
Abstract
Background:
This study assessed the efficacy and safety of ultrasound (US)-guided radiofrequency ablation (RFA) for treatment of skin-involving recurrent thyroid cancer.
Methods:
In this retrospective case series study, 43 patients (mean age: 67.9 ± 14.4 years; 31 females) with skin-involving recurrent thyroid cancer were treated with RFA for a total of 50 tumors between May 2008 and March 2023. The location of the tumor was classified into epidermis, dermis, or hypodermis on the basis of the involved skin layer. After RFA, the technique efficacy (absence of detectable vasculature and volume reduction at 12 months), clinical success (resolution of symptoms or cosmetic problems), volume reduction ratio (VRR), complete disappearance of tumor, and complications were assessed.
Results:
Of the 50 recurrent tumors, 9 involved the epidermis, 10 involved the dermis, and 31 involved the hypodermis. A total of 88 RFA sessions (mean, 1.8; range: 1–6) were performed. The technique efficacy at 1 year was 72% (36/50 [confidence interval or CI: 59.6–84.4%]). At the last follow-up (median [interquartile range]: 2.7 [1.1–4.5] years), the clinical success rate was 86% (44/50), the complete disappearance rate 54% (27/50), and the mean VRR 77.3% ± 44.2%. In a subgroup analysis comparing epidermis/dermis vs. hypodermis, there was no statistical difference in technique efficacy (57.9% [11/19] vs. 80.6% [25/31], p = 0.085), clinical success rate (78.9% [15/19] vs. 90.3% [28/31], p = 0.265), complete disappearance rate (42.1% [8/19] vs. 51.6% [16/31], p = 0.541), or mean VRR (65.5% vs. 84.6%, p = 0.141). Skin burns were observed in 4.9% per treatment session (2/41 [CI: 0–11.3%]) of epidermis/dermis-involving tumor procedures and none of the hypodermal tumor procedures. No patients experienced life-threatening or major complications.
Conclusions:
RFA might serve as a promising approach for managing skin-involving recurrent thyroid cancer, with no major complications reported in this preliminary study. Recurrent tumors involving the epidermis/dermis may pose a higher risk of skin burns than tumors involving the hypodermis. Early intervention with RFA before the tumor extends to the epidermis/dermis may thus be preferable.
Introduction
Thyroid cancer is the most common type of endocrine cancer and generally has a relatively good prognosis. 1 However, it frequently metastasizes and recurs locally. 2 The standard treatment for recurrent thyroid cancer is reoperation followed by radioactive iodine therapy. 3 However, reoperation poses challenges due to tissue plane distortion and fibrosis from scar tissue formation, increasing the risk of complications. 4,5 Additionally, it can be difficult to pinpoint small recurrences without ultrasound (US) guidance. 6 Recently, US-guided radiofrequency ablation (RFA) has emerged as a promising treatment option for recurrent thyroid cancer, offering both curative and palliative benefits, especially for patients at high surgical risk or those who refuse repeated surgery. 7 A meta-analysis on the efficacy and safety of RFA for locally recurrent thyroid cancer reported treatment success rates ranging from 89.5% to 100%, with a complete disappearance rate of 68.8%. 8
Although skin involvement in recurrent thyroid cancer is rare, 9 –11 it can lead to significant cosmetic and symptomatic issues such as skin necrosis, bleeding, and pain, severely impacting the patient’s quality of life. A previous review article suggested RFA as a treatment option to control these problems 12 ; however, there is a potential risk of skin burns when RFA is used to treat tumors involving the skin. To prevent complications from the use of RFA for treatment of skin-involving thyroid cancers, Lee et al. stressed the value of the hydrodissection technique and knowledge of skin anatomy (i.e., three skin layers: epidermis, dermis, and hypodermis). 12 Addressing recurrent cancer with skin involvement poses distinct challenges, and to our knowledge, no original study has yet evaluated the efficacy and safety of RFA in this context.
Therefore, this study assessed the efficacy and safety of RFA for the control of skin-involving recurrent thyroid cancer and explored associations between the involved skin layer and treatment outcomes.
Methods
This retrospective case series study was approved by our institutional review board (No. S2024-0357), which waived the requirement for informed patient consent. Written informed consent for RFA was obtained from all patients before the procedure.
