
Abstract
Background:
Calcitonin (CT), a well-established tumor marker for medullary thyroid carcinoma (MTC), is limited by a high rate of false positives in the diagnostic phase. Potential new markers for MTC are procalcitonin (PCT) and progastrin-releasing peptide (proGRP). Where literature has proven noninferiority for PCT, evidence is lacking for proGRP. Therefore, the present study prospectively evaluated the clinical performance of proGRP and PCT in a multicohort study of patients with MTC compared with other thyroid diseases.
Methods:
Adult patients undergoing thyroid surgery for thyroid nodular disease diagnosed in a tertiary center from the Netherlands (discovery cohort) between 2013 and 2025 were prospectively included. Serum samples were collected preoperatively. Diagnostic performance of CT, PCT, proGRP, and carcinoembryonic antigen was calculated separately. A two-step approach, combining different markers, was investigated. Analyses were repeated in a validation cohort from Switzerland.
Results:
The discovery and validation cohorts consisted of 335 and 61 patients, respectively. Patients had benign disease (n = 166), other thyroid carcinomas (non-MTC, n = 186), or MTC (n = 44). Median proGRP and PCT levels were significantly higher in MTC compared with benign disease and non-MTC. ProGRP had a low sensitivity (69.2% [CI 48.2–85.7]), while PCT performed similarly to CT (100.0% [CI 89.1–100.0] and 100.0% [CI 88.8–100.0], respectively). The combination of CT and PCT, both in the individual cohorts and when combining the two cohorts, showed the best diagnostic performance with a sensitivity of 100% [CI 91.8–100.0] and negative predictive value of 100% [CI 98.9–100.0] and specificity and positive predictive value of 99.7% [CI 98.4–100.0] and 97.7% [CI 88.0–99.9], respectively.
Conclusions:
ProGRP alone or with CT does not have additional value as a diagnostic marker for MTC. A two-step approach combining the use of CT and PCT measurement, in the CT concentration range between 10 and 100 pg/mL, is a promising method to diagnose MTC in patients with thyroid nodules with high diagnostic accuracy.
Introduction
Medullary thyroid carcinoma (MTC) is a neuroendocrine tumor derived from the parafollicular C-cells, accounting for 1–3% of all thyroid carcinomas. 1,2 A substantial part of patients present with metastatic disease: 35% with cervical lymph node metastasis and 5–10% with distant metastasis. 3 Survival in MTC patients is strongly correlated with the stage of disease at time of diagnosis. The 10-year survival rate ranges from up to 100% in stage I to 20% in stage IV and emphasizes the need for early diagnosis. 4
Most patients with MTC present with a thyroid nodule. 5 The standard workup for patients presenting with thyroid nodules is an ultrasound and fine needle aspiration (FNA). Unfortunately, in almost half of the cases, neck ultrasound is unsuccessful in correctly identifying MTC as a suspicious or malignant nodule. 6 Furthermore, the sensitivity of FNA in patients with MTC nodules is low, ranging between 56% and 69% in different studies, and can fail to raise preoperative suspicion of MTC, potentially causing a delay in delivering the right treatment to the patient. 7,8
Calcitonin (CT) and carcinoembryonic antigen (CEA) are valuable tumor markers for MTC but have their limitations in the diagnostic phase. A serum CT concentration >100 pg/mL has a 100% positive predictive value (PPV) for MTC. However, due to nonspecific increases in CT levels, the PPV of CT within the 10–100 pg/mL concentration range is only 25%. 9 Nonspecific increases in CT levels can be seen both in physiological and pathological conditions other than MTC, such as age, male sex, smoking, certain drugs, other neuroendocrine tumors, pancreatic or breast cancer, small cell carcinoma of the lung, systemic mastocytosis, hyperparathyroidism, and chronic renal failure. 10 –13 The effect of (autoimmune) thyroiditis and differentiated thyroid cancer on basal serum CT levels remains a subject of debate, with previous studies reporting elevated CT levels in these conditions. 14 However, more recent studies with larger cohorts show that these conditions do not have a relevant effect on serum CT levels. 15 –17 Thus, given the considerable risk of false positive findings, the utility of CT in the low concentration range is limited, particularly based on the high prevalence of thyroid nodules and the rarity of MTC. Therefore, guidelines do not recommend for nor against measuring serum CT levels in patients with nodular goiters. CEA serves well as a marker for disease progression during follow-up, but its use in early diagnosis is of no added value since it is not a specific marker for MTC. 18
Additionally, CT measurement is troubled by a series of preanalytic and analytic drawbacks affecting its clinical reliability. First, CT is unstable at room temperature, being rapidly degraded by serum proteases. 19 It therefore needs to be kept on ice immediately after collection. Second, due to the availability of multiple commercial kits and assays on the market, there is poor intermethod and interlaboratory comparability. 20 Thus, better markers are needed for rapid and reliable diagnosis of MTC in patients with thyroid nodules.
