
Abstract
Background:
In this narrative review, we assess published data on subclinical hyperthyroidism (SCHyper) and its association with cardiovascular disease (CVD) in the general population.
Summary:
We present data on the risk of SCHyper in relation to CVD outcomes, including atrial fibrillation (AF), heart failure, stroke, coronary heart disease (CHD), major adverse cardiac events (MACE), CVD mortality, and all-cause mortality. Evidence indicates that SCHyper is associated with an elevated risk of AF, heart failure, MACE, CVD mortality, and all-cause mortality. SCHyper appears to have little association with stroke risk and has shown conflicting results regarding CHD risk. Regarding the degree of serum TSH suppression, evidence shows a higher risk of CVD in SCHyper individuals with suppressed TSH (<0.1 mIU/L) compared with those with low TSH (0.1–0.4 mIU/L). Despite evidence that older individuals are inherently at a higher risk for CVD, no studies have yet demonstrated an age-related increase in the relative risk of CVD in SCHyper.
Conclusion:
The studies indicate that SCHyper is associated with an increased risk of AF, heart failure, MACE, CVD mortality, and all-cause mortality. Considering the importance of the degree of serum TSH suppression and age as risk factors for CVD, treatment decisions should be individualized based on their specific risk factors.
Introduction
Subclinical hyperthyroidism (SCHyper) is a biochemical condition characterized by a low or suppressed serum concentration of thyroid-stimulating hormone (TSH), while levels of the peripheral thyroid hormones, thyroxine and triiodothyronine, remain within the normal range. 1 With widespread availability of thyroid function tests in primary care settings, SCHyper is becoming increasingly recognized. 2 SCHyper is generally asymptomatic, is often diagnosed incidentally, and may not progress to overt hyperthyroidism 1 ; therefore, the potential importance of SCHyper lies in whether it increases clinical risk of complications of hyperthyroidism.
Cardiovascular disease (CVD) is not only a leading cause of death worldwide but also has serious health, social, and economic implications. Given that overt hyperthyroidism has important impacts on the cardiovascular system
3
and the thyroid gland has crucial roles in growth, reproduction, energy metabolism, and overall human homeostasis, the relationship between SCHyper and CVD has been investigated by multiple cohorts. With the prevalence of SCHyper in the community,
4
–6
any increased risk of CVD from SCHyper could have a
We present a narrative review detailing scientific knowledge regarding the clinical aspects of SCHyper and CVD, with a focus on individuals with SCHyper and euthyroidism in the general population. We also review the existing treatment guidelines and contemplate the future research directions that should be pursued.
Etiology and epidemiology
The etiology of SCHyper can be either exogenous or endogenous. Exogenous TSH suppression may result from deliberate administration of thyroid hormones to intentionally suppress thyroid cancer or from excessive thyroid hormone replacement therapy in individuals with hypothyroidism. Common endogenous causes of SCHyper are the same as those of overt hyperthyroidism and include Graves' disease, autonomous functioning thyroid nodules, and toxic multinodular goiters. Other conditions, such as nonthyroidal illness, the administration of drugs (especially high-dose glucocorticoids or dopamine), central hypothyroidism, and the late first-trimester of pregnancy, can also present with thyroid hormone patterns similar to those seen in SCHyper. 1 This review focuses on the endogenous SCHyper.
SCHyper can be classified by the degree of serum TSH suppression. Although some literature describes these groups as either severe SCHyper (TSH <0.1 mIU/L) or mild SCHyper (TSH 0.1–0.4 mIU/L), we prefer the terms of SCHyper with suppressed TSH (TSH <0.1 mIU/L) or SCHyper with low TSH (TSH 0.1–0.4 mIU/L) 9 because most patients are asymptomatic, patients with SCHyper have milder disease than those with overt hyperthyroidism, and overt hyperthyroidism with minimally elevated thyroid hormone levels can be called mild hyperthyroidism. 9 Approximately 65–75% of SCHyper patients have SCHyper with low rather than suppressed TSH. 1 It is important to note that TSH reference ranges can vary between laboratories, with some setting the lower normal limit below 0.4 mIU/L. 5 These variations may affect the classification of SCHyper and should be considered when interpreting results. In addition, low serum TSH levels are often transient; 10 up to 50% of cases of SCHyper, likely due to Graves' disease or thyroiditis, may revert to normal thyroid function within 5 years. 11 When examining studies that investigate outcome associations based on a single abnormal TSH measurement, this transient nature should be taken into consideration.
