
Abstract
Background:
Higher center and surgeon volume correspond to better outcomes for patients with thyroid cancer. This study aims to investigate how a hospital’s safety-net burden, the proportion of a hospital’s patients who are insured by state Medicaid plans or are uninsured, influences the outcomes of high-volume (HV) surgeons.
Methods:
We performed a retrospective cohort study of all patients who underwent surgery for thyroid cancer in California from 1999 to 2017. We stratified treating facilities by the proportion of Medicaid-type and indigent payors into safety-net burden quartiles. We compared the perioperative and oncologic outcomes of HV surgeons (annual case volume ≥10) for patients undergoing total thyroidectomy across safety-net burden quartiles. A mixed-effects regression model controlled for surgeon random effects and fixed effects of patient and tumor characteristics.
Results:
Our sample comprised 42,347 patients (78% female, median age 50), of whom 13,848 (32%) were treated by HV surgeons (n = 276). Compared to patients of lower-volume surgeons, patients of HV surgeons were more likely to be White, from the upper quartiles of socioeconomic status and well insured (all p < 0.001). HV surgeons in each hospital’s safety-net burden quartile displayed similar case number distributions. Compared to patients treated by HV surgeons at Q1 (lowest safety-net burden) hospitals, those treated by HV surgeons at Q4 (highest safety-net burden) hospitals had higher absolute risks of endocrine complications (+7%, p = 0.007), airway complications (+6%, p = 0.004), disease-specific mortality (+1.3%, p = 0.046), and all-cause mortality during the study period (+3%, p = 0.046) in multivariable analysis.
Conclusion:
The performance of HV thyroid cancer surgeons differs by a hospital’s safety-net burden, with patients treated at high safety-net burden hospitals experiencing higher rates of operative complications, disease-specific mortality, and all-cause mortality. Having a HV surgeon alone may be insufficient to provide optimal short- and long-term outcomes for patients with thyroid cancer.
Introduction
Although the 5-year survival rate for well-differentiated thyroid cancer approaches nearly 100%, 1 racially and financially marginalized patients are more likely to experience adverse outcomes along the thyroid cancer continuum of care, which spans from cancer prevention to the survivorship period. 2 –6 The current thyroid cancer treatment paradigm has endorsed referral of patients to high-volume (HV) surgeons and centers, but there are both geographic and racial inequities in access to these HV surgeons and centers. 7 –11 Identifying the locus where health inequities emerge is of serious importance for those interested in reducing the well-documented inequities in thyroid cancer outcomes. While the surgeon volume–outcome and hospital volume–outcome associations for thyroid cancer are now well described, no research has yet examined how safety-net and resource-constrained settings impact clinical outcomes for patients undergoing thyroid surgery by HV surgeons.
Health care professionals operating within safety-net contexts are familiar with navigating the high-friction environment of resource constraints. The safety-net burden of a hospital, calculated as the summed percentages of Medicaid type and indigent patients, is correlated with adverse outcomes along a host of domains in the perioperative phase of care delivery. After adjusting for center volume, hospitals with a high safety-net burden have higher mortality, higher rates of surgical complications, and higher readmissions for a number of common surgical procedures. 12 –15
The current study expands on previous work to investigate whether perioperative and long-term thyroid cancer outcomes of HV surgeons differ based on the safety-net burden of the hospital where patients undergo surgery. In order to evaluate the impact of hospital resource context on outcomes, the present study evaluated the incidence of perioperative complications as well as several outcomes across the thyroid cancer continuum of care: use of guideline-concordant radioactive iodine (RAI), loss to follow-up, disease-specific mortality, and all-cause mortality. We hypothesized that HV thyroid cancer surgeons would not have the same perioperative or long-term cancer outcomes at hospitals with high safety-net burdens when compared to hospitals with low safety-net burdens. With this work, we strive to inform and drive collaborative and comprehensive efforts to reduce known inequities, while respecting the desires and needs of patients to be treated close to home 16,17 and at the hospitals of their choice.
