
Abstract
Background:
Thermal ablation is a minimally invasive treatment for benign thyroid nodules, but its impact on subsequent thyroidectomy and pathological evaluation is uncertain. This study investigates whether preoperative ablation complicates thyroidectomy and poses challenges for pathological diagnosis.
Study Design:
This retrospective cohort study used prospectively collected institutional registry data on patients with benign thyroid nodules who underwent thyroidectomy after prior radiofrequency ablation. Perioperative outcomes, including thyroidectomy difficulty scale (TDS) and macroscopic adhesion score (MAS), were compared with a control group without prior ablation. Histopathological and cytological changes within the ablated zone and periphery were also evaluated.
Results:
This study included 165 patients, with 145 in the nonablation group and 20 in the postablation group (17 females, mean age 53.4 years, mean nodule size 4.4 cm, mean interval between ablation and thyroidectomy 29.5 months). Compared with the nonablation group, the ablation group had longer operative time (99.5 vs. 69.5 minutes, p < 0.05), higher TDS (9 vs. 6, p < 0.05), more severe MAS (anterior 50.0% vs. 16.6%, p < 0.05; posterior: 35.0% vs. 16.6%, p < 0.05), and increased incidental parathyroidectomies (10.7% vs. 1.6%, p < 0.05). Histopathologically, the ablated area showed acellular hyalinization (95%), coagulative necrosis (60%), and chronic inflammation (85%). Both central and peripheral regions displayed cytological alterations (nuclear enlargement, focal chromatin clearing, and clear-cell change). Challenges in defining tumor capsule integrity were noted in eight follicular neoplasms, complicating the diagnosis of three follicular carcinomas and two follicular tumors of uncertain malignant potential.
Conclusions:
Thermal ablation of thyroid nodules may be associated with increased surgical difficulty and adhesion formation during subsequent thyroidectomy. Additionally, ablation-induced tissue alterations can potentially complicate pathological diagnosis. However, due to the small number of study cases, further confirmatory research is needed.
Introduction
Despite being the standard treatment for symptomatic benign thyroid nodules, surgery now faces competition from minimally invasive thermal ablation techniques, which offer effectiveness with a favorable complication profile. 1 –3 The postablation volume reduction rate (VRR) ranges from 50% to 80%. 4,5 The adoption of radiofrequency ablation (RFA) has been increasing globally. 6 While precise global utilization data are limited due to the absence of a centralized registry, its growing popularity is evident in regions such as Asia. 7,8 From 2016 to 2020, the number of RFA procedures increased, and more than 1500 patients with benign thyroid nodules were treated in Taiwan. 7 However, a substantial proportion of patients still require retreatment or surgery after initial thermal ablation. A recent multicenter study found that thyroidectomy comprised 60% of retreatments, affecting roughly 10% of those initially treated with thermal ablation. 6 This raises concerns, prompting questions with future surgical resection and histological diagnosis due to thermal ablation potentially altering tissue planes.
Studies show postablation tissues exhibit varying degrees of inflammation, 9 –11 potentially complicating thyroidectomy similar to surgery for thyroiditis (longer operative time, higher complication rates). 12 Several critical structures are located in the perithyroidal area, and surgeons are concerned about the added difficulty of thyroidectomy due to previous ablation, which may result in severe adhesions or fusion of these critical structures. 13,14 Limited data suggest postablation thyroidectomy often differs from nonablation cases. One study reported two postablation thyroidectomies and found no evidence of perithyroidal fibrosis, suggesting minimal surgical interference. 10 However, a small number of cases may not accurately represent the true condition.
RFA of benign nodules likely follows a similar pathological course to laser ablation, with progressive macrophage-mediated reabsorption of necrotic tissue and subsequent fibrosis. 11,15 Prior research suggests RFA for benign thyroid nodules prioritizes symptom relief through debulking, not complete ablation. This approach, with the active tip kept within the nodule, might leave undertreated zones near the capsule. 16 However, this approach can lead to a high rate of regrowth of the incompletely treated nodule margin. 17 –20 Therefore, a more aggressive procedure, involving the tip crossing the tumor capsule, has been suggested with an understanding of the critical structures in the perithyroidal area. 14,21 However, the tip crossing the tumor capsule could potentially result in capsular disruption, hindering histological assessment of capsular invasion, and, thus, precluding optimal assessment of malignancy.
This study investigates if thermal ablation before thyroidectomy increases surgical difficulty, complications, or pathology diagnosis challenges. We compared patients with and without prior ablation regarding intraoperative, postoperative, and histopathological findings. We hypothesize that ablation may lead to greater surgical difficulty and hinder pathological diagnosis.
