
Abstract
Background:
Autonomously functioning thyroid nodules (AFTNs) represent ∼5% of all thyroid nodules and often necessitate definitive treatments such as surgery or radioiodine (131I), both of which have inherent risks. Radiofrequency ablation (RFA) has emerged as an effective and safe therapeutic option for managing AFTNs. This study aims to assess the effectiveness and safety of RFA for solitary AFTNs in various countries across Latin America.
Methods:
This retrospective, observational, multicenter cohort study included patients with a solitary AFTN that was histologically confirmed as benign and treated with a single session of RFA. The study included an analysis of patient demographics, sonographic characteristics of the nodules, thyroid profile assessment at each follow-up visit, evaluation of clinical symptoms to determine the achievement of a euthyroid state, and the measurement of nodule volume reduction. In addition, a bivariate analysis was conducted to identify associations between these variables and the resolution of hyperthyroidism.
Results:
Our study enrolled 81 patients with a solitary, benign AFTN. The volume reduction ratio (VRR) consistently increased over the follow-up period, with medians of −50%, −74.9%, −78.4%, and −90.2% at 1, 3, 6, and 12 months, respectively. The rate of resolution of hyperthyroidism was 93.8% (76/81). Following the RFA procedure, 58.02% of patients (47/81) normalized their thyrotropin levels within 1 month of follow-up, and by 3 months, an additional 33.3% had achieved normalization (27/81). Notably, a baseline volume ≥10, 20, or 30 mL did not affect the achievement of clinical success. In bivariate analyses, a VRR ≥50% at the 6-month follow-up was associated with the resolution of hyperthyroidism. Overall complications occurred in 6.2% of patients (5/81), including 1.2% (1/81) of a major complication (transient Horner syndrome), 3.7% cases of transient dysphonia (3/81), and 1.2% (1/81) of hypothyroidism requiring low-dose levothyroxine replacement.
Conclusions:
The results of this multicenter study suggest that RFA is a promising treatment option for patients with solitary AFTN, regardless of their baseline characteristics, including volume, age, or composition. The clinical success of the intervention may be related to the VRR at 6 months.
Introduction
Autonomously functioning thyroid nodules (AFTNs) constitute ∼5% of thyroid nodules, 1 with a reported incidence of 1.6–3.6 cases per 100,000 person-years, 2 making them the second most common cause of hyperthyroidism after Graves’ disease. 3
The commonly used therapeutic modalities are typically definitive, such as surgery or radioiodine 131I (RAI). 4 However, offering surgical procedures for benign nodules is associated with inherent risks, such as hypothyroidism rates of 39.4%, 5 general anesthesia, scarring, and laryngeal nerve lesions. 6 In addition, the use of RAI entails radiation exposure 7 and a risk of permanent hypothyroidism in the context of toxic thyroid nodules, which ranges from 30.8% 8 to 49% when follow-up is conducted during a period of 10 years. 9 Consequently, European guidelines recommend considering thermal ablation (TA) only for young patients with small AFTN to mitigate the risks associated with irradiation and the potential for late-onset hypothyroidism. 10
As a result, radiofrequency ablation (RFA) has emerged as a minimally invasive modality that may obviate the necessity for general anesthesia, incisions, or thyroid gland removal. 11 Medical societies 10,12 –19 have published recommendations for identifying suitable candidates with AFTNs for TA modalities such as RFA. These ablative techniques have demonstrated effectiveness in the management of AFTNs that cause subclinical or overt hyperthyroidism. However, it is essential to note that large AFTNs (>20 mL) may exhibit reduced responsiveness to treatment. 13,14 This leads European guidelines to caution against using TA as a first-line treatment for large AFTNs. 10 Other guidelines suggest that TA is a safe alternative if first-line treatments (surgery/RAI) are contraindicated. 12,15,16,18,20
Adopting a patient-centered approach and recognizing the direct and indirect economic burden of hypothyroidism, which results in total medical costs ranging from $460 to $2555 per patient per year, 21 it is imperative to demonstrate the cost-effectiveness of RFA to establish this procedure as the primary treatment modality for AFTNs. This study aims to assess the effectiveness and safety of RFA for solitary AFTNs in various countries across Latin America.