Methods
Data and patient selection
Institutional Review Board approvals from the California Committee for the Protection of Human Subjects (IRB #14-10-1768) and the UCLA Office of the Human Research Protection Program (IRB #14-001553-CR-00005) were obtained. We reviewed data obtained through the linked California Cancer Registry (CCR) and California Office of Statewide Planning and Development Patient discharge data (OSHPD-PDD) and California Office of Statewide Planning and Development ambulatory surgery center (OSHPD-AS) data for patients with thyroid cancer diagnosed from 1999 to 2017. The CCR is the state’s repository for all diagnosed cancer cases: reporting all new cancer cases to the CCR is mandated by state law and therefore is considered a comprehensive resource that is representative of the true incidence of diagnosed thyroid cancers in the state. The linked CCR and OSHPD-PDD and OSHPD-AS databases include diagnostic, procedural, and discharge data linked by unique patient identifiers. This allows for the review of oncologic outcomes alongside both cancer-related and non-cancer-related episodes of care throughout the patient’s thyroid cancer care continuum. Our study was limited to patients with thyroid cancer who underwent thyroid cancer surgery—either a thyroid lobectomy (TL), total thyroidectomy (TT), a neck lymph node dissection, or any combination of the three, during the study period. Patient demographic characteristics were evaluated, including patient-reported race and ethnicity from the CCR, the Charleston Comorbidity Index at the time of cancer diagnosis, patient insurance status, and the patient’s Yang quintile of socioeconomic status, which are area-based economic measures extrapolated from the American Community Survey data and are the validated measures of socioeconomic status in the CCR. 18
High-volume surgeons
Based on prior research regarding the correlation between thyroid cancer surgeon annual thyroid surgery volume and improved perioperative outcomes, 19 –22 a HV surgeon was defined in this study as a surgeon performing ≥10 thyroid cancer surgeries in a particular year. In prior studies, high surgeon volume included both benign and malignant cases and set a threshold for improved outcomes at >20–25 thyroid surgeries per annum. Given that the CCR exclusively comprises malignant thyroid surgeries, and our qualitative research suggesting that a 50–50 mix of benign and malignant thyroid cancer cases is typical in busy academic, community, and rural practices, 2 we used a cutoff of 10 thyroid cancer surgeries in this study. Because surgical practices are dynamic and procedural volume of individual surgeons can change dramatically throughout their career, each surgeon’s volume was reviewed for each year of the study. Thus, outcomes were evaluated as being attributed to a HV surgeon only for the years in which they achieved that level of thyroid cancer surgical volume.
Safety-net burden
All hospitals at which HV surgeons performed thyroid cancer surgery were placed into quartiles of safety-net burden. There is no static definition for safety-net institutions: in general, the designation is used to refer to hospitals at which higher proportions of economically marginalized patients access care, often operating under significant resource constraints. 23,24 In the United States, as the only high-income nation that links insurance to employment, economically marginalized patients tend to be either uninsured or underinsured, that is, insured through Medicaid and Medicaid expansion plans. Therefore, in the United States, the payor mix representing the uninsured and underinsured is a good proxy for the extent to which a hospital serves a “safety-net” population. 12,14,15 In this study, a hospital’s safety-net burden was defined as the proportion of Medi-Cal (the California state Medicaid program that provides health care coverage to low-income individuals and families), Medicaid, and indigent payors of the total payor mix. Indigent payors include county-based safety-net programs and charity, non-reimbursed care. All hospitals at which a HV surgeon operated were ordered from the lowest proportion of safety-net burden payors to highest proportion of safety-net burden payors. These hospitals were then assigned quartile designations from the lowest safety-net burden (Q1), mid-low safety-net burden (Q2), mid-high safety-net burden (Q3), and highest safety-net burden (Q4). To test whether our results would be confounded by changes in how HV surgeons conduct their thyroid operations over time, we performed a sensitivity analysis that restricted our analysis to only patients with thyroid cancer diagnosed between 2010 and 2017.
Outcomes
Complications
As described in prior work, 2,3 CPT and ICD codes in the OSHPD-PDD and OSPHD-AS databases were operationalized in order to ascertain the occurrence of perioperative complications. These were categorized by complication subtypes: airway, nerve, wound, bleeding, and endocrine complications (Supplementary Data S1). The occurrence of a complication was treated as a binary event, regardless of the particular complication.