The prevalence of SCHyper ranges approximately 1–5% and depends on factors such as age (increases with age), 4 sex (higher in women than men), 5 race/ethnicity (higher in black individuals than white individuals), 6 geography/iodine intake (higher in iodine-deficient areas than iodine-excess areas), 5 and serum TSH cutoff values. 5 The risk of progression from SCHyper to overt hyperthyroidism is approximately 1–15% per year dependent on serum TSH concentrations and cause. 12 Higher rates of progression are observed in individuals with suppressed TSH 13 –15 and those exposed to high iodine levels. 16
Mechanisms of cardiovascular disease associated with subclinical hyperthyroidism
The cardiovascular effects of thyroid hormones are on the heart (by influencing rate, rhythm, myocardial contraction, and risk of coronary artery disease), the vasculature (regulating blood pressure via smooth muscle tone and endothelial function), and effects on cardiovascular risk factors (via lipid metabolism and modulation of inflammatory pathways); these mechanisms are described in detail elsewhere. 17,18 Overt hyperthyroidism is associated with increased cardiac output, tachycardia, widened pulse pressure, and sometimes congestive heart failure and atrial fibrillation (AF). 3 The cardiovascular effects of excess thyroid hormone in overt hyperthyroidism are present to a lesser extent in SCHyper. 12 SCHyper is linked with tachycardia and premature beats, 19,20 changes in cardiac morphology and function, 19,20 susceptibility to endothelial dysfunction, 21 and/or the acceleration of atherosclerosis 22,23 in most but not all studies. 24 –27 Whether subtle increase in thyroid hormone levels is associated with long-term CVD has therefore been investigated in observational clinical studies.
Challenges in reviewing evidence and study design considerations
Proving whether SCHyper is associated with CVD is difficult, even with well-designed observational studies. CVD events may only manifest in a small proportion of individuals with SCHyper during any study period, and the prevalence of SCHyper in the general population is relatively low. Therefore, detecting the effects of SCHyper on CVD with sufficient statistical power requires an extraordinarily large sample size or an extended duration of the study. 28 Most individual cohort studies will be severely under powered.
Several study designs may help overcome issues of statistical power, including individual participant data (IPD) meta-analysis, population-based registry data, and large cross-sectional studies. IPD meta-analyses consolidate data from prospective cohort studies and are considered the gold standard for meta-analyses because they offer a standardized classification of participant characteristics or diseases/conditions, translate various definitions into a common scale, and provide update follow-up of time-to-event or other outcomes beyond what has been previously reported. 29 The Thyroid Studies Collaboration (TSC) 30,31 has played a critical role in providing high-quality IPD evidence for subclinical thyroid disease. Population-based registries, including the Copenhagen General Practitioners (GP) Laboratory, 32,33 the Thyroid Epidemiology, Audit, and Research Study (TEARS), 15 the OPENTHYRO Register cohort, 34 and the Clalit Health Medical Organization (CHMO) database, 35 and large cross-sectional studies, 36 have also been published that allow assessment of the associations between SCHyper and CVD with adequate statistical power.
Focusing on priority studies with larger sample sizes and clear event rates, as described above, we now describe data on the risk of SCHyper on the cardiovascular outcomes of AF, heart failure, stroke, coronary heart disease (CHD), major adverse cardiac events (MACE), CVD mortality, and all-cause mortality (search strategy to identify relevant literature—see online-only Supplementary Appendix SA1). For completeness, we also document individual population-based cohort studies not included in the TSC and sought to include those with more than 10 outcome events, even if they were underpowered.
Evidence for the risk of cardiovascular morbidity and mortality in subclinical hyperthyroidism
Atrial fibrillation
The TSC analysis of AF events comprised five prospective cohorts 37 –41 and involved 11,084 people (7,901 euthyroid and 810 with SCHyper). The age- and sex-adjusted analysis found that SCHyper (TSH <0.45 mIU/L) was associated with an increased risk of AF [hazard ratio (HR) 1.68; 95% confidence intervals (CI), 1.16–2.43] during a mean follow-up of 8.8 years. 30 Compared with those with euthyroidism, the risk of AF was higher for SCHyper with suppressed TSH (TSH <0.10 mIU/L) (HR 2.54; 95% CI, 1.08–5.99) than those with low TSH (TSH 0.10–0.44 mIU/L) (HR 1.63; 95% CI, 1.10–2.41).
