
Abstract
Background:
Thyroid hormones (THs) are essential endocrine hormones that play key roles in individual’s growth and development. There is limited knowledge about the association between maternal TH concentrations variations with normal thyroid function during pregnancy and offspring’s glycolipid metabolism.
Methods:
A total of 1130 mother–child pairs from the Ma’anshan birth cohort were included in this prospective study. Maternal TH levels and thyroid peroxidase antibodies were measured in the 1st, 2nd, and 3rd trimesters of pregnancy during the childhood follow-up period. Fasting venous blood was collected from children at 4–6 years of age and glycolipid metabolic indicators were assayed. Analyses were performed using Binary logistic regression models, linear regression models, and Generalized linear regression model.
Results:
Maternal TH trajectories were fitted via latent category growth models. During the 1st trimester of pregnancy, maternal T3 and free thyroxine (fT4) levels were positively associated with children’s blood glucose levels (β = 0.007 [CI 0.028–0.181]; β = 0.022 [CI 0.004–0.040]), whereas high levels of fT4 may be associated with decreased risk of children’s hypercholesterolemia (OR = 0.870 [CI 0.768–0.986]). Maternal T4 concentrations during the 3rd trimester of pregnancy were negatively associated with children’s cholesterol levels (β = −0.002 [CI −0.003–0.00]). High maternal TH levels were associated with high fasting glucose level and low low-density lipoprotein concentrations in children.
Conclusions:
Maternal TH dynamic variations may be associated with glycolipid metabolism in preschoolers, even when women do not have clinically diagnosed thyroid disorders. The exact associations between maternal THs in specific trimesters of pregnancy under normal thyroid function conditions and glycolipid metabolism in offspring require further investigation.
Introduction
Thyroid hormones (THs) are essential endocrine hormones during pregnancy and play a key role in fetal development. Maternal THs are the only source of THs for fetuses in the 1st trimester of pregnancy. THs promote the synthesis of proteins, RNA, DNA, and specific enzymes in fetal tissues and cells and are critical for early brain development, somatic growth, and bone maturation. 1,2 Studies have shown that TH levels fluctuate dynamically during pregnancy 3 and subclinical longitudinal changes in TH concentrations during pregnancy are reportedly associated with fetal growth 4 and preterm birth. 5 TH concentrations significantly affect cholesterol and fatty acid metabolism 6,7 as well as glucose metabolism. 8 –10
Abnormal metabolism, including impaired glucose tolerance, impaired fasting glucose, and diabetes, is a common clinical endocrine disorder. Over the past decade, several countries have reported an increase in the prevalence of type 2 diabetes in children and adolescents. 11,12 Glycolipid metabolism status at preschool age is predictive of development of metabolic syndrome later in life. Evidence suggests that children with pediatric metabolic syndrome are more likely to have type 2 diabetes mellitus later in life than their peers are, 13 and this risk increases with metabolic syndrome severity. 14,15 Additionally, studies have shown that lipid and lipoprotein levels in childhood and adolescence can persist into adulthood and are strongly associated with dyslipidemia and cardiovascular diseases in adulthood. 16 Ludvigsson et al. 17 suggested that factors influencing glucose and lipid metabolism in children can be sought in the direction of the nonexternal environment factors.
Studies have shown that adult glucose and lipid metabolism may be programmed during fetal life and changes in the intrauterine environment can have long-term effects on glycolipid metabolism. 18 –20 Research on the associations between maternal TH levels during pregnancy and glucose and lipid metabolism in offspring is limited. Muller et al. 21 reported that mothers with poor thyroid function treated with levothyroxine had offspring with slightly decreased high-density lipoprotein (HDL) levels at 9 years of age compared with those who did not receive the treatment. A study based on a birth cohort from northern Finland revealed that compared with mothers with negative thyroid peroxidase antibody (TPOAb) results, mothers with positive TPOAb results were more than twice as likely to have offspring with metabolic syndrome at 16 years of age. 22 Another study in Hubei, China revealed that elevated serum thyroid-stimulating hormone (TSH) levels within the normal reference range were associated with an increased risk of metabolic diseases in adults. 23 Notably, maternal TH levels are important for offspring development even in the context of normal thyroid function. For example, maternal TSH levels in the upper range of the reference interval have been found to be associated with an increased risk of delivering small-for-gestational-age neonates. 24 Moreover, female offspring born to euthyroid pregnant women with low levels of maternal free thyroxine (fT4) presented better vocabulary acquisition. 25 However, no studies have examined the significance of maternal TH levels on glucose and lipid metabolism in offspring in the context of normal maternal thyroid function.
In summary, research on the associations between variations in maternal TH levels and glycolipid metabolism in offspring is scarce, particularly in women with normal thyroid function during pregnancy. This study aimed to fill this gap by repeatedly measuring maternal TH levels in the 1st, 2nd, and 3rd trimesters of pregnancy to examine the relationships between variations in maternal TH levels and glycolipid metabolism children in the context of normal maternal thyroid function.
Materials and Methods
Participants
In accordance with the Ma’anshan Birth Cohort study in China, pregnant women who had their first antenatal visit at Ma’anshan Maternal and Child Health Hospital were enrolled from May 2013 to September 2014. The inclusion criteria were as follows: (1) having a gestational age of less than 14 weeks; (2) planning to have antenatal checkups and deliver at the hospital; (3) being able to understand and complete the questionnaires; and (4) being willing to participate in follow-up visits during childhood. In total, 3474 pregnant women were recruited. 26
The exclusion criteria for this study were as follows: (1) multiple births; (2) nonlive births; (3) a family history of thyroid diseases or thyroid disorders; (4) missing data on maternal TH levels; (5) TPOAb or thyroglobulin antibody (TGAb) positivity; (6) a TSH or fT4 level in an abnormal range during pregnancy; and (7) missing data on lipid metabolism or glucose metabolism in preschool children. A total of 1130 participants were included in the final analysis (Fig. 1).
