
Abstract
Background:
Exposure to particles with an aerodynamic diameter of ≤2.5 μm (PM2.5) is associated with the occurrence of thyroid dysfunction among pregnant women and neonates, but it is not known if this association occurs in the general population. We aimed to determine the association of prolonged exposure to PM2.5 with the prevalence of thyroid disorders among adults in China.
Methods:
A nationally representative cross-sectional study of thyroid disorders, iodine status, and diabetes status was carried out in all 31 provinces across China from 2015 to 2017. In total, 73,900 adults aged 18 years and older were included. Serum concentrations of thyroid hormones, thyrotropin, and thyroid antibodies and the urine iodine concentration were measured. The environmental concentration of PM2.5 for each participant’s residential address at a spatial resolution of 1 × 1 km was estimated.
Results:
The average long-term exposure to PM2.5 at residential addresses was 66.41 μg/m3, ranging from 17.58 μg/m3 to 120.40 μg/m3. Compared with that of individuals with lower exposure levels, the prevalence of thyroid diseases such as autoimmune thyroiditis and subclinical hypothyroidism was greater in those with PM2.5 concentrations within the third quartile range (60.18 to 73.78 μg/m3). Compared with those in the first quartile (17.58 to 46.38 μg/m3), participants in the highest PM2.5 quartile (73.78 to 120.40 μg/m3) presented an increased risk of overt hypothyroidism (OR 1.23 [CI 0.94–1.61]), subclinical hypothyroidism (1.10 [1.01–1.21]), autoimmune thyroiditis (1.09 [1.00–1.18]), and thyroglobulin antibody positivity (1.17 [1.07–1.29]). However, there was no association between PM2.5 exposure and overt hyperthyroidism, subclinical hyperthyroidism, Graves’ disease, or thyroid peroxidase antibody positivity (p > 0.05). Each 10 μg/m3 increase in the PM2.5 concentration was associated with an increased risk of overt hypothyroidism (OR 1.05 [1.00–1.11]), subclinical hypothyroidism (1.02 [1.00–1.03]), and thyroglobulin antibody positivity (1.02 [1.00–1.04]). Furthermore, a nearly linear exposure–response relationship was observed between long-term PM2.5 exposure and thyroglobulin antibody positivity.
Conclusions:
PM2.5 exposure was associated with thyroid disorders among Chinese adults. A dose–response relationship between PM2.5 exposure and autoimmune thyroiditis, as well as thyroglobulin antibody positivity, was also observed.
Introduction
Environmental air pollution, specifically particulate matter (PM2.5, particles with an aerodynamic diameter ≤2.5 μm), has been acknowledged as a pervasive global environmental and public health concern. 1 The World Health Organization (WHO) data show that almost all of the global population (99%) breathes air that exceeds the WHO’s annual mean PM2.5 standard, which is set at 10 μg/m3, with low- and middle-income countries having the highest exposure. 2 Pollution is the most common environmental cause of disease and premature death worldwide. 3 A Global Burden of Disease study estimated that air pollution contributed to 213.3 million healthy life years lost due to premature death and disability in 2019. 4
Exposure to air pollution has been reported to be associated with a range of adverse health outcomes, including cardiovascular diseases and respiratory conditions. 3 –5 Thyroid disease, specifically subclinical hypothyroidism, is among the most prevalent endocrine disorders. 6 Subclinical hypothyroidism has been reported to be associated with an increased risk of coronary events and mortality, as well as increased cancer-related mortality, diabetes, and other related conditions. 7
While the relationship between iodine intake and thyroid disorders remains significant, previous surveys have indicated that even with adequate iodine intake, the prevalence of subclinical hypothyroidism among the Chinese population is 12.9%. 8 Several studies have documented the detrimental impact of exposure to environmental air pollution on thyroid function. 9,10 Given the potential link between air pollution and maternal thyroid hormone deficiency, as well as impaired neurodevelopment in children, most related studies have focused on mothers or newborns, with less attention given to the general population. 11 –13 Previous research has been limited to specific geographic areas and lacks representativeness. 12 Furthermore, some studies have analyzed city-wide levels of pollution exposure rather than individual-level pollution exposure, which can lead to inaccurate estimates. 14 Before 2013, the absence of a conventional air quality monitoring network in China hindered epidemiological studies on the chronic health effects of PM2.5 exposure. This study utilized the Space-Time Extra-Trees (STET) model to obtain high-quality, high-resolution (1 × 1 km) data on PM2.5 exposure levels. 15
This study integrated pollutant data with a nationally representative cross-sectional study conducted across 31 provinces of China from 2015 to 2017. The aim of this study was to evaluate the relationship between long-term PM2.5 exposure and the prevalence of thyroid diseases in the general population of China.