We retrospectively reviewed the medical records of patients who underwent RFA for skin-involving recurrent thyroid cancer after thyroidectomy between May 2008 and March 2023. The inclusion criteria were: (1) patients with skin-involving recurrent thyroid cancer confirmed by fine-needle aspiration or core-needle biopsy; (2) those who refused or were ineligible for surgery; and (3) a follow-up period of more than 6 months. Among 55 skin-involving recurrent tumors treated with RFA in 48 patients, 5 patients were excluded because of an insufficient follow-up period. Finally, a total of 50 recurrent tumors in 43 patients were included. A flow diagram of patient selection is shown in Figure 1.
Flow diagram of patient selection.
Pre-ablation assessment
Before the RFA procedure, the patients were asked about the presence of symptoms and a cosmetic grading score was assessed by the physician (1, no palpable mass; 2, no cosmetic problem but a palpable mass; 3, a cosmetic problem on swallowing only; and 4, an easily detected cosmetic problem). 13,14 The size, volume, location, composition, and vascularity of each recurrent tumor were evaluated by US examination. The three orthogonal diameters of each tumor (i.e., its largest diameter and two other perpendicular diameters) were measured, and the volume of each tumor was calculated as V = πabc/6 (where V is the volume, a is the largest diameter, and b and c are the two perpendicular diameters). 15 The location of the tumor was classified into epidermis, dermis, or hypodermis on the basis of the involved skin layer, determined by the tumor’s central location. In the US evaluation, the epidermis appears as a hyperechoic line, the dermis as a hyperechoic band, and the hypodermis as a hypoechoic layer 16 (Supplementary Fig. S1). All patient medical records and US images were reviewed by one radiologist (H.H.M.) with 7 years of clinical experience in thyroid imaging.
RFA procedure
US-guided RFA was performed by one of three experienced radiologists (J.H.B., J.H.L, and S.R.C., with 26, 20, and 7 years of experience in RFA, respectively). A radiofrequency generator (Cool-Tip RF system, Radionics, Burlington, MA, USA; SSP-2000, Taewoong Medical, Gyeonggi, Korea; VIVA RF system, STARmed, Goyang, Korea) and an 18- or 19-gauge internally cooled electrode with a 0.7–1.5 cm active tip (Cool-Tip, Radionics; Well-point RF electrode, STARmed; VIVA, STARmed) were used, depending on the size and location of the targeted tumor. The patients were treated with 1% lidocaine for local anesthesia at the puncture site and around the tumor. The skin puncture site for local anesthesia was 3–4 cm away from the tumor, so as not to puncture the tumor directly. RFA was started at the point of the feeding artery, with the electrode tip positioned in the deepest most remote portion of the lesion. The treatment was then gradually moved anteriorly using the moving shot technique, according to the Korean thyroid RFA guidelines. 7 When tumors presented with a considerable amount of hemorrhagic fluid, it was aspirated after ablation of hypervascular tumor and feeding vessels. To prevent skin necrosis, electrode puncture was performed on normal skin instead of directly puncturing the tumor. To prevent skin burns, hydrodissection with a 5% dextrose solution was performed between the tumor and epidermis. The tumor and surrounding normal tissue were ablated together to prevent marginal recurrence. During the ablation, frequent checks were made on the patient’s voice and pain level. The power was reduced or turned off for several seconds if a patient could not tolerate the pain during ablation. After the ablation, each patient was observed for 1–2 hours in the hospital, during which time any complications occurring immediately after ablation were carefully evaluated according to their clinical signs and symptoms.
Post-ablation assessment
Patients were followed-up using US and clinical evaluation at 1, 3, 6, and 12 months and then every 6 to 12 months thereafter. Tumor size, volume, vascularity, development of new metastatic tumors, cosmetic score, and presence of symptoms were evaluated during the follow-up period in the same manner as before the ablation. If necessary, a contrast-enhanced thyroid computed tomography (CT) protocol was performed to evaluate viable tumor. Additional RFA was performed if patients complained of unresolved symptoms or cosmetic problems or an undertreated tumor area was found to be growing during follow-up. Residual unablated tumor refers to incomplete RFA sessions resulting in observation of a remnant tumor either immediately post-RFA or during initial follow-up imaging, with this being characterized by increased vascularity on advanced Doppler imaging or enhancement on thyroid-protocol CT scan. 13 Technique efficacy was assessed at 12 months post-RFA using both conventional grayscale US and advanced Doppler imaging techniques, along with thyroid CT protocol. Technique efficacy was defined according to the absence of detection of vasculature (or no enhancement) and a volume reduction (or disappearance) of the index tumor on both imaging modalities. 17 –19 For patients who received multiple RFA treatments, technique efficacy was evaluated 1 year after the final RFA. Clinical success was defined as the resolution of symptoms or cosmetic problems. 13,20 The percentage reduction in volume was calculated as the volume reduction ratio (VRR) = ([initial volume — final volume] × 100)/initial volume. 15
Complications during follow-up were assessed using the reporting standards of the Society of Interventional Radiology. 21,22
The primary outcome of our study is the complete disappearance of the recurrent tumor. Secondary outcomes include clinical success and any complications.
