
Abstract
Background:
The coexistence of v-Raf murine sarcoma viral oncogene homolog B1 (BRAFV600E ) and telomere reverse transcriptase promoter (TERT-p) mutations is considerably associated with aggressiveness and poor prognosis in papillary thyroid carcinoma (PTC). However, the association between gross findings and genetic alterations in PTC remains unknown. We aimed to investigate the association between clinicopathologic features, including macroscopic features, and the coexistent BRAFV600E and TERT-p mutations in patients with PTC.
Methods:
We retrospectively analyzed 375 cases of PTC surgically resected between January 2018 and October 2023 at a single institution, based on the presence of BRAFV600E and TERT-p double mutation. Clinicopathologic features, including gross features on the cut surface of tumors, were evaluated. Subsequently, the association between clinicopathologic features and mutation status was statistically examined. Cox proportional hazard models were used to analyze the impact of molecular pathological features on disease-free survival (DFS).
Results:
The BRAFV600E and TERT-p double mutation was identified in 78 (20.8%) patients among the PTC cases and was significantly correlated with shorter DFS. Multivariable analysis revealed that factors such as relatively older age (≥55 years) (odds ratio [OR] = 12.083, 95% confidence interval [CI] 4.498–32.456), larger tumor size (>2.0 cm) (OR = 2.722, CI 1.104–6.712), lobulated tumor margins (OR = 16.114, CI 3.155–82.296), papillary excrescences on the cut surface (OR = 17.573, CI 3.462–89.201), solid-cut surface (OR = 4.012, CI 1.084–14.849), minimal extrathyroidal extension (ETE) (OR = 4.156, CI 1.209–14.282), gross ETE (OR = 6.517, CI 1.734–24.490), and Ki-67 labeling index (LI) (≥5%, OR = 12.145, CI 4.354–33.877) were significantly associated with the double mutation.
Conclusions:
The BRAFV600E and TERT-p double mutation in PTC was significantly associated with relatively old age, larger tumor size, lobulated configuration in tumor margin, papillary excrescences on the cut surface, solid-cut surface, ETE, and high Ki-67 LI. These features are suggestive of the presence of the double mutation and should be analyzed at the molecular level in patients with PTC.
Introduction
Papillary thyroid carcinoma (PTC) is the main histological subtype of thyroid malignancy, with an increasing global incidence. 1 –3 Although the majority of patients with PTC show a favorable long-term survival rate, 4,5 less than 5% of patients present adverse outcomes with recurrence, distant metastasis, and cancer-related death. 5 –7 Many studies have examined indicators, including clinicopathologic features and molecular alterations, to predict poor clinical outcomes in patients with PTC. 6 –11
Missense mutations in v-Raf murine sarcoma viral oncogene homolog B1 (BRAFV600E ) and telomere reverse transcriptase promoter (TERT-p) (C228T [chr5:1,295,228C > T] and C250T [chr5:1,295,250C > T]) are the most commonly investigated genetic alterations in thyroid carcinomas. 8 –21 Although the prognostic value of the BRAFV600E mutation remains controversial, 8 –14 several studies have consistently indicated that the TERT-p mutation represents a potential prognostic marker and often coexists with BRAFV600E mutations in PTC. 14 –24 The combination of BRAFV600E and TERT-p mutations is significantly associated with tumor aggressiveness, radioactive iodine-refractory cancer, and a worse prognosis of PTC in patients, whereas either of the mutations alone has a relatively mild impact. 22 –30
In the pathology practice, gross examination of resected tissues is necessary to choose relevant sections for microscopic examination leading to accurate diagnosis. 31 The histopathological features analyzed depend on appropriate and complete sampling by gross evaluation. 32 However, it remains unknown whether there is an association between macroscopic features and mutations in PTC. Therefore, we aimed to identify the association between clinicopathologic features, including macroscopic features, and the coexistent BRAFV600E and TERT-p mutations in patients with PTC.