Methods
Sampling and study population
The Thyroid disorders, Iodine status, and Diabetes Epidemiological (TIDE) study, which was conducted from 2015 to 2017, was a population-based cross-sectional investigation. A comprehensive description of the study design has been previously published elsewhere. 8,16 A detailed flowchart outlining the study’s methodology is presented in Supplementary Figure S1. Briefly, 31 provincial regions in mainland China were considered. A nationally representative sample was obtained through a multistage stratified random sampling method based on demographic data, including age, sex distribution, urban–rural proportions, and 2010 national census data. 17 In total, 80,937 Chinese adults (≥18 years old) were invited to participate in the survey, and 73,900 individuals were included in the final analysis. Because this study focused on the general adult population in China, the inclusion criteria for the study participants were as follows: (1) aged 18 years and older, (2) residing in the selected community for a minimum of 5 years, (3) not taking iodine-containing medications or contrast agents within the past three months, and (4) not pregnant. Individual information about each participant and the results of thyroid ultrasonography were obtained by trained interviewers who were proficient in data collection and qualified physicians who were trained by the same instructor, respectively. The questionnaire included demographic variables, behavioral factors, family history of chronic diseases, and personal medical history. Ultrasonography was performed using the same ultrasonic frequency instrument (LOGIQ 100 PRO, 7.5 MHz; GE Healthcare). Fasting blood and spot urine samples were collected from each participant. All samples were transported through a cold chain system to the central laboratory in Shenyang, China, for centralized testing. The levels of serum thyrotropin (TSH), thyroid peroxidase antibodies (TPOAbs), and thyroglobulin antibodies (TgAbs) were measured using an electrochemiluminescence immunoassay on a Cobas e601 analyzer (Roche Diagnostics) in a central laboratory in Shenyang. Serum-free thyroxine (fT4) and free triiodothyronine (fT3) levels were measured only if the level of TSH was outside the reference range. The urinary iodine concentration (UIC) was determined through inductively coupled plasma mass spectrometry (Agilent 7700x; Agilent Technologies).
The research protocol was approved by the Ethics Committee of the First Hospital of China Medical University. Following a comprehensive explanation of the research procedures, written informed consent was provided by all participants.
Air pollution exposure assessment
This study used the STET model to integrate remote sensing, meteorological, and land use data for estimating PM2.5 environmental concentrations at a spatial resolution of 1 × 1 km. The detailed methodologies have been previously published elsewhere. 18
On the basis of this model, we determined the monthly PM2.5 exposure concentration for each participant’s residential address from 2010 to 2017 using longitudinal and latitudinal data. We subsequently derived the average monthly PM2.5 concentrations for the past five years at the time of questionnaire completion.
Diagnostic criteria
The diagnostic criteria for thyroid disorders are listed in Table 1.
Diagnostic Criteria for Thyroid Disorders
fT3, free triiodothyronine; fT4, free thyroxine; TgAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody; TRAb, TSH receptor antibodies; TSH, thyrotropin.
Statistical analyses
We present participant characteristics as the means with corresponding confidence intervals (CIs) for continuous variables and percentages with CIs for categorical variables. The Kruskal–Wallis test was used to compare groups for continuous variables, whereas categorical variables were analyzed using χ2 tests or Fisher’s exact tests. To estimate the overall population characteristics of Chinese adults in the general population aged 18 years and older in this study, computations were weighted using the 2010 Chinese Population Census data along with the sampling scheme of the present survey. The weighting coefficient represented the inverse of the adjusted probability for respondents to acquire the data; each case in the analysis was assigned a specific coefficient (individual weight) derived by multiplying the coefficient by the actual population sharing the same sex, age, province, and location characteristics.