Materials and Methods
Patient eligibility and study design
This is a retrospective cohort study conducted using prospectively collected institutional registry data from
Participant flowchart. RFA, radiofrequency ablation.
Baseline Characteristics of Patients Who Underwent Thyroidectomy with Prior Thermal Ablation
Values are presented as mean ± standard deviation or number of patients unless otherwise indicated.
dL, deciliters; μIU, micron international units; mL, milliliters; ng, nanograms;TI-RADS, Thyroid Imaging Reporting & Data System; T4, thyroxine; TSH, thyrotropin.
This cohort (ablation group) was compared with a control group of patients who underwent thyroidectomy for benign thyroid nodules without prior RFA (nonablation group) during the same study period (Table 2). The study excluded patients with prior neck/thyroid surgery, head and neck cancer, or history of radiation therapy to the neck.
Comparison of Demographic and Clinical Parameters between Patients Who Underwent Thyroidectomy with Prior Thermal Ablation and Those without Ablation
Values are presented as mean ± standard deviation or number (percentage, %) of patients unless otherwise indicated.
Continuous variables were compared using Student’s t-test and analysis of variance.
Categorical variables were compared using the chi-square test or Fisher’s exact test.
Fisher’s exact test.
Chronic lymphocytic thyroiditis.
BMI, body mass index; BH, body height; BW, body weight; cm, centimeters; kg, kilograms; m2, square meter.
Thyroid RFA
Benign thyroid nodules were confirmed by fine needle aspiration (FNA) cytology. 22,23 The indications for RFA at our institution included nodule-related cosmetic and/or compressive symptoms, nodules that continued to grow and willingness to undergo RFA therapy. 7,23,24 Patients provided their consent and chose the minimally invasive procedure after comprehensive discussions with the surgeons regarding the indications. 24 Typically, a single session would be dedicated to treating the predominant thyroid nodule causing symptoms. However, if there are other nodules on the same side that also contribute to the symptoms, they are addressed in the same session. After RFA, follow-up was conducted at 3, 6, and 12 months. 24
The decision for subsequent thyroidectomy was recorded.
Surgical difficulty and adhesion assessment
We evaluated adhesion between the thyroid gland and surrounding tissues (strap muscles anteriorly and posterior danger triangle) using Zühlke’s macroscopic adhesion score (MAS) as follows
25
: Grade 1: Filmy adhesions—easy to separate by blunt dissection (no vascularization). Grade 2: Minimally adhesions—blunt dissection possible, but partly sharp dissection possible (beginning of vascularization). Grade 3: Strong adhesions—adhesions requiring sharp dissection (obvious vascularization). Grade 4: Dense adhesions—lysis possible by sharp dissection only (organ strongly attached with severe adhesions, and damage of organs hardly preventable).
Thyroidectomy difficulty was objectively assessed using Schneider’s thyroidectomy difficulty scale (TDS), a 4-parameter scoring system (vascularity, friability, mobility/fibrosis, and gland size) with a maximum score of 20 (most difficult). 26 Scores ≥6 were classified as difficult.
Immediately following the operation, the 4-grade MAS and 20-point TDS scores were completed by the independent, experienced endocrine surgeons (M-.H.W., K-.Y.C., and T-.C.K.), each performing more than 100 operations annually. Perioperative clinicopathological outcomes, including operative time, blood loss, and postoperative complications such as recurrent laryngeal nerve (RLN) injury and hypoparathyroidism, were recorded meticulously. Hypoparathyroidism was defined as a serum intact parathyroid hormone (PTH) level below 10 pg/mL and a calcium level below 2.15 mmol/L. Postoperative RLN injury or hypoparathyroidism was categorized as transient if they resolved within 3 months and as permanent if they persisted beyond 3 months. Incidental parathyroidectomy in the pathological findings was also documented.
Histopathological examination
Following thyroidectomy, benign thyroid nodules underwent routine paraffin embedding and hematoxylin and eosin staining for histopathological analysis. Two pathologists (H-.W.H. and K.C.) evaluated the slides and confirmed the pathology diagnoses, assessing cytomorphological alterations in “central” (within the ablated zone) and “peripheral” (within 1 cm of the ablation zone) areas. Lesions with changes in both areas were categorized as “diffuse.” Additionally, an independent senior pathologist (J-.Y.J.) rereviewed the slides with malignant findings. Immunohistochemical stains for neuroblastoma rat sarcoma (NRAS) Q61R, 27 galectin-3 (Gal-3), Hector Battifora mesothelial cell-1, 28 and BRAFV600E mutation (VE1) 29 were performed on selected samples as potential malignancy markers. Immunohistochemical staining for PAX8 and CD68 was performed to identify the cells as follicular cells and histiocytes, respectively.
