
Abstract
Background:
Levothyroxine to suppress thyrotropin (TSH) to <0.5 mIU/L following thyroidectomy in differentiated thyroid cancer (DTC) may reduce recurrence in higher-risk DTC. However, there is limited evidence to support guideline recommendations to maintain TSH in the low-normal range of 0.5–2 mIU/L to reduce recurrence in patients with lower risk DTC. The primary objective was to assess the association between exposure to high normal serum TSH (2–4 mIU/L) as compared with low normal TSH (0.5–2 mIU/L) target ranges and cancer recurrence in patients with DTC after thyroidectomy.
Methods:
This population-based retrospective cohort study used linked, administrative health care databases from Ontario, Canada, to follow patients with DTC post-thyroidectomy from 2007 to 2018. The exposure was time updated, serum TSH, treated as a cumulative and instantaneous exposure. Multivariable cause-specific proportional hazard regression analyses were performed to determine time to DTC recurrence from index date, defined as a composite of repeat neck surgery, radioactive iodine (RAI) treatment, and/or DTC-specific death. Results were also stratified by initial treatment as a marker of baseline recurrence risk in a sensitivity analysis.
Results:
This cohort of 26,336 individuals (78% female) with DTC and a median age of 50 years were followed for a median of 5.9 (interquartile range 3.6–8.6) years; 40.9% were initially treated with a hemi-thyroidectomy only and 38.2% received a total thyroidectomy and RAI. Compared with exposure to TSH 0.5 to ≤2 mIU/L, DTC recurrence rate was similar for each additional 3 months of exposure to TSH >2 to ≤4 mIU/L (adjusted cause specific [cs] hazard ratio [HR] 0.99 [confidence interval or CI 0.97–1.02]) but was significantly increased with each additional 3 months of exposure to TSH >4 mIU/L (adjusted csHR 1.07 [CI 1.04–1.09]). Results were similar across baseline treatment groups.
Conclusion:
There was no difference in clinically significant recurrence in those with low-risk DTC maintained with a TSH of 0.5–2 mIU/L compared with 2–4 mIU/L. Guidelines should consider liberalizing target TSH level post thyroidectomy in low-risk cohorts. These results cannot be applied to patients with high-risk DTC.
Introduction
Thyroid cancer is the most common endocrine neoplasm and ninth most common cancer globally. 1 Differentiated thyroid cancer (DTC) comprises 90% of all thyroid cancer cases. 1 Between 1998 and 2012, there was a significant increase in thyroid cancer incidence globally. 2 This rising incidence has been driven by an increase in small, early-stage papillary thyroid cancers, which are associated with an excellent 5-year disease-specific survival of >99%. 3,4
DTC is treated with total or hemi-thyroidectomy with or without radioactive iodine (RAI), followed by levothyroxine (LT4) therapy to replace thyroid hormone and to reduce the risk of DTC recurrence. 5 The American Thyroid Association (ATA) recommends treatment to a target serum thyrotropin (TSH) below normal (<0.5 mIU/L) in high-risk DTC, which has been associated with improved survival. 6 For low-risk DTC treated with total or hemi-thyroidectomy, the ATA recommends maintaining TSH in the low normal range of 0.5 and 2 mIU/L. However, evidence for this recommendation is limited and mixed. 5 Moreover, more than half of patients treated with a hemi-thyroidectomy require LT4 not necessarily to maintain normal thyroid function but to achieve the recommended TSH target. 7 Given most of the increased incidence of DTC is mediated by small, low-risk tumors, it is important to better define ideal TSH targets in this population in order to avoid unnecessary overtreatment.
Targeting a tighter TSH range in patients with DTC may also be harmful for patients and costly to the health care system. 8 Potential harms include unnecessary treatment, extra laboratory monitoring and physician visits, effects of overtreatment such as atrial fibrillation, osteoporosis, and reduced quality of life. 8,9 It is also projected that the cost of managing thyroid cancer in the United States will exceed $3.5 billion by 2030. 10 If the TSH target range can be safely broadened, then this may improve patient outcomes and reduce health care costs.