Methods
The institutional review boards (IRBs) of each of the eight participating institutions approved the study protocol. The institutions involved were as follows: Colombia: Integral Endocrine Surgery Clinic (IRB: 311), Torre Medica Tesoro 2, located in Medellin. Brazil: Núcleo Integrado de Cirurgia de Cabeça e Pescoço in Santa Catarina (IRB: 2024-112); Instituto Amato de Medicina Avanzada (IRB: 234); Instituto de Câncer Dr. Arnaldo (IRB: 106); Clinica Steck, all located in São Paulo (IRB: 135). Ecuador: Institute of Thyroid and Head and Neck Diseases, located in Quito (IRB: 2024-92). Argentina: Hospital Italiano (IRB: 614) Hospital Universitario (IRB: 549), both located in Buenos Aires.
This study complied with the Declaration of Helsinki and the International Conference on Harmonization/Good Clinical Practice Guidelines. All participants were provided with comprehensive information regarding the study’s nature and objectives of the study and provided their informed consent before participating.
Study design
A retrospective, observational, multicenter cohort study of RFA procedures was conducted at eight specialized institutions from December 2022 to August 2024. Specialists in managing thyroid conditions performed RFA procedures, with those in Brazil having experience in RFA since 2018 and specialists from other countries since 2020. Each specialist has conducted between 50 and 100 RFA procedures annually.
Patients
The cohort comprised patients who underwent a single session of RFA for the treatment of benign thyroid nodules known as solitary AFTNs and completed follow-up until August 2024. Follow-up data were collected across the participating institutions at intervals of 1, 3, 6, 12, 18, and 24 months. To be considered for inclusion in the study, the patients fulfilled the following criteria:
Presence of a solitary AFTN: This was assessed through serum thyrotropin (TSH) levels and thyroid scintigraphy. All enrolled patients underwent a complete thyroid profile, which included measurements of TSH, free thyroxine (fT4), total triiodothyronine (tT3) levels, and 99mTcO4
–scintigraphy. The diagnosis of AFTN was based on subnormal TSH levels and the identification of a distinct nodule exhibiting increased radionuclide uptake relative to the surrounding thyroid tissue on 99mTcO4
–scintigraphy.
22
The definition of a pretoxic nodule was derived from complementary fT4 and tT3 levels, indicating subclinical hyperthyroidism (both within normal limits). Confirmation of benign thyroid nodule through one fine-needle aspiration (FNA) Absence of suspicious features on ultrasound Completion of at least two follow-up assessments, with one occurring 6 months post-procedure. Refusal or contraindications for surgery or RAI therapy.
Variables and sources of information
Patient variables were recorded, including age, gender, antithyroid medication consumption, and sonographic characteristics of the nodule, such as size, location, composition, and volume. The nodule volume was calculated using the formula: V = πabc/6, where V represents the volume, and a denotes the largest diameter, while b and c correspond to the other two perpendicular diameters. 23 In addition, thyroid function assessments were conducted, including tests for TSH, fT4, and tT3 levels before the ablation procedure and during follow-up. The total energy delivered during the procedure was documented when available.
The reference ranges for TSH levels were 0.27–5.33 mIU/L, for fT4 were 0.7–1.8 ng/dL, and for tT3 were 35–193 ng/dL, with all measurements performed using chemiluminescence.
Supplementary Table S1 details the reference ranges according to the participating institution.
Definitions
The results described were defined in accordance with international guidelines for the assessment of clinical success (specifically for toxic nodules) and safety concerning TA in general. 23 –25 Technique efficacy was evaluated through the volume reduction ratio (VRR), which quantifies the reduction in nodule volume as a percentage of the baseline volume following ablation treatment. It was calculated using the formula ([initial volume − post-ablation volume] / initial volume) × 10023. Solid nodules were classified as such if the cystic component constituted <10% of the nodule, cystic if the fluid component accounted for >90%, and mixed if the fluid component fell within 11–90%.