Materials and Methods
Participants
We retrospectively screened the medical records of 1936 consecutive patients who underwent thyroidectomy as the first surgery at the Yamashita Thyroid Hospital in Fukuoka, Japan, between January 2018 and October 2023, and for which cases were histologically diagnosed as PTC at Atomic Bomb Disease Institute, Nagasaki University. Among them, data on the status of both BRAFV600E and TERT-p mutations c.-124C > T (C228T) or c.-146C > T (C250T) were available for 532 patients. Subsequently, 157 patients with tumor sizes ≤1.0 cm were excluded because of the rarity of TERT-p mutations and excellent prognosis in most cases. 33 –37 We found only one case (0.6%) harboring both mutations from the excluded 157 cases. Ultimately, 375 patients were selected for evaluation in this study (Fig. 1).

Flow diagram showing the number of participants in this study. PTC, papillary thyroid carcinoma.
This study was conducted in accordance with the tenets of the Declaration of Helsinki and approved by the Institutional Ethical Committee for Medical Research at Nagasaki University (approval date: April 28, 2023; #15062617-6). Informed consent was obtained from all participants involved in the study in the form of opt-outs.
Processing of resected thyroid glands
The resected thyroid glands were immediately immersed in a fixative (neutral buffered, 10% formalin solution) for 20–24 hours. The fixed specimens were sagittally sliced to yield specimens with a thickness of 3–5 mm 38 ; subsequently, the obtained sagittal slices were photographed. All gross images have been stored in a computerized system for pathological diagnosis, along with clinical information, at our department (Department of Tumor and Diagnostic Pathology, Atomic Bomb Disease Institute, Nagasaki University). Clinical information includes age, sex, medical history, thyroid biochemical tests, preoperative diagnosis, and surgical procedure, provided by Yamashita Thyroid Hospital, Fukuoka, Japan. The system includes only the computer and software.
Definition of pathological features
At least three thyroid pathology specialists in our department confirmed the pathological features of thyroid tumors. Macroscopic features, including tumor size, margins, presence of papillary excrescences, and solid/cystic cut surfaces, were retrospectively evaluated based on macroscopic images. Tumor size was measured based on the maximal dimensions of the tumor. 32 A tumor size exceeding 2.0 cm independently impacts the prognosis of recurrences in PTC. 39,40 Furthermore, 2.0 cm is the threshold dividing T1 and T2 stages of PTC. 41 Therefore, we divided the patients into two groups using 2.0 cm as the cutoff point. Features of tumor margins were classified into four types (Fig. 2): (i) smooth margin (well-circumscribed and smooth pushing-type boundary), (ii) irregular shape (spiculated and/or pointed portion in the tumor border), (iii) lobulated configuration (round and consecutive protrusions in the tumor border), and (iv) ill-defined border (could not be clearly distinguished from the surrounding thyroid tissue) according to the US-imaging classification system, which exhibits high consistency among observers. 42 –44 Cases with mixed feature types of tumor margin were classified based on the dominant feature. Considering the notable prevalence of the double mutation in PTC tumors with lobulated configuration (81.3%; 26 of 32 cases), we divided the patients into two groups based on tumor margins, with and without lobulated configuration. Papillary excrescences were defined as microcystic and solid patterns, comprising delicate papillae interspersed with dot-shaped, yellow-whitish components. These components reflect a microscopic growth pattern characterized by slender, extended, and branching papillae, accompanied by psammoma bodies or scant organized stroma (Fig. 3); it was recorded when papillae occupied more than 50% of the tumor. A solid-cut surface was reported if there was no apparent cystic component. 42 Representative images of macroscopic features are presented in Figures 2 and 3.