Oncologic outcomes
As in prior studies, the evaluation of appropriateness of adjuvant RAI treatment was based on existing guidelines for the use of patients with regional disease. 2,25 The subset analysis for adjuvant RAI treatment was limited to patients with well-differentiated thyroid cancer who had Surveillance, Epidemiology, and End Results (SEER) regional disease, who either underwent a TT as their index operation or underwent a partial thyroidectomy, followed by a completion thyroidectomy within 90 days. A binary indicator for whether or not this subset of patients received RAI was defined as “appropriate use” or “inappropriate omission,” respectively. There are no consensus guidelines for follow-up surveillance after thyroid cancer diagnosis, 24 and prolonged intervals or no further follow-up may be appropriate for low-risk cancers after a period of time. Active follow-up was therefore limited to an analysis of patients diagnosed with thyroid cancers within the final 5 years of the study period (diagnosis after December 31, 2014) and who had follow-up in the final 1 year of (any follow-up visit on January 1, 2020 or later). Lastly, overall and disease-specific mortality were evaluated.
Statistical analysis and regression modeling
Demographic and clinical characteristics were summarized with descriptive statistics to characterize the study population, and the results were analyzed by the patient’s receipt of surgery by a HV surgeon or lower-volume surgeon. Mixed-effects logistic and linear regression models were used to estimate the odds ratios and risk differences associated with hospital’s safety-net burden, with a random intercept for surgeon to account for the surgeon effect. Patient characteristics of age, sex, and their Charlson comorbidity index at the time of cancer diagnosis were included in the regression model as contributing covariates to clinical outcomes. Clinical characteristics that are associated with both worse perioperative and long-term oncologic outcomes were included in the regression model. These clinical characteristics were tumor size greater >4 cm, extrathyroidal extension, lymphovascular invasion, and high-risk thyroid cancer histopathologic variants (medullary thyroid cancer, high-risk variants of papillary and follicular thyroid cancer, and poorly differentiated and anaplastic thyroid cancer). This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines to ensure the comprehensive and transparent reporting of its observational design and findings.