Potential new markers for MTC are procalcitonin (PCT) and progastrin-releasing peptide (proGRP). 21 PCT is the prohormone of CT and is secreted by the C-cells of the thyroid. It is currently mainly used in the diagnosis and prognosis of sepsis. However, in the absence of an infection, PCT is almost exclusively produced by C-cells. 22 PCT is very stable in blood at room temperature, and the available assays are highly comparable, since there is only one company that holds the intellectual property for commercial PCT assays. 19,23,24 A number of studies have shown that PCT is a reliable alternative tumor marker and that it is noninferior to CT. 19,25 –29
ProGRP is the biologically inactive precursor of gastrin-releasing peptide, a neuropeptide widely expressed in the central nervous system and the gastrointestinal tract, and is highly expressed in MTC. 30,31 The potential of proGRP as a tumor marker for MTC has been explored in studies with limited sample size or retrospective design. 30 –33 Furthermore, there is a large variability in the reported sensitivity, specificity, and cutoff value of proGRP. So, based on the current literature, it is not possible to draw definite conclusions on the potential value of proGRP as a tumor marker in MTC diagnosis.
Therefore, in the present study, we prospectively evaluated the clinical performance of proGRP and PCT as diagnostic markers in a cohort of patients with MTC compared with other thyroid diseases. The first aim was to evaluate the individual performance of these markers in comparison to CT. The second aim was to explore a two-step approach using a combination of tumor markers. To validate the findings, we subsequently aimed to replicate the findings in an independent cohort with available data.
Materials and Methods
Study population
For the current study, we used two independent patient cohorts from the Netherlands and from Switzerland. The cohort from the Netherlands will be referred to as the “discovery cohort,” and the cohort from Switzerland will be referred to as the “validation cohort.”
From the Erasmus Medical Center, Rotterdam, the Netherlands, we prospectively included adults undergoing thyroid surgery for thyroid nodular disease, diagnosed with either benign or malignant thyroid disease, between 2013 and 2025. Serum samples were collected preoperatively in all patients. As an additional control, we included eight postoperative samples from MTC patients who underwent surgery and had no evidence of disease at the time of blood withdrawal. Supplementary Figure S1 shows the full selection process of the cohort and reasons for exclusion. The study was approved by the Medical Ethics Committee of the Erasmus Medical Center (MEC 2012-561).
From the Ente Ospedaliero Cantonale, Bellinzona, Switzerland, a cohort of patients was collected between 2006 and 2025. Blood samples were collected before surgery, and diagnosis was confirmed with pathology after thyroidectomy. Fourteen patients presented with benign unsuspicious nodules on ultrasound and did not undergo thyroidectomy. A blood sample was collected at diagnosis. Patients were followed by ultrasound evaluation and were only included if the nodule was unchanged on ultrasound after 1 year. They were followed for a median of 5.3 (4.0–5.8) years in which all nodules remained stable. The study was approved by the Canton Tessin Ethical Committee, Bellinzona (Switzerland) (references CE 3466 and BASEC 2019-00662). Informed consent was obtained from all participants from both centers involved in the present study. The study was performed in accordance with the World Medical Association Declaration of Helsinki regarding ethical conduct of research involving human participants.
All patients were categorized as follows: Benign disease, including benign thyroid nodules, thyroiditis, Graves’ disease, Hashimoto’s disease, and goiter. Nonmedullary thyroid cancer (non-MTC), including papillary thyroid cancer, follicular thyroid cancer, anaplastic thyroid cancer, and poorly differentiated thyroid cancer. MTC with evidence of disease (MTC-ED). MTC with no evidence of disease (MTC-NED). This category was added as an extra control group in Figure 1 and Table 2. NED was determined at the first postoperative control visit. NED was defined as having an undetectable CT, CEA in normal range, and no structural disease on imaging.