Statistical analysis
Comparisons of tumor characteristics treated with single and multiple RFA sessions were made using chi-square tests or Fisher’s exact test for categorical variables and two-sample t-tests for continuous variables. Treatment outcomes, such as changes in tumor diameter, volume, presence of symptoms, and cosmetic score, before and after RFA were compared using the Wilcoxon signed-rank test. Comparisons of treatment characteristics and outcomes of RFA between tumors involving the epidermis/dermis and those involving the hypodermis were made using chi-square tests for categorical variables and two-sample t-tests for continuous variables. All statistical analyses were performed using SPSS version 21.0 for Windows (IBM Corp., Armonk, NY, USA) and MedCalc version 19.1 (MedCalc Software, Mariakerke, Belgium) software, with p-values <0.05 defined as statistically significant.
Results
Patient and lesion characteristics
The characteristics of the patients and their lesions are shown in Table 1. A total of 50 recurrent tumors in 43 patients (mean age ± standard deviation [SD], 67.9 ± 14.4 years; 31 females) were included. Of the 43 patients, 39 were diagnosed with papillary thyroid carcinoma, 2 with follicular thyroid carcinoma, and 2 with medullary thyroid carcinoma. All patients underwent total thyroidectomy (42/43) or lobectomy (1/43) with neck node dissection. Thirty-six patients received radioactive iodine treatment after surgery. The mean largest diameter and volume of the initial tumor were 2.6 ± 2.2 cm (range, 0.6–10 cm) and 14.3 ± 31.9 mL (range, 0.04–151.2 mL), respectively. Of the 50 recurrent tumors, 16 were located in the central neck (including the thyroid operative bed, level VI, and pretracheal area), 30 in the lateral neck, 3 in the axilla, and 1 in the back. Of the 50 recurrent tumors, 9 involved the epidermis, 10 involved the dermis, and 31 involved the hypodermis. Of the 50 recurrent tumors, 22 were symptomatic, all presenting with skin bulging; 11 were associated with pain, 2 with skin necrosis, and 5 with bleeding. Of the 50 recurrent tumors, 1, 19, 4, and 26 were assigned cosmetic scores of 1, 2, 3, and 4, respectively. Of the 50 recurrent tumors, 22 were ablated for curative purposes and 28 for palliative purposes.
Patient and Recurrent Tumor Characteristics
Data are reported as mean ± standard deviation (range) or as number (%).
aCentral location included thyroid operative bed, level VI, and pretracheal area.
CND, central neck dissection; FTC, follicular thyroid carcinoma; MRND, modified radical neck dissection; MTC, medullary thyroid carcinoma; PTC, papillary thyroid carcinoma; RAI, radioactive iodine; RFA, radiofrequency ablation.
Comparisons of tumor characteristics treated with single and multiple RFA sessions
The characteristics of tumors treated with single and multiple RFA sessions are shown in Table 2. Twenty-nine recurrent tumors were treated with a single RFA session, while 21 recurrent tumors required multiple sessions, ranging from 2 to 6. Tumors treated with multiple RFA sessions were larger (diameter: 3.5 cm vs. 1.9 cm, p = 0.005; volume: 26.3 mL vs. 5.7 mL, p = 0.023), were more frequently symptomatic (71.4% vs. 24.1%, p = 0.001), had higher cosmetic scores (p = 0.001), and were more often involved the epidermis and dermis (p = 0.028).
Comparison of Tumor Characteristics Treated with Single and Multiple Radiofrequency Ablation Sessions
Data are reported as mean ± standard deviation or as number (%).
aCentral location included thyroid operative bed, level VI, and pretracheal area.
The bold values indicate P values less than 0.05.
Treatment characteristics of RFA
The RFA treatment characteristics are summarized in Table 3. A total of 88 RFA sessions (mean, 1.8; range: 1–6) were performed for the 50 recurrent tumors. The number of RFA sessions tended to be higher for tumors involving the epidermis/dermis than for those involving the hypodermis, but the difference did not reach statistical significance (2.2 vs. 1.5, p = 0.071). There was no statistically significant difference observed in the RF power, RF time, total energy, or electrode size between tumors involving the epidermis/dermis and those involving the hypodermis (all p > 0.05).