In this context, our primary objective was to determine whether cumulative exposure to high normal serum TSH (2–4 mIU/L) is associated with a higher risk of DTC recurrence than exposure to the recommended low normal TSH (0.5–2 mIU/L) in patients with DTC after a total or hemi-thyroidectomy.
Materials and Methods
Overall study design, setting, and ethics
We performed a retrospective, population-based, cohort study from 2007 to 2018 using linked, health care administrative databases, housed at Institute for Clinical Evaluative Sciences (CES) in Ontario, Canada. These data contain health records of over 13 million residents covered by the universal health care insurance program in Ontario. This study was approved by ICES and the Office of Research Ethics at University of Toronto (study number 2022 0990 519 000). The use of the data in this project was authorized under section 45 and approved by ICES’ Privacy and Legal Office.
Data sources
We used the Ontario Cancer Registry to identify persons with DTC and to determine cancer-specific death. This is a well-validated registry that captures 99% of cancer cases in Ontario. 11 The Office of the Registrar General—Deaths database was used to determine all-cause death. Health services use to identify procedures and diagnoses was determined using data from the Canadian Institute for Health Information (CIHI) Discharge Abstract Database/Same-Day Surgery database, The CIHI National Ambulatory Care Reporting System, and the Ontario Health Insurance Plan (OHIP) physician billing claims database. The OHIP database captures physician billings under the fee for service model and does not include private health care or services rendered by physicians who are salaried and are reimbursed through alternative payment plans. Of note, there is no alternate care plan or private health care for oncology patients in Ontario. 12 MOMBABY database was used to identify patients who had a pregnancy during the study period. 13
We used Ontario Laboratories Information System (OLIS) to determine serum TSH values and their measurement dates. OLIS captures almost all outpatient, community laboratory tests in Ontario. 14 While not all hospital laboratories send data to OLIS, as of 2017, 134 of 147 (91%) of hospitals in Ontario were contributing. 15 We used ICES-derived Ontario Hypertension Dataset, Ontario Congestive Heart Failure Database, and Ontario Diabetes Database to identify individuals with pertinent comorbidities. 16 –18 All datasets were linked, anonymized, encoded, and analyzed at ICES.
Study timeline
Supplementary Appendix Figure S1 shows the study timeline and variable definitions. Patients were followed for serum TSH measurements and DTC recurrence from the index date, defined as 12 months after the date of their initial thyroidectomy. The first 12 months after thyroidectomy were excluded from follow-up to allow for additional surgery or initial RAI treatment to be given to eligible patients and for intended TSH targets to be achieved. Follow-up was discontinued if there was no TSH measurement for 12 months or if a patient became pregnant. Patients re-entered the cohort, and follow-up was resumed if a new TSH value became available or 12 months after conception. Outcomes that occurred during these inactive periods were not included for analyses. Censoring occurred if patients had reached the end of follow-up, if they developed an exclusion criterion, or if a competing event had occurred.
Study population
We included men and women, age ≥18 years, diagnosed with DTC (Internal Classification of Disease ICD-O-3: C739) between 2007 and 2018, treated surgically either with hemi-thyroidectomy or total thyroidectomy 3 months prior to and up to 12 months following the DTC diagnosis. Eligibility criteria included a valid health card identification number, alive 1 year after surgery, and at least one TSH value available during follow-up.
Exclusion criteria included (i.) missing birth date, death date (for those who died), or sex; (ii.) invalid health coverage; (iii.) a hospital admission for more than 30 days following thyroidectomy; (iv.) previous history of any cancer prior to DTC; (v) long-term or complex continuing care at baseline; and (vi.) any delivery within 12 months between DTC diagnosis and index date.