Clinical success was defined as the normalization of serum thyroid hormones and TSH, along with the suspension of oral antithyroid therapy during follow-up. 23
The total delivered energy was calculated in kilocalories by the generator and then converted to joules per milliliter by multiplying by 4184 and dividing by the nodule volume in milliliters.
The primary outcome was clinical success, while the secondary outcomes included technique efficacy, defined as a VRR of at least 80% 23 at 6 months, and adverse events related to the procedure, which were also defined according to international guidelines. 23 –25
Procedural details
Typical procedural settings varied between institutions. RFA procedures were performed under anesthesia care sedation, accompanied by a local lidocaine ultrasound-guided injection for thyroid capsular anesthesia. In cases where the thyroid nodules showed a mixed composition of solid and fluid components, an initial aspiration of the primary fluid component was performed to identify predominantly solid lesions. The RFA procedures utilized either the STARmed system manufactured by Taewoong in Seoul, Korea, or the Rf Medical Co Ltd (Geumcheon-gu, Seoul, Korea), with an internally cooled, straight-type electrode with a 7-mm or 1.0 cm active tip. The procedure employed the ultrasound-guided trans-isthmic method, utilizing the “moving-shot” technique, according to the most recent international guidelines. 17,18 A 25–50 W power range was applied during the procedure, and the impedance was closely monitored to prevent tissue carbonization. To ensure the safety of the adjacent anatomical components, including the trachea, carotid sheath, and laryngeal nerves, a hydrodissection technique was performed using a solution containing 5% dextrose. The ablation procedure was performed until hyperechoic zones were observed throughout the entire nodule, indicating that the treatment had induced changes. The patients were discharged after an observation period of 20–30 minutes.
Patients were evaluated at each visit for primary and secondary outcomes, including any adverse events. However, no telephone interviews were conducted with patients. The entire cohort had access to their physician via email or messaging to report any concerns or adverse events at times other than the control visits (the first and second visits primarily occurred during the first 3 months). Patients were given clear instructions to contact their physician if they developed any symptoms or had questions following the RFA session, and all patients were capable of communicating via email or phone.
Statistical analyses
Continuous variables were reported as mean or median, depending on the normality of their distribution, which was assessed using the Shapiro–Wilk test. Categorical variables are described using absolute frequencies and percentages. The Mann–Whitney U test or Wilcoxon signed-rank test was used to compare continuous variables based on the nature of the data. For categorical variables, comparisons were made using the chi-squared or Fisher’s exact test, as appropriate. We conducted a bivariate analysis to identify associations between clinical, ultrasonographic, and electrical variables and the resolution of hyperthyroidism. A level of statistical significance of α = 0.05 was established a priori. Statistical analyses were performed using Stata® version 12 (Stata Corp).
Results
Patients characteristics
A total of 81 patients with a solitary, benign AFTN were included in this study (Fig. 1). Notably, only 2 patients presented with a pretoxic AFTN, while the remaining (79) had toxic nodules. The median age of the study cohort was 44 years (range: 13–88 years), with 69 females (85.2%). Most of the nodules were solid (74.1%), with a median thyroid nodule volume of 6.8 mL (range: 0.5–60 mL). The median duration of active ablation was 5.7 minutes, accompanied by a median energy of 2.11 Kcal (8828.24 J), and a median follow-up period of 6 months (interquartile range [IQR]: 6–12 months) (Table 1).