Tumor margins of resected papillary thyroid carcinoma tissues. (

Tumors showing papillary excrescences on the cut surface. This figure shows a microcystic (white asterisks) and solid pattern, consisting of delicate papillae mixed with dot-shaped, yellow-whitish components (green arrows) (
The following data on clinicopathologic features of PTC were reported: age, sex, multifocality, extrathyroidal extension (ETE), histological subtypes, lymphatic invasion, vascular invasion, calcification, chronic thyroiditis, lymph node metastasis (LNM), Ki-67 labeling index (LI), molecular testing results, distant metastasis, and recurrence. ETE was classified as minimal ETE (tumor invaded the peri-thyroidal connective tissue) and gross ETE (tumor invaded the strap muscles or major neck structures). 41 Aggressive histological subtypes included diffuse sclerosing, tall cell, columnar cell, solid, and hobnail subtypes. 45 Ki-67 LI was evaluated as previously reported, 46 and cases with an LI <5% were considered low-risk tumors. 47 Disease recurrence was defined as the reappearance of a tumor (local lesion, regional, or distant metastasis) and histologically confirmed at least 6 months after the initial surgery. 6,48
DNA extraction and droplet digital polymerase chain reaction for BRAFV600E and TERT-p mutations c.-124C> T (C228T) or c.-146C > T (C250T)
To analyze BRAFV600E and TERT-p mutations, genomic DNA was extracted from formalin-fixed, paraffin-embedded (FFPE) tumor tissues of the PTC tumor via macrodissection, guided by a hematoxylin and eosin-stained slide. DNA extraction was performed using the Maxwell RSC DNA FFPE Kit (Promega, Madison, WI, USA) and Maxwell RSC Instrument (Promega) as described previously. 49 Droplet digital polymerase chain reaction analysis was performed to detect BRAFV600E and TERT-p mutations c.-124C > T (C228T) or c.-146C > T (C250T) as described previously. 48 –50
Statistical analyses
Categorical parameters are presented as numbers and percentages. Non-normally distributed continuous variables are presented as the median and interquartile range (IQR). Pearson’s chi-square or Fisher’s exact tests were used to analyze the relationship between clinicopathologic features and the coexistence of BRAFV600E and TERT-p mutations c.-124C > T (C228T) or c.-146C > T (C250T) when appropriate. The Mann–Whitney U test was used for continuous variables. All examined clinicopathologic features, including demographic factors (age and sex), gross features, and microscopic features, were simultaneously included in the multivariable logistic regression analyses to identify features associated with the double mutation. The Kaplan–Meier method was used to calculate the disease-free survival (DFS) rate, with statistical significance determined using the log-rank test. The duration of DFS was calculated from the date of initial surgery to the date of recurrence. In patients with PTC, tumor recurrence is significantly associated with multifocality, ETE, LNM, distance metastasis, and Ki-67 LI. 6,47 Cox proportional hazards models were applied to investigate the association between DFS and potential factors, including age, sex, gross features, the double mutation, and the identified features. The odds ratios (OR), hazard ratios (HR), and 95% confidence intervals (CI) were determined. Statistical analyses were performed using the IBM SPSS Statistics software version 29.0 (IBM, Armonk, NY, USA). p values <0.05 were considered significant, and all p values were two-sided.
Results
Clinicopathologic and molecular features of PTC analyzed in this study
The clinicopathologic and molecular features of the PTC cases are summarized in Table 1. Among the 375 patients studied, including 307 females (81.9%), the median age was 53 years (IQR 39–69), and the age of 176 patients was ≥55 years (46.9%). The median tumor size was 1.9 cm (IQR 1.4–2.7); this included 170 cases with a tumor size >2.0 cm (45.3%). Regarding the gross appearance of tumors, we found smooth margins, irregular shape, lobulated configuration, and ill-defined borders in 63 (16.8%), 264 (70.4%), 32 (8.5%), and 16 (4.3%) cases, respectively. Papillary excrescences were observed in 54 (14.4%) cases, and solid-cut surfaces were recorded in 286 (76.3%) cases. Minimal ETE was present in 145 (38.7%) patients, and gross ETE was found in 108 (28.8%) patients. Aggressive histological subtypes were identified in 13 (3.5%) patients. The prevalences of multifocality, lymphatic vessel invasion, vascular invasion, calcification, and chronic thyroiditis were 34.4%, 30.9%, 54.4%, 18.4%, and 28.3%, respectively. A majority (70.4%) of patients had LNM. The Ki-67 LI was ≥5% in 212 (56.5%) patients. At the time of diagnosis, distant metastases were identified in nine (2.4%) patients. A total of 68 (18.1%) patients were negative for both BRAFV600E and TERT-p mutations, while 78 (20.8%) patients harbored both mutations. There were 226 (60.3%) patients who were positive for BRAFV600E but negative for TERT-p mutations. Additionally, three (0.8%) cases carried TERT-p mutations without the presence of BRAFV600E mutations. The median follow-up period was 49 months, and recurrence occurred in 12 (3.2%) patients. The association between gross and clinicopathologic features is summarized in Supplementary Table S1.