Statistical analysis
We used descriptive statistics to summarize the data. Categorical variables are presented as percentages, while continuous variables are shown as means with standard deviations or medians with interquartile ranges (IQRs) depending on data distribution. Student’s t-test or analysis of variance was used for continuous patient characteristics, and chi-square or Fisher’s exact test for categorical variables. All analyses were performed in SAS 9.4 (SAS Institute) with two-sided p-values and a significance level of 5%.
Results
A total of 445 patients underwent RFA for benign nodules at our institution during the study period. Of these, 20 patients (4.5%) required subsequent thyroidectomy (Fig. 1).
The age of participants was 53.4 ± 15.1 years (range: 26.8–80.1 years). Of these, 17 were female and 3 were male. The nodule volume decreased from 49.5 ± 42.4 mL to 18.2 ± 20.9 mL after a 6-month follow-up, representing a mean volume reduction of 67.8 ± 19.56%. The Thyroid Imaging Reporting & Data System classification of the index nodule for ablation was as follows: before ablation, 12 were TR3 and 8 were TR4; 6 months after ablation, 6 were TR3, 11 were TR4, and 3 were TR5; prior to surgery, 6 were TR3, 11 were TR4, and 3 were TR5, respectively (Table 1).
The interval between ablation and surgery was 29.5 ± 27.9 months (range: 3.9–128.8 months). The nodule volume prior to surgery was 26.4 ± 33.3 mL. Thirteen patients underwent FNA cytology prior to surgery, and the results were as follows: two were Bethesda 1, eight were Bethesda 2, one was Bethesda 3, and two were Bethesda 4. The decisions for surgery were depicted as follows: 10 were for nodule regrowth or suboptimal VRR, 5 were due to patient preference, 3 were due to suspicious ultrasonic features, and 2 were based on cytology indicating a follicular neoplasm. None of them were under levothyroxine treatment at last follow-up prior to surgery. Serum thyrotropin and thyroxine (T4) levels were within normal range before ablation (0.9 ± 0.9 μIU/mL and 1.2 ± 0.2 ng/dL) and prior to surgery (0.8 ± 0.9 μIU/mL and 1.0 ± 0.5 ng/dL), respectively (Table 1).
Surgical changes
This study compared 20 patients in the ablation group and 145 patients in the nonablation group. There was no statistically significant difference in demographic and clinical parameters, including age, sex, body mass index, nodule size or volume, thyroiditis, extent of thyroidectomy, presence of multiple nodules, and pathological diagnosis between the two groups (Table 2).
The ablation group showed no significant difficulty with vessel ligation, and the recurrent nerves as well as parathyroid glands were readily identified. In the comparison of surgical outcomes, shown in Table 3, the mean operative time was significantly longer in the ablation group (99.5 ± 46.3 vs. 69.5 ± 21.5 min, p = 0.010). This difference likely reflects the increased adhesion severity observed in the ablation group. However, ablation resulted in challenges, including altered thyroid tissue consistency with visible scarring and increased adhesions, particularly between the thyroid and strap muscles. Despite encountering challenges due to prior ablation, there were no major postoperative complications such as RLN palsy, hematoma requiring reoperation, hypocalcemia, or levothyroxine treatment after surgery in the ablation group. However, the ablation group experienced a significantly higher rate of incidental parathyroidectomy (incidence per lobe: 3/28 [10.7%] vs. 3/185 [1.6%], p = 0.031). This difference is likely due to the presence of severely adherent parathyroid glands near the ablation zone in three patients from the ablation group.
Comparisons of Surgical Outcomes Between Patients Who Underwent Thyroidectomy with Prior Thermal Ablation and Those Without Ablation
Values are presented as mean ± standard deviation, median (interquartile range, IQR), or number (percentage, %) of patients unless otherwise indicated.
Continuous variables were compared using Student’s t-test and analysis of variance.
Categorical variables were compared using the chi-square test.
Statistically significant, p < 0.05.
Statistically significant, p < 0.01.
Statistically significant, p < 0.001.
min, minutes; RLN, recurrent laryngeal nerve.
When adhesion in the anterior area and posterior danger triangle were evaluated using the MAS, the nonablation group had 65 patients with Grade 1 and 56 with Grade 2 adhesions. In the ablation group, two had Grade 1, eight had Grade 2, eight had Grade 3, and two had Grade 4 adhesions. This indicated significantly higher adhesion severity in the ablation group, with a greater proportion of patients exhibiting severe MAS (grade 3/4), while the nonablation group had more patients with lower grades (1/2) (p < 0.001). In the posterior danger triangle, the nonablation cohort had 66 patients with Grade 1 adhesions and 55 with Grade 2 adhesions. In contrast, the ablation group had four with Grade 1, nine with Grade 2, five with Grade 3, and two with Grade 4 adhesions. This indicates that the ablation group had significantly higher adhesion severity in this area compared with the nonablation group, with a larger 15 proportion of patients exhibiting Grade 3/4 adhesions, while the nonablation group predominantly had Grade 1/2 adhesions (p = 0.048).