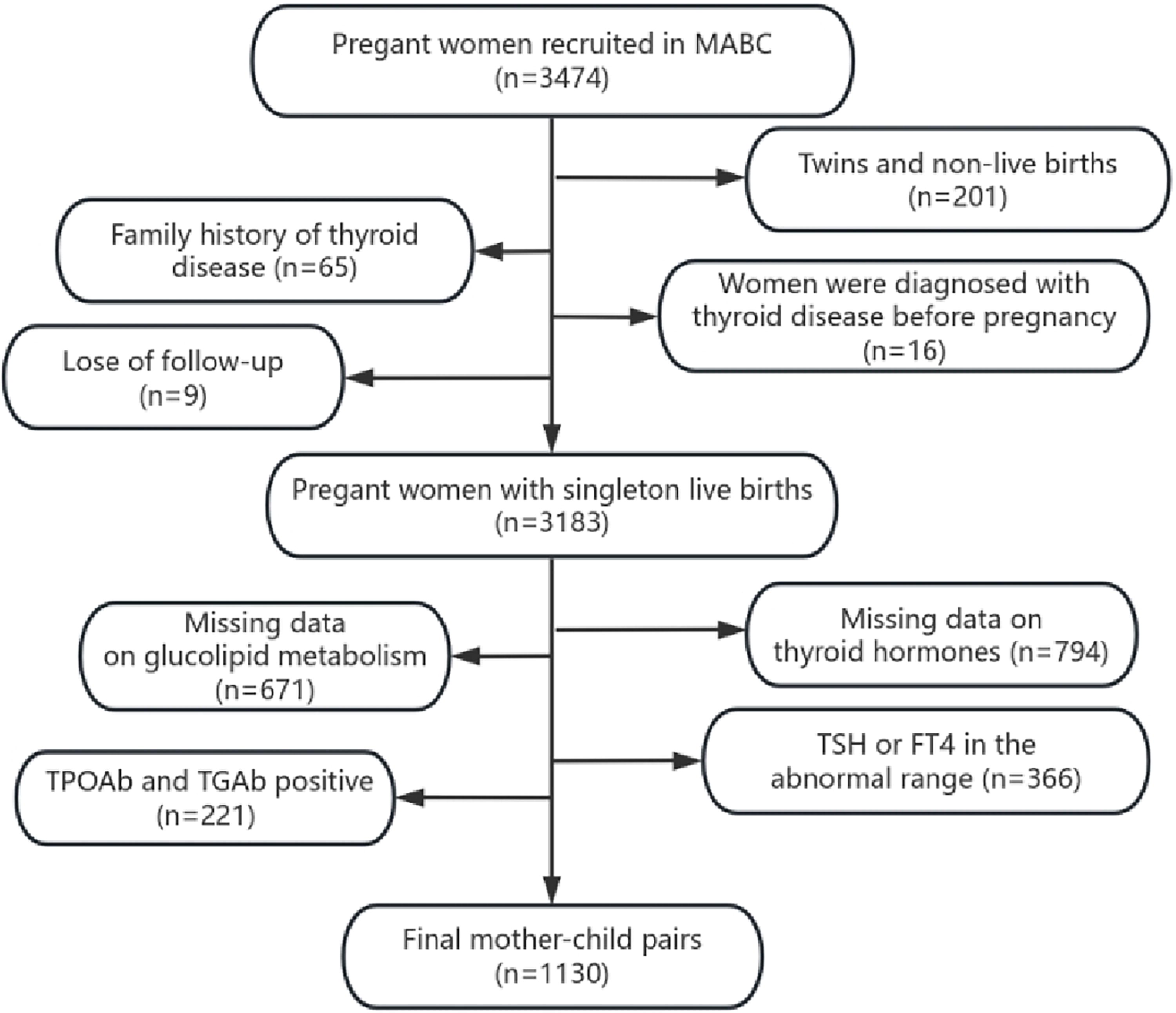
Flow chart of participants. The figure showed the detailed procedure for participants recruitment. A total of 1130 participants entered the final analysis.
All the women provided written informed consent. The study was approved by the ethical committee of Anhui Medical University (No. 20131401).
Maternal thyroid function assessment
Fasting venous blood samples were collected from pregnant women during routine antenatal checkups in the 1st trimester (1–13 weeks), 2nd trimester (14–27 weeks), and 3rd trimester (after 28 weeks) of pregnancy. After centrifugation, the serum was stored in refrigerators at −80°C. During the childhood follow-up period, maternal thyroid function indicators were assessed via electrochemiluminescence immunoassay (Roche Diagnostics GmbH, Mannheim, Germany). The indicators included TSH, total triiodothyronine (TT3), total thyroxine (TT4), free triiodothyronine (fT3), fT4, TPOAb, and TGAb levels.
Normal thyroid function was defined as maternal TSH and fT4 levels within the normal range with negative TPOAb and TGAb results (TPOAb level <34 IU/mL and TGAb level <115 IU/mL). In the present study, the reference ranges of average values for TSH and fT4 levels in the 1st, 2nd, and 3rd trimesters of pregnancy were determined based on previous studies (2.5–97.5th percentile), 27 with a TSH level ranging from 0.04 to 4.90 μIU/mL and an fT4 level ranging from 13.19 to 23.27 pmol/L in the 1st trimester of pregnancy; a TSH level ranging from 0.75 to 6.08 μIU/mL and an fT4 level ranging from 9.14 to 15.32 pmol/L in the 2nd trimester of pregnancy; and a TSH level ranging from 0.58 to 5.59 μIU/mL and an fT4 level ranging from 9.53 to 17.45 pmol/L in the 3rd trimester of pregnancy.
Because TH levels were measured at follow-up during childhood, pregnant women were not treated on the basis of the results of the TH assay in our laboratory. However, one woman was treated with levothyroxine in the 2nd trimester and three women were treated with levothyroxine in the 3rd trimester via routine obstetric examinations.
Evaluation of glucose and lipid metabolism in preschoolers
Fasting venous blood samples were collected from children at the age of 4–6 years. Triglycerides (TG), total cholesterol (TC), HDL, and low-density lipoprotein (LDL) were assayed via a Roche biochemical analyzer (enzyme colorimetric method). Insulin levels were measured via the electrochemiluminescence method and fasting glucose levels were assessed via the glucokinase method. According to the diagnostic criteria for dyslipidemia in children and adolescents over 2 years of age recommended by the “Expert: control of hyperlipid in children and adolescents in China,” 28 TG level ≥1.70 mmol/L indicated hypertriglyceridemia, TC level ≥5.18 mmol/L indicated hypercholesterolemia, LDL level ≥3.37 mmol/L indicated high LDL-C levels, and HDL level <1.04 mmol/L indicated HDL-C levels. If one of these criteria was met, a child was considered to have dyslipidemia. In accordance with “The definition of metabolic syndrome and prophylaxis and treatment proposal in Chinese children and adolescents” 29 from the Pediatrics Branch of the Chinese Medical Association, children with fasting blood glucose level ≥5.60 mmol/L were considered to have abnormal blood glucose.