We categorized the participants into four groups according to quartiles of exposure to PM2.5 (17.58 to 46.38 μg/m3, 46.38 to 60.18 μg/m3, 60.18 to 73.78 μg/m3, and 73.78 to 120.40 μg/m3). We utilized generalized linear models to compute the adjusted odds ratios (ORs) and CIs for examining variations in the prevalence of thyroid disorders at different PM2.5 exposure levels. Adjustments were made in the models for several potential confounding factors. In Model 1, we adjusted for age and sex. Model 2 was further adjusted for race/ethnicity, body mass index (BMI), UIC, education level, average annual household income, smoking history, family history of thyroid disorders, and urbanization. Based on Model 2, interaction terms were incorporated to estimate the potential effect of PM2.5 exposure on thyroid disorders. The statistical significance of any interaction was assessed, prompting subsequent stratification of risk factors if deemed significant (Supplementary Tables S1–S5). The associations between PM2.5 concentrations and thyroid disorders were evaluated on a continuous scale with restricted cubic spline curves on the basis of weighted generalized linear model analysis. This approach allowed for the exploration of potential nonlinear effects and facilitated the construction of an exposure–response curve. Multiple comparisons were also performed (Supplementary Table S7). In addition, the ORs for the risk of thyroid disorders per 10 μg/m3 increase in PM2.5 exposure level were estimated.
A bilateral p value of <0.05 was considered statistically significant. All the statistical analyses were performed using R software, version 4.2.3.
Results
In the TIDE project, 87,900 individuals were invited to participate, and a total of 80,937 participants completed the survey, yielding an overall response rate of 92.1%. Information from 73,900 participants was utilized for the present analysis after excluding those lacking details on age and sex (n = 167), thyroid function testing (n = 2300), and specific residential addresses (n = 4570) (Fig. 1).