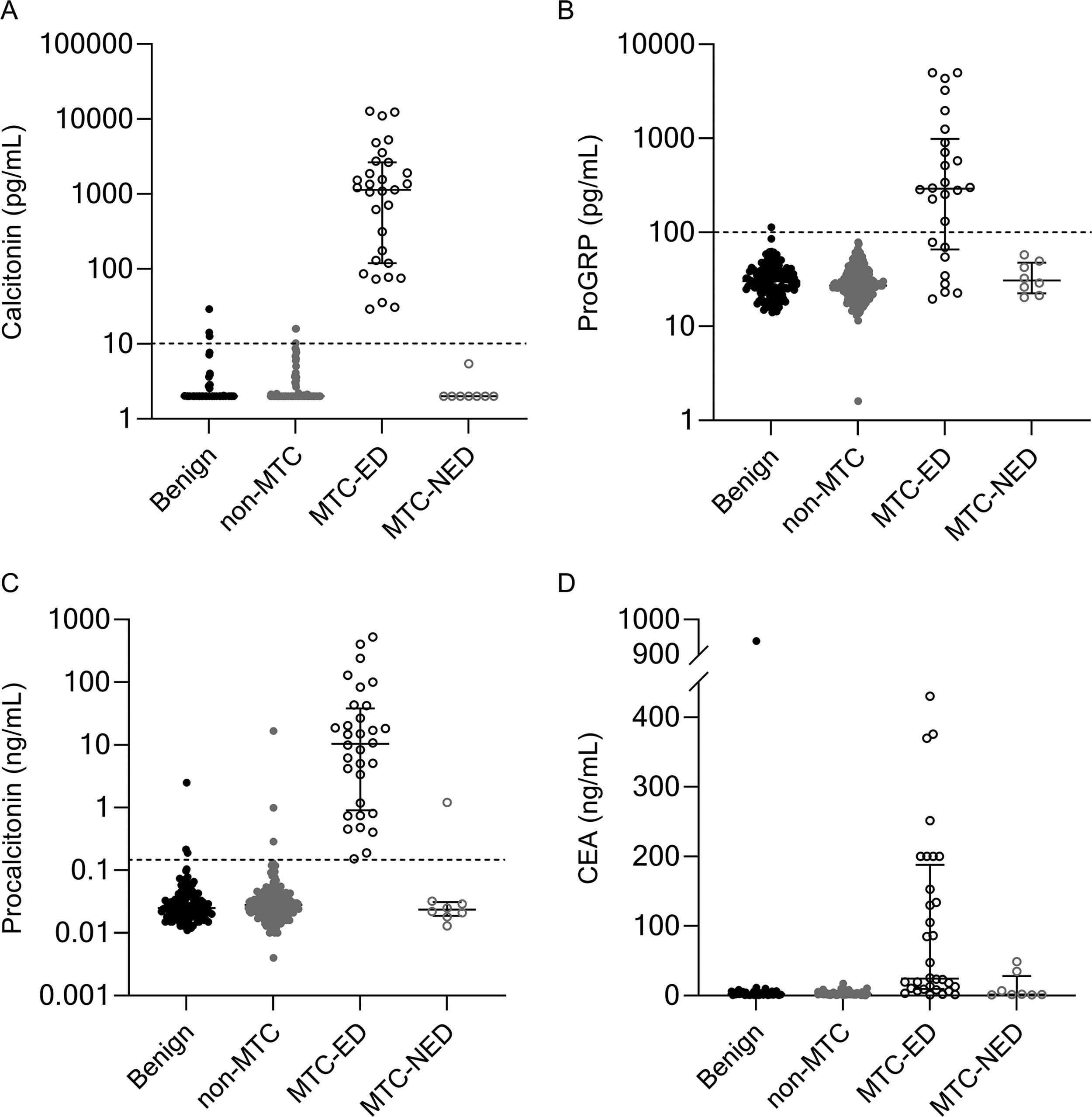
Scatterplot of tumor marker serum concentrations in all patients of the discovery cohort: (
Clinical characteristics were retrospectively obtained from patient records. The following variables were collected: age, sex, American Joint Committee on Cancer (AJCC)/TNM stage, tumor size, and heritability for MTC patients. Age was chosen as age at the time of thyroidectomy. All patients in the discovery cohort had germline RET testing for multiple endocrine neoplasia, type 2 (MEN2). In the validation cohort, all patients received genetic counseling. All patients were classified according to the AJCC and TNM staging eighth edition. 34
The pathologist and treating physician were blinded to tumor marker serum levels. The lab technician was blinded to the final histopathological diagnosis. The researcher conducting the analyses was not blinded to the final histopathological diagnosis.
Measurement of tumor marker serum concentrations
Serum samples were stored at −80°C immediately after blood was drawn, until testing for the tumor markers was performed for the present study. In the discovery cohort, serum levels of proGRP, PCT, and CEA were measured using Lumipulse G1200 (Fujirebio, Ghent, Belgium), except for six samples where PCT was measured with Atellica (Siemens, The Hague, Netherlands) and CEA with Cobas (Roche Diagnostics, Penzberg, Germany). CT was measured using IMMULITE 2000 XPi (Siemens). Additional dilutions were performed to get the true concentration in all samples with analyte concentrations above the upper limits of measurement. For CT, there were eight missing values, one in the MTC-ED group, three in the benign disease group, and four in the non-MTC group.