The Copenhagen GP Laboratory study, a Danish population-based registry involving 586,460 adults (562,461 euthyroid and 6,276 with SCHyper), followed for a median of 5.5 years, demonstrated that the risk of AF increased as TSH levels decreased. 32 This ranged from high-normal euthyroidism with a TSH level of 0.2–0.4 mIU/L [incidence rate ratio (IRR) 1.12; 95% CI, 1.03–1.21), to SCHyper with a TSH level of 0.1–0.2 mIU/L (IRR 1.16; 95% CI, 0.99-1.36), and SCHyper with a TSH level <0.1 mIU/L (IRR 1.41; 95% CI, 1.25–1.59), when compared with euthyroidism (TSH 0.4–5.0 mIU/L). 32 The risk of AF in SCHyper was significantly increased after 12 months, implying the importance of early detection and treatment of SCHyper to avoid development of AF. 32 Similar findings have been reported in the Scottish Tayside population-based registry, TEARS. 15 This study investigated incident AF in 2,004 individuals with SCHyper and 10,111 controls matched by age and sex among adults aged 18 years or older who had at least two serum TSH measurements at least 4 months apart. 15 TEARS analysis found that individuals with SCHyper (TSH <0.4 mIU/L) had a higher incidence of dysrhythmia compared with those with euthyroidism over a 5.6-year period (HR 1.65; 95% CI, 1.26–2.17). 15 In addition, the risk for dysrhythmia was higher in SCHyper with suppressed TSH (TSH <0.1 mIU/L) (HR 2.07; 95% CI 1.30–3.29) than SCHyper with low TSH (TSH 0.1–0.4 mIU/L) (HR 1.52; 95% CI, 1.11–2.08). 15
In a large Austrian cross-sectional community-based population study of 23,638 adults from the city of Wels (22,300 euthyroid and 613 with SCHyper), the prevalence of AF in individuals with SCHyper (TSH <0.4 mIU/L) was almost the same as those with overt hyperthyroidism (12.7% vs. 13.8%) and significantly higher than the prevalence in those with euthyroidism 2.3% [risk ratio (RR) 5.2; 95% CI, 2.1–8.7]. 36
Figure 1 presents a compilation of all studies mentioned above 15,30,32,36 and others that included 10 or more outcomes related to AF within the SCHyper group. 42,43 Taken together, high-quality data reported to date provide evidence of an increased risk of AF in patients with SCHyper.