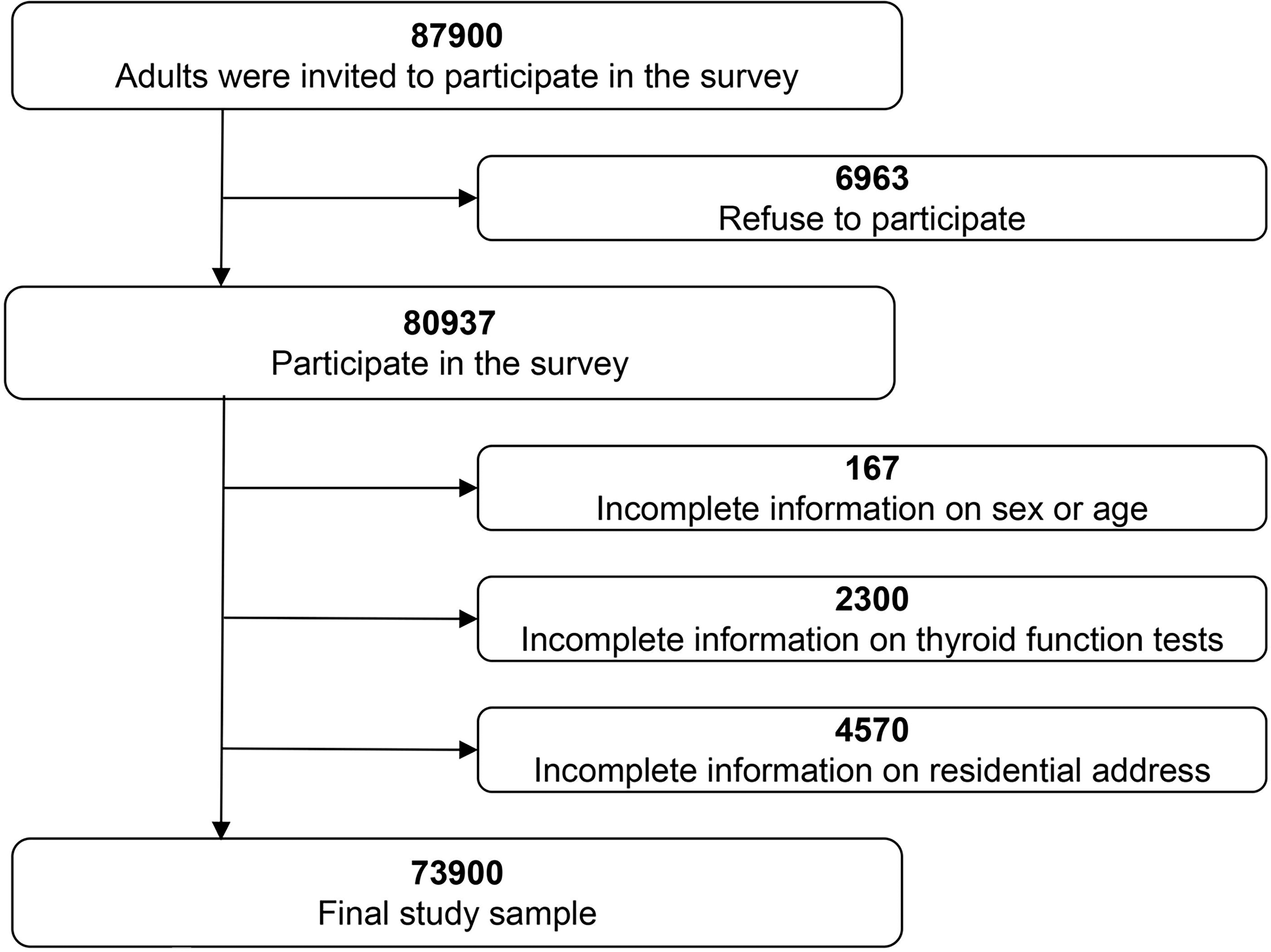
Flowchart of study participants included and excluded in analyses.
Characteristics of participants
Table 2 presents the background characteristics of the study population categorized by overall levels and quartiles of PM2.5 exposure. Overall, 73,900 individuals were included, 52.4% of whom were male (n = 37,560). Overall, 46.8%, 66.0%, and 94.6% of the participants were aged younger than 40 years, had less than a high school education, and had no family history of thyroid disorders, respectively. The median UIC in the general adult population was 251.83 µg/L. Approximately 40.22% of the general adults had UICs ranging between 100 and 200 μg/L. From 2000 to 2017, participants were exposed to an average PM2.5 concentration of 66.41 μg/m3 in their residential areas, ranging from 17.58 μg/m3 to 120.40 μg/m3. Compared with the group exposed to lower levels of PM2.5, the group exposed to higher levels had a smaller proportion of smokers but a higher BMI and UIC.
General Characteristics of Adults Living in Mainland China and According to Quartiles of PM2.5 a Concentrations
Values are percentage (confidence interval) unless stated otherwise.
Particles of diameter ≤2.5 μm.
Associations between PM2.5 and thyroid disorders
Table 3 presents the prevalence of thyroid disorders in individuals with different levels of PM2.5 exposure. Overall, the weighted prevalence of autoimmune thyroiditis was 13.9% (CI 13.5–14.2) and that of subclinical hypothyroidism was 12.8% (12.5–13.2). Notably, the prevalence of TgAb positivity increased with increasing PM2.5 exposure. Moreover, we observed that participants with a higher prevalence of thyroid disorders were primarily exposed to PM2.5 concentrations in the third quartile.
Weighted Prevalence of Thyroid Disorders according to Quartiles of PM2.5 a Concentrations
Values are percentage (confidence interval) unless stated otherwise.
Particles of diameter ≤2.5 μm.