The surgical difficulty, assessed by the TDS, was significantly greater in the ablation group (median score 9, IQR 7.5–9) compared with the nonablation group (median score 6, IQR 6–7) (p < 0.001). Notably, the increased difficulty stemmed primarily from factors such as altered vascularity, friability, and mobility/fibrosis. In contrast, the gland size remained comparable between groups.
Overall, the ablation group had significantly higher operative times, rates of incidental parathyroidectomy, MAS, and TDS scores compared with the nonablation group (Table 3).
Pathological changes
The histopathological examination of the ablation group revealed 11 cases of follicular nodular disease (nodular hyperplasia), 3 cases of follicular adenoma, 3 cases of follicular carcinoma, 2 cases of follicular tumors of uncertain malignant potential, and 1 case of thyroiditis. Additionally, there was one case of follicular nodular disease accompanied by incidental papillary microcarcinoma (Table 2).
The ablated area was filled with colloid, shadows of necrotic follicles, and aggregates of inflammatory cells. Acellular hyalinization was observed in 95.0% of cases (19/20), followed by inflammation in 80.0% (16/20, predominantly chronic), and coagulative necrosis in 55.0% (11/20). Other findings included hemorrhage (9/20), calcification (8/20), blackish particles, cholesterol granuloma, and cavity formation. Among the cases showing acellular hyalinization, 73.7% exhibited hyalinization centrally, while 26.3% had hyalinization in both central and peripheral areas (diffusely). Regarding inflammation, 61.5% showed diffuse chronic inflammation, and 38.5% had inflammation with a central distribution (as shown in Fig. 2 and Table 4).
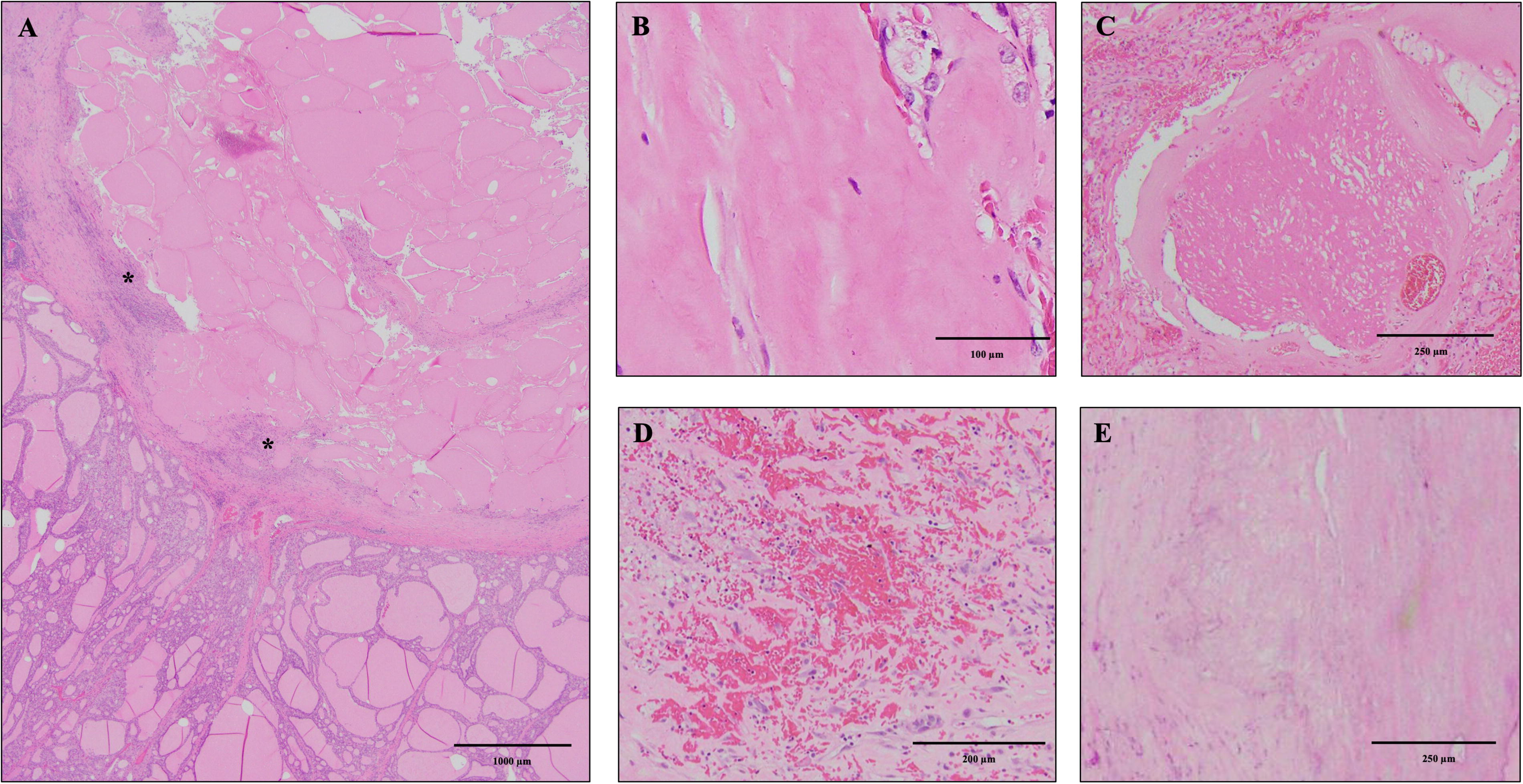
Histological features in a patient who underwent thyroidectomy with prior thermal ablation.