Outcomes
The primary composite outcome was time from index date to death from DTC or a first treatment for DTC recurrence (hereby referred to as DTC recurrence). DTC recurrence was defined as the first event of (i) death from DTC, or DTC recurrence requiring treatment based on (ii.) repeat surgery (thyroidectomy or neck dissection), or (iii.) RAI occurring after index date. Hall et al. have previously demonstrated internal reliability of these data. 12,19,20 Secondary outcomes included each individual event comprising the composite outcome. A full list of definitions and codes used to identify the outcomes is shown in Supplementary Appendix Table S1.
Primary exposure
The primary exposure was serum TSH, which was treated as a time-dependent covariate, updated every 90 days if a new TSH measurement was available. If there was more than one TSH value during any given 90-day period, the mean of all TSH values was calculated and used as the TSH exposure for that particular time period. We chose 90-day intervals as LT4 doses are usually not changed more frequently than every 2–3 months. 21 If a new TSH value was not available after 3 months, the TSH from the prior 3 months was carried forward until a new TSH became available. A TSH measurement within 1 week of a recurrence outcome for which RAI was used as treatment was excluded due to the possibility of an intentionally stimulated TSH in preparation for RAI.
Serum TSH was classified into mutually exclusive categories, with TSH >2 to ≤4 mIU/L as the primary exposure and TSH of 0.5–2 mIU/L as the referent category. Secondary exposures were TSH <0.5 mIU/L and >4 mIU/L. We first considered TSH level as a time-updated “cumulative” exposure, based on a hypothesized direct dose–response relationship with cancer recurrence. We examined the cumulative effect of exposure to a particular TSH level on cancer recurrence with the following question: for any given individual, how does recurrence risk change for each additional 3 number of months of exposure to TSH of >2 to ≤4 mIU/L rather than a TSH of 0.5–2 mIU/L, assuming cumulative exposure at the other two levels remains the same. Time-updated, cumulative TSH was modeled by creating three separate variables that counted the total number of periods exposed to a particular TSH level (one for cumulative TSH <0.5 mIU/L, one for cumulative TSH >2 to ≤4 mIU/L, and one for cumulative TSH >4 mIU/L; Supplementary Appendix Fig. S2). We adjusted for the number of 3-month periods spent in different TSH levels for each patient as a covariate in a multivariable model.
As secondary analyses, TSH was considered as (i.) a time-updated, instantaneous categorical variable where we treated TSH as a 4-level categorical time-dependent variable (TSH <0.5 mIU/L, 0.5–2.0 mIU/L, TSH >2 to ≤4 mIU/L, and >4 mIU/L) and (ii.) a time-updated, instantaneous continuous variable.
Covariates
Covariates that were measured at index date included year of DTC diagnosis, age, sex, rurality, and deprivation quintile, a measure of socioeconomic status. History of hypertension, heart failure, and diabetes were all defined at index date and updated annually during follow-up. We also captured any history of atrial fibrillation, cerebrovascular disease, and fracture 5 years prior to index and comorbidities measured by Johns Hopkins ACG® System (v10.0) Aggregated Diagnosis Groups (ADG) score in the 2 years prior to index date. 22 Baseline DTC treatment was categorized as follows: (i.) hemi-thyroidectomy only (which includes partial thyroidectomy, lobectomy, and hemithyroidectomy); (ii.) total thyroidectomy only; and (3) total thyroidectomy and RAI treatment. A list of covariates, their definitions, and data sources is shown in Supplementary Appendix Table S2.
Statistical analysis
Distributions of baseline clinical characteristics were examined for the entire cohort, using descriptive statistics.
For the primary outcome of time to cancer recurrence and each of the secondary outcomes, we constructed a multivariable cause-specific regression model to evaluate whether serum TSH exposure was significantly associated with time to the composite DTC recurrence after adjustment for other factors. We adjusted for clinically relevant covariates which were selected a priori and accounted for competing risks. The competing events were as follows: (i.) all cause death and RAI were competing events for the subcomponent of repeat surgery, (ii.) all cause death and repeat surgery were competing events for RAI, and (iii.) noncancer death, RAI, and repeat surgery were competing events for DTC-specific death.