Results
Demographic and clinical characteristics of the study population
Our sample comprised 42,347 patients (77% female and median age 50), of whom 13,848 (32%) were treated by HV surgeons (n = 276). The index operation for the overall patient cohort was a TT (71%), TL (26%), and TT with neck dissection (3%) (Fig. 1). Compared to lower-volume surgeons, patients of HV surgeons were more likely to be White, from the upper quartiles of socioeconomic status and insured through private, Preferred Provider Organization, and Health Maintenance Organization insurance plans (all p < 0.001) (Table 1). As a corollary, patients of lower-volume surgeons were more likely to be Black, Hispanic, Asian American, and Pacific Islander, from the lowest three quintiles of socioeconomic status and uninsured (all p < 0.001) (Table 1).
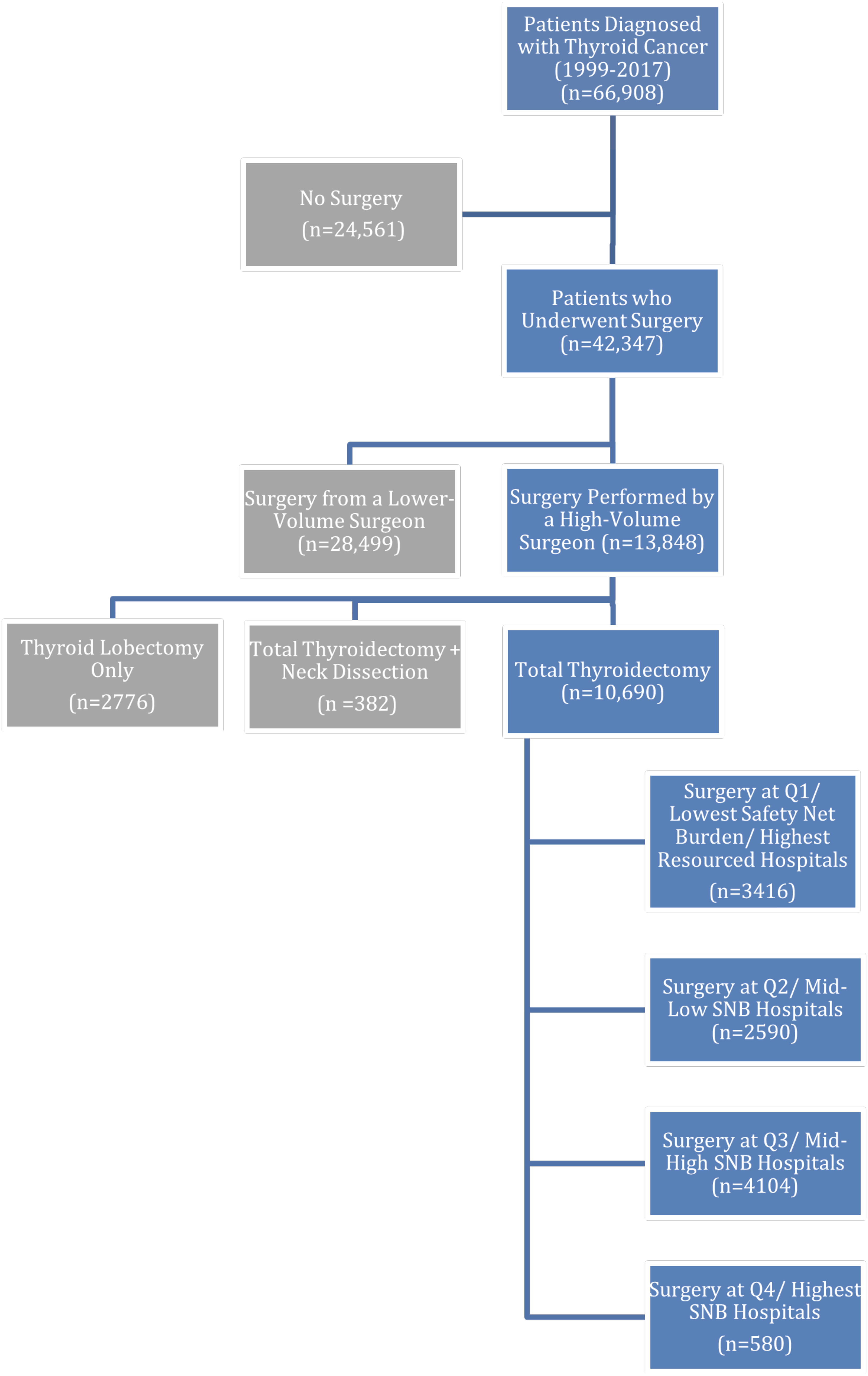
Study population.
Demographic and Clinical Characteristics of Patients Who Underwent Surgery for Thyroid Cancer (1999–2017)
Confidence intervals and p-values in bold indicate statistically significant results.
HMO, Health Maintenance Organization; PPO, Preferred Provider Organization.
Trends in regionalization and surgical volume
The number of thyroid cancer operations increased steadily from 1999 until the mid-2010s (Fig. 2). By the end of the study period, surgeons in the state of California were performing 234% more thyroid cancer operations than at the beginning of the study period. In tandem, an increasing proportion of thyroid cancer operations was being performed by HV surgeons, with 9% of thyroid cancer cases being performed by HV surgeons in 1999 versus 42% in 2017 (Fig. 2). The 132 hospitals in study that provided thyroid cancer care had significant variation in the percent of Medicaid-type and uninsured patients (defined in this study as safety-net burden) in their payer mix. Specifically, Q1 hospitals had 31–56% Medicaid-type and uninsured patients, Q2 had 57–68%, Q3 had 68–80%, and Q4 had 80–93%.

Trends in thyroid cancer surgery, including the proportion of thyroid cancer operations performed by high-volume surgeons over the study period.
Of all thyroid cancer operations performed by HV surgeons, Q1 hospitals hosted 32% of cases, while Q2 hospitals hosted 24% of cases, Q3 hosted 38% of cases, and Q4 hosted 4% of all HV surgeons’ cases.