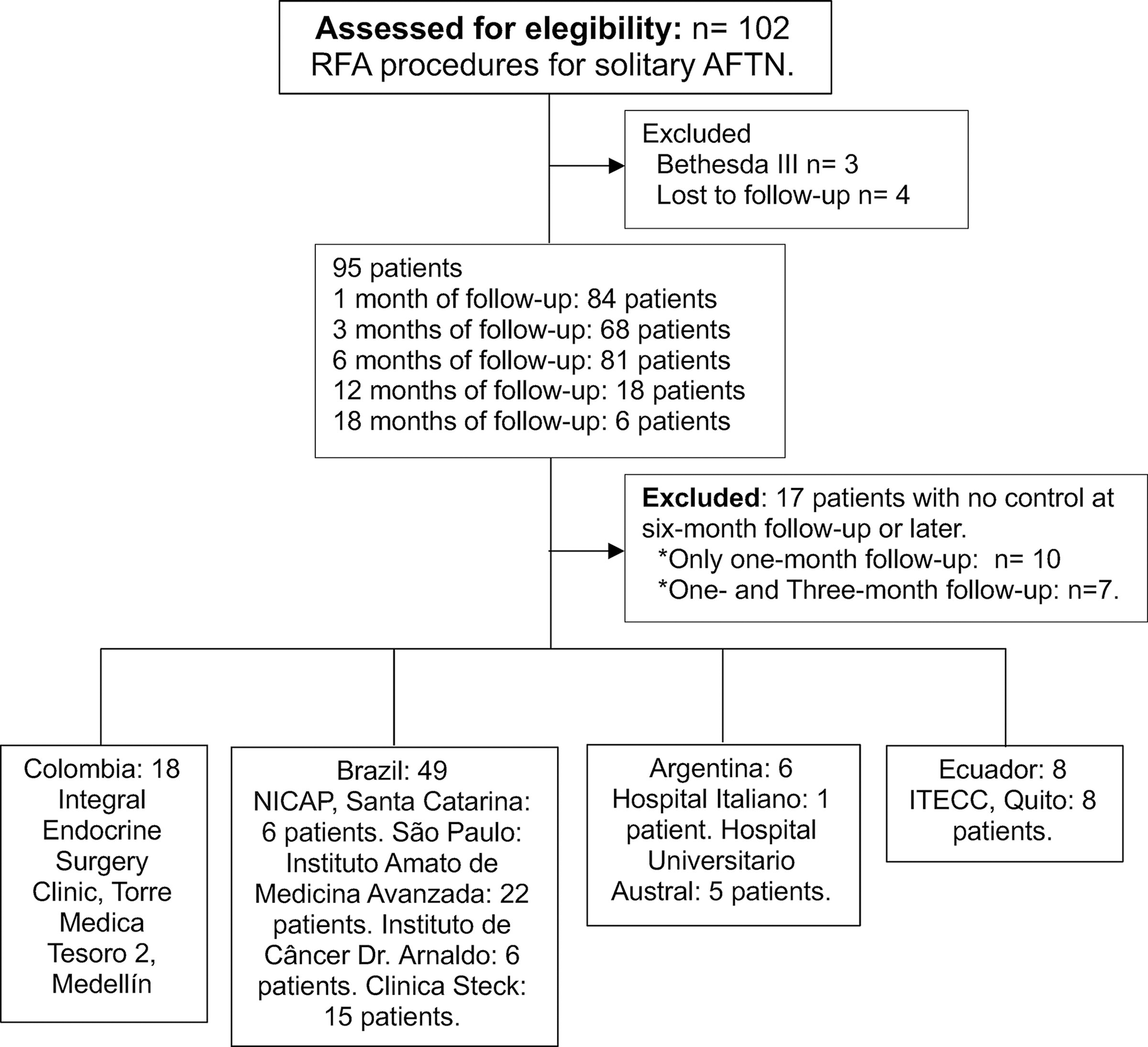
Patient flowchart. ITECC, Institute of Thyroid and Head and Neck Diseases; NICAP, Núcleo Integrado de Cirurgia de Cabeça e Pescoço.
Characteristics of Patients with Solitary AFTNs and Radiofrequency Treatment
AFTNs, autonomously functioning thyroid nodules; fT4, free thyroxine; IQR, interquartile range; TSH, thyrotropin; tT3, total triiodothyronine; SD, standard deviation.