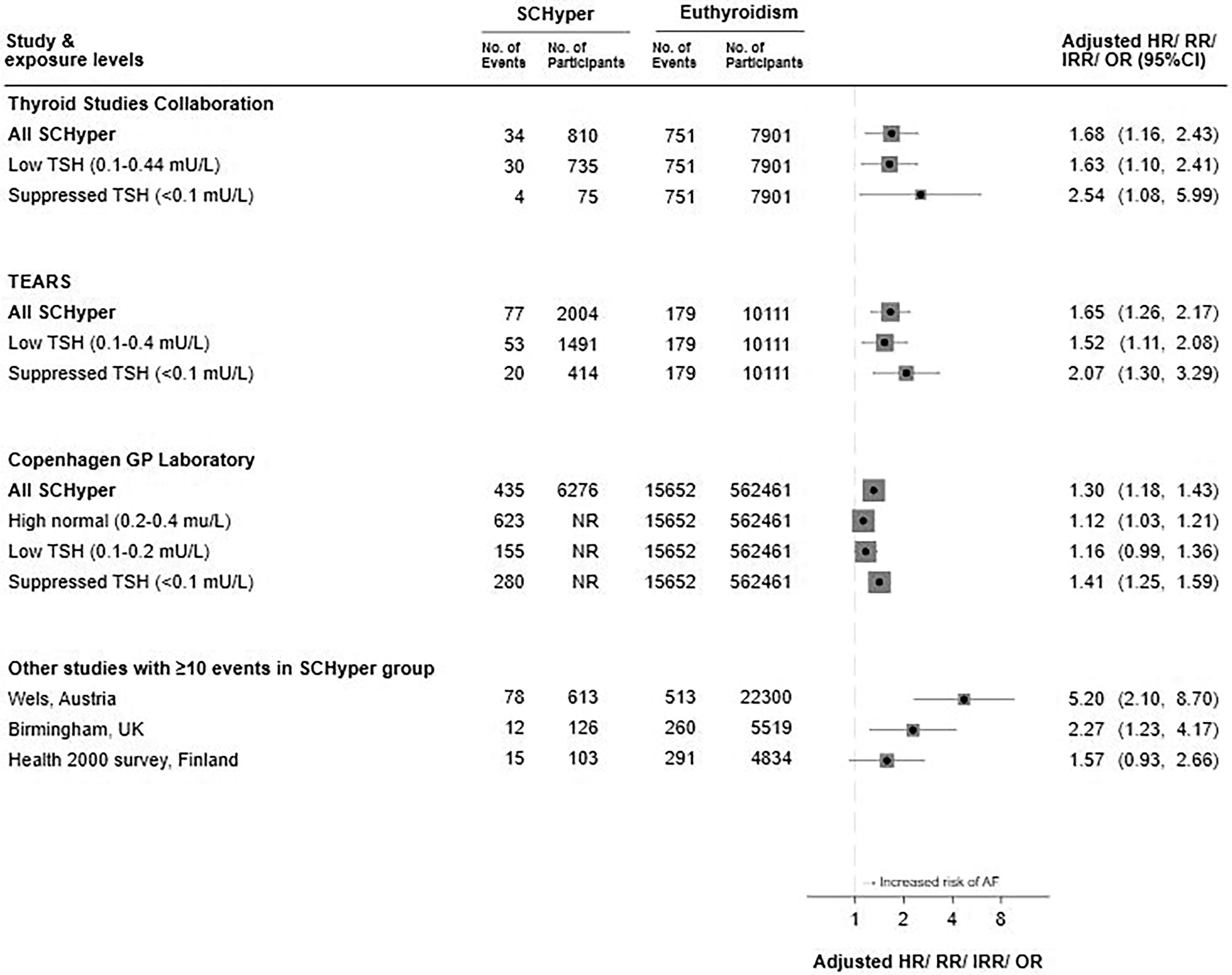
Forest plots for subclinical hyperthyroidism and risk of atrial fibrillation (figure based on references 15,30,32,36,42,43 ). SCHyper, subclinical hyperthyroidism; HR, hazard ratio; RR, risk ratio; IRR, incidence rate ratio; OR, odds ratio; CI, confidence intervals; TSH, thyroid-stimulating hormone; TEARS, Thyroid Epidemiology, Audit, and Research Study; Copenhagen GP Laboratory, Copenhagen General Practitioners Laboratory; NR, not reported; AF, atrial fibrillation. Adjusted ratio and their 95% confidence intervals are depicted using squares and solid lines. The size of each square corresponds to the number of atrial fibrillation events in individuals with subclinical hyperthyroidism. Confidence intervals for Birmingham, UK study not reported in paper but calculated via Mantel-Haenszel method based on data reported.
Heart failure
The TSC analysis of heart failure outcomes assessed 25,390 people (22,674 euthyroid and 648 with SCHyper) from six prospective cohorts 37,40,41,44 –46 with median follow-up of 10.4 years. The age- and sex-adjusted HR for heart failure events among all individuals with SCHyper (TSH <0.45 mIU/L) was 1.46 (95% CI, 0.94–2.27) compared with euthyroid people. 31 In addition, risks of heart failure events were further increased with lower TSH levels; the HR was 1.31 (95% CI, 0.88–1.95) for TSH of 0.10-0.44 mIU/L and 1.94 (95% CI, 1.01–3.72) for TSH <0.10 mIU/L (p for trend = 0.047). 31 The risk of heart failure remained similar after further adjustments for potential confounding risk factors and after the exclusion of those with preexisting heart failure or AF. 31
The Copenhagen GP Laboratory registry analysis of heart failure assessed data of 563,700 people (540,710 euthyroid and 5,979 with SCHyper), 8.4% of individuals with SCHyper experienced a heart failure event during 5.5-year median follow-up periods. 33 The IRR of heart failure in individuals with SCHyper (TSH <0.2 mIU/L) was 1.20 (95% CI, 1.10–1.31) compared with those with euthyroidism, with similar results seen across all levels of SCHyper. 33