Histopathology Findings of Patients Who Underwent Thyroidectomy with Prior Thermal Ablation
The undertreated areas maintained follicular architecture and exhibited benign cytological characteristics. However, occasional atypical cytological changes, such as nuclear enlargement, chromatin clearing, atypical cyst lining, and clear-cell change identified both centrally and peripherally (as shown in Fig. 3 and Table 4).
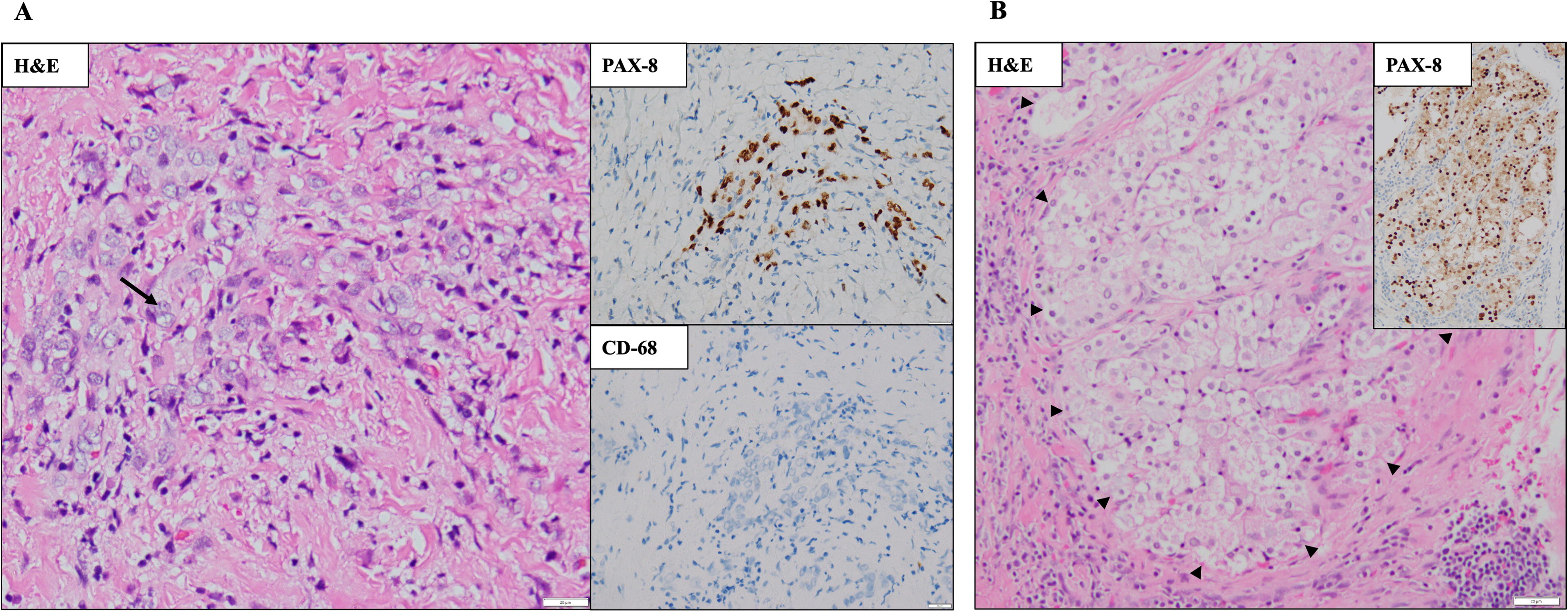
Cytological changes in residual thyroid tissue following thermal ablation. Higher magnification of follicular nodules following RFA reveals rare cytological changes within follicular cells.
