
Abstract
Background:
Anaplastic thyroid cancer (ATC) is a rare but one of the most lethal types of human cancer. Although increasing evidence demonstrated that ATC tumors had a high mutation burden, little is known about the aberrancy of the noncoding genome of ATC except the well-investigated telomerase reverse transcriptase (TERT) promoter mutations.
Methods:
The mutational statuses of TBC1D12 5′ untranslated region (5′UTR), GPR126 intron 6, SDHD and PLEKHS1 promoters, as well as the TERT promoter and BRAFV600E mutations were determined using Sanger sequencing in 28 patients with ATC (19 women and 9 men) with a median (interquartile range) age of 64 (55–71) years, 14 thyroid cancer cell lines and a normal thyroid cell line. The prevalence of TBC1D12 5′UTR mutations in papillary thyroid cancer (PTC) and their association with clinicopathologic characteristics were explored by analyzing The Cancer Genome Atlas thyroid cancer dataset.
Results:
The noncoding mutations in TERT, SDHD and PLEKHS1 promoters, TBC1D12 5′UTR, and GPR126 intron 6 were collectively found in 82.1% (23/28) of ATC samples. Specifically, TERT promoter mutations were detected in 22 (78.6%) samples; GPR126 intron mutations were detected in 2 (7.1%) samples; and both SDHD and PLEKHS1 promoter mutations were detected in 1 (3.6%) ATC sample. Two hotspot mutations in TBC1D12 5′UTR were observed in 14 of 28 (50%) ATCs, 7 of 492 (1.4%) PTCs, and 1 cell line derived from ATC. TBC1D12 5′UTR mutations were significantly associated with older age at diagnosis (60 vs. 46 for wild type, p = 0.003), pathological T3/T4 stage (85.7% vs. 37.7%, p = 0.010), and advanced tumor stages (85.7% vs. 32.5%, p = 0.006) in PTC.
Conclusions:
This preliminary study for the first time showed a high prevalence of TBC1D12 5′UTR mutations in ATC and indicated an association between TBC1D12 mutation and aggressive characteristics of PTC, which needs to be confirmed in large cohort studies.
Dear Editor
Anaplastic thyroid cancer (ATC) accounts for 1–2% of all thyroid cancer cases, but it is the most aggressive and lethal form of thyroid cancer, with a median overall survival of 6–10 months. Several studies have sequenced the genome of thyroid cancer and revealed that ATC carried a higher mutation burden than differentiated thyroid cancer (DTC). 1 –3 However, those studies were mainly focused on exome, the noncoding region of thyroid cancer genome was rarely investigated except for two hotspot mutations in the core promoter region of telomerase reverse transcriptase (TERT). 4
The TERT promoter mutations occur in about 10% of DTC and increase up to 40–80% in ATC. 4,5 They activate TERT transcription by recruiting ETS transcriptional factors, 6,7 and correlate with aggressive characteristics and poor prognosis of thyroid cancer, particularly when coexisting with BRAF or RAS mutations. 4,5,8,9 Whether there is other common mutation in the noncoding genome of thyroid cancer, particularly in ATC, is largely unknown. To address this question, we sequenced ATC tissues and thyroid cancer cell lines for several noncoding mutations that had been reported in at least one cancer type other than thyroid cancer. These mutations are located in the 5′ untranslated region (5′UTR) of TBC1D12, intron 6 of GPR126, and promoter regions of SDHD and PLEKHS1. The TERT promoter mutations and the classical mutation BRAFV600E were also investigated.