Clinicopathologic Features and Mutation Status of Papillary Thyroid Carcinoma in This Study
BRAFV600E and TERT promoter C228T/C250T.
ETE, extrathyroidal extension; gross ETE, invasion to strap muscles or major neck structures; IQR, interquartile range; minimal ETE, invasion to peri-thyroidal connective tissue.
Association between clinicopathologic features and the BRAFV600E and TERT-p double mutation c.-124C > T (C228T) or c.-146C > T (C250T)
Univariable analysis indicated a significant association between the double mutation and age ≥55 years, tumor size >2.0 cm, lobulated configuration, papillary excrescences, ETE, Ki-67 LI ≥5%, and recurrence (p < 0.001; Table 2). No significant association was found between the double mutation and other factors.
Univariable Analysis for the Association Between Clinicopathologic Features and the Coexistence of BRAFV600E and Tert Promoter Mutations
Coexistence of BRAFV600E and TERT promoter mutation.
Multivariable analysis for factors associated with BRAFV600E and TERT-p double mutations c.-124C > T (C228T) or c.-146C > T (C250T)
Multivariable analysis revealed that relatively old age (≥55 years) (OR = 12.083, CI 4.498–32.456, p < 0.001), large tumor size (>2.0 cm) (OR = 2.722, CI 1.104–6.712, p = 0.030), lobulated configuration at the tumor margin (OR = 16.114, CI 3.155–82.296, p < 0.001), papillary excrescences on the cut surface (OR = 17.573, CI 3.462–89.201, p < 0.001), solid-cut surface (OR = 4.012, CI 1.084–14.849, p = 0.037), minimal ETE (OR = 4.156, CI 1.209–14.282, p = 0.024), gross ETE (OR = 6.517, CI 1.734–24.490, p = 0.006), and Ki-67 LI (≥5%, OR = 12.145, CI 4.354–33.877, p < 0.001) were significantly associated with the double mutation (Table 3).
Multivariable Analysis for Features Associated with Coexistence of BRAFV600E and Tert Promoter Mutations
CI, confidential interval; OR, odds ratio.
Analysis for clinicopathologic and molecular features associated with DFS in PTC
Fig. 4 represents Kaplan–Meier survival curve illustrating DFS according to the presence of the double mutation (A) and gross features, such as lobulated configuration (B) and papillary excrescences (C), analyzed using the log-rank test. The association between DFS and clinicopathologic and molecular features was investigated (Table 4). In the univariable analysis, lobulated configuration, the presence of papillary excrescences, and the double mutation were associated with DFS. However, in the multivariable analysis, only the double mutation remained correlated with DFS (HR = 7.789, CI 1.279–47.443, p = 0.026). The association between recurrence and clinicopathological and molecular features is shown in Supplementary Table S2.