In the validation cohort, serum levels of PCT were measured using the Kryptor® system (Brahms Thermo Fischer, Hennigsdorf, Germany). CT was measured on the Immulite® 2000 XPi platform (Siemens Healthcare Diagnostics, Erlangen, Germany). An overview of assay characteristics and reference intervals is provided for all tumor markers in both cohorts in Supplementary Table S1. Previous literature has shown a good correlation (r = 0.99) between Kryptor and Lumipulse for measuring PCT. 35
Cutoff levels for CT (10 pg/mL), PCT (0.15 ng/mL), and CEA (5 ng/mL) were based on literature and current clinical practice. 9,32,36 Cutoff level for proGRP (100 pg/mL) was based on previous studies and validated in a local cohort of apparently healthy individuals (n = 470). 37
Statistical analysis
For the purpose of statistical analysis, CT values below the lower limit of detection were replaced with 2 pg/mL. For continuous variables, means and standard deviations or medians with range were calculated. Categorical variables were reported as absolute numbers with percentages. To analyze differences between the groups (MTC-ED, MTC-NED, non-MTC, and benign disease), one-way analysis of variance, χ2-test, Mann–Whitney U test, or Kruskal–Wallis test were used, depending on the type of variable. Sensitivity, specificity, PPV, and negative predictive value (NPV) with their corresponding confidence intervals (CIs) were calculated. When combining different tumor markers, the test result was interpreted as positive when all tumor markers were above their cutoff.
Statistical analysis was performed using R statistical software (version 4.3.2) and GraphPad Prism version 9.0.0 (GraphPad Software, San Diego, CA). A p-value <0.05 was considered statistically significant.
Results
Demographic characteristics of discovery and validation cohort
Blood samples of 343 patients were obtained in the discovery cohort. MTC was diagnosed in 40 patients (32 and 8 with MTC-ED and MTC-NED, respectively), non-MTC in 180 patients, and the remaining 123 patients had benign thyroid disease. Table 1 shows the demographic characteristics of the study populations of both the discovery and validation cohorts. In the discovery cohort, the mean age was 51.5 years, and 66% of the patients were females. The percentage of females was higher in the non-MTC and benign disease groups than in the MTC group. There were more patients with stage 4 disease in the MTC group than in the non-MTC group. In the MTC group, 81% of patients had sporadic disease versus 19% with MEN2A syndrome.
Demographic Characteristics of the Study Population
Values are means (±standard deviation), medians (IQR), or numbers (percentages).
Stage according to AJCC and TNM staging eighth edition. 34
AJCC, American Joint Committee on Cancer; MTC, medullary thyroid carcinoma; non-MTC, nonmedullary thyroid carcinoma.
The validation cohort consisted of 61 patients, of whom 12 were diagnosed with MTC, 6 with non-MTC, and 43 with benign thyroid disease. MTC patients in the validation cohort had a younger age at diagnosis, smaller tumor size, and more often AJCC stage I disease at diagnosis in comparison with the discovery cohort.
Diagnostic performance of individual markers
Figure 1 shows the concentration of the different tumor markers in all patient groups of the discovery cohort. There was a significant difference between all groups for the median CT, proGRP, PCT, and CEA concentration. Median concentration of CT, proGRP, PCT, and CEA was the highest in the MTC-ED group (see Table 2). For all tumor markers, the median concentrations in the benign, non-MTC, and MTC-NED groups were below their cutoff level. For CEA, the only outlier in the benign group with a CEA concentration of 938.4 ng/mL was also diagnosed with a metastatic adenocarcinoma of unknown primary origin. In the validation cohort, PCT and CT concentrations were also the highest in the MTC-ED group (see Supplementary Table S2).
Median Concentration of Tumor Markers in All Patient Groups (Discovery Cohort)
Values are medians (range).
p-Value comparing all groups.
CT, calcitonin; CEA, carcinoembryonic antigen; ED, evidence of disease; NED, no evidence of disease; PCT, procalcitonin; proGRP, progastrin-releasing peptide.
In the discovery cohort, CT and PCT had similar high sensitivity (100% [CI 88.8–100.0] and 100% [CI 89.1–100.0], respectively), specificity (98.0% [CI 95.6–99.3] and 98.0% [CI 95.7–99.3]), and NPV (100% [CI 98.7–100.0] and 100% [CI 98.8–100.0], respectively). ProGRP had a low sensitivity (69.2% [CI 48.2–85.7]), but high specificity (99.7% [CI 98.2–100.0]). Data on the diagnostic performance of CT, PCT, proGRP, and CEA in the discovery cohort are summarized in Table 3. A sensitivity analysis excluding the six samples where PCT and CEA were measured with different assays (Atellica and Cobas, respectively) did not alter any results.