Figure 2 summarizes all studies that included 10 or more outcomes related to heart failure within the SCHyper group. 31,33,47
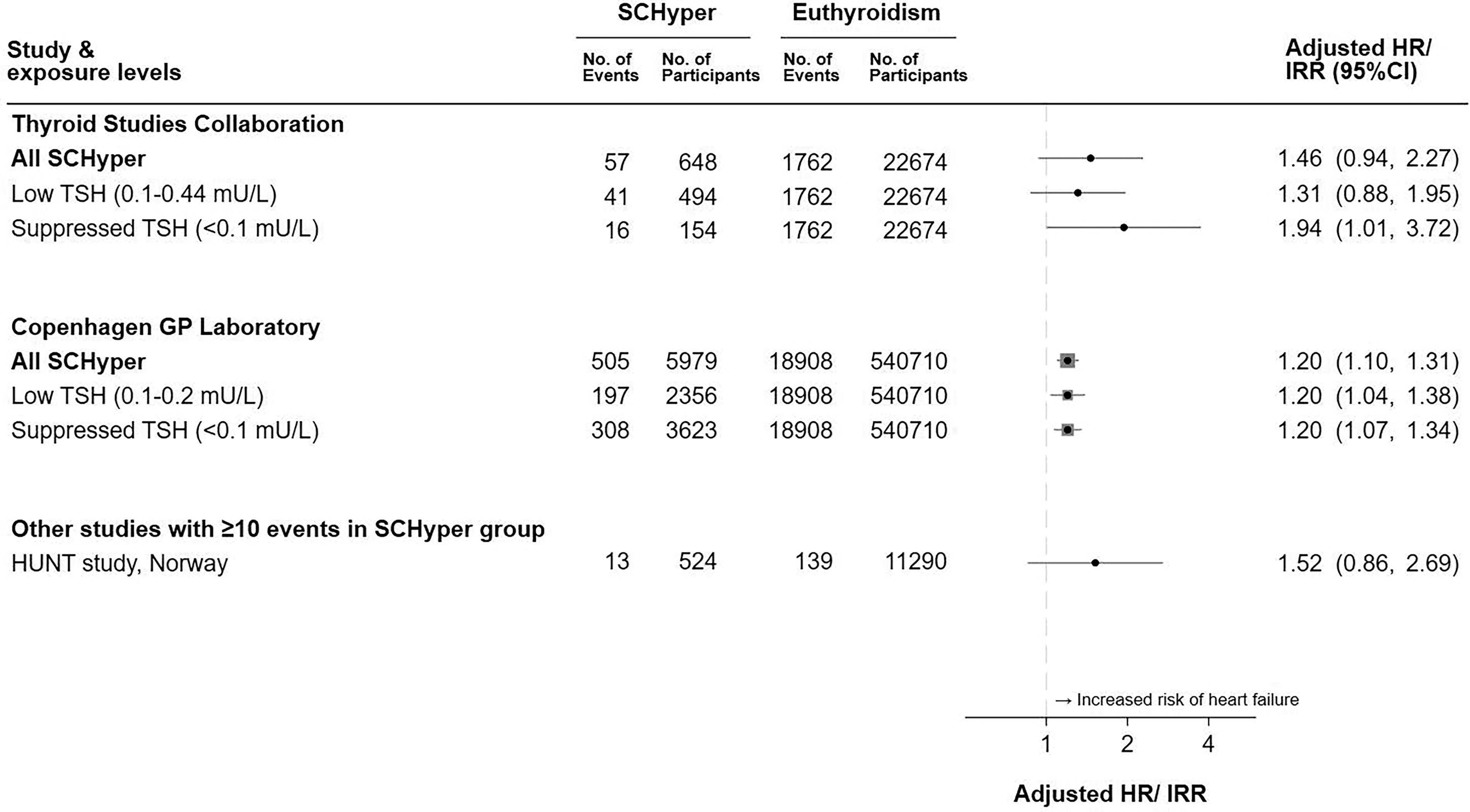
Forest plots for subclinical hyperthyroidism and risk of heart failure (figure based on references 31,33,47 ). SCHyper, subclinical hyperthyroidism; HR, hazard ratio; IRR, incidence rate ratio; CI, confidence intervals; TSH, thyroid-stimulating hormone; Copenhagen GP Laboratory, Copenhagen General Practitioners Laboratory; HUNT, Nord-Trøndelag Health Study. Adjusted ratio and their 95% confidence intervals are depicted using squares and solid lines. The size of each square corresponds to the number of heart failure events in individuals with subclinical hyperthyroidism.
Stroke
The TSC found no evidence supporting an increased risk for SCHyper being associated with stroke from nine studies 37 –41,45,48 –50 ; no other details were reported. 30 A subsequent study-level meta-analysis, based on four cohorts, 37,48,51,52 also revealed no significant association between SCHyper and stroke when compared with euthyroidism (HR 1.17; 95% CI, 0.54–2.56), although there was considerable heterogeneity among the studies included this meta-analysis (I2 of 67%). 53
Similarly, the analysis of the Copenhagen GP Laboratory study did not find any link between SCHyper and the risk of stroke (IRR 1.02; 95% CI, 0.93–1.12). 33
The only other cohort with 10 or more events in the SCHyper group to report on the outcome of stroke was the Atherosclerosis Risk in Communities study from the United States (approximately 40 events), which estimated the HR for stroke in the SCHyper group to be 1.23 (95% CI, 0.87–1.74), compared with those who were euthyroid. 54
Based on the research results reported to date, SCHyper appears to have little association with stroke risk.