To address our primary objective, we compared outcomes between exposure with a high-normal TSH range of >2 to ≤4 mIU/L and a low-normal TSH range of 0.5 to ≤2 mIU/L (referent). Exposure to other TSH categories was also compared with the referent category as a secondary analysis. Additional secondary analyses also included TSH modeled as an instantaneous, categorical, time-updated variable and an instantaneous, continuous, time-updated variable. Sensitivity analyses included stratification by baseline DTC treatment as an estimate of baseline recurrence risk, and changing the index date from 12 months after initial thyroidectomy to 18 months due to the possibility that initial RAI treatment may have been delayed beyond 12 months after surgery and misclassified as a recurrence.
All analyses were performed using SAS software v9.4 (SAS Institute Inc, Cary, NC, USA). All tests were two-sided with p-values <0.05 considered statistically significant.
Results
Baseline data
Our final cohort consisted of 26,336 individuals with DTC (Fig. 1). As shown in Table 1, the mean age at index was 50.4 years (standard deviation [SD] 13.7 years), and the majority were women (78%) living in urban centers (93%). Approximately 20% of the cohort underwent hemi-thyroidectomy, 40% had a total thyroidectomy, and about 40% had total thyroidectomy followed by RAI.
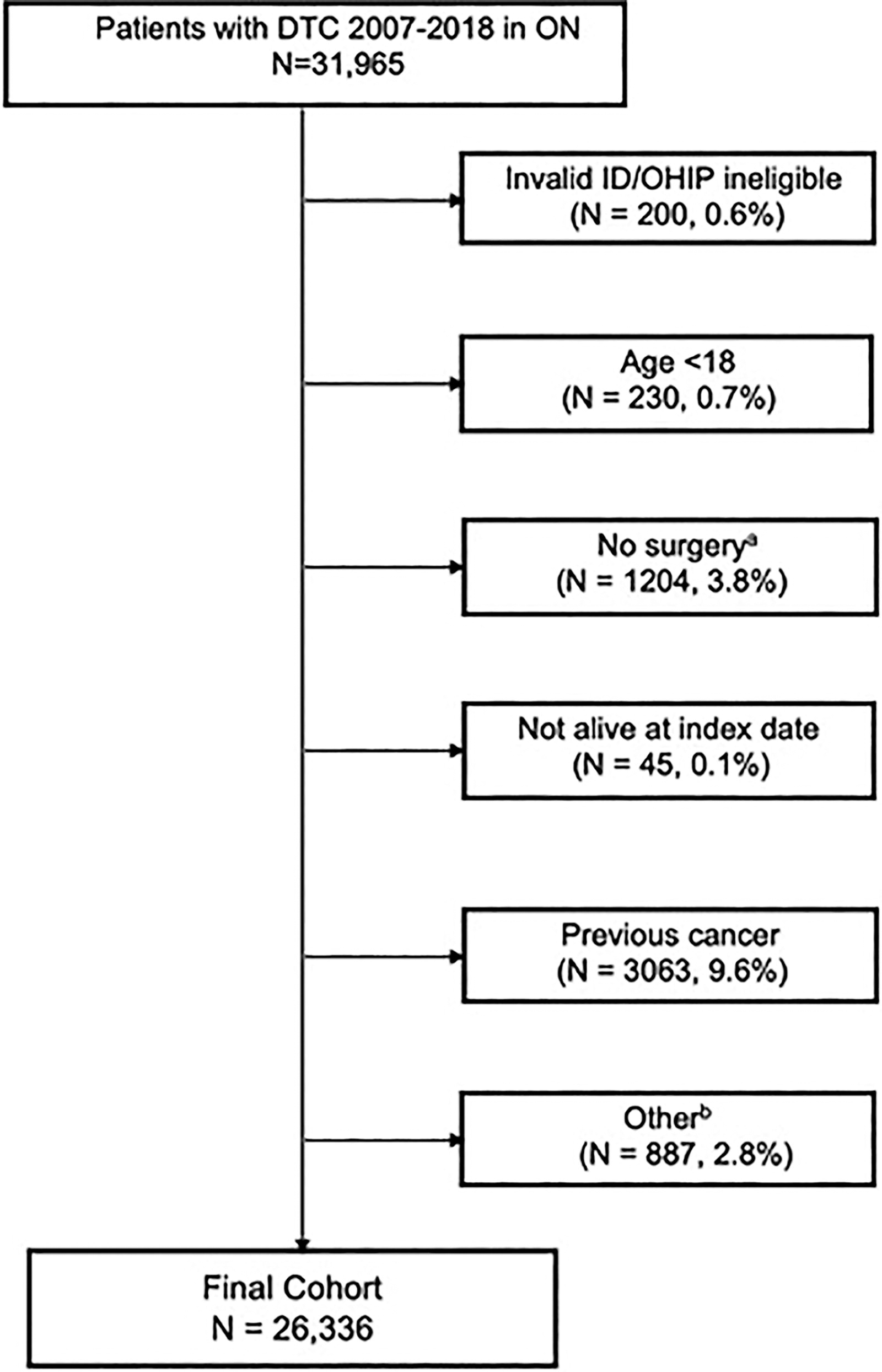
Cohort creation. aWithin −3 to +12 months following diagnosis. bAdmission for surgery >30 days or resides in long-term care, no TSH. DTC, differentiated thyroid cancer; ID, identification; OHIP, Ontario Health Insurance Plan; ON, Ontario; TSH, thyrotropin.