Diagnostic Performance of All Tumor Markers for MTC in All Patients
For all combinations, positivity was defined as all individual markers being above their respective cutoff. Any other combination was classified as negative.
Comb, combined; CI, confidence interval; Disc, discovery; NPV, negative predictive value; PPV, positive predictive value; Val, validation.
Two-step approach
We then explored the option of a two-step approach that might be used in the diagnostic workup of MTC. All patients with a serum CT >100 pg/mL had MTC, and no MTC was found when CT was <10 pg/mL. In the two-step approach, first, CT would be measured, and in case of a result in the concentration range between 10 and 100 pg/mL, proGRP or PCT would be measured as well. All patients were divided into two groups: the MTC-ED group versus the no MTC group (comprising the benign disease and non-MTC groups, see Fig. 2). There were seven and six patients in the MTC-ED group and the no MTC group, respectively, with a CT between 10 and 100 pg/mL. With proGRP as a second step, five (83%) patients in the MTC-ED group would have been wrongfully diagnosed as having no MTC, since the proGRP result was below the cutoff for MTC. For PCT, all samples (n = 7, 100%) would have been diagnosed correctly as MTC. In the no MTC group, both proGRP and PCT (n = 6, 100% and n = 6, 100%) would have correctly diagnosed the patients as having no MTC in a two-step approach. Combining CT and PCT resulted in perfect (100%) sensitivity, specificity, PPV, and NPV. Conversely, the combination of proGRP and CT resulted in poorer diagnostic performances than CT or proGRP alone (see Table 3).