Treatment Characteristics of Radiofrequency Ablation According to Tumor Location
Data are reported as mean ± standard deviation (SD) or as number (%).
Treatment outcomes of RFA
The treatment outcomes of RFA are summarized in Table 4. At the first follow-up following RFA, residual unablated tumor was observed in 28% (14/50) of tumors, while the technique efficacy at one-year follow-up was 72% (36/50 [confidence interval or CI: 59.6–84.4%]) after additional RFA. At the last follow-up (mean duration of follow-up 3.1 ± 2.7 years; median [interquartile range]: 2.7 [1.1–4.5] years), both symptoms and mean cosmetic scores showed significant improvements (44% [22/50] vs. 12% [6/50], 3.1 vs. 0.5, respectively, both p < 0.001), the mean diameter and volume of the tumor were significantly decreased (2.6 vs. 1.2 cm, 14.3 vs. 5.6 mL, respectively, both p < 0.001), the clinical success rate was 86% (43/50), the complete disappearance rate was 54% (27/50), and the mean VRR was 77.3 ± 44.2%. A representative case of a well-treated tumor with complete disappearance after RFA is shown in Figure 2.
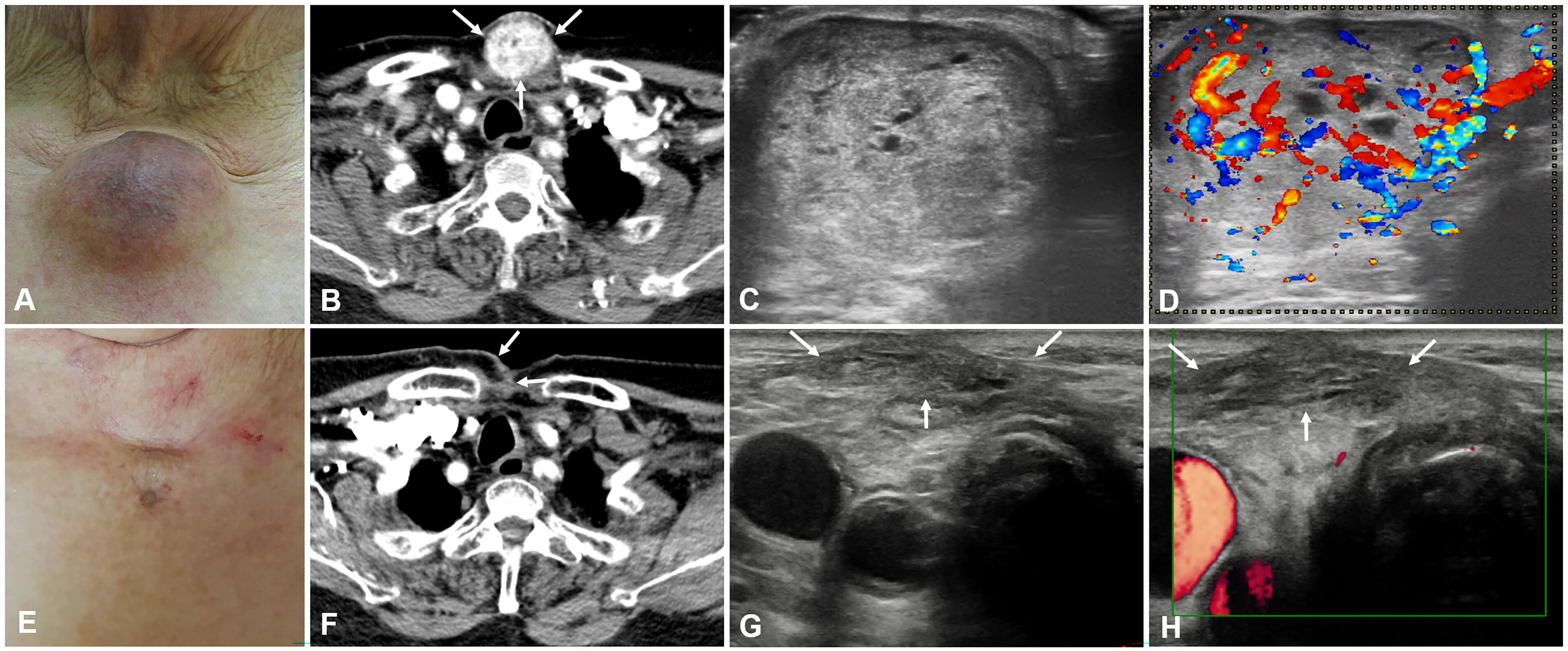
An 83-year-old woman with recurrent thyroid cancer in the right suprasternal area complained of skin bulging, pain, and redness (
Outcomes of Radiofrequency Ablation
Data are reported as mean ± standard deviation (range) or as number (%).