Baseline Characteristics of Patients with Differentiated Thyroid Cancer Diagnosed in Ontario and Treated with Surgery Between 2007 and 2018 (N = 26,336)
Over a median follow-up of 5.9 (interquartile range [IQR] 3.6–8.6) years from index date, the median serum TSH was 0.6 mIU/L (IQR 0.1–1.8 mIU/L), and the mean TSH was 2.6 mIU/L (SD 9.7 mIU/L). There were 2817 DTC recurrence events (10% of the cohort). Of those, 361 (1.3%) had a repeat thyroidectomy, 689 (2.6%) had a neck dissection, 1664 (6.3%) had RAI treatment, and there were 103 (0.3%) DTC-specific deaths. Less than 3% of the cohort were censored due to death (103/26,336 DTC-specific deaths, or 0.3% of the cohort and 617/26,336 for noncancer deaths, 2.3% of the entire cohort).
Primary and secondary analyses
In adjusted analyses, there was no increase in recurrence risk for each additional 3 months of cumulative exposure to TSH >2 to ≤4 mIU/L as compared with TSH 0.5 to ≤2 mIU/L, accounting for competing risks (adjusted cause specific [cs] hazard ratio [HR] 0.99 [confidence interval or CI 0.97–1.02], p = 0.55). In contrast, there was a significantly higher estimated DTC recurrence for each additional 3 months of cumulative exposure to TSH >4 mIU/L compared with TSH 0.5 to ≤2 mIU/L (csHR 1.07 [CI 1.04–1.09], p < 0.01; Fig. 2). As shown in Table 2, the estimated risk of composite recurrence increased with longer duration of exposure to TSH >4 mIU/L in a dose-dependent fashion.