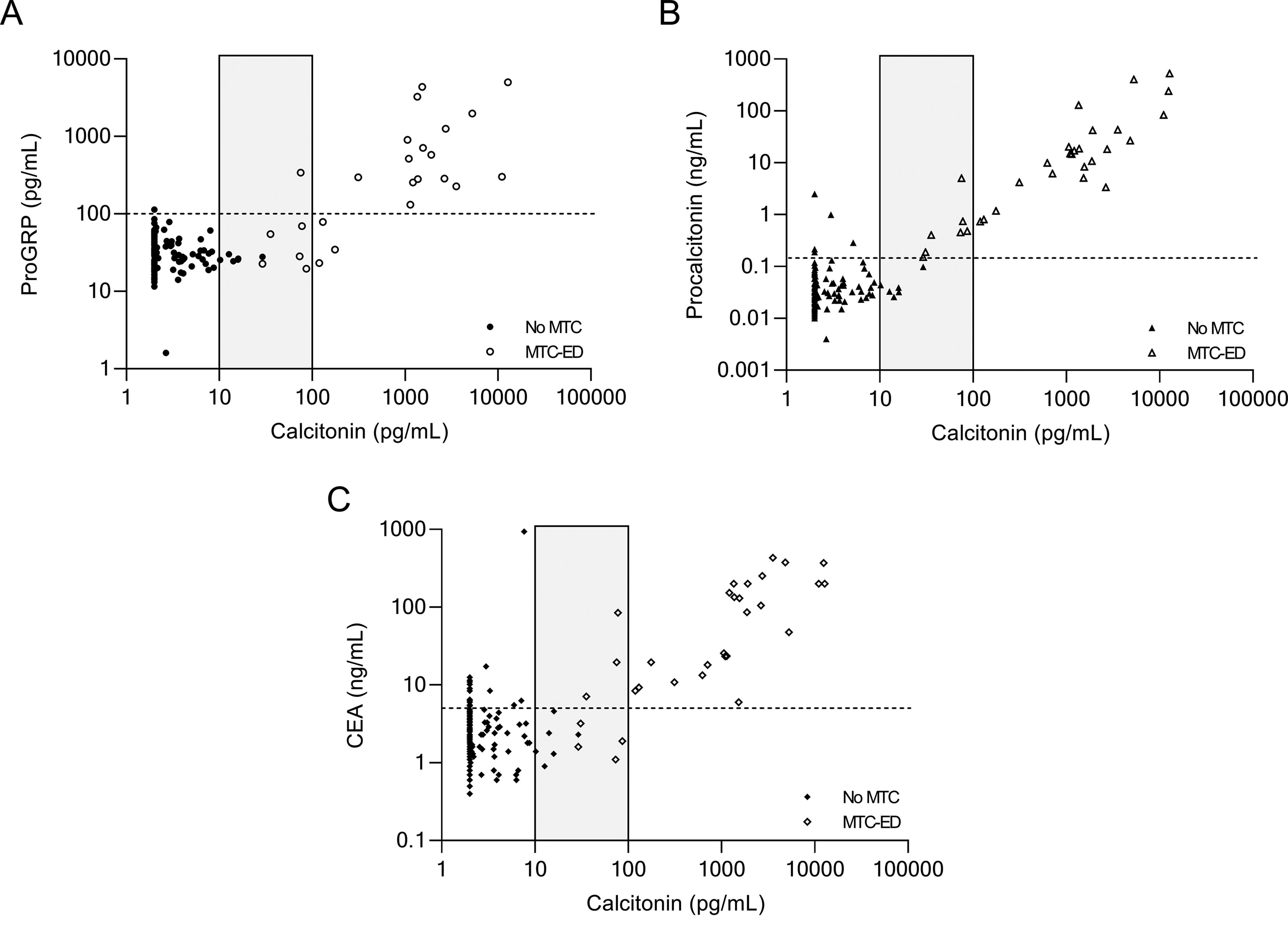
Correlation between serum CT and proGRP (
Results from validation cohort
Given these findings, we then aimed to validate these findings by studying if we could replicate the results of the two-step approach for CT and PCT in an independent cohort with available data (see Fig. 3). In the validation cohort, there were 22 patients with a CT between 10 and 100 pg/mL. Using the two-step approach with CT and PCT, all MTC-ED patients would have been correctly diagnosed as MTC. In the no MTC group, 18 out of 19 patients (95%) would have rightfully been identified as no MTC. An overview of all patients and their characteristics in the CT concentration range between 10 and 100 pg/mL can be found in Supplementary Table S3.
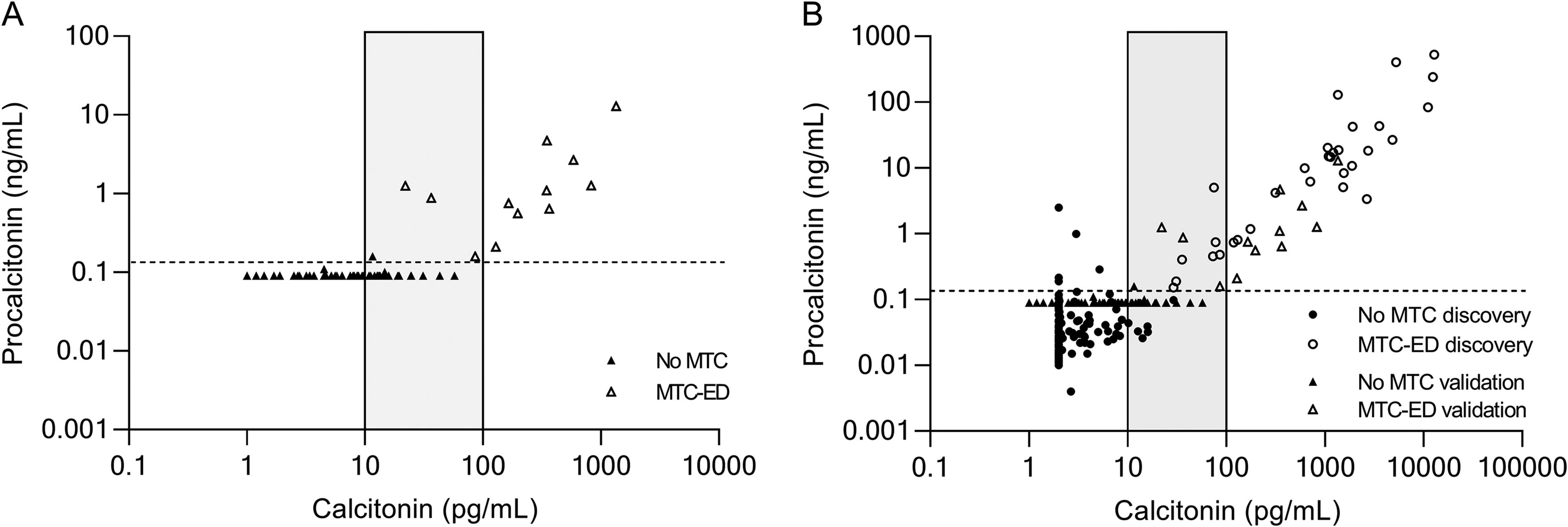
Correlation between serum CT and PCT (
In the validation cohort, PCT and the combination of CT + PCT demonstrated higher specificity (98.0 [CI 89.1–99.9] vs. 61.2 [CI 46.2–74.8]) and PPV (92.3 [CI 64.0–99.8] vs. 38.7 [CI 21.8–57.8]) than CT. Merging the discovery and validation cohorts, consistently, the combination of CT and PCT showed better diagnostic performance than CT and PCT alone with a sensitivity of 100.0% [CI 91.8–100.0] and NPV of 100.0% [CI 98.9–100.0] and specificity and PPV of 99.7% [CI 98.4–100.0] and 97.7% [CI 88.0–99.9], respectively (see Table 3).