This study was approved by the Institutional Ethics Committee of The First Affiliated Hospital of Sun Yat-sen University (approval number: [2023]041) in accordance with the Declaration of Helsinki, and the patient consent was waived because of the retrospective and anonymized nature of this study. A total of 28 formalin-fixed paraffin-embedded (FFPE) tissues from patients with ATC (19 women and 9 men), with a median (interquartile range [IQR]) age of 64 (55–71) years, who were diagnosed with and treated for ATC at The First Affiliated Hospital of Sun Yat-sen University between 1998 and 2023, were included in this study. The diagnosis of ATC was according to the criteria established by the World Health Organization, and all the tissues enrolled in the present study were confirmed by a senior pathologist (A.H.). As listed in Supplementary Table S1, 14 thyroid cancer cell lines, including BCPAP, K1, KTC-1, MDA-T41, TPC1, WRO, 8505C, 8305C, ACT-1, C643, CAL-62, HTh-7, KHM-5M, and TTA1, and the normal thyroid follicular epithelial cell line Nthy-ori 3-1 were also included. All these cell lines were routinely authenticated by short tandem repeat profiling and tested for mycoplasma. The genomic DNA was isolated from FFPE tissues and cell lines using the QIAamp DNA FFPE Advanced Kit (#56604, QIAGEN), and the mutational status of all interest genes was determined by polymerase chain reaction (PCR) amplification and Sanger sequencing. The PCR primers are listed in Supplementary Table S2. We also explored the distribution of TBC1D12 5′UTR mutation in papillary thyroid cancer (PTC) by analyzing The Cancer Genome Atlas (TCGA) thyroid cancer dataset and analyzed the correlation between TBC1D12 mutation and other common mutations, clinicopathological characteristics, and outcomes. The continuous variables were shown as median with IQR and compared by the Mann–Whitney U test; the categorical variables were shown as frequencies with percentiles and compared by Fisher’s exact test.
As shown in Figure 1A, we found highly prevalent mutations in TERT promoter and TBC1D12 5′UTR in ATC tissue samples, with a frequency of 78.6% (22/28) and 50% (14/28), respectively. The GPR126 intron mutations were found in 2 of 28 (7.1%) samples, both SDHD and PLEKHS1 promoter mutations were found in 1 (3.6%) sample. These noncoding mutations collectively occurred in 82.1% (23/28) of ATC samples. The BRAFV600E mutation was observed in 50% (14/28) of ATC samples. TBC1D12 5′UTR mutations occurred in 13 of 22 (59.1%) TERT promoter mutation positive cases versus 1 of 6 (16.7%) TERT wild-type cases (p = 0.165, per two-tailed Fisher’s exact test) and occurred in 9 of 14 (64.3%) BRAF mutation-positive cases versus 5 of 14 (35.7%) BRAF wild-type cases (p = 0.257). Notably, as shown in Figure 1B and C, the highly prevalent TBC1D12 5′UTR mutations occurred in two nucleotides close to the translation start site of TBC1D12 (chr10:96,162,368C>T and chr10:96,162,370G>A, referred as C368T and G370A for short hereafter, respectively). Specifically, the C368T and G370A mutation were found in 8 (28.6%) and 3 (10.7%) ATC cases, respectively. The C368T and G370A mutation co-occurred in 3 of 28 (10.7%) cases (Fig. 1D). Among the 15 cell lines enrolled in this study (Supplementary Table S1), TERT promoter mutations were found in 10 of 14 (71.4%) thyroid cancer cell lines, the BRAFV600E mutation was found in 7 (50%) thyroid cancer cell lines, TBC1D12 5′UTR mutations were detected in one ATC cell line (KHM-5M). On the contrary, genetic mutations in GPR126, SDHD, or PLEKHS1 were not observed in any of the thyroid cancer cell lines. No mutation was found in the normal cell line Nthy-ori 3–1.