Covariates
Potential confounders, including maternal age, monthly household income per capita, maternal education, residence, previous adverse pregnancy outcomes, prepregnancy body mass index (BMI), pregnancy complications, smoking during pregnancy, any alcohol consumption during pregnancy, and TPOAb levels during pregnancy, were identified via a directed acyclic graph (Supplementary Fig. S1). Maternal age, maternal education, monthly household income per capita, previous adverse pregnancy outcomes, and maternal smoking and any alcohol consumption during pregnancy were self-reported via a questionnaire survey. Previous adverse pregnancy outcomes included abortion, preterm birth, stillbirth, and birth defects. Women who had any one of the abovementioned conditions were defined as having a history of adverse pregnancy outcomes. Pregnancy complications included hypertensive disorders of pregnancy and gestational diabetes mellitus, and the data were extracted from medical records. Women who had any one of the mentioned conditions were regarded as having pregnancy complications. The women’s height and weight were measured during the first obstetric examination, and BMI was calculated as the prepregnancy BMI. Data on weeks of gestation, birth weight, and child sex were obtained from medical records. Maternal TPOAb and TgAb levels were extracted from thyroid function datasets.
Statistical analyses
EpiData 3.0 was utilized to create the database. SPSS version 23.0 statistical software was used to analyze the data. Mplus was used to fit maternal TT3, TT4, fT3, fT4, and TSH levels in the 1st, 2nd, and 3rd trimesters of pregnancy. Latent category growth models were adopted to group TH levels into different levels. The models were used to identify groups of individuals with similar trajectories over time and the trajectory characteristics of each group were analyzed. The model utilized polynomial methods to analyze variability among different classes of individuals over time and the model parameters were estimated via maximum likelihood estimation. The optimal number of potential category trajectories was determined with reference to the Bayesian information criterion, clinical significance, and outcome interpretability. BIC values closer to 0 and entropy values closer to 1 indicated better model fit. 30,31
Binary logistic regression models were adopted to analyze the associations between maternal TH levels (i.e., maternal TH levels during each trimester and overall TH trajectories during pregnancy) and normal and abnormal glycolipid metabolism in children. These were the primary strategies used in the main analyses. Moreover, linear regression models were used to analyze the associations between continuous variables of maternal TH levels in each trimester of pregnancy and glycolipid metabolism indicators in children. Generalized linear regression models were used to analyze the associations between maternal TH trajectories during pregnancy and glycolipid metabolism indicators in children. These were the secondary strategies used in the main analyses.
Four sensitivity analyses were conducted. First, thyroid function during pregnancy may affect children’s physical development 32 and obesity indicators are risk factors for metabolic disorders. 33,34 Trajectories of children’s BMI at 6, 12, 18, 24, 30, 36, 42, 48, 54, 60, 66, and 72 months of age were fitted (Supplementary Fig. S2) and child BMI was further adjusted for as a mediating variable. Second, abnormal maternal thyroid function is a risk factor for preterm labor and low birth weight, 35,36 which are associated with metabolic disorders later in life. 37 –39 Therefore, gestational week and birth weight may play a mediating role in the associations between maternal TH levels and glucose and lipid metabolism in offspring. Birth weight z scores were thus calculated and further adjusted for. Third, studies have shown that metabolism differs between boys and girls before puberty. 40 Child sex was used as an effect modifier and served as a stratification variable in the sensitivity analysis. Fourth, since high blood glucose levels in children aged 4–6 years are associated primarily with type 1 diabetes, 41,42 we excluded children with abnormal blood glucose levels from the sensitivity analysis.
Results
Distribution of the baseline characteristics of included and excluded participants
The baseline characteristics of the included and excluded participants are shown in Table 1. Compared with the group of pregnant women excluded from the study, the group of pregnant women who were included was younger, had a higher proportion of nulliparous births, had a lower proportion of smokers, and had a lower incidence of pregnancy complications.
Basic Characteristics of Participants by Thyroid Hormone Grouping
Women with gestational hypertension and/or gestational diabetes were defined as having pregnancy complications.
BMI, body mass index.
Grouping for thyroid hormone trajectories
On the basis of the best model fit results combined with clinical significance, we developed a model for the latent category growth of maternal TH levels in three trimesters of pregnancy. As shown in Figure 2, three trajectories were obtained for fT4, T4, and TSH levels, whereas two trajectories were identified for T3 Levels. For fT4, the uppermost curve represented high levels (15.2% of the pregnant women), the middle curve represented intermediate levels (45.6%), and the lowermost curve represented low levels (39.2%). Similar definitions were applied for the T4 and TSH trajectories. For T4, the high-level trajectory accounted for 16.0% of the pregnant women, the intermediate trajectory accounted for 57.6%, and the low trajectory accounted for 26.4%. For TSH, the high-level trajectory accounted for 11.6% of the pregnant women, the intermediate trajectory accounted for 50.9%, and the low trajectory accounted for 39.2%. For T3, the upper trajectory represented a high level (40.2%), whereas the lower trajectory represented a low level (59.8%).