Discussion
To our knowledge, the present study is the first to prospectively evaluate the diagnostic performance of PCT alone, but also in combination with CT, in cohorts from two different centers. We demonstrated the superiority of a two-step approach combining the use of CT and PCT measurement to diagnose MTC over CT or PCT measurement alone, in the CT concentration range between 10 and 100 pg/mL. Additionally, we showed that proGRP by itself and in combination with CT is not a better diagnostic marker for MTC than CT alone.
CT has been used in the diagnosis and management of MTC for many years. However, the debate on the use of CT as a screening marker for MTC is still ongoing, and decisive evidence is lacking. 38 Especially in the low concentration range, there is a high risk of false positive findings leading to possible overtreatment or unnecessary follow-up. Although the implementation of more sensitive CT assays has improved the accuracy of CT in diagnosing MTC, 39,40 a significant limitation remains the lack of universally shared cutoff values. Moreover, there is evidence that cutoff values for MTC should ideally be sex-specific. As a result, numerous different sex-specific cutoffs for basal CT have been proposed. 41,42 Therefore, each laboratory must redefine its own appropriate cutoffs based on the reference population.
Stimulated CT testing and CT measurement in FNA washout fluids are methods used to enhance the accuracy of basal CT measurement. However, both methods have their limitations. Stimulated CT testing was traditionally performed with pentagastrin, which is now unavailable in many countries. Although calcium-stimulated CT measurement has demonstrated high sensitivity, its specificity is suboptimal, and universally accepted, reliable cutoffs are still lacking. 40,41,43 Additionally, patients may experience potential unpleasant side effects. Similar to calcium-stimulated CT measurement, CT measurement in FNA washout fluids lacks a standardized threshold for clinical practice and necessitates the development of institutional cutoffs. 44
These limitations in combination with multiple analytical drawbacks of CT prompt the search for better markers. Previous literature has already shown noninferiority of PCT compared with CT in terms of diagnostic performance for MTC. 19,25,27,45 –48 Moreover, PCT has many practical advantages over CT, and therefore, it is a very promising marker to replace CT measurement in routine clinical practice. A meta-analysis by Giovanella et al., including 11 studies with in total 5817 patients, demonstrated a high accuracy of PTC in the diagnosis of MTC with similar performance of serum CT and serum PCT. 25 However, one of the limitations of this meta-analysis and of the included studies is that the design is in such a way that an alternative marker can only be shown to be equal to the golden standard, CT. When slightly elevated CT serum levels are detected in a patient with a thyroid nodule, a full clinical workup for MTC will follow, even in the presence of undetectable, but unmeasured PTC levels. Vice versa, if serum CT concentration is within the reference range, no further analysis into MTC will be performed without considering PTC serum concentrations that potentially could be elevated. Consequently, the diagnostic performance of CT is biased to a sensitivity of 100%, and the best diagnostic performance PCT can show is equal to that of CT. Moreover, since there are many years of clinical experience with CT, clinicians will be hesitant to replace this marker in clinical practice. Therefore, it seems more feasible to first adopt PCT as an additional marker in the management of MTC. Our results, in agreement with those reported by Costante et al., showed that a CT concentration >100 pg/mL has an excellent ability to diagnose MTC. 9 The diagnostic challenge is in the CT range between 10 and 100 pg/mL, where multiple false positives are recorded. The addition of PCT measurement in these cases resulted in very high diagnostic performance with a sensitivity, specificity, PPV, and NPV of 100%, 99.7%, 97.7%, and 100%, respectively. Most importantly, the performance of the combination of PCT and CT yielded better performance than CT and PCT measurement alone.
Implementing the two-step approach of additional PCT measurement in cases where the CT serum concentration is between 10 and 100 pg/mL could potentially lead to lower health care costs. With the two-step approach, patients with thyroid nodules and slightly elevated CT levels but undetectable PCT will no longer require unnecessary follow-up visits and ultrasounds. Moreover, it could also prevent unnecessary total thyroidectomies in patients with benign thyroid nodules that are wrongfully diagnosed as MTC by CT measurement alone. The additional costs of an extra PCT assay vastly outweigh the costs of surgery, hospital admission, or extra imaging and follow-up visits.