Coronary heart disease and major adverse cardiac events
In TSC analysis, CHD event data were available for 22,445 people (21,714 euthyroid and 723 with SCHyper) from six cohorts. 37,38,40,41,45,49 The age- and sex-adjusted HR for CHD event in individuals with SCHyper (TSH <0.45 mIU/L) was 1.21 (95% CI, 0.99–1.46) compared with euthyroid individuals. 30
The Copenhagen GP Laboratory study demonstrated that the risk of MACE, which consists of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke, was higher (IRR 1.09; 95% CI, 1.02–1.16) in SCHyper individuals (TSH <0.2 mIU/L) compared with euthyroid population. 33 However, no increased risk of CHD, defined as myocardial infarction (IRR 1.02; 95% CI, 0.89–1.18), was found in the SCHyper group. 33 In TEARS, SCHyper (TSH <0.4 mIU/L) was associated with an increased risk of nonfatal cardiovascular morbidity (HR 1.39; 95% CI, 1.22–1.58) compared with euthyroidism, 15 although it must be noted that the definition of nonfatal cardiovascular morbidity used in TEARS likely encompassed a broader spectrum of pathology than CHD.
In summary, the most recent large, well-designed study demonstrated conflicting results for CHD but indicated an increased risk of MACE in individuals with SCHyper compared with euthyroid individuals. Figure 3 illustrates a compilation of all studies mentioned above 15,30,33 and others that included 10 or more outcomes related to CHD and MACE within the SCHyper. 43,47,54,55
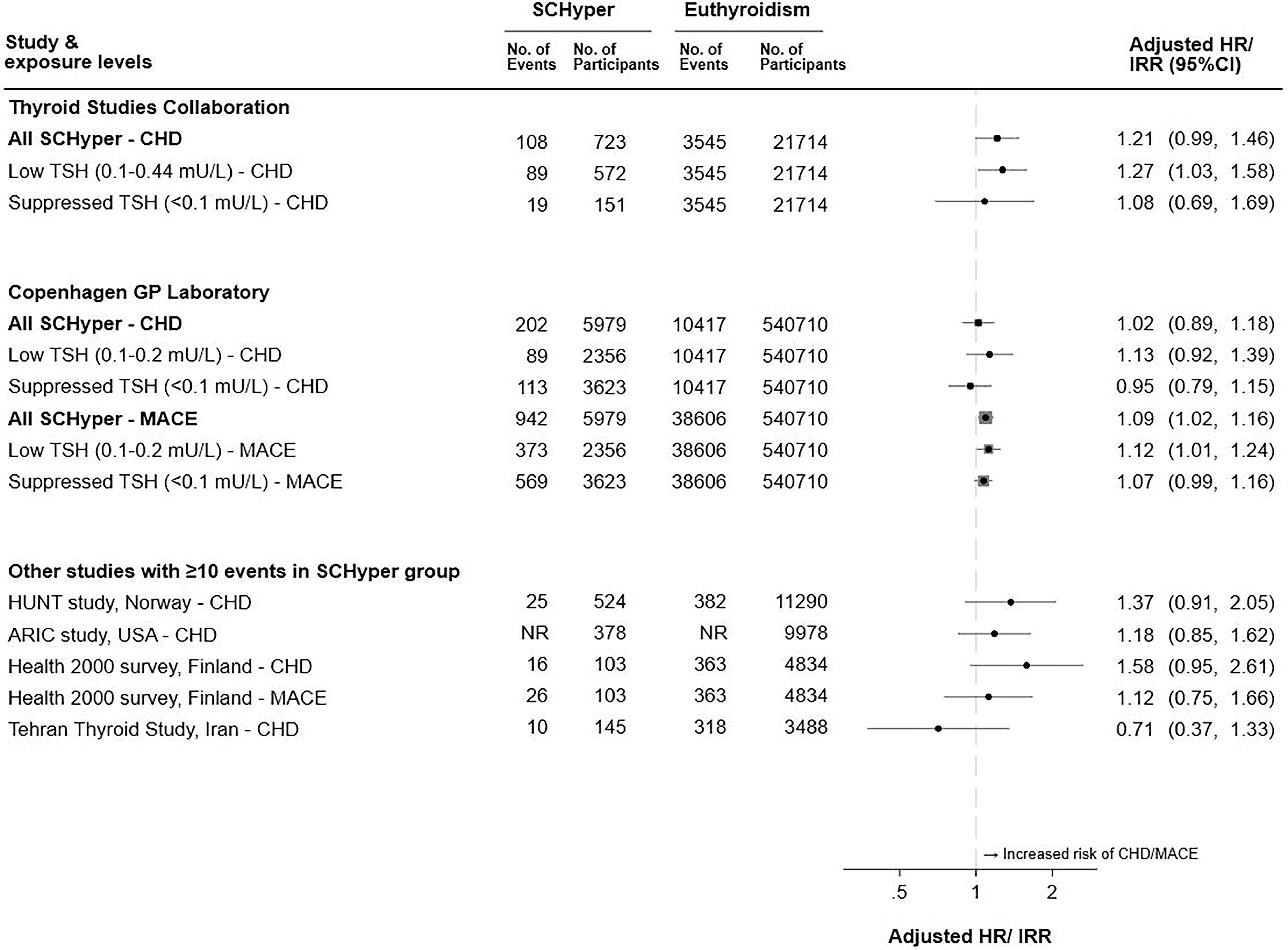
Forest plots for subclinical hyperthyroidism and risk of coronary heart disease and major adverse cardiac events (figure based on references 30,33,43,47,54,55 ). SCHyper, subclinical hyperthyroidism; HR, hazard ratio; IRR, incidence rate ratio; CI, confidence intervals; CHD, coronary heart disease; TSH, thyroid-stimulating hormone; Copenhagen GP Laboratory, Copenhagen General Practitioners Laboratory; MACE, major adverse cardiac events; HUNT study, Nord-Trøndelag Health Study; ARIC study, Atherosclerosis Risk in Communities study; NR, not reported. Adjusted ratio and their 95% confidence intervals are depicted using squares and solid lines. The size of each square corresponds to the number of coronary heart disease and major adverse cardiac events in individuals with subclinical hyperthyroidism.