There was no significant difference in HV surgeons’ thyroid cancer volume by hospital safety-net burden quartile (Fig. 3). HV surgeons in each hospital safety-net burden quartile displayed similar case number distributions (Q1 lowest safety-net burden: median annual thyroid cancer surgical volume 19 (interquartile range [IQR] 19); Q2 mid-low safety-net burden: 20 (IQR 23); Q3: mid-high SNB 22 (IQR 21); and Q4: highest safety-net burden 26 (IQR 30). HV surgeons frequently operate at more than one safety-net burden quartile in a given year: 67% of HV surgeons operated at ≥2 different safety-net burden quartiles (30% operate at 2 different safety-net burden quartiles, 26% at 3 different safety-net burden quartiles, and 11% operate at all hospitals from all 4 safety-net burden quartiles within a given calendar year).

Violin plot of annual thyroid cancer case volume of individual high-volume surgeons (≥10 thyroid cancer operations/year) by safety-net burden quartile, demonstrating no significant between-group variation in surgical volume by safety-net burden quartile.
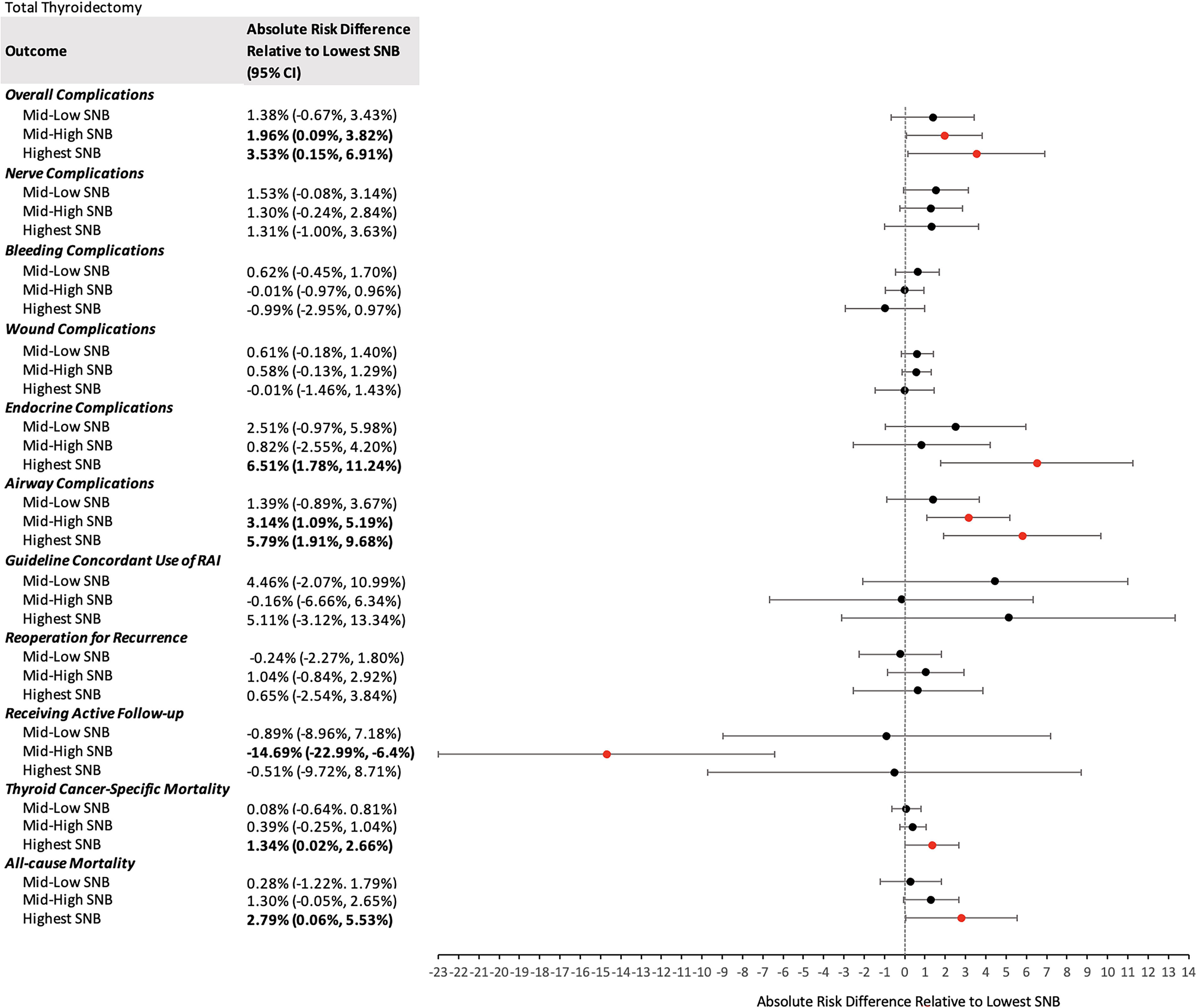
Forest plot demonstrating changes in absolute risks for patient undergoing total thyroidectomy at mid-low, mid-high, and highest safety-net burden hospitals when compared to receipt of thyroid cancer surgery at the lowest SNB hospitals. Bold text and red dots indicate statistically significant findings. RAI, radioactive iodine.