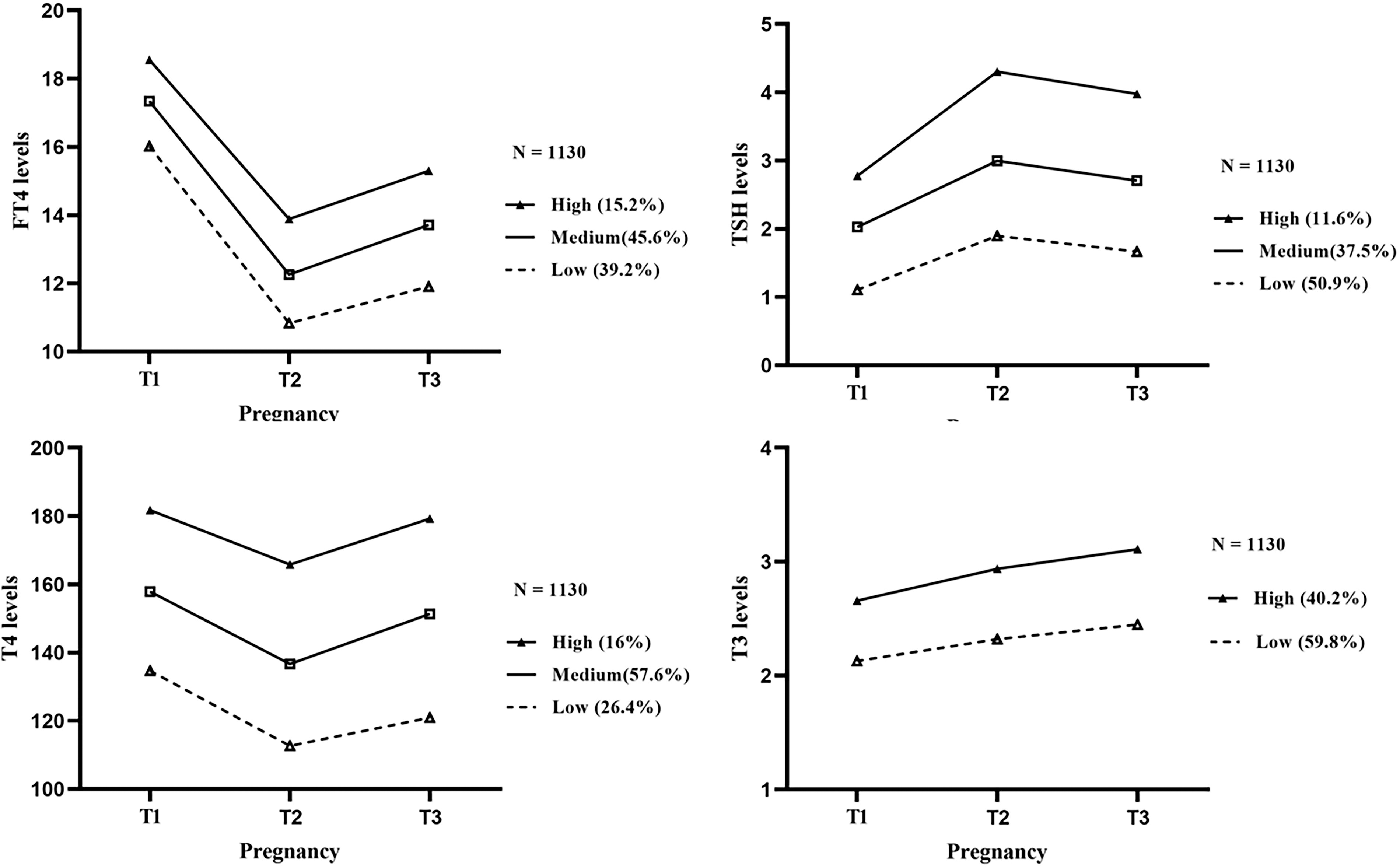
Maternal TH trajectories grouping during pregnancy. It showed the TH trajectories in women throughout pregnancy. Three trajectories were obtained for fT4, T4, and TSH, and two trajectories were obtained for T3. Among three trajectories, the uppermost curve represented high levels, the middle curve represented intermediate levels, and the lowermost curve represented low levels. As for two trajectories, the upper trajectory represented high level and the lower trajectory represented low level. fT4, free thyroxine; TH, thyroid hormone; TSH, thyroid-stimulating hormone.
As shown in Figure 2, the TSH trajectories were lowest in the 1st trimester, increased in the 2nd trimester, and slightly decreased in the 3rd trimester. The trajectories for fT4 and T4 showed a decreasing trend in the 1st trimester, followed by an increase after decreasing to the lowest level in the 2nd trimester. The T3 trajectories tended to increase throughout pregnancy.
Associations between maternal thyroid hormone levels and abnormal glycolipid metabolism in preschoolers
Among the children in this study, 130 (11.5%) had abnormal lipid levels and 18 (1.6%) had abnormal blood glucose levels.
The binary logistic regression analysis demonstrated that high levels of fT4 in the 1st trimester of pregnancy may be associated with decreased risk of children’s hypercholesterolemia. For every 1 pmol/L increase in fT4 levels in the 1st trimester of pregnancy, the risk of the offspring’s hypercholesterolemia decreased 13% (OR = 0.870 [CI 0.768–0.986]) (Figs. 3 and 4).
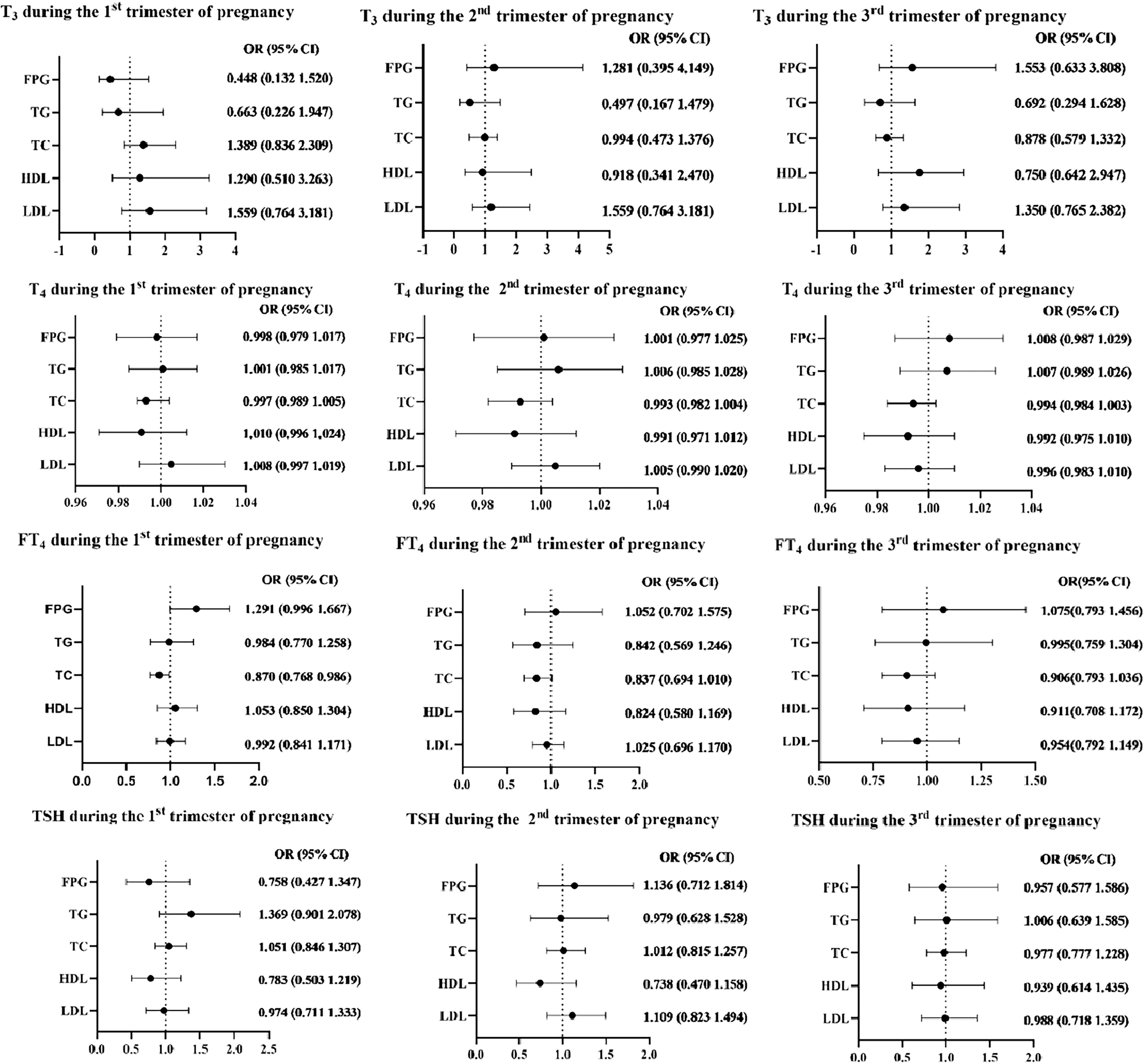
Binary logistic regression models on maternal THs and preschoolers’ glycolipid metabolism in each trimester of pregnancy. Adjusting for maternal age, monthly household income per capita, maternal education, residence, prepregnancy BMI, smoking and alcohol use during pregnancy, and maternal TPOAb. BMI, body mass index; TPOAb, thyroid peroxidase antibody.