Table 4 presents the crude and adjusted ORs and CIs for the association of thyroid disorder risk with long-term exposure to PM2.5. We observed an association between higher levels of PM2.5 (compared with first-quartile PM2.5 levels) and an increased risk of subclinical hypothyroidism (in the third (OR 1.10 [CI 1.01–1.20]) and fourth (1.10 [1.01–1.21]) quartiles). The risk of overt hypothyroidism and autoimmune thyroiditis was found to be highest under the PM2.5 concentrations in the third quartile, with a 40% (OR 1.40 [CI 1.10–1.78]) increase in the risk of overt hypothyroidism and a 12% (1.12 [1.03–1.21]) increase in the risk of autoimmune thyroiditis, as determined by Model 2 in the multivariate analysis. In addition, after Model 2 was implemented for variable adjustments, an increase of 10 μg/m3 in the PM2.5 concentration was associated with an increased risk of overt hypothyroidism (1.05 [CI 1.00–1.11]) and subclinical hypothyroidism (1.01 [1.00–1.03]). We observed a significant association between higher levels of PM2.5 exposure and an increased risk of TgAb positivity. Even after adjusting for multiple variables, this association persisted. The ORs of participants exposed to PM2.5 concentrations in the second, third, and fourth quartiles were 1.05 (CI 0.95–1.15), 1.14 (1.04–1.25), and 1.17 (1.07–1.29), respectively. An increased odds of TgAb positivity was associated with a 10 mg/m3 increase in the PM2.5 concentration (OR 1.02 [CI 1.00–1.04]). However, no associations were found between PM2.5 exposure and the risk of overt hyperthyroidism, subclinical hyperthyroidism, Graves’ disease, or TPOAb positivity. Further analysis of the associations between autoimmune thyroiditis-related hypothyroidism and an increased risk of autoimmune overt hypothyroidism and exposure to PM2.5 was conducted for the third (OR 1.82 [CI 1.32–2.49]) and fourth (1.71 [1.20–2.42]) quartiles. A 10 μg/m3 increase in the PM2.5 concentration was significantly associated with an 11% increase in the prevalence of autoimmune overt hypothyroidism (1.11 [1.05–1.18]) after multivariate adjustment in Model 2 (Supplementary Tables 6).
Thyroid Disorders Weighted Prevalence Associated with Long Term Exposure to Fine Particulate Matter (PM2.5) * . Values are Odds Ratios (95% Confidence Intervals) Unless Stated Otherwise
Particles of diameter ≤ 2.5 μm. Crude model: unadjusted model. Model 1: adjusted for age and sex. Model 2: Model 1 + adjusted for ethnicity, body mass index, urine iodine concentration, education, average annual household income, smoking history, family history of thyroid disorders and urbanization.
Fig. 2 shows the exposure–response curve depicting the association between thyroid disorders and PM2.5 levels. The analysis revealed that PM2.5 concentrations in the third quartile range (60.18 to 73.78 μg/m3) were associated with the highest risks of overt hypothyroidism, subclinical hypothyroidism, and elevated TSH levels. However, across the entire range of PM2.5 concentrations, we observed a linear concentration–response correlation between the PM2.5 concentration and both autoimmune thyroiditis and TgAb positivity.

Multivariable adjusted odds ratios for all thyroid disorders according to levels of PM2.5 on a continuous scale. Note: Solid purple lines are multivariable-adjusted odds ratios, with shaded areas lines showing confidence intervals derived from restricted cubic spline regressions with three knots. Analyses were adjusted for age, sex, race/ethnicity, body mass index, urine iodine concentration, education, average annual household income, smoking history, family history of thyroid disorders, and residential addresses. ORs, odds ratios; PM2.5, particles of diameter ≤2.5 μm; TgAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody; TSH, thyrotropin.
Subgroup and sensitivity analyses
The Supplement presents subgroup analyses, sensitivity analyses, and multiple comparisons related to fluctuations in thyroid disease prevalence associated with PM2.5 levels. None of the sensitivity analyses yielded significant deviations from our primary model outcomes (Supplementary Tables S1–S5). In both our primary analysis (Table 4) and sensitivity analyses (Supplementary Tables S1–S5), there was no evidence supporting an association between subclinical hyperthyroidism and exposure to PM2.5. The stratification results for the risk factors are detailed in the appendix (Supplementary Tables S1–S5).