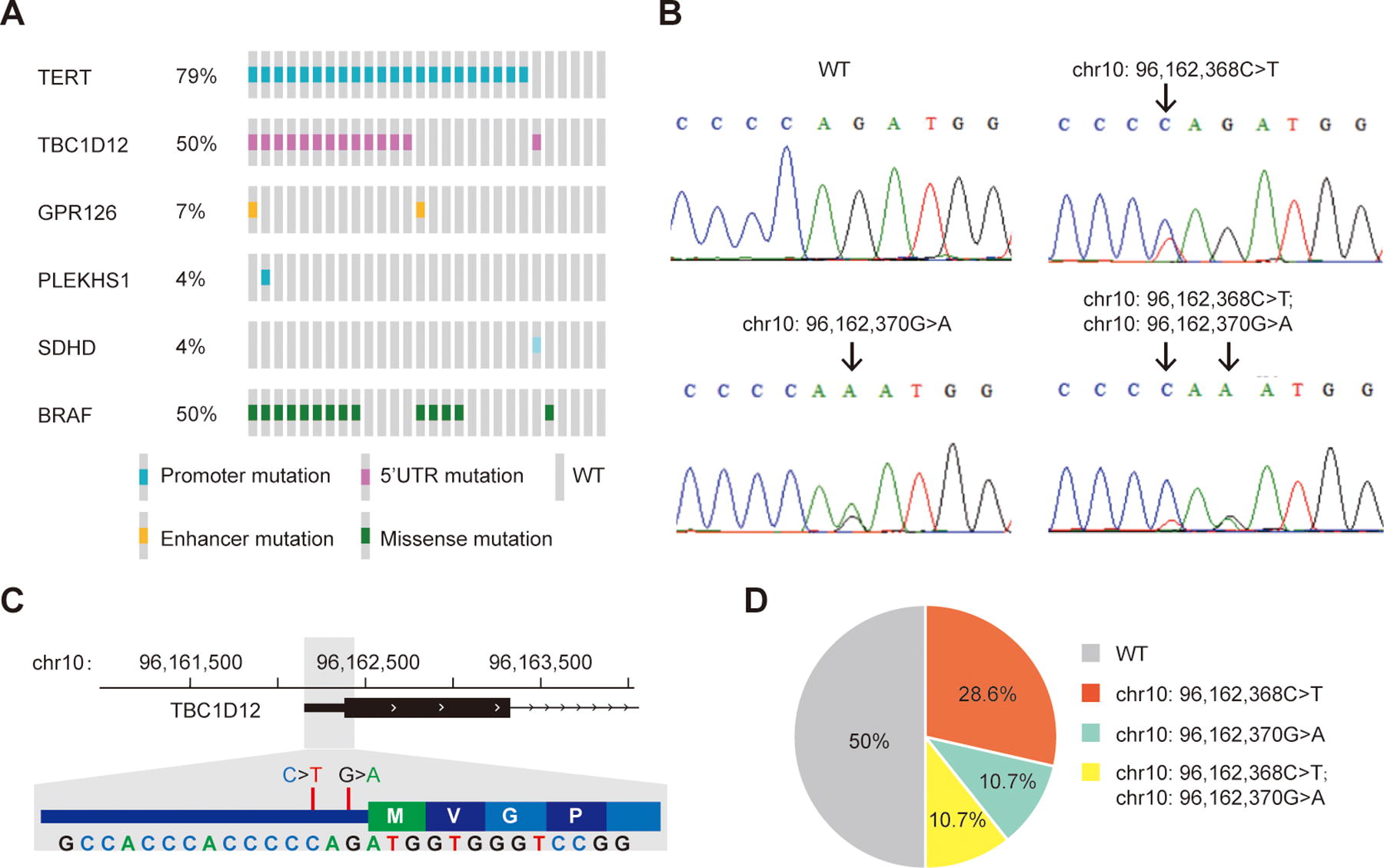
Identification of TBC1D12 5′UTR mutations in ATC.
Given the high prevalence of TBC1D12 5′UTR mutation in ATC, we next assessed the distribution of TBC1D12 5′UTR mutations in PTC by analyzing the TCGA thyroid cancer dataset. 10 As a result, TBC1D12 5′UTR mutations were identified in 7 of 492 (1.4%) informative tumors, with 4 (0.8%) C368T, 2 (0.4%) G370A, and 1 (0.2%) C368T and G370A co-occurrence. As shown in Table 1, TBC1D12 5′UTR mutations were significantly associated with older age at diagnosis, pathological T3/T4 stage, and advanced tumor stages. Specifically, the median (IQR) age of patients with ATC was 60 (57–73) versus 46 (35–57) in TBC1D12 mutation-positive versus -negative patients (p = 0.003), pathological T3/T4 stage was observed in 6 of 7 (85.7%) TBC1D12 mutation-positive patients versus 182 of 483 (37.7%) patients with wild-type TBC1D12 (p = 0.010), and tumor stage III/IV was 6 of 7 (85.7%) in TBC1D12 mutation-positive cases versus 157 of 483 (32.5%) in TBC1D12 mutation-negative cases (p = 0.006). There was no significant association of TBC1D12 5′UTR mutation with other clinicopathological characteristics and prognosis of PTC. In addition, no significant association was observed between TBC1D12 5′UTR mutations and BRAF, RAS, TERT mutations, or the mRNA level of TBC1D12 in PTC.