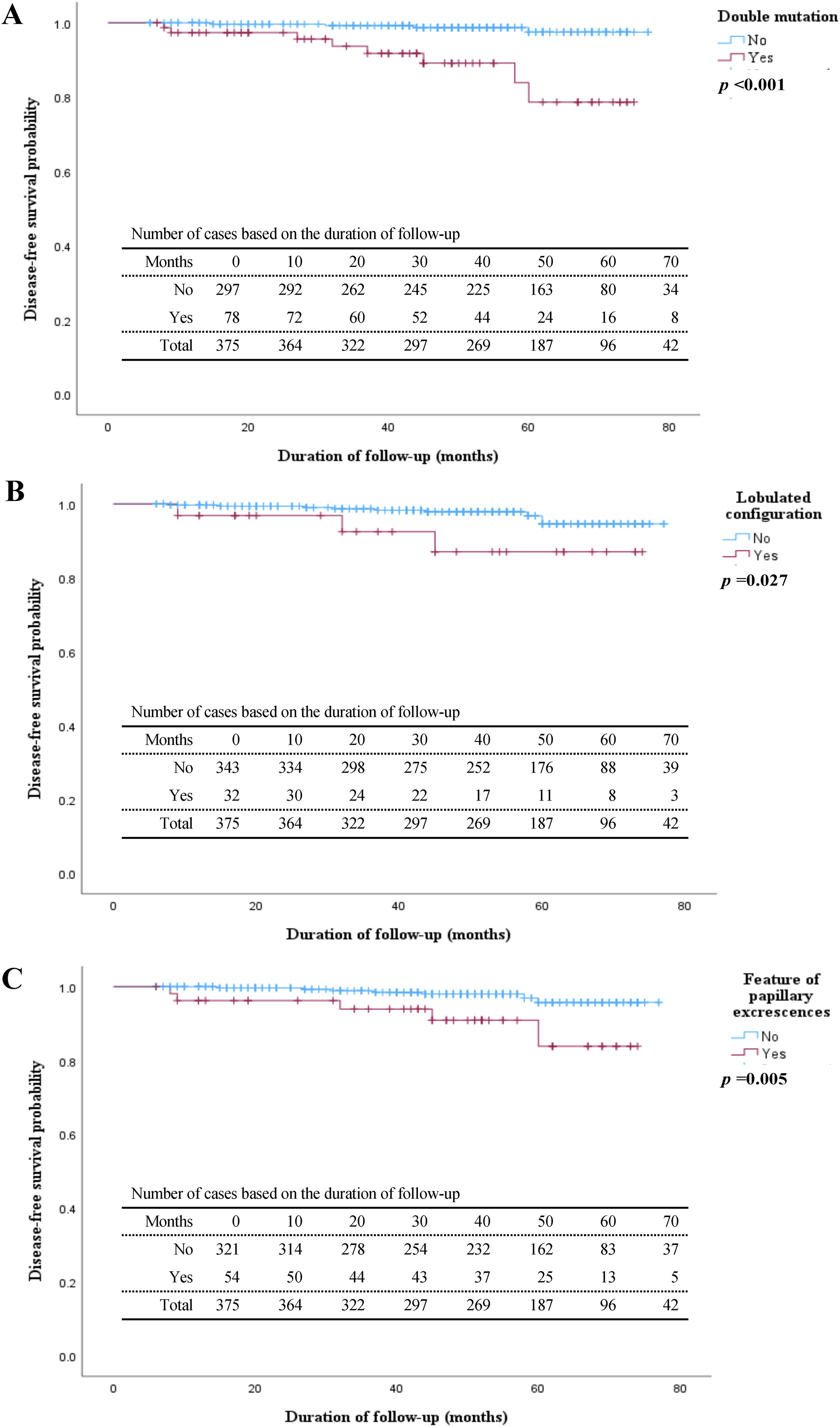
Kaplan–Meier survival curve illustrating disease-free survival according to the presence of the double mutation (coexistence of BRAFV600E
and TERT promoter mutations) (
Cox Proportional Hazards Regression Analysis for Clinicopathologic and Molecular Features Associated with Disease-Free Survival in Papillary Thyroid Carcinoma
Coexistence of BRAFV600E and TERT promoter mutations.
HR, hazard ratio.
Discussion
Several meta-analyses have reported that the BRAFV600E and TERT-p double mutations can be considered strong predictors for poor outcomes of PTC. 23,24 The present study demonstrated that the combination of these mutations in PTC was significantly associated with relatively old age, large tumor size, lobulated configuration in tumor margin, papillary excrescences on the cut surface, solid-cut surface, ETE, Ki-67 LI, and short DFS. The gross examination of resected tissues is necessary to select relevant sections for microscopic examination, leading to an accurate diagnosis. 31 However, although the number of thyroid cancer publications is increasing annually, 51 studies addressing the macroscopic characteristics of PTC are limited. To the best of our knowledge, our study is the first to investigate the association between macroscopic information from resected tumors and the status of two gene mutations with other clinicopathologic features of PTC.