Discussion
To our knowledge, this study is the first to estimate the relationship between long-term exposure to PM2.5 at a spatial resolution of 1 × 1 km and the prevalence of thyroid disorders in the general adult population. Our findings reveal the associations between prolonged exposure to elevated levels of PM2.5 and increased risks of overt hypothyroidism, subclinical hypothyroidism, and autoimmune thyroiditis. Even within subgroup and sensitivity analyses, these associations remained robust.
In the present study, the average concentration of PM2.5 was 66.41 μg/m3, nearly seven times greater than that recommended by the WHO air quality guideline (10 μg/m3). 2 The analysis revealed a 5% increase in the risk of overt hypothyroidism with every 10 μg/m3 increase in the PM2.5 concentration. Consequently, compared with the PM2.5 level recommended in the WHO standard, the risk among the Chinese general adult population exposed to the average PM2.5 concentration is estimated to increase by more than 30%.
This study underscores the associations between long-term exposure to PM2.5 and increased risks of overt hypothyroidism and subclinical hypothyroidism among adults in the general population. This finding is consistent with the findings of previous studies conducted on pregnant women and neonates. 10,13,19,20 Hypothyroidism has been the most extensively studied pollutant-associated thyroid disorder in recent years. A previous study revealed that preconception exposure to PM2.5 increased the risk of thyroid dysfunction during pregnancy. 20 Zhao et al. demonstrated that during the first and second trimesters, there was a 28% increase (OR 1.28 [CI 1.05–1.57]) and 23% increase (1.23 [1.00–1.51]) in the risk of maternal hypothyroidism for each increase of 10 μg/m3 in the PM2.5 concentration, respectively. 12 In addition, a European cohort study yielded similar conclusions regarding exposure to PM2.5 in early pregnancy and mild thyroid dysfunction throughout pregnancy. 10 PM2.5 exposure affects pregnant mothers and can also impact the thyroid function of subsequent generations. A study based on a Chinese national database revealed a positive association between maternal exposure to PM2.5 and an increased risk of congenital hypothyroidism in offspring. 13 The present study differed from previous studies that focused on thyroid function in pregnant women and fetuses; instead, we studied the general adult population, expanding the scope of PM2.5 exposure within our research. A Mendelian randomization study provided evidence for the causal relationship between PM2.5 exposure and the risk of thyroid dysfunction. The study revealed an association between elevated concentrations of PM2.5 and an increased risk of thyroid dysfunction. Hence, air pollution control may be important for preventing thyroid dysfunction. 21
Previous studies have rarely reported the associations between air pollution exposure and autoimmune thyroid diseases. A study from Bosnia and Herzegovina failed to demonstrate the significant effects of air pollution on the incidence of autoimmune thyroiditis. 22 However, our findings indicated that a greater risk of autoimmune thyroiditis was associated with long-term exposure to high levels of PM2.5. These discrepancies in the conclusions might be attributed to varying pollution levels, differing methods of pollution estimation, and variations in exposure duration among studies, which led to differences in the levels of exposure among the participants involved in the analysis. Moreover, there was a substantial difference in the sample sizes analyzed; this study had a smaller sample size (n = 174), which could have limited its statistical power and the interpretability of the results.
Previous findings suggested that pregnant women who were TPOAb positive were more susceptible to the effects of air pollution, yet TPOAb status did not influence the relationship between air pollution exposure and fT4 levels. 12 Similarly, the present study did not find a statistically significant difference between PM2.5 exposure and TPOAb positivity. However, we observed a linear relationship between long-term exposure to PM2.5 and TgAb positivity. TgAb levels are important for the adjunctive diagnosis and treatment of autoimmune thyroiditis. 23 However, there are no reported studies on the relationship between PM2.5 exposure and TgAb positivity.