Perioperative complications
Compared to patients treated by HV surgeons at Q1 hospitals, those treated by HV surgeons at both Q3 and Q4 hospitals had significantly increased absolute risks of overall complications (+2.0%, p = 0.04 and +3.5%, p = 0.04, respectively) and airway complications (+3.1%, p = 0.003 and +5.8%, p = 0.004, respectively). Patients treated by HV surgeons at Q4 hospitals had significantly higher rates of endocrine complications (+6.5%, p = 0.007) compared to those treated at Q1 hospitals. Patients receiving surgery at Q2 hospitals had no significant differences in absolute risk of all-cause complications, compared to those receiving surgery at Q1 hospital, nor in subsets of complications. (FIG. 4.) (Table 2)
Occurrence of Perioperative and Oncologic Outcomes Among Patients Undergoing Total Thyroidectomy by a High-Volume Surgeon, by Safety-Net Burden Quartile
(Q1 = lowest safety-net burden, where there is the lowest proportion of Medicaid-type and indigent payors).
Receipt of guideline concordant adjuvant RAI
Compared to patients treated by HV surgeons at Q1 hospitals, those treated by HV surgeons at both Q2, Q3, and Q4 hospitals had similar likelihoods of receiving guideline-concordant adjuvant RAI.
Loss to follow-up
Patients receiving surgery at Q2 and Q4 hospitals had no significantly lower odds of receiving active follow-up for thyroid cancer when compared to those treated at Q1 hospitals. Patients receiving surgery at Q3 hospitals had significantly lower odds of receiving active follow-up for thyroid cancer when compared to those treated at Q1 hospitals.
Disease-specific and all-cause mortality
Patients at Q4 hospitals, when compared to Q1 hospitals, had higher absolute risks of thyroid cancer-specific mortality (+1.3%, p = 0.05) and all-cause mortality during the study period (+2.8%, p = 0.05) in multivariable analysis. Patients receiving surgery at Q2 and Q3 hospitals had no significant differences in all-cause mortality.
Sensitivity analysis
A sensitivity analysis was performed to ensure our results were not confounded by changes in how thyroid surgery was performed over time. Given that the percentage of thyroid operations performed by HV surgeons plateaued following 2010, we conducted our analysis only on patients diagnosed between 2010 and 2017 (n = 7,328). When limited to this more contemporary cohort, there was no significant differences in the associations between safety-net burden quartile and disease-specific mortality, all-cause mortality, or complications.
Discussion
Our study elucidated both trends in thyroid cancer care and the possible effects on patients being served by HV surgeons at high safety-net burden hospitals. First, our study demonstrates that thyroid cancer surgery underwent a transformation in health services delivery over the past 20 years: thyroid cancer operations are increasingly performed by HV surgeons at regional hubs. In tandem, significant inequities in perioperative and oncologic outcomes, even among those receiving their care by HV surgeons, demonstrate that the hospital resource context plays a central role in shaping outcomes. Specifically, we found that patients treated by HV surgeons at hospitals with high safety-net burdens had significantly higher rates of overall, nerve, airway, and endocrine complications. They are also more likely to experience worse outcomes along the thyroid cancer continuum of care, including more frequent loss to follow-up and higher both disease-specific and overall mortality.