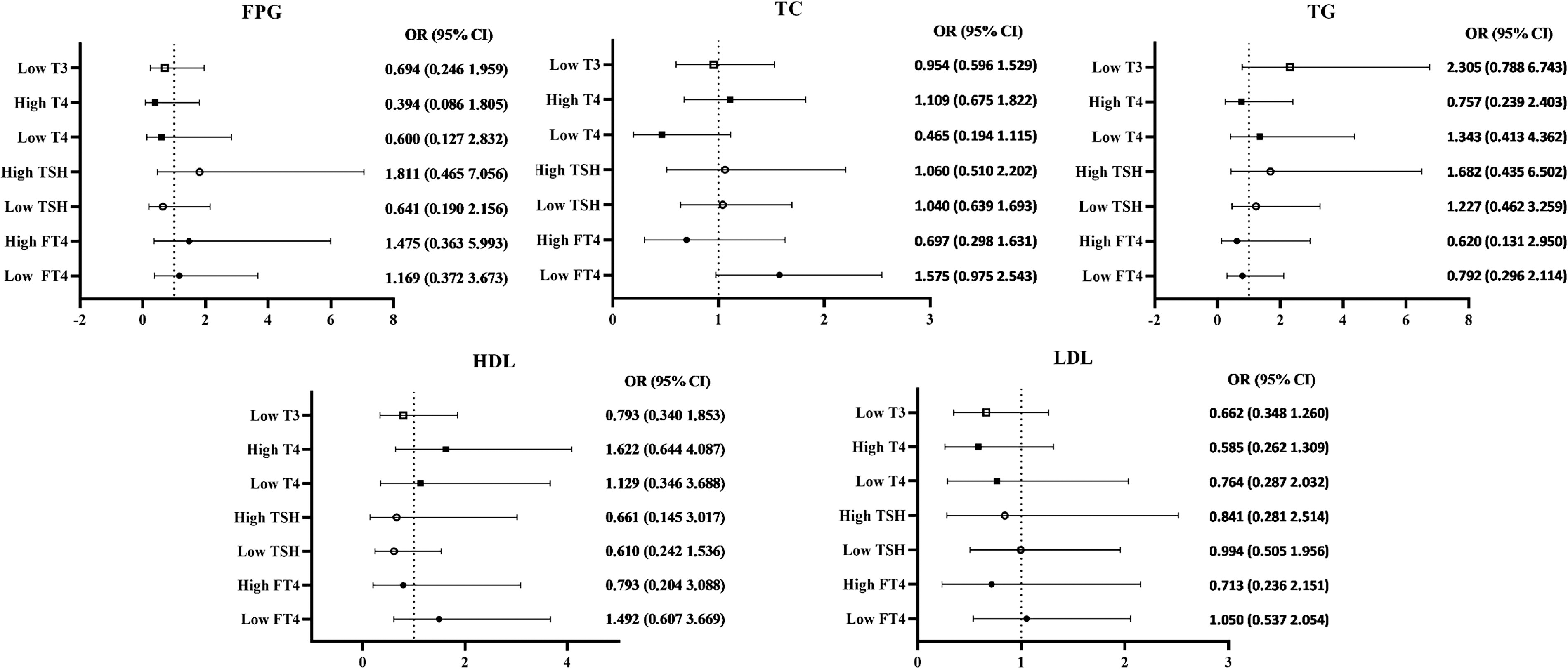
Binary logistic regression models on maternal TH trajectories and preschoolers’ glycolipid metabolism. The medium trajectories of T4, TSH, fT4 were used as reference group, and the high trajectory of T3 was used as reference group. Adjusting for maternal age, monthly household income per capita, maternal education, residence, prepregnancy BMI, smoking and alcohol use during pregnancy, and levels of TPOAb during pregnancy.
Essentially, the sensitivity analyses essentially did not change the main results (Table 2, Supplementary Tables S1, S4, S5, Tables S8, S9, S10, S11, S16, and S17).
Sensitivity Analysis: Binary Logistic Regression Models on Maternal Thyroid Hormones and Preschoolers’ Glycolipid Metabolism in Each Trimester of Pregnancy (Further Adjusting for Offspring Body Mass Index Trajectories)
Adjusting for maternal age, monthly household income per capita, maternal education, residence, previous adverse pregnancy outcomes, prepregnancy BMI, pregnancy complications, smoking during pregnancy, any alcohol consumption during pregnancy, levels of TPOAb during pregnancy, and offspring BMI trajectories.
fT4, free thyroxine; FPG, fasting blood glucose; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TC, total cholesterol; TG, total triglyceride; TSH, thyroid-stimulating hormone.