Cardiovascular disease mortality and all-cause mortality
The TSC analysis of CVD mortality and all-cause mortality assessed 52,674 people (50,456 euthyroid and 2,177 with SCHyper for CVD mortality, and 50,486 euthyroid and 2,188 with SCHyper for all-cause mortality) involving 10 cohorts 37 –41,45,48 –50,56 with a median follow-up of 8.8 years. SCHyper (TSH <0.45 mIU/L) was associated increased CVD mortality (HR 1.29; 95% CI, 1.02–1.62) and all-cause mortality (HR 1.24; 95% CI, 1.06–1.46). 30
In the analysis of the Copenhagen GP Laboratory study, SCHyper individuals (TSH <0.2 mIU/L) was associated with an increased risk of all-cause mortality (IRR 1.23; 95% CI, 1.16–1.30) compared with euthyroid population. 33 In another large Danish population study from the OPENTHYRO Register cohort (222,138 euthyroid and 2,408 with SCHyper), SCHyper (TSH <0.3 mIU/L) was associated with increased all-cause mortality (HR 1.09; 95% CI, 1.02–1.17). 34 A retrospective cohort study, conducted on 17,440 individuals aged over 65 years (14,946 euthyroid and 538 with SCHyper) from the CHMO database in Israel, revealed that the all-cause mortality rate in those with SCHyper (TSH <0.35 mIU/L) was higher than in those with euthyroidism in multivariate analysis (HR 1.93; 95% CI, 1.71–2.17). 35
In summary, high-quality data provided evidence of an increased risk of CVD mortality and all-cause mortality in patients with SCHyper. Figure 4 summarizes of all studies mentioned above 30,33 –35 and others that included 10 or more outcomes related to CVD mortality and all-cause mortality within the SCHyper group. 43,47,57 –59

Forest plots for subclinical hyperthyroidism and (A) cardiovascular disease mortality and (B) all-cause mortality [figure (A) based on references 30,47 and figure (B) based on references 30,33,34,35,43,57,58,59 ]. CVD, cardiovascular disease; SCHyper, subclinical hyperthyroidism; HR, hazard ratio; IRR, incidence rate ratio; CI, confidence intervals; TSH, thyroid-stimulating hormone; HUNT study, Nord-Trøndelag Health Study; Copenhagen GP Laboratory, Copenhagen General Practitioners Laboratory; CHMO database, Clalit Health Medical Organization database; InCHIANTI study, Invecchiare in Chianti study; LASA, Longitudinal Aging Study Amsterdam. Adjusted ratio and their 95% confidence intervals are depicted using squares and solid lines. The size of each square corresponds to the number of cardiovascular disease mortality and all-cause mortality in individuals with subclinical hyperthyroidism.
Which patients with subclinical hyperthyroidism are at highest risk for cardiovascular disease?
The most compelling evidence regarding a specific risk factor influencing CVD lies in the degree of serum TSH suppression. As mentioned in the atrial fibrillation section, data from the TSC analysis, 30 the Copenhagen GP Laboratory, 32 and TEARS15 clearly demonstrate differences in AF risk according to the degree of TSH suppression.
To date, no studies have reported an increase in the relative risk of CVD in SCHyper by age with statistical power. However, even if there are no differences in relative risk by age, the absolute risk differences for CVD in SCHyper may vary significantly, as older people are inherently at a higher risk for CVD. 60
Which patients with subclinical hyperthyroidism should be considered for treatment?