The prevalence of coexistent BRAFV600E and TERT-p mutations in our study was higher than that in previously reported rates (20.8% vs. 8.3%–13.0%, respectively). 24,25 Possible explanations for this difference include the large tumor size (>1.0 cm) and the high median age (53 years) of our cohort. Another explanation may be the use of ddPCR assay, which is a highly sensitive method for detecting BRAFV600E and TERT-p mutations in PTC. 52 –54
We found that the relative frequency of lobulated configuration was 16 times higher in the PTCs with the double mutation. Our results also indicated that papillary excrescences on the cut surface were significantly associated with the double mutation. Particularly, 30.8% of PTC tumors carrying the double mutation exhibited papillary excrescences in the present study. Additionally, tumor size >2.0 cm and a solid-cut surface were significantly correlated with the double mutation in multivariable analysis. Thus, our gross classification represents a feature related to the double mutation in PTC tumors.
A positive association of ETE with the double mutation in PTC has been previously reported. 22,24,37 Although minimal ETE is not included in the staging for differentiated thyroid cancer in the eighth edition of the American Joint Committee on Cancer staging manual, 41 several studies indicated that minimal ETE represents a risk factor for poor prognosis in patients with PTC. 55,56 Our multivariable analysis indicated that both minimal and gross ETE were significantly related to the double mutation in PTC (OR 4.156 vs. 6.517, respectively).
Our multivariable analysis found that a high Ki-67 LI, such as ≥5%, was significantly associated with the presence of a double mutation. Particularly, 89.7% of PTC cases with the double mutation showed a high Ki-67 LI. The Ki-67 LI has been considered a promising predictor for the recurrence of PTC, and PTC cases with Ki-67 LI <5% are considered low-risk for tumor recurrence regardless of the presence of BRAFV600E or TERT-p mutation. 47 The present study demonstrated a significant association of high Ki-67 LI (≥5%) with lobulated configuration in tumor margin, but no significant association with papillary excrescences (Supplementary Table S1).
Our study demonstrated the association between macroscopic characteristics of resected tumors, such as tumor size, type of tumor margin, features on the cut surface of tumors, and mutation status, with other clinicopathologic features of PTC. Therefore, a gross examination should be considered in the pathological analysis of PTC. However, our study had some limitations. First, it was conducted retrospectively at a single center, which may introduce selection bias. Second, ultrasound features were not included due to the retrospective study design. Third, the short median follow-up time and low recurrence rate limited our ability to assess the impact of macroscopic factors on DFS. Multicenter prospective studies with large sample sizes and prolonged follow-up durations are needed to further clarify the findings of this study.
In conclusion, the BRAFV600E and TERT-p double mutation in PTC was significantly associated with relatively old age, large tumor size, lobulated configuration in tumor margin, papillary excrescences on the cut surface, solid-cut surface, ETE, and high Ki-67 LI. These features were suggestive of the presence of the double mutation and should be analyzed at the molecular level in patients with PTC.
Footnotes
Authors’ Contributions
N.T.N.A. and N.V.P.T. were involved in conceptualization, data acquisition, methodology, formal analysis, and writing original draft. H.K., K.M., Z.M., Y.M., N.T.N, Y.S., and M.N. were involved in methodology, histological diagnosis, and molecular analysis. Y.A. was involved in editing the original draft. K.Y. was involved in statistical analyses. S.S. and H.Y. were involved in surgical treatment, sample collection, and data acquisition. M.N. was involved in conceptualization, methodology, histological diagnosis, writing the original draft, editing, and supervision. All the authors reviewed the work critically for important intellectual content, approved the final version of the article to be published, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Author Disclosure Statement
The authors have stated that they have no conflicts of interest.
Funding Information
This work was funded by the Atomic Bomb Disease Institute, Nagasaki University, and
Supplementary Material
Supplementary Table S1
Supplementary Table S2