All patients underwent FNA confirming the benign nature of their nodules. These patients did not exhibit any suspicious ultrasound features.
Changes in thyroid profile levels and VRR during follow-up
The median TSH level at baseline was 0.05 (IQR: 0.002–0.136), with a range from 0.00 to 0.32. At diagnosis, all patients exhibited suppressed TSH levels; however, prior to the RFA procedure, only 59.3% maintained suppressed TSH levels. Almost all patients (96.3%) were on methimazole before the procedure, with the exception of three patients: one female seeking pregnancy and two with subclinical hyperthyroidism. The normal TSH range across participating institutions varied from 0.27 to 5.33 mIU/mL, with all normal values detailed in the Methods section.
The thyroid profile was measured during each follow-up assessment, including mainly TSH and fT4. tT3 was available for most, but not all, patients during these assessments, as specified in Table 2. Within the cohort, the median levels of TSH, fT4, and tT3 normalized over the follow-up periods, considering that antithyroid drugs were deprescribed on the same day as the RFA session. In addition, the VRR showed consistency, culminating in a plateau at the 18-month follow-up (Table 2 and Fig. 2). The technique efficacy was achieved in 36 patients (44.4%) at 6 months.

VRR during follow-up. VRR1: Follow-up at 1 month. VRR2: Follow-up at 3 months. VRR3: Follow-up at 6 months. VRR4: Follow-up at 1 year. VRR, volume reduction ratio.
VRR and Thyroid Profile Levels During Follow-up
Every patient was deprescribed antithyroid drugs the same day as the RFA session.
RFA, radiofrequency ablation; VRR, volume reduction ratio.
Following the RFA procedure, 58.02% (47/81) of patients normalized their TSH levels by 1 month of follow-up. By 3 months, an additional 33.3% (27/81) had achieved normalization. In addition, 2.5% of patients reached normal TSH levels by 6 months (1/81), and 1.23% of patients did so by the 12-month follow-up (1/81). The remaining 6.2% of patients did not achieve TSH normalization after the procedure (5/81).
Larger nodules
The median VRR for nodules ≥30 mL compared with <30 mL was as follows: at 1 month, 54.7% (IQR: 36.1–80.5) versus 50% (IQR: 38.6–61), p = 0.6805; at 3 months, 68.3% (IQR: 53.5–88.9) versus 74.9% (IQR: 57.2–82.2), p = 0.9132; at six months, 68 (IQR: 64–91.8) versus 78.4 (IQR: 67.7–88.1), p = 0.6439; at 12 months, 85.5 (IQR: 56.6–90.9) versus 90–3 (IQR: 82.2–94.4), p = 0.2880. There was no significant difference in the median VRR at 1, 3, 6, and 12 months based on the baseline nodule volume of ≥30 mL, nor were there differences in the achievement of clinical success at 6 months (nodules ≥30 mL: 100% vs. <30 mL: 93.2%) (Supplementary Table S2).
Clinical success
The rate of resolution of hyperthyroidism was 93.8% (76/81) in the overall cohort of patients and 100% in those with pretoxic nodules. Five patients did not achieve TSH levels’ normalization. Among these, two are currently receiving antithyroid medication (methimazole). In addition, two patients who initially normalized their thyroid profiles later experienced suppression again: one resumed methimazole treatment at the 6-month follow-up, while the other tested positive for thyroid peroxidase antibodies, with a normal 99mTcO4 –scintigraphy suggesting possible thyroiditis. Three patients continued to exhibit suppressed TSH levels, and they are under observation, with follow-up assessments completed at 6 months (one patient), 1 year (one patient), and 18 months (one patient), all of whom had normalized fT4 and tT3 levels. The patient with persistently suppressed TSH levels at the 18-month follow-up demonstrated a VRR of −87.8% and the following laboratory values: TSH: 0.03 mIU/L; tT3: 99 ng/dL (60–180 ng/dL); and fT4: 0.81 ng/dL (0.8–1.8 ng/dL), in addition to a normal 99mTcO4 –scintigraphy.