Association of TBC1D12 5′UTR Mutations with Clinical Characteristics and Outcomes of PTC
5′UTR, 5′ untranslated region; PTC, papillary thyroid cancer; TPM, transcripts per million; TERT, telomerase reverse transcriptase.
The two recurrent mutations in 5′UTR of TBC1D12 were initially identified in breast cancer by whole genome sequencing, 11 and then confirmed in urothelial bladder cancer, 12 but not in other common types of cancer. 13 Here, we report for the first time, to the best of our knowledge, TBC1D12 5′UTR are frequently mutated in ATC. Unlike TERT promoter mutations, we found that the TBC1D12 5′UTR mutations had no correlation with the gene’s mRNA expression in thyroid cancer. Notably, TBC1D12 mutations were not present in optimal APOBEC3A hairpins, the TBC1D12 site was not an efficient APOBEC3A substrate and the mutation frequency did not correlate with APOBEC3A activity, suggesting that TBC1D12 mutations are likely potential novel cancer drivers. 14 The function of TBC1D12 and the biological effect of the two 5′UTR hot spot mutations in the pathogenesis of thyroid cancer should be further explored, although a previous study has shown that TBC1D12 5′UTR mutations might confer an oncogenic role by modifying the translation efficiency of TBC1D12 or generating truncated protein. 11
Although the overall prevalence of TBC1D12 5′UTR mutations was low in PTC, the remarkably higher prevalence of TBC1D12 5′UTR mutations in patients with advanced PTC than in early-stage patients suggests that mutations in TBC1D12 5′UTR play a role in the progression of PTC, and it might be a candidate genetic marker for risk stratification. Moreover, as PTC is well differentiated and ATC is an undifferentiated thyroid cancer, the strikingly higher prevalence of TBC1D12 5′UTR mutations in ATC over PTC indicates that TBC1D12 5′UTR mutations may promote the conversion of PTC to ATC by accelerating PTC dedifferentiation. It is noteworthy that the frequency of TBC1D12 mutations was lower in ATC cell lines than in tumor specimens in our cohort. This discrepancy may be caused by the limited number of cell lines used in this study, or by ethnic difference since the TBC1D12 mutation-positive cell line KHM-5M was derived from an Asian patient with ATC, and all the seven cell lines from Caucasian patients with ATC were negative for TBC1D12 mutation.
Besides TBC1D12 5′UTR and TERT promoter mutations, we detected several noncoding mutations in GPR126, SDHD, and PLEKHS1 in this study. Most noncoding genetic variations are enriched in gene-regulatory regions and involved in regulating gene expression. Two hotspot mutations in intron 6 of GPR126 had been reported to correlate to aberrant GPR126 expression and promote angiogenesis in bladder cancer. 15 The SDHD promoter mutation was commonly observed in melanoma, and it reduced SDHD expression by ablating the binding of GABPA/B1 transcription factor complex to the gene’s promoter. 16 PLEKHS1 promoter mutations were frequently identified in bladder cancer and could serve as a potential biomarker for diagnosis and monitor the posttreatment surveillance of the disease. 17 Although increased PLEKHS1 expression was associated with aggressive characteristics and adverse outcomes of PTC, PLEKHS1 promoter hotspot mutations were only commonly identified in radioiodine refractory DTC, but relatively uncommon in sporadic PTC, ATC, and thyroid cancer cell lines. 18 –20 According to the results in the current study, all these noncoding mutations in GPR126, SDHD, and PLEKHS1 genes were identified in ATC, indicating the complexity of the genetic basis of ATC, although the prevalence of these mutations was not very high.
In summary, this preliminary study identified two hotspot mutations in the 5′UTR of TBC1D12 as common genetic events in ATC, and they were associated with aggressive behaviors of PTC, although their frequency was very low in PTC. Our findings need to be confirmed in large cohort studies.
Footnotes
Authors’ Contributions
R.L. and J.L. designed the research. J.L., J.Y., A.H., and W.L. contributed to clinical evaluation of the patients and collection of tissue samples. G.H., J.X., Q.D., and Y.S. performed mutation detection and data analysis. G.H. and R.L. drafted the article, with input from all authors.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
This study was supported by grants from the National Natural Science Foundation of China (No. 82072952 and No. 82222051).
Supplementary Material
Supplementary Table S1
Supplementary Table S2