Capsule and vascular invasion evaluation
In eight cases diagnosed with follicular tumors on pathological examination, the capsules of these tumors were carefully reviewed for signs of capsular invasion or vascular invasion. Three tumors had intact capsules without invasive features. Five follicular neoplasms displayed obliterated vessels adjacent to the capsules, yet the direct causality of RFA in these vascular changes remains uncertain. Assessing capsular invasion proved challenging in five cases due to irregular nodular growth caused by extensive stromal hyalinization or tissue fragmentation. This resulted in separated microfollicular regions with indistinct borders in one case. Additionally, elongated areas of stromal hyalinization could mimic capsule formation, complicating the accurate identification of tumor island invasion. Two cases were classified as follicular tumor of uncertain malignant potential.
One case revealed a tumor nest extending into the surrounding parenchyma. However, ablation-induced tissue alterations obscured the true growth pattern. Nevertheless, positive NRAS Q61R immunostaining within the tumor nest confirmed its clonal nature, establishing it as a case of true capsular invasion. In another case, a tumor nest clearly invaded the true capsule, while a separate area of stromal hyalinization simulated a capsule, further complicating the assessment. Vascular obliteration hindered the identification of potential tumor cell invasion within vessels in one case. These three cases were diagnosed as follicular carcinoma due to evidence of invasive growth, including capsular and/or vascular invasion (Fig. 4).
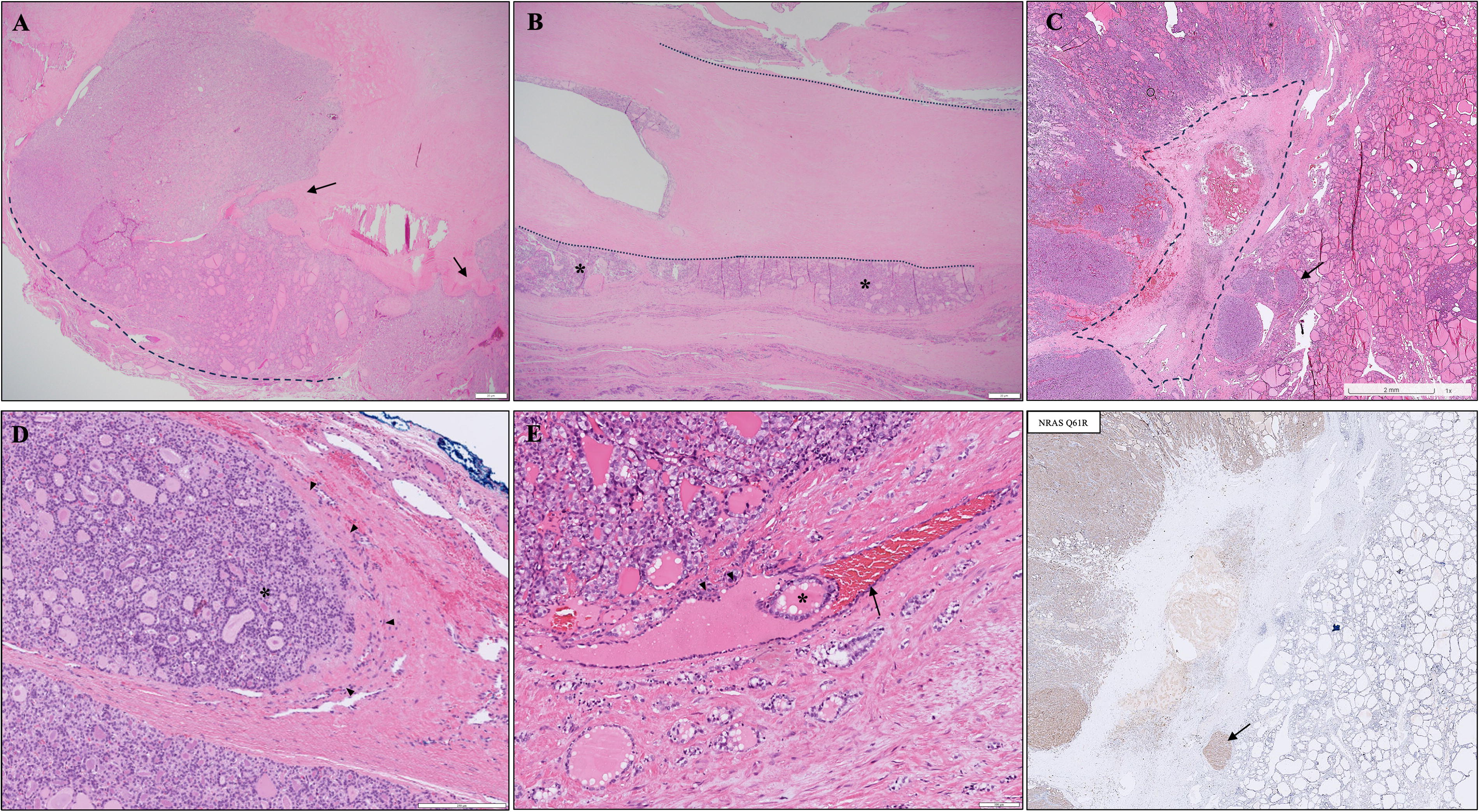
Challenges in assessing whether postablation thyroid nodules exhibit capsular and vascular invasion. Representative images illustrate the difficulty in differentiating between malignancy and postablation changes in thyroid nodules.