The clinical success rates at each follow-up period were 58.02% (47/81) at 1 month, 33.3% (27/81) at 3 months, and 1.2% at both 6 and 12 months (1/81).
Features associated with the clinical success of RFA in solitary AFTN
Various demographic variables, including age and sex, and ultrasound characteristics, such as baseline volume (≥10, 20, or 30 mL with p-values of 0.146, 0.414, and 0.478, respectively) and solid composition (p = 0.700), did not impact the achievement of hyperthyroidism resolution. Bivariate analyses showed that a VRR ≥50% at 6 months was significantly correlated with the resolution of hyperthyroidism in 93.4% of patients (71/76), p = 0.01. In addition, the energy delivered ≥2100 J/mL was not correlated with hyperthyroidism resolution, a finding that remained consistent regardless of the threshold used (Table 3).
Subgroup Classification of the Resolution of Hyperthyroidism at 6 Months
Resolution of hyperthyroidism was defined as the normalization of serum thyroid hormones and TSH, along with the suspension of oral antithyroid therapy during follow-up. 23
Mann–Whitney U test.
Adverse events related to the procedure
The safety profile of the procedure was notably favorable. The overall complication rate was 6.2% (five patients). Specifically, one patient (1.2%) experienced a major complication (type C), 23 –25 characterized by Horner syndrome, which lasted for 8 months; the patient has since fully recovered. In addition, three patients reported transient dysphonia (a minor complication), with two achieving voice normalization within 1 month and the third at 6 months. Furthermore, one patient developed persistent hypothyroidism and is currently receiving low-dose levothyroxine (25 mcg) as part of her treatment regimen with normalized TSH levels. This patient had a history of lobectomy 30 years ago for benign pathology, with negative thyroid peroxidase and thyroglobulin antibodies. It is also worth noting that two patients experienced mild elevations in their TSH levels, which normalized at 3 and 12 months of follow-up without requiring treatment.
Discussion
This multicenter study demonstrated that RFA as a therapeutic option could be effective and exhibits a favorable safety profile for patients with solitary AFTN across diverse regions in Latin America. The median age of our patient cohort is consistent with previously reported ranges, which fall between 41.4 26 and 69.1 years old. 27 Similarly, our observation of a female predominance aligns with findings from prior RFA studies on AFTN, reflecting the gender distribution commonly documented in the literature. 4,7,26 –33 Furthermore, the median baseline nodule volume in our study was comparable with published data, which typically ranges from 5.4 to 22.5 mL. 4 The safety profile observed in our research also corresponds with those reported in various series and reviews, 3 thus reaffirming the favorable safety outcomes associated with RFA for solitary AFTN.
The volume at baseline has been identified as a factor associated with treatment success in previous studies, 1,26,34 and guidelines 13,14 often recommend a volume <20 mL when considering RFA as a suitable option. In contrast to the findings from the systematic review by Kim et al., 1 the prospective study by Cesareo, 26 and the retrospective multicenter study by Mauri et al., 34 which reported a higher rate of TSH normalization in smaller nodules, our study observed that all patients with a baseline volume exceeding 10, 20, or even 30 mL achieved normalization of their thyroid hormone levels. This suggests that patients with larger nodules may benefit from considering RFA as a viable therapeutic option. The discrepancy in findings may be attributed to the significantly higher volume reduction observed in smaller nodules in previous studies. 26 In contrast, in our results, the VRR was similar in both groups (≥20 mL vs. <20 mL).
VRR ≥80% has been acknowledged as an essential factor associated with therapeutic success. 35 However, our study found that this threshold at 6 months was not linked to clinical success, possibly due to the limited number of patients achieving technique efficacy within this period. In contrast, a VRR threshold of ≥50% was statistically significant, underscoring the significance of attaining greater volume reduction to ensure therapeutic effectiveness. Notably, the 81 patients who completed the 6-month follow-up presented a median VRR of 78.4%, surpassing the mean VRR reported in various series and reviews. 1,36 –39 This observation may explain the higher rate of hyperthyroidism resolution observed in our patient cohort, reaching 93.8%, exceeding the range of 23.8% 4 to 90.9% 7 reported in the literature reviews. The notable variability in effectiveness across studies could be ascribed to the technical methodologies employed, with the fixed electrode technique contrasting with the currently accepted approach, namely the moving shot technique.