Existing literature highlights the challenges faced by racially, economically, and geographically marginalized patients in accessing equitable and high-quality thyroid cancer care. 2 –4,26 The push toward regionalization, demonstrated in the increasing proportion of care being delivered by HV surgeons at low safety-net burden hospitals, may have had unintended consequences, as has been shown in the past for those who are unable to travel long distances for cancer care for a host of social and economic reasons. 17,27 In particular, the suggestion that patients continue to be referred to regional hubs for surgery by a HV thyroid surgeon may be problematic. Adjacent surgical oncology literature has demonstrated that regionalization of cancer surgery has resulted in worsened inequities for some demographic groups. 7,9,11 Hospitals vary widely with respect to resource abundance, infrastructure, and multidisciplinary knowledge and support, factors that may moderate the positive impact that a HV surgeon alone is able to have on a patient’s thyroid cancer trajectory.
In this study, we documented increased absolute risks of operative complications for patients undergoing surgery by HV surgeons at high safety-net burden hospitals compared to those undergoing surgery by HV surgeons at low safety-net burden hospitals. Given the spectrum of complications incurred (nerve, airway, and endocrine), there is unlikely to be a single factor explaining these increased risks. Rather, these increased perioperative risks may arise from a broad array of limitations including resource constraints, unaddressed social needs, long-wait times, personnel shortages, high staff turnover, and inefficient care delivery models that converge to create a high-friction environment. For these reasons, providing the highest standard of care at high safety-net burden hospitals can be difficult, despite sufficient knowledge, expertise, and technical skill on the part of the individual provider. 24,28 Higher safety-net burden is associated with lower compliance on a number of Surgical Care Improvement Project standards, including a number of infection prevention metrics, and higher rates of delay in the provision of emergency care. 12 Thus, our findings are consistent with surgical literature from other disciplines regarding the influence of safety-net burden on patient outcomes.
We acknowledge several limitations to this retrospective study. Our study relies on administrative and registry data, which may lack detailed clinical information, be coded differently across different sites, and may not capture all relevant patient outcomes. Additionally, the study may have more limited generalizability as it only includes data from the California health care system: patients in different states or nations with divergent health care infrastructures and policies may experience different outcomes.
Policy implications
Our findings demonstrated that a HV surgeon is not sufficient to guarantee parity of outcomes for racially and economically marginalized patients, particularly those receiving care at high safety-net burden hospitals. Addressing these disparities will likely require the implementation of quality improvement (QI) initiatives to assess the root causes of elevated complication rates at high safety-net burden hospitals, focusing on adequate resource allocation, staff training, and improving the efficiency of cancer care delivery. With robust QI initiatives, we believe that low-volume and low-resource hospitals are capable of providing the highest quality cancer care. 29,30 Next, policy efforts should incentivize collaboration and multidisciplinary care that would traverse different safety-net burden quartiles. Examples may include participation in regional multidisciplinary tumor boards, regional quality standard review boards for thyroid cancer, and the promotion of longitudinal collaboration between high-resource, HV institutions, and lower-resource, lower-volume institutions. The goal of reducing inequities in care delivery is dependent on regional expertise not remaining concentrated in a few, well-resourced institutions
The performance of HV thyroid cancer surgeons differs by a hospital’s safety-net burden, with patients treated at high safety-net burden hospitals experiencing higher rates of operative complications, higher disease-specific mortality, and higher all-cause mortality. Having a HV surgeon alone may be insufficient to provide optimal short- and long-term outcomes for patients with thyroid cancer.
Footnotes
Acknowledgment
The authors thank Dr. Joshua Tiao and Dr. Yusuke Tsugawa for guidance on defining Safety-Net Burden.
Authors’ Contributions
H.H.H-P.: Conceptualization, methodology, and writing—original draft, Y.V.M.: writing—original draft and review and editing, C.-H.T.: methodology and formal analysis, J.K.: methodology and formal analysis, D.W.C.: methodology and writing—review and editing, J.X.W.: methodology and writing—review and editing, and M.W.Y.: supervision, methodology, and writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
H.P. was supported by the
Supplementary Material
Supplementary Data S1