Furthermore, differentiating between RFA-induced hyalinization and true capsule boundaries posed a challenge, as elongated or irregularly shaped hyalinized regions often resembled capsular invasion. In one instance, a tumor nest extended into the surrounding parenchyma, exhibiting characteristics similar to the ablated primary nodule.
Discussion
Thermal ablation is employed as a treatment option for thyroid nodules; however, it can impact the subsequent surgical procedure in several ways. First, it may lead to tissue scarring, fibrosis, or changes in the texture and vascularity of thyroid nodule and surrounding tissue. These changes can potentially make it more challenging for the surgeon to differentiate and manipulate the tissue during surgery. Second, thyroid surgery demands precision in identifying and preserving critical anatomical structures, and alterations in tissue consistency or vascularity resulting from prior ablation may make it more difficult to identify and protect these structures.
Inflammation induced by ablation can indeed elevate the complexity of thyroidectomy, potentially leading to an increase in postoperative complications. McManus et al. demonstrated that the overall surgical complications were significantly higher in the thyroiditis group compared with the nonthyroiditis group. 30 Many surgeons have expressed concerns about the additional difficulties they might encounter due to the effects of RFA, and there have been limited prior studies reporting a subjective evaluation of surgery difficulty after RFA. Our results indicate that there were no significant differences in postoperative complications between the groups, consistent with recently published data. 31 However, our findings do show that patients who underwent ablation prior to thyroidectomy had a longer operative time compared with those who did not undergo ablation (99.5 [44–228] minutes vs. 69.5 [33–126] minutes, p = 0.010; Table 3).
Dissecting procedures were more difficult in patients previously treated with RFA, as indicated by higher MAS and TDS scores. In this study, we utilized these two objective scoring systems (MAS and TDS) rather than relying on personal experience as an assessment tool, providing stronger evidence compared with previous research. This indicates that RFA may indeed increase the surgical challenge. However, it is important to note that this does not mean thyroid surgery cannot or should not be performed after ablation. Surgeons should carefully consider the specific circumstances and may need to adjust their surgical approach accordingly. 32 Our study findings are consistent with previous research on the morphological changes observed after RFA. 11,15 These changes include signs of tissue damage such as histiocytes and hemorrhage, as well as indications of irreversible damage such as infarction, cavity formation, and acellular hyalinization. The heating process can also alter cellular architecture and nuclear characteristics, impacting the cytohistological diagnosis of thyroid nodules. These changes complicate the interpretation of postablation cytohistological features, as they are critical factors in cytological interpretation. In our study, we observed atypical features in follicular cells within both central and peripheral regions of the ablated zone. Notably, nuclear changes such as focal enlargement, grooves, prominent nucleoli, and chromatin clearing may mimic features of papillary thyroid carcinoma, potentially affecting the Bethesda cytological classification postablation. In a study by Piana et al., 5 out of 16 patients showed atypical cytology after ablation. 11 Similarly, in our study, 1 out of 20 patients displayed atypia, and 2 were classified as nondiagnostic according to the Bethesda system. As a result, cytopathologists must consider a patient’s ablation history when evaluating diagnostic results.