aTechnique efficacy was defined as the absence of detectable vasculature (or enhancement) and reduction in the volume (or disappearance) of the index tumor on both US and CT scans at 12 months post-RFA.
bClinical success was defined as the resolution of symptoms or cosmetic problems.
The bold values indicate P values less than 0.05.
Treatment outcomes of RFA according to involved skin layer
The treatment outcomes of RFA according to the involved skin layer are summarized in Table 5. Before RFA, the initial tumors involving the epidermis/dermis had significantly higher cosmetic scores (3.84 vs. 2.65, p < 0.001), were more frequently symptomatic (84.2% vs. 19.4%, p < 0.001), and were larger in size (diameter: 3.40 cm vs. 2.49 cm, p = 0.033; volume: 26.19 mL vs. 7.08 mL, p = 0.039) than those involving the hypodermis. The incidence of residual unablated tumors tended to be higher and the technique efficacy lower in tumors involving the epidermis/dermis than in those involving the hypodermis, but the differences were not statistically significant (residual unablated tumors: 42.1% [8/19] vs. 19.4% [6/31]; technique efficacy: 57.9% [11/19] vs. 80.6% [25/31]; both p = 0.085). At the last follow-up, there was no statistically significant difference in clinical success rate (78.9% [15/19] vs. 90.3% [28/31], p = 0.265), complete disappearance rate (42.1% [8/19] vs. 61.3% [19/31], p = 0.191), or mean VRR (65.5% vs. 84.6%, p = 0.141) between tumors involving the epidermis/dermis and those involving the hypodermis.
Outcomes of RFA according to Location
Data are reported as mean ± standard deviation (range) or as number (%).
aTechnique efficacy was defined as the absence of detectable vasculature (or enhancement) and reduction in the volume (or disappearance) of the index tumor on both US and CT scans at 12 months post-RFA.
bClinical success was defined as the resolution of symptoms or cosmetic problems.
The bold values indicate P values less than 0.05.
Complications of RFA
The complications associated with RFA are summarized in Table 4. Skin burns were observed in 4.9% per treatment session (2/41 [CI: 0–11.3%]) of epidermal/dermal tumor treatments but not in any hypodermal tumor treatments (p = 0.128). First-degree skin burns were noted immediately after RFA in two patients, and these healed within 3 months (Fig. 3). No statistically significant differences between epidermal/dermal and hypodermal tumors were found in the occurrence of voice changes (2.4% [1/41] vs. 2.1% [1/47], respectively, p = 0.922) or pain (22.0% [9/41] vs. 25.5% [12/47], respectively, p = 0.696). Vocal change spontaneously recovered within 1 month following RFA in all patients. No patient experienced a life-threating or major complications.

A 57-year-old woman with recurrent thyroid cancer in the right level 6. Initial CT
Discussion
Our study demonstrated that RFA effectively managed the clinical problems of skin-involving recurrent thyroid cancers, achieving technique efficacy of 72%, a clinical success rate of 86%, a complete disappearance rate of 54%, and mean VRR of 77.3%. No patients experienced life-threatening or major complications. To our knowledge, this is the first report on RFA for the treatment of recurrent thyroid cancers involving skin. Among the patients with epidermal/dermal tumors, two suffered skin burns (4.9%), but no burns were reported in patients with hypodermal tumors. These findings make it clear that when tumors involve the epidermis/dermis, where hydrodissection is less effective, the possibility of skin burns should be considered. Additionally, a thorough understanding of skin anatomy and the tumor location from pre-treatment US examinations is crucial for devising a safe and effective treatment strategy.