There has been no large, randomized, placebo-controlled trial concerning the effects of treatment in patients with SCHyper on CVD risk. Based on the degree of TSH suppression and age, which are important risk factors for CVD as well as osteopenia and fracture risk, guidelines and other authorities have incorporated these as key elements of treatment algorithms. Recent guidelines advocate treating SCHyper in individuals older than 65 years with suppressed TSH to avoid serious potential complications. 7,9 Observation is recommended in young asymptomatic SCHyper patients with low TSH because of their low cardiovascular and skeletal risks and the infrequent progression of SCHyper to overt hyperthyroidism. 7,9 For SCHyper individuals older than 65 years with low TSH or those younger than 65 years with suppressed TSH, treatment decisions should be individualized based on the risk factors identified in SCHyper (e.g., individuals with CVD or osteoporosis; postmenopausal women who are not on estrogens or bisphosphonates and where SCHyper with persistent suppression of serum TSH) and/or the risk factors derived from patients, systems, or treatment (e.g., patients with hyperthyroid symptoms, assessment of treatment accessibility, ease of cure, and risks of treatment or loss to follow-up) (Figure 5). 1,7,9 Observational studies provide valuable insights; however, when interpreting treatment recommendations, it is important to consider the limitations of these data and the potential pitfalls of applying these findings to clinical practice without robust randomized controlled trial evidence.

Management of subclinical hyperthyroidism [adapted and modified from Biondi et al. 1 with permission to reproduce]. CVD, cardiovascular disease; TSH, thyroid-stimulating hormone. The blurring of boundaries between the quadrants is intended to illustrate that the cutoffs of age and thyrotropin level for therapy are not precisely defined.
Limitations of existing studies
Even large studies struggle with subgroup analyses due to insufficient participants experiencing CVD events. 30,31 Although some cohort studies report a relatively large number of events, 32,33 their observational nature precludes establishing causality. Conflicting findings on the association between SCHyper and CVD risk likely stem from differences in study populations, follow-up durations, TSH cutoff values, single TSH measurements, outcome definitions, and confounder adjustments (Table 1).
Characteristics of studies included in review
Participants were selected from five prospective cohorts37-41 for atrial fibrillation, nine37-41,45,48-50 for stroke, six37,38,40,41,45,49 for coronary heart disease, and 1037-41,45,48-50,56 for cardiovascular disease mortality and all-cause mortality.
A total of 11,084 participants for atrial fibrillation, 28,383 for stroke, 22,445 for coronary heart disease, and 52,674 for cardiovascular disease mortality and all-cause mortality.
Data from 10 prospective cohorts.37-41,45,48-50,56
The number of women (%) were 5,703 (51.5%) for atrial fibrillation, 14,322 (50.5%) for stroke, 11,335 (50.5%) for coronary heart disease, and 30,828 (58.5%) for cardiovascular disease mortality and all-cause mortality.
Participants from six prospective cohorts.37,40,41,44-46
Participants from four prospective cohorts.37,48,51,52
All subclinical hyperthyroid cases are matched with five controls based on age and sex.
Repeated TSH measurements; a minimum interval of 4 months between measurements.
Participants aged 18 years or older.
Participants aged 40 years or older.
Participants aged 65 years or older.
TSH, thyroid-stimulating hormone; NA, not applicable or not available; AF, atrial fibrillation; CHD, coronary heart disease; CVD, cardiovascular disease; Copenhagen GP Laboratory, Copenhagen General Practitioners Laboratory; MACE, major adverse cardiac events; TEARS, Thyroid Epidemiology, Audit, and Research Study; CHMO database, Clalit Health Medical Organization database; HDL, high-density lipoprotein; HUNT study, Nord-Trøndelag Health Study; ARIC study, Atherosclerosis Risk in Communities study; InCHIANTI study, Invecchiare in Chianti study; LASA, Longitudinal Aging Study Amsterdam.
Summary and conclusions
SCHyper has been linked to an increased risk of CVD and related outcomes, leading to an elevated risk of AF, heart failure, MACE, CVD mortality, and all-cause mortality, particularly in those with suppressed TSH. Treatment of SCHyper is recommended for individuals older than 65 years with suppressed TSH based on expert opinion. For now, treatment decisions for SCHyper individuals older than 65 years with low TSH or those younger than 65 years with suppressed TSH should be individualized based on their risk factors, future prospective research may clarify these decisions although will require large samples of SCHyper patients, involving a long follow-up, carefully selected patients based on rigorous criteria, and confirmatory thyroid function tests repeated during follow-up.
Footnotes
Acknowledgment
The authors thank Sangkeun Hyon, MA, Dong Won Shin, BA, and Saeam Kim, BA for their excellent work in literature search.
Authors’ Contributions
D.S.A.M. and H.J.K. analyzed and interpreted the study concept and design, and prepared, wrote, and edited the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding to declare.
Supplementary Material
Supplementary Appendix SA1