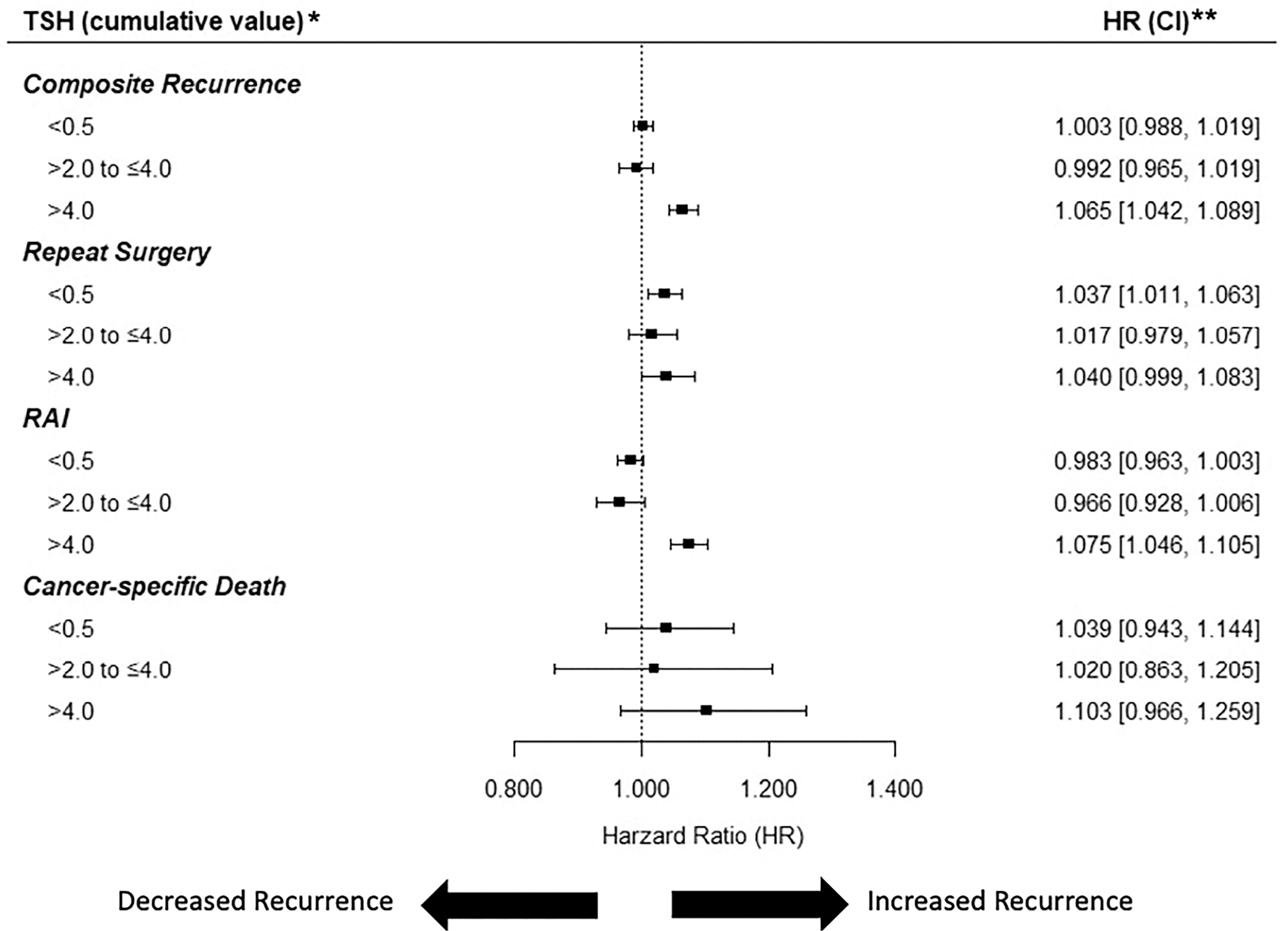
Forest plot showing the association between cumulative TSH and composite recurrence with subcomponents adjusted for relevant covariates and competing risks. TSH analyzed as a cumulative exposure. *Compared with referent TSH category of 0.5 to ≤2 mIU/L, TSH values expressed in mIU/L. **Hazard ratio adjusted for year of diagnosis, age, sex, rurality, neck dissection, Johns Hopkins Aggregated Diagnosis Groups (ADG score), treatment group (three groups). CI, confidence interval; HR, hazard ratio; RAI, radioactive iodine.