On the basis of the relationship between the tumor and involved skin layers, we subclassified the tumors into those involving the epidermis/dermis and those involving the hypodermis. We found that epidermis/dermis-involving tumors were more frequently accompanied by cosmetic issues and symptoms and tended to have a larger size. They tended to require more RFA sessions for treatment and exhibited slightly lower treatment efficacy compared with hypodermis-involving tumors, although these differences were not statistically significant. Skin burns were observed only in two patients with epidermis/dermis-involving tumors, probably because the efficacy of hydrodissection, which plays a vital role in preventing skin burns, 23,24 varies according to the location and composition of the skin layers. 12 Tumors involving the hypodermis can be easily separated from the dermis because the hypodermis is predominantly comprised of loose fat lobules. 25 By contrast, the epidermis possesses a keratin-rich compact nature, while the dermis is composed of dense collagen and elastin. 16 When tumors involve these latter two layers, hydrodissection becomes challenging, and there is consequently an increased risk of skin burns and it is more difficult to achieve adequate ablation of surrounding tissues. Therefore, ablation of recurrent thyroid cancer before it involves the epidermis/dermis yields better treatment efficacy and safety. When tumors involve the epidermis/dermis, more careful monitoring and cautious treatment are necessary during ablation.
The treatment of recurrent cancer involving the skin is technically challenging. 12 To ensure effective and safe RFA treatment for these cancers, we propose several treatment strategies. First, the skin puncture for the electrode should be 3–4 cm from the target tumor, because direct puncturing of the tumor with the electrode can lead to skin damage and necrosis, which are difficult to heal. Second, hydrodissection with a cold 5% dextrose solution is recommended between the tumor and the epidermis to prevent skin burns. Lastly, in cases where tumors contain significant hemorrhagic fluid, we initially ablate the feeding artery, then target the hypervascular tumor, and then ultimately aspirate the hemorrhagic fluid to avoid further bleeding during the procedure.
RFA can be performed for curative or palliative purposes in recurrent thyroid cancer, especially for patients at high surgical risk or those who refuse surgery. 7 The efficacy of the technique can be defined according to the treatment goal, either curative or palliative. For curative purposes, efficacy should be evaluated using the VRR of the index tumor and the rate of complete disappearance. For palliative purposes, the focus should be on symptom alleviation and improvement in quality of life through reduction of the size of the index tumor. In this study, we found that RFA was effective for treating recurrent tumors involving the skin, for both curative intent (mean VRR of 77.3% and complete disappearance rate of 54%) and palliative intent (clinical success rate of 86%). The VRR and complete disappearance rate in the present study were slightly lower than those in previous studies, which reported VRR ranging from 81.2% to 98.4% and complete disappearance rates ranging from 61.1% to 100% at a mean follow-up of 21.4–47.9 months. 18,19,26 –31 These differences may be due to our inclusion of only recurrent tumors involving the skin and patients who underwent RFA for both curative and palliative purposes. The treatment of skin-involving tumors for curative purposes can be somewhat challenging. However, skin-involving tumors can lead to skin necrosis and bleeding, significantly impacting the patient’s quality of life. Therefore, palliative treatment, aimed at alleviating symptoms and improving quality of life, holds significant importance.
Our study has several limitations. The patient sample size was rather low, and additionally, the retrospective design and single-center approach introduce inherent biases. To validate our findings, a future prospective study involving a larger and more diverse population is warranted. Retrospective analysis is also subject to limitations concerning the measurement of clinical outcomes.
In conclusion, based on our data, RFA appears to be a promising and safe technique for managing skin-involving recurrent thyroid cancer, achieving an 86% clinical success rate with no major complications. Notably, recurrent tumors involving the epidermis/dermis may pose a higher risk of skin burns than tumors involving the hypodermis, suggesting that early intervention before the tumor extends to those layers may be preferable. However, the present findings are preliminary, and further investigation in larger, prospective studies is needed to solidify RFA’s role in managing skin-involving recurrent thyroid cancer.
Footnotes
Authors’ Contributions
H.H.M.: Formal analysis (lead), writing—original draft (lead), and writing—review and editing (equal); J.H.B.: Conceptualization (lead), methodology (lead), validation (lead), writing—review and editing (lead), supervision (lead), and project administration (lead); S.R.C. and Y.J.C.: Conceptualization (supporting), methodology (supporting), supervision (supporting), and writing—review and editing (equal); K.-W.C. and T.Y.K.: Resources (supporting), conceptualization (supporting), and writing—review and editing (equal); J.H.L.: Resources (supporting), methodology (supporting), supervision (supporting), and writing—review and editing (equal). All authors approved the final version of the article.
Author Disclosure Statement
J.H.B. has been a paid consultant for STARmed since 2017.
Funding Statement
No funding was received for the research described in this article.
Supplementary Material
Supplementary Figure S1