Currently, conclusive evidence linking air pollution exposure to thyroid disruption is lacking. Animal experiments suggest that exposure to PM2.5 may disrupt thyroid hormone homeostasis in female rats by affecting the negative feedback regulation of thyroid secretion controlled by the hypothalamic–pituitary–thyroid axis. 24 Perturbations in the gut–thyroid axis could also be one of the causes of thyroid toxicity induced by PM2.5 exposure. 25 PM2.5-induced thyroid toxicity leads to alterations in the gut microbiota and metabolites in rats, which can in turn influence thyroid function. Furthermore, compounds within air pollutants might disrupt estrogen receptor signaling. 26
Exposure to PM2.5 has been shown to impact human immune function, 27 and these effects are also evident in the thyroid. This study revealed a significant association between long-term exposure to PM2.5 and increased susceptibility to autoimmune overt hypothyroidism and autoimmune subclinical hypothyroidism. This association was notably stronger than that for overt and subclinical hypothyroidism (Supplementary Table S6). These findings reaffirmed that chronic inflammation due to prolonged exposure to PM2.5 disrupts the balance of the immune system, consequently increasing the risk of immune-related hypothyroidism.
The toxicity of pollutants may directly cause tissue damage or induce a cascade of pathophysiological effects through oxidative stress 28 and the activation of pro-inflammatory signals. 29 Individuals with preexisting conditions are more susceptible to the impact of particulate air pollution; 30,31 however, the detailed underlying mechanisms involved remain incompletely understood and warrant further investigation.
Strengths and limitations of this study
Compared with previous studies, this study has several advantages. First, this was a large-scale cross-sectional study based on a population comprising 31 provinces across China, with PM2.5 levels ranging from 17.58 μg/m3 to 120.40 μg/m3, thereby ensuring nationwide representativeness. Second, the assessment of PM2.5 exposure levels is important. In contrast to satellite-derived data, which possess temporal constraints and relatively coarse spatial resolutions (3–10 km), our use of the STET model yielded more accurate PM2.5 data (1 × 1 km). This approach also enables more precise analyses of urban areas and the history of pollution. Third, our study included six thyroid disorders and two thyroid antibody positivity outcomes while simultaneously adjusting for various potential risk factors, including the UIC. This comprehensive approach allowed for a more holistic evaluation of the association between the prevalence of thyroid disorders and PM2.5 exposure.
Moreover, there are limitations to this study. First, our research had a cross-sectional study design, thereby restricting causal inferences due to the constraints of an observational study design, necessitating prospective cohort studies for validation. Second, our statistical analyses did not consider other air pollutants, heavy metals, environmental noise, wildfires, or similar contaminants, limiting our access to higher quality exposure data. Furthermore, we were unable to assess the interactions among pollutants. Third, we collected environmental PM2.5 exposure data based solely on participants’ residential addresses, without accounting for their daily activity durations, occupational exposure periods, specific locations, or indoor air pollution exposure. These factors might have led to an overestimation or underestimation of participant exposure levels.
Conclusion
In summary, this study revealed an association between long-term exposure to relatively high concentrations of PM2.5 and an increased risk of thyroid disorders. However, further prospective cohort studies are needed to corroborate these findings, assess effect modifications and interactions, and examine the potential biological mechanisms involved. This research is crucial to guide future longitudinal research, environmental monitoring, and health policy development in heavily polluted low- and middle-income nations, such as China. The potential effect of air pollution exposure on thyroid disorders requires further attention.
Footnotes
Acknowledgments
The authors thank the participants of this study. For continuous support, assistance, and cooperation, the authors thank the investigators for the Thyroid Disorders, Iodine Status and Diabetes Epidemiological Survey Group.
Authors’ Contributions
Y.L., Z.S., and W.T. are joint corresponding authors. Y.L., Z.S., and W.T. conceived and designed the study. K.Y., K.C., Y.L., Z.S., and W.T. supervised the study. K.Y. and C.L. performed the statistical analysis. The Thyroid Disorders, Iodine Status and Diabetes Epidemiological Survey Group conducted the epidemiological survey. All the authors contributed to the acquisition, analysis, or interpretation of the data. K.Y. and Y.L. drafted the article. All authors revised the report and approved the final version before submission. Y.L., Z.S., and W.T. are the guarantors and attest that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Data Sharing
All the data will be made available upon request to the corresponding author. Proposals will be reviewed and approved by the sponsor, investigator, and collaborators on the basis of scientific merit. After approval of a proposal, data will be shared through a secure online platform after the signing of a data access agreement.
Author Disclosure Statement
All authors declare no competing interests.
Funding Information
This work was supported by the
Supplementary Material
Supplementary Data S1
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7