The bolded part indicates that P < 0.05, and there is a statistically significant difference.
Associations between maternal thyroid hormone levels and glycolipid metabolism indicators in preschoolers
Linear regression models revealed that the maternal T3 concentration in the 1st trimester of pregnancy was positively associated with the fasting glucose concentration in children (β = 0.007 [CI 0.028–0.181]). Maternal fT4 levels in the 1st trimester of pregnancy were positively associated with fasting glucose and insulin concentrations in children (β = 0.022 [CI 0.004–0.040]; β = 0.111 [CI 0.004–0.217]). Maternal T4 levels in the 3rd trimester of pregnancy were negatively associated with LDL levels in children (β = −0.002 [CI −0.003–0.00]) (Fig. 5).
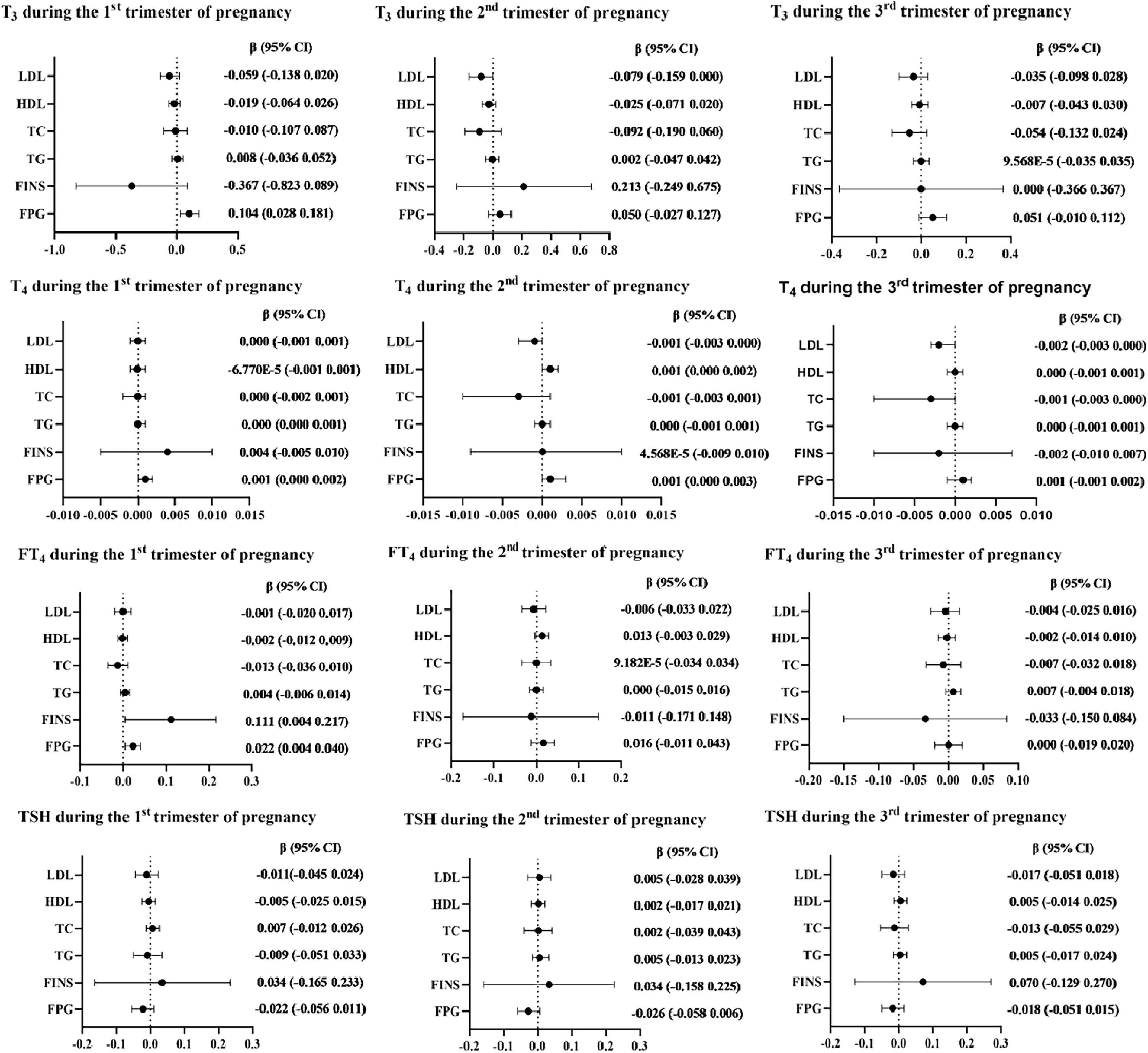
Linear regression models on maternal THs and glycolipid metabolism in preschoolers in each trimester of pregnancy. Continuous levels of maternal THs were used as independent variables, and continuous values of children’s glycolipid metabolism indicators were used as dependent variables in each trimester of pregnancy. Adjusting for maternal age, monthly household income per capita, maternal education, residence, prepregnancy BMI, smoking and alcohol use during pregnancy, and maternal TPOAb.
Generalized linear models revealed that fasting glucose levels were lower in children born to mothers with a medium T4 trajectory than in those with a high trajectory (β = −0.125 [CI −0.221 to −0.030]). Lower fasting glucose concentrations (β = −0.084 [CI −0.152 to −0.016]) and higher LDL concentrations (β = 0.080 [CI 0.009–0.150]) were observed in children born to mothers with low T3 levels than in those born to mothers with high T3 levels. Fasting glucose levels were lower in children born to mothers with a low TSH trajectory than in those born to mothers with a medium trajectory (β= −0.081 [CI −0.152 to −0.009]) (Fig. 6).