Estimated Effect of 3 Months, 6 Months, 12 Months, 2 Years, and 4 Years of Exposure to TSH >4 mIU/L Compared with TSH 0.5 to <2.0 mIU/L on Composite DTC Recurrence
The estimated effect of 3, 6, 12, 24, and 48 additional months of exposure at a particular TSH level rather than TSH level of 0.5–2.0, assuming cumulative exposure at the remaining two TSH groups is the same.
Adjusted for year of diagnosis, age, sex, rurality, neck dissection, ADG score, and treatment (3-group).
ADG, Aggregated Diagnosis Groups; CI, confidence interval; DTC, differentiated thyroid cancer; HR, hazard ratio; TSH, thyrotropin.
In secondary analyses, results were largely similar to the primary analysis when TSH was considered an instantaneous categorical variable (Supplementary Appendix Fig. S3). We found a modestly significant association between TSH and composite recurrence when TSH was treated as a continuous variable (csHR 1.001 [CI 1.001–1.001], p < 0.01).
Sensitivity analyses
Findings were similar when analyses were stratified by baseline treatment (Table 3) and when we changed the index date from 12 months to 18 months after thyroidectomy (Supplementary Appendix Table S3).
Adjusted Cause Specific Hazard Ratios—Subgroup Analyses Based on Initial Treatment, TSH as Cumulative Exposure (Referent Category: TSH 0.5–2 mIU/L) a
Hazard ratio shown for each additional 3 months of exposure to a particular TSH rather than a referent TSH level of 0.5 to ≤ 2 mIU/L, assuming cumulative exposure at the remaining two TSH groups is the same.
Adjusted for year of diagnosis, age, sex, rurality, neck dissection, and ADG score.
csHR, cause-specific hazard ratio.
Discussion
In this large population-based cohort study of patients with DTC who underwent thyroidectomy, exposure to serum TSH in the high normal range of 2–4 mIU/L was associated with a similar DTC recurrence compared with exposure to a low normal serum TSH of 0.5–2 mIU/L. In contrast, DTC recurrence significantly increased with increasing exposure to an elevated TSH of over 4 mIU/L in a dose-dependent fashion. These results were similar for patients who received a hemithyroidectomy and a total thyroidectomy with or without RAI, after adjustment for relevant covariates, and when TSH was considered as both a cumulative and instantaneous exposure, demonstrating the robustness of our findings. Our findings suggest that there is no added benefit of maintaining a low normal compared to high normal TSH range on reducing DTC recurrence, and thus do not support the current ATA guidelines for LT4 treatment targets in patients with low-risk DTC.
The ATA recommendation for a low normal TSH target post total thyroidectomy is based on evidence primarily from one cohort study. 23 In this single center study of <400 patients, Hovens et al. found that TSH >2 mIU/L as compared with TSH <2 mIU/L was associated with a greater risk of DTC recurrence. 23 As TSH was not treated as a time updated variable like in our study, these findings were vulnerable to a survival bias. 24 This study also did not distinguish between TSH values in the normal versus abnormal range, whereas our study of over 26,000 patients enabled more specific comparisons of TSH ranges. Finally, ∼40% of the patients in the study by Hovens et al. had nodal or metastatic disease, whereas most of our cohort likely had lower-risk disease based on their relatively lower recurrence rate. Our findings are similar to previous smaller reports in which TSH suppression did not improve disease-free survival in low-risk DTC 25,26 and provide more robust evidence against an increased risk of DTC recurrence with exposure to serum TSH in the high normal range. Updated guidelines that consider these more recent studies alongside our findings are warranted to avoid unnecessary treatment of low-risk DTC survivors after total thyroidectomy.
Among those who underwent a hemi-thyroidectomy only, which likely represent those at lowest risk of DTC recurrence, the risk of DTC recurrence was similar between exposure to low normal TSH and high normal TSH. These findings confirm previous reports, which demonstrated no benefit in keeping the TSH <2 mIU/L for DTC recurrence prevention in this population. 27,28 As over half of DTC survivors treated with a hemi-thyroidectomy are given LT4 therapy to maintain a TSH <2 mIU/L, broadening the TSH target to 0.5–4 mIU/L should be considered to reduce unnecessary lifelong treatment. In addition, this will help reduce potential adverse treatment-related effects such as atrial fibrillation, osteoporosis, cognitive disorders, 29 –32 reduce health care costs, 10 and enhance patient quality of life 8 without compromising disease-free survival. Although randomized controlled trials would provide a higher level of evidence, such a trial would require a large sample size, long follow-up, and high costs and, as such, may be difficult to complete. Until then, our findings likely provide the most robust evidence on this topic to date.