In our study five patients did not achieve clinical success; three of these patients completed 6 months of follow-up, one completed a year, and one completed 18 months of follow-up. While most patients in our study achieved symptom normalization and restoration of thyroid profile levels at 1 and 3 months of follow-up, some patients attained this normalization at 6 and 12 months. This trend was also observed in a study conducted by Mauri et al. 34 showing a gradual increase in the withdrawal of antithyroid therapy throughout the follow-up period, rising from 32.5% at 2 months to 41.3% at 12 months. These findings suggest that the clinical success of treatment may be more pronounced during long-term follow-up.
It has been suggested that higher energy delivery is linked to enhanced effectiveness in resolving hyperthyroidism when the delivered energy exceeds 2.1 kJ/mL. 40 In our bivariate analyses, we did not observe any differences regardless of the threshold employed. However, it is essential to acknowledge that complete data for this variable were only available for a subset of the cohort, and only three out of the five patients with unresolved hyperthyroidism had complete information for this variable. Notably, two of these patients are not currently receiving methimazole and have normalized levels of fT4 and tT3, as well as normal 99mTcO4 –scintigraphy results. This phenomenon, which simulates subclinical hyperthyroidism, may indicate a delayed normalization of TSH levels, a pattern also observed following thyroidectomy for Graves’ disease. 41
The primary limitation of the current study is its retrospective nature, which precludes the establishment of definitive conclusions regarding associations and results in some loss of data, particularly concerning electrical parameters such as delivered energy, thereby limiting conclusions related to this information, in addition to the absence of a control group and a multivariable analysis to adjust for confounders. In addition, the study population did not encompass individuals with multifocal AFTN or thyrotoxicosis in the form of goiter, which has been noted to be less responsive to RFA. In addition, the follow-up period was insufficient to analyze the recurrence rate of thyrotoxicosis due to nodule regrowth. This condition may develop with a median follow-up of 4 years and has been reported to occur even up to 10 years, as described in a recently published long-term follow-up study. 42 Nonetheless, the data presented herein bolster the evidence supporting the safety and efficacy of RFA for solitary AFTN across South American countries. These findings may facilitate the adoption of RFA as a leading therapeutic approach.
Furthermore, it is important to note that this procedure is not universally covered by public health insurance. Consequently, some patients in this study had to pay out of pocket, with costs varying by country and ranging from $2000 to $5500 USD, unless they were participating in a research project or had private insurance that would cover the expenses. This situation underscores the necessity of conducting cost-effectiveness studies in our countries to better identify the patients who would benefit the most from these therapeutic options.
In summary, this multicenter study indicates that RFA could be an effective and safe treatment modality for patients with solitary AFTN, irrespective of baseline volume, age, or composition. The success of the intervention may be linked to achieving a VRR ≥50% at the 6-month mark. These findings provide substantial evidence to support RFA as a viable treatment option for solitary AFTN patients.
Footnotes
Acknowledgments
The authors express their gratitude to the American Thyroid Association meeting for presenting this work as an abstract poster (ID 0257) on October 31, 2024, in Chicago, IL. They also thank the Department of Epidemiology at CES University College of Medicine for their statistical support, as well as to every participating institution.
Authors’ Contributions
J.P.D.: Conceptualization, methodology, supervision, writing, editing, investigation, review, and RFA treatment performance. N.B.-G.: Investigation, data curation, methodology, review, writing, and formal analysis. A.R., J.H.S., C.G., R.D.C., L.G.R., A.V., L.S., and E.M.V.: Conceptualization, RFA treatment performance, data curation, editing, and review.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.
Supplementary Material
Supplementary Table S1
Supplementary Table S2