Thermal ablation may lead to fibrosis and scarring in the treated area, complicating histological assessment. A previous study reported that 11% of patients who underwent thermal ablation subsequently required thyroidectomy, with 35% of these patients showing nonbenign pathology on histological examination. 6 In our study, 3 out of 20 patients were diagnosed with malignancy, even though all had been initially considered benign during preablation evaluation. The relatively high prevalence rate of follicular carcinoma (15–25%, 3–5 out of 20) likely reflects selection bias and it may also raise some questions regarding the potential influence of RFA in neoplastic transformation. Insufficient RFA might facilitate tumor cell progression, with suboptimal heat potentially promoting angiogenesis in nontumor cells. 33 As reported by Dobrinja et al., regrowth of follicular lesions or follicular neoplasms after ablation may indicate potential malignancy. 10
In our cohort, eight out of 20 patients were ultimately diagnosed with follicular neoplasms, which is a relatively high percentage considering that their cytological classification before RFA was almost entirely Bethesda category 2. 24,34 Discrepancies may arise from small nodules yielding mixed FNA results and overlooked mixed-pattern neoplasms. Our study highlights post-RFA morphological changes in follicular neoplasms, emphasizing the need for cautious FNA interpretation. 35,36
The presence of a follicular neoplasm following thermal ablation presents unique diagnostic challenges. Differentiating between benign and malignant follicular neoplasms typically relies on identifying capsular or vascular invasion. However, thermal effects may alter capsular regions, with phenomena such as hyalinization and coagulative necrosis potentially obscuring or destroying key diagnostic features. These thermal effects may also make it difficult to distinguish between areas of hyalinization caused by RFA and the actual follicular capsule. Our findings, along with prior evidence, highlight the continuing challenges in evaluating true capsular invasion after ablation. 37 In addition, five out of eight cases showed obliterated vessels near the capsule. However, it is unclear whether these vascular changes were directly caused by RFA. This uncertainty raises a significant concern: if RFA does induce vascular obliteration, it might mask the true extent of tumor vascular invasion, potentially leading to an underestimation of the tumor’s aggressiveness. 38,39 These findings indicate the need for further investigation to understand the impact of thermal ablation on vascular structures and its implications for assessing tumor invasiveness. The treatment-induced changes may make it difficult to accurately assess malignancy, potentially leading to misinterpretation or overlooking signs of invasiveness. Strict criteria for angioinvasion, like fibrin coating on follicular nests, are crucial for predicting metastasis. 40 Collaboration between pathologists and physicians and providing with RFA history as accurate assessment is crucial to avoid overdiagnosis and misinterpretation of artifacts as malignancy, ensure precise diagnosis, optimal patient care, and well-informed treatment decisions. 36 RFA may obscure or mask invasive features, complicating diagnostic accuracy.
A limitation of our study is the relatively small sample size, which may not be generalizable to a larger population. The low rate of surgery after ablation makes it challenging to collect a large prospective cohort to thoroughly evaluate factors such as surgical adhesion and difficulty. Given that our cohort is a selected group with potential confounding factors, comparing it with the control group may be challenging. Future randomized studies are unlikely to be conducted with these patients; however, other methods to control for potential confounders may be feasible, such as propensity score matching between the groups. Additionally, our study’s outcomes from RFA may not necessarily apply to other methods using different energy sources such as microwave or high-intensity focused ultrasound. Moreover, variations in pathological characteristics may also arise from the specific technique and individual performing the procedure. We currently have to analyze the differences between patients who underwent RFA with or without subsequent thyroidectomy; further evidence is needed. In addition, molecular testing was not included in this study. While it could be informative, its diagnostic accuracy for thyroid tissue with prior ablation remains questionable. 41
Conclusions
Our study provides initial evidence suggesting that thermal ablation may increase the difficulty of future thyroidectomy by affecting the adhesion to adjacent tissue, without causing significant major complications. Additionally, RFA may alter cytology of follicular cells and disrupt the nodule capsule, thereby complicating histological assessment and pathological diagnosis. Larger prospective studies are needed to confirm our findings.
Footnotes
Acknowledgments
All the authors have read and agreed to the published version of the article. The authors would like to express their thanks to the staff of NTUH-Statistical Consulting Unit for statistical consultation and analyses. In addition, the authors thank the Department of Medical Research and Pathology (Dr. Koping Chang) of NTUH for supporting this study.
Authors’ Contributions
T-.C.K.: Conceptualization, methodology, software, validation, formal analysis, investigation, resources, data curation, writing—original draft, writing—review and editing, visualization, project administration, and funding acquisition. K-.Y.C.: Validation, investigation, data curation, resources, and supervision. H-.W.H.: Validation, data curation, and writing—original draft. J-.Y.J.: Validation, data curation, writing—review and editing. M-.T.L.: Investigation, resources, visualization, supervision, and funding acquisition. C-.H.C.: Software and formal analysis. M-.H.W.: Conceptualization, methodology, validation, supervision, resources, data curation, writing—review and editing, visualization, project administration, and funding acquisition.
Author Disclosure Statement
Each author listed (T-.C.K., K-.Y.C., H-.W.H., J-.Y.J., M-.T.L., C-.H.C., and M-.H.W.) had no relevant financial disclosure.
Funding Information
The work was supported in part by grants from NTUH (111-S0125) and the Ministry of Science and Technology (110-2314-B-002-047).