Consistent with previous evidence, 33 we demonstrated that exposure to TSH >4 mIU/L was correlated with higher recurrence in a dose-dependent fashion. There is strong biological basis for this association. DTC usually retains TSH receptors, and residual DTC tissue may grow in response to TSH stimulation. 5 Our findings indicate that a supraphysiologic TSH may thus lead to greater DTC recurrence, supporting the recommendation to maintain a TSH <4.0 mIU/L in all DTC survivors.
Strengths of this study include the large, population-based nature of the study, which minimized potential confounders and increased the generalizability of our data. We also used validated and comprehensive registries with an excellent DTC capture rate and rigorous methods, with robust findings across multiple secondary and sensitivity analyses. There are also several limitations. First, we did not have access to pathology reports or information on disease stage so baseline disease recurrence risk estimates were based on initial treatment patterns, which may have differed after the change in DTC treatment recommendations in 2015. Second, we did not have details on RAI dose, which may confound the association between TSH levels and disease recurrence. Third, the definition for recurrence was limited to recurrences that resulted in treatment; therefore, we could have missed some untreated recurrences. Fourth, our median follow-up of about 5 years was relatively short, and longer follow-up may be needed to detect differences in DTC recurrence. However, the highest risk of recurrence occurs within the first 5 years after DTC diagnosis 31 making this possibility less likely. Fifth, some TSH measurements may be missing as some hospital laboratories did not start contributing to OLIS until mid-2010s. In addition, residual confounding cannot be excluded due to the retrospective, observational nature of the study. Finally, as we had a primarily low-risk cohort, these results cannot be applied to patients with high-risk DTC, and further studies will be needed for that population.
To our knowledge, this is the first, large, population-based study with adequate power to determine that exposure to TSH in the higher normal range is not associated with worse disease-free survival in patients with DTC. An updated recommendation to allow serum TSH targets to be liberalized to 0.5–4 mIU/L in patients with low-risk DTC should be considered to help reduce unnecessary treatment and health care costs.
Footnotes
Acknowledgments
Parts of this material are based on data and information compiled and provided by CIHI, Ontario Health (OH), the Ontario Ministry of Health, and Ontario Registrar General (ORG). This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from ©Canada Post Corporation and Statistics Canada. Parts of this report are based on ORG information on deaths, the original source of which is ServiceOntario.
Authors’ Contributions
J.K.Q. was involved in study conception, design, data analysis, interpretation, and article writing and editing. R.S. was involved in study conception, design, data interpretation, and article editing. K.E. was involved in data analysis and interpretation as well as article editing. I.C.L., A.E., and A.Z. were involved in study design, data interpretation, and article editing. L.L. was involved in study conception, design, data analysis, interpretation, and article writing and editing.
Disclaimer
The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. The views expressed therein are those of the author and do not necessarily reflect those of ORG or the Ministry of Public and Business Service Delivery.
Author Disclosure Statement
None of the authors have any conflict of interest to declare.
Funding Information
This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care. This study also received funding from Canadian Institutes of Health Research and Peter Gilgan Centre for Women’s Cancers Research. The funding sources had no role in study design, collection, analysis, interpretation of data, in the writing of the report, or in the decision to submit the paper for publication. ICES is an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement.
Supplementary Material
Supplementary Appendix Figure S1
Supplementary Appendix Figure S2
Supplementary Appendix Figure S3
Supplementary Appendix Table S1
Supplementary Appendix Table S2
Supplementary Appendix Table S3