression 15 and have a longer life expectancy, it is the ideal choice for patients >60 years. 16 Consequently, physicians tend to prefer AS in older patients. 17 Previous studies also reported older age as a predictor of the choice of AS. 4,6 Not only physicians’ preferences but also patients’ preferences influence the decision. Patients who had a family history of thyroid cancer and prior knowledge or awareness of AS were more likely to choose AS. Unfortunately, this study did not collect information on how patients became aware of AS, whether they learned from family members, other physicians, or through mass media. This is a limitation of the study. This study suggests that patients were informed about AS before consulting with a physician and already had a preference for it, leading to a higher selection of AS. This indicates the importance of promotion and education regarding AS as a feasible treatment option. Additionally, our study is the first to report the association between high income level and the preference for AS, although the reasons behind this trend remain unclear. Surgery is more cost-effective over time but has a significant upfront cost. 18 –20 Therefore, although it might be expected that patients with lower incomes would be more likely to choose AS due to its lower upfront cost, the opposite was observed. Thus, it could be speculated that the higher frequency of choosing AS among patients with higher incomes may not necessarily be influenced by medical costs. Instead, it is possible that their greater financial and psychological resources allow them the flexibility to opt for AS.
This study revealed that the AS group generally had better KT-QoL scores compared with the Lobectomy group, aligning with findings from previous research. 5,10,21 Interestingly, even before undergoing surgery, the baseline KT-QoL scores in the Lobectomy group were significantly lower than in the AS group. The diagnosis of thyroid cancer can profoundly impact patients, potentially diminishing their QoL. It is possible that patients who suffered a significant drop in QoL following the cancer diagnosis were more tend to choose surgery. Fear and concerns associated with cancer could make patients more attentive to minor physical symptoms such as fatigue and increased mental stress, leading them to opt for the more aggressive intervention. Sawka et al. reported that the fear of cancer progression played a significant role in patients opting for surgery. 6 Conversely, those whose QoL remained relatively unaffected and stable after cancer diagnosis may have been more likely to choose AS. As patients can experience postoperative complications such as hypoparathyroidism and vocal cord palsy after thyroid surgery, the QoL scores during the early period remain lower in patients who underwent surgery than those under AS. However, as time passes, the KT-QoL scores in the Lobectomy group increase, eventually resulting in no significant difference in the KT-QoL scores between the Lobectomy and AS groups. The first reason may be the resolution of surgical complications. The permanent surgical complications are very low in patients with low-risk PTMC. Oda et al. have reported a 1.6% of permanent hypoparathyroidism and 0.2% of vocal cord palsy among 974 patients who underwent immediate surgery at Kuma Hospital. 22 Hwang et al. have reported that among 384 patients who underwent immediate surgery, only one patient experienced permanent hypoparathyroidism and another patient suffered from permanent vocal cord palsy. 23 Therefore, as temporary surgical complications resolve, physical QoL may be improved. Chen et al. also reported that QoL temporarily worsened following thyroid surgery but recovered over the course of a year. 24 The second reason for the improvement of QoL in the Lobectomy group may be the reduction in fear about cancer due to its removal through surgery. In addition, age, male sex, and Bethesda category V were significantly associated with better KT-QoL scores in this study. The reason for better KT-QoL scores in patients with Bethesda category V was difficult to determine. Patients may have been reassured by the possibility that the Bethesda V thyroid nodules are not cancer.
A key consideration in interpreting the results of our study is that we enrolled only patients who were expected to undergo thyroid lobectomy, not total thyroidectomy. Our study focuses on comparing the clinical outcomes of AS and immediate lobectomy for patients with low-risk PTMC to ensure a better comparison. Previous studies comparing QoL between AS and surgery typically included both thyroid lobectomy and total thyroidectomy, with total thyroidectomies accounting for 20–25% of surgeries. Notably, patients undergoing total thyroidectomy often experience more postoperative complications and lower QoL than those undergoing lobectomy. Consequently, the QoL levels reported for the surgery group in our study, which included only lobectomy patients, are likely higher than those in other studies including both surgical types. Previous studies have reported that AS has significant advantages over surgery in terms of QoL, supporting its use as a feasible and safe treatment option for thyroid cancer. 5,10,21 However, when the extent of surgery is limited to lobectomy alone and compared with AS, the advantages of AS in terms of QoL are significantly reduced. Our cohort continues to enroll participants and plans to continue long-term follow-up until 2030. Further analysis is planned to deepen our understanding of these findings.
This study has several limitations. First, we excluded patients who underwent total thyroidectomy, making our study population different from real-world practice. Second, 15.4% were lost to follow-up during the 2-year study period and the rate of loss to follow-up was significantly higher in the Lobectomy group (18.1%, 86/474) than in the AS group (12.6%, 57/453) (p = 0.019). In Korea, health care accessibility is very high, and it is common for patients to change hospitals to get a second opinion, which may explain the loss to follow-up. The higher rate of loss to follow-up in the Lobectomy group may be because patients who decided to have surgery often switched to another hospital if the surgery date was delayed or sought out more renowned surgeons. In contrast, because AS does not involve an immediate procedure, patients may have had fewer reasons to change doctors or hospitals. The difference in the rate of loss to follow-up between the two groups could have influenced the QoL results. However, in both groups, there was no statistically significant difference in baseline KT-QoL scores between those who remained in the study and those who were lost to follow-up (7.1 ± 1.2 vs. 6.8 ± 1.2, p = 0.136 in the AS group and 6.8 ± 1.2 vs. 6.5 ± 1.3, p = 0.139 in the Lobectomy group, respectively). Therefore, the difference in the rate of loss to follow-up is unlikely to have had a significant impact on the QoL results. Finally, this is an interim analysis of our prospective cohort, and the final results may change after patient enrollment is completed. We have plans to analyze the long-term clinical outcomes, including disease progression rate, QoL, and cost-effectiveness, between AS and lobectomy. Especially, cost-effectiveness is an important aspect of QoL, but it was not analyzed in this study. Previous studies in Korea have shown that the initial cost of lobectomy is much higher than that of AS. 20 However, health care costs in Korea are very low, with the cost of lobectomy and related costs being $839, compared with $7967 for lobectomy alone in the United States. 25
In conclusion, this study demonstrated that older age, smaller tumor size, family history of thyroid cancer, prior knowledge of AS, and higher income were significantly associated with the choice of AS among patients with low-risk PTMC. Although QoL scores initially differ between the AS and Lobectomy groups, they become comparable after 12 months. These findings give important information for shared decision-making between patients with low-risk PTMC and physicians regarding their treatment options.
Footnotes
Authors’ Contributions
Conceptualization: W.B.K., E.K.L., C.Y.L., M.J.J., and J.H.M. Data curation: M.J.K., W.B.K., E.K.L., C.Y.L., S.W.C., H.-S.B., Y.S.L., Y.E.K., H.-C.K., J.L., M.K. M.J.J., and J.H.M. Formal analysis: M.J.K., H.W., and J.H.M. Writing—original draft: M.J.K., H.W., M.J.J., and J.H.M. Writing—review and editing: M.J.K., W.B.K., E.K.L., C.Y.L., S.W.C., H.-S.B., Y.S.L., Y.E.K., H.-C.K., J.L., M.K., M.J.J., and J.H.M.
Author Disclosure Statement
No potential conflict of interest relevant to this article was reported.
Funding Information
This research was supported by a grant from the Korea Health Technology R&D Project through the
Supplementary Material
Supplementary Figure S1
Supplementary Table S1