With regard to proGRP, this study clearly demonstrates that proGRP is not a good marker for the diagnosis of MTC. Our results are in line with the article from Giovanella et al., showing low sensitivity and high specificity for discriminating between MTC and other thyroid diseases. 32 When using proGRP as a diagnostic marker, its low sensitivity will lead to many missed diagnoses of MTC. In contrast to our results, the article by Parra-Robert et al. showed very high sensitivity and lower specificity, respectively, 100% and 76.9%, when combining CT and proGRP. 33 This could possibly be explained by the difference in cutoff level for proGRP. In this study, a cutoff of 100 pg/mL was used, whereas Parra-Robert et al. used a very low cutoff of 50 pg/mL, which could explain the discrepancy in results. In our opinion, the cutoff used in the current study represents a more reliable cutoff as it was based on the upper limit of a large cohort of healthy individuals and checked with ROC curves for the current study. Furthermore, it is in line with the article by Korse et al., which shows a similar large cohort from Kiel with multiple healthy individuals with proGRP values >100 pg/mL. 37 Possibly, proGRP is better suited as a marker for late disease and could be of interest in the follow-up of MTC. 32
One of the main strengths of the current study is that we are able to demonstrate our results in two independent cohorts from different countries with different clinical practice. As a consequence of a diffuse ultrasound screening of thyroid nodules in Switzerland, the validation cohort had younger patients, smaller tumors, and more often stage I disease at diagnosis. Furthermore, in the validation cohort, 14 patients were included who did not undergo surgery and therefore did not have histopathological confirmation of the final diagnosis. However, they were followed for a median of 5.3 (4.0–5.8) years, and nodules remained unchanged in this period. In addition, repeated CT levels were <10 pg/mL, and PCT levels were consistently at 0.09 ng/mL, further minimizing the likelihood of undetected MTC. The distinctions between the two cohorts further strengthened the results, since they demonstrate that even despite these differences, the outcome remained unchanged. Furthermore, it reflects the true case mix of patients with thyroid nodules, which also improves the external generalizability.
A possible limitation of this study is the inclusion and sampling of patients. Unfortunately, 89 patients could not be included due to a missing preoperative blood sample. However, we believe the missingness is at random. The missing samples were distributed across all diagnostic groups without a systematic pattern. Reasons for missing samples included the following: blood not being drawn, incorrect sampling, loss of the sample during workup, or failure to retrieve the sample from storage. Since these reasons are unrelated to diagnosis or outcome, the missing data are unlikely to introduce bias or influence the results. Despite having a large overall sample size, the number of samples with a CT concentration between 10 and 100 pg/mL and the number of MTC cases were low. The study was conducted in two academic centers where the risk of having MTC a priori is higher than in the total population of patients with thyroid nodules, leading to an enrichment of MTC in the study population. The prevalence of MTC in the discovery and validation cohort (10% and 13%, respectively) is much higher than the prevalence of MTC in all patients with thyroid nodules (0.4–2.85%). 49 Furthermore, in the discovery cohort, only patients undergoing total thyroidectomy were included. This is both a strength, since all final diagnoses were confirmed with histology, but also a limitation, because nodules without indication for surgery are not included. Finally, the study population included MEN patients, where detection of premalignant C-cell hyperplasia is important. Investigating the potential of PCT for this aim was beyond the scope of the current study. Thus, the current study population might not be the best representative of the true population. However, since MTC is a rare disease, collecting a cohort reflecting the true population with still a large number of MTC patients is very challenging. Large international collaboration studies will be needed to address this matter.
With this study, we demonstrated the superiority of a two-step approach combining CT and PCT measurement in the diagnosis of MTC in patients with thyroid nodules with CT concentrations between 10 and 100 pg/mL. Furthermore, we robustly showed that proGRP can be disregarded as a marker in the diagnosis of MTC. Future studies should focus on confirming the two-step approach in large prospective cohorts of patients with thyroid nodules.
Footnotes
Authors’ Contributions
L.E.S., R.P.P., S.A.A.v.d.B., and W.E.V.: Designed the current study. M.v.B., L.E.S., and L.G.: Collected the clinical data. L.E.S.: Conducted the statistical analyses and wrote the article. All authors reviewed and revised the article to improve its intellectual and technical content.
Author Disclosure Statement
L.G. is a member of the Roche Diagnostics Advisory Board and has received research grants from Roche Diagnostics and speaker honoraria from Roche Diagnostics unrelated to the present work. L.E.S., S.A.A.v.d.B., M.v.B., W.E.V., R.P.P., and L.G. declare no conflicts of interest, and no competing financial interests exist.
Funding Information
Part of this work was supported by Fujirebio.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.