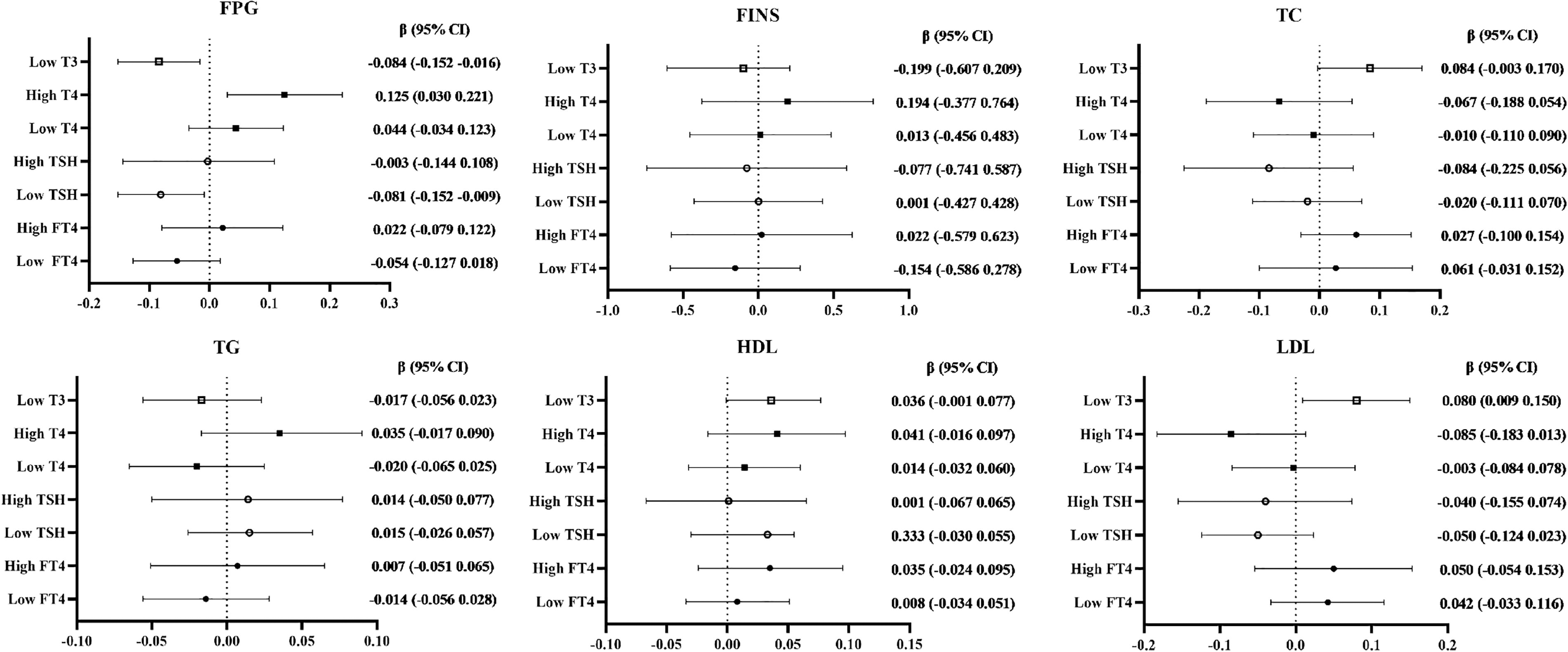
Generalized linear regression models on maternal TH trajectories and preschoolers’ glycolipid metabolism. The medium trajectories of T4, TSH, and fT4 were used as reference group and the high trajectory of T3 was used as reference group. Adjusting for maternal age, monthly household income per capita, maternal education, residence, prepregnancy BMI, smoking and alcohol use during pregnancy, and levels of TPOAb during pregnancy.
Essentially, the sensitivity analyses essentially did not change the main results (Supplementary Tables S2, S3, S6, S7, Tables S12, S13, S14, S15, S18, and S19).
Discussion
In this prospective cohort study, we found that TH levels in mothers with normal thyroid function during pregnancy were associated with fasting glucose, insulin, LDL, and TC concentrations in preschool children.
There is a lack of studies on mothers with normal thyroid function during pregnancy and glycolipid metabolism in offspring. A Chinese cohort study revealed that maternal serum TSH and fT4 levels were associated with various neonatal metabolites, including amino acids and carnitine. 43 Maternal serum fT4 levels may have a positive linear dose—effect relationship with the level of methionine in offspring, which plays a vital role in protein synthesis and cellular energy production in the 1st trimester of pregnancy, suggesting that maternal fT4 levels may influence glycolipid metabolism in offspring in the long term by influencing metabolic profiles in the neonatal period. Carnitine, which contributes to the translocation of long-chain fatty acid coenzyme A into the mitochondria of muscle cells for heat production, may be associated with fatty acid metabolism disorders. 44 However, since the leading indicators in these studies were related to the detection of inborn metabolic disorders and rare diseases, the associations with glycolipid metabolism indicators were more limited, warranting further research.
Experiments in mice revealed that gestational hypothyroidism led to impaired insulin synthesis, reduced pancreatic cell proliferation, glucose intolerance, and increased susceptibility to metabolic stress in offspring. 45,46 T3 is the primary active hormone involved in glucose metabolism. 47 It participates in glucose metabolism in various ways, including promoting pancreatic β-cell proliferation and insulin secretion, 48 positively regulating mitochondrial function, inducing mitochondrial biogenesis, 49 and controlling energy expenditure. Thus, abnormal glucose metabolism in offspring may be caused by an intrauterine hypothyroid environment. Previous studies on thyroid receptors (TRs) have shown that most of the actions of biologically active THs are mediated by TRs. 50,51 The loss of TRs was shown to result in reduced islet density and impaired glucose-stimulated insulin secretion. 52 However, due to the limited studies, it remains unclear whether the effect is cross-generational. Notably, Farahani et al. 53 reported that the offspring whose mothers had hypothyroid during pregnancy would demonstrate impaired glucose tolerance and reduced insulin secretion capability in adulthood, even when the offspring’s thyroid function was normal. This suggests that maternal thyroid function during pregnancy may influence offspring’s glucose metabolism through effects on pancreatic function, potentially resulting in transgenerational impacts. It has been described that a study has shown that reduced LDL receptor (LDLR) activity due to diminished control of sterol regulatory element-binding protein 2 by T3 is the leading cause of hypercholesterolemia in individuals with hypothyroidism, 54 which might explain the increased LDL concentrations in the low-level T3 trajectory group. This association of high LDL concentrations in offspring with the low-level T3 latent class growth model was still observed in mothers with normal thyroid function in the present study. This finding suggests that T3 plays a sensitive role in LDL regulation and that there may be a transgenerational effect.
da Luz et al. 55 reported that high concentrations of T4 lead to increases in LDLR in endothelial cells, which might explain the negative association between maternal T4 levels in the 3rd trimester of pregnancy and LDL levels in preschool children. LDLR plays a significant role in the development of atherosclerosis via endocytosis, allowing cells to absorb cholesterol-dominant lipids and regulate cholesterol homeostasis. 56 Moreover, a Chinese study has revealed that the sensitivity of a multibiomarker model incorporating serum fT4, TG, and LDL-C levels for predicting cardiovascular disease (CVD) risk is significantly greater than that of a model including the single biomarker of fT4. 57 Another study suggested that the increased risk of CVD in patients with hypothyroidism may be due to increased TC, TG, and lipoprotein (a) levels. 58 These findings suggest that in addition to being an essential regulator of cardiac function and cardiovascular hemodynamics, 59 T4 may play a lipid-mediated role in CVD. However, these studies were cross-sectional in design and the cross-generational associations between maternal T4 levels and lipid metabolism in offspring and the underlying mechanisms need to be clarified.
Maternal fT4 concentrations in the 1st trimester of pregnancy were found to be positively associated with fasting glucose and insulin concentrations and high concentrations of fT4 were associated with decreased risk of hypercholesterolemia. THs enhance glucose absorption by increasing gastrointestinal motility, 9 promote liver gluconeogenesis glycogenolysis, and stimulate endogenous glucose production. 60,61 There is no consensus on whether TH concentrations within the physiological range increase the risk of diabetes. Some studies have shown that in individuals with normal thyroid function, the risk of diabetes is correlated with their high-TSH levels and low T3 and fT4 levels. 62 Gu et al. 63 reported that a reduction in fT4 and fT4 levels within the normal range is associated with hyperglycemia and insulin resistance, whereas other scholars have argued that there is a positive correlation between an individual’s own fT4 and fasting blood glucose levels. 64 In terms of lipid metabolism, high fT4 levels in individuals with normal thyroid function are reportedly associated with a reduced risk of developing metabolic syndrome. 65,66 Although the studies mentioned above have not focused on the association between maternal TH levels and glycolipid metabolism in offspring, they may indirectly suggest that high levels of THs may be linked to high glucose levels, which could be interpreted as detrimental. However, they are also associated with fewer hypercholesterolemia, which are beneficial. These glycolipid variations could have different meanings during periods of rapid growth and development.
This study has several advantages. First, to our knowledge, this is the first intergenerational study on maternal TH concentrations in mothers with normal thyroid function during pregnancy and glycolipid metabolism in preschoolers. This study was based on a large-sample, prospective birth cohort that examined TH levels in the 1st, 2nd, and 3rd trimesters of pregnancy. This allowed us to fit the mothers’ TH trajectories, which would better reflect fluctuations in TH levels during pregnancy. Second, this study focused on mothers with normal thyroid function, moving beyond previous studies that focused on pathological states. This suggests that clinicians should also be mindful of high TH levels in women with normal thyroid function during pregnancy. Except for those who received treatment for thyroid function abnormalities detected during routine obstetric examinations, most women did not receive interventions related to thyroid function during pregnancy, as would provide a true, natural course of thyroid function in pregnant women. Third, this study was a prospective cohort study, and in addition to exposure and outcomes, potential confounders were prospectively and accurately collected to reduce recall bias. The further control of multiple precise variables increased the precision and stability of the results.
There are several limitations in this study. First, glycolipid metabolism is influenced by lifestyle, 67 dietary habits, 68 and the external environment. However, such data were lacking in the present study. Therefore, these findings should be interpreted with caution. Second, there are no uniform criteria for determining abnormal glucose metabolism in preschool children, and only the glucose metabolism criteria for children and adolescents are available for classification and analysis. Third, studies have shown an association between iodine intake and metabolic disorders. 66 Iodine nutritional status during pregnancy is significantly associated with thyroid function. 69,70 In this study, maternal iodine levels were not measured, and information on iodine supplementation during pregnancy was not collected. However, all the women in this study had lived in Ma’anshan city for a long period. According to the Ma’anshan Center for Disease Control and Prevention, Ma’anshan city is not an iodine-deficient area, 71 salt iodine fortification has been implemented in China since 1995, 72 which might decrease the potential impact of maternal iodine levels on the association between maternal TH levels and glycolipid metabolism in children to some extent.
Conclusions
This study found an association between maternal thyroxine levels during different trimesters of pregnancy in euthyroid women and glycolipid metabolism in children. In particular, during the 1st trimester of pregnancy, the maternal concentrations of maternal T3 and T4 are positively associated with blood glucose levels in children, whereas high maternal fT4 levels are associated with decreased risk of hypercholesterolemia in children. Maternal T4 concentrations during the 3rd trimester of pregnancy are negatively associated with cholesterol levels in children. High maternal TH levels are associated with high fasting glucose and low LDL concentrations in children. These findings indicate that dynamic variations in maternal TH levels may be associated with glycolipid metabolism in preschoolers, even when women do not have clinically diagnosed thyroid disorders. The exact associations between maternal TH levels in specific trimesters of pregnancy under normal thyroid function conditions and glycolipid metabolism in offspring require further investigation.
Footnotes
Acknowledgments
The authors are grateful to the mothers and children in the study for their active cooperation and would like to thank all the investigators at Ma’anshan Maternal and Child Health Hospital for their assistance and support throughout the study.
Authors’ Contributions
W.C. drafted the work and made substantial contributions to the acquisition, analysis, and interpretation of the data. L.C., M.Z., J.O., and P.W. contributed to the analyses and interpretation of the data. J.T., G.G., S.Y., and F.T. contributed to the study of field organization and coordination, as well as resource acquisition. K.H. was responsible for the conception and design of the work, acquisition of the data, and critical revision of the important intellectual content. All the authors were involved in the review, editing, and final approval of the article.
Author Disclosure Statement
All the authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Funding Information
National Natural Science Foundation of China (82273639)—Kun Huang; The National Key Research and Development Program of China (2022YFC2702901)—Kun Huang; Scientific Research Promotion Project of Anhui Medical University (2023xkjT005)—Kun Huang; Research Fund of Anhui Institute of translational medicine (ZHYX2020A001)—Yunxia Cao; Scientific Research Platform Base Construction Foundation of Anhui Medical University (2023xkjT053)—Yunxia Cao; “Early Scientific Exposure” Training Program of Anhui Medical University (2022-ZQKY-82)—Kun Huang.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
Supplementary Table S10
Supplementary Table S11
Supplementary Table S12
Supplementary Table S13
Supplementary Table S14
Supplementary Table S15
Supplementary Table S16
Supplementary Table S17
Supplementary Table S18
Supplementary Table S19