
Abstract
Background:
Thyroid-stimulating hormone (TSH) and subsequent free thyroxine (FT4) concentrations outside the reference interval (RI) are used to diagnose thyroid diseases. Most laboratories do not provide age-specific RIs for TSH and FT4 beyond childhood, although TSH concentrations vary with age. Therefore, we aimed to establish TSH and FT4 age-specific RIs throughout life and aimed to determine whether using these RIs would result in reclassification of thyroid disease diagnoses in adults.
Methods:
This multicenter retrospective cross-sectional study used big data to determine indirect RIs for TSH and FT4. These RIs were determined by TMC and refineR-analysis, respectively, using four different immunoassay platforms (Roche, Abbott, Siemens, and Beckman Coulter). Retrospective data (2008–2022) from 13 Dutch laboratories for general practitioners and local hospitals were used. RIs were evaluated per manufacturer. Age groups were established from 2 to 20 years by 2-year categories and decade categories between 20 and 100 years.
Results:
We included totally 7.6 million TSH and 2.2 million FT4 requests. TSH upper reference limits (URLs) and FT4 lower reference limits were higher in early childhood and decreased toward adulthood. In adulthood, TSH URLs increased from 60 years in men, and from 50 years in women, while FT4 URLs increased from 70 years onward. Using adult age-specific RIs resulted in a decrease in diagnoses of subclinical and overt hypothyroidism in women above 50 and men above 60 years in our Roche dataset.
Conclusion:
This study stressed the known importance of using age-specific RIs for TSH and FT4 in children. This study also showed the clinical relevance of using age-specific RIs for TSH in adulthood to reduce diagnoses of subclinical hypothyroidism in older persons. Therefore, implementation of adult TSH age-specific RIs should be strongly considered. Data are less uniform regarding FT4 age-specific RIs and more research should be performed before implementing these in clinical practice.
Introduction
Serum thyroid-stimulating hormone (TSH) and free thyroxine (FT4) are two of the most frequently requested laboratory parameters. Overt hypo- and hyperthyroidism and subclinical hypo- and hyperthyroidism are diagnosed based on TSH concentrations that fall outside the reference interval (RI) and subsequent FT4 concentrations. In specific cases, total triiodothyronine (TT3) and free T3 can be measured in addition to TSH and FT4. It is known that TSH and FT4 RIs need to be adjusted in neonates to correctly interpret these concentrations. 1 Furthermore, it has been recommended to use age-specific RIs for TSH and FT4 during childhood. 2 However, most laboratories do not differentiate these RIs based on age beyond childhood. Previous studies showed that TSH concentrations also increase with aging in adults, both in cross-sectional and longitudinal cohorts, 3 –8 although some studies observed a decrease in TSH concentrations with aging. 9,10 The influence of aging upon changes in FT4 concentration in adults is even less conclusive. Ma et al. 11 showed slightly lower FT4 RIs in adults above 60 years compared with adults younger than 60 years, as described in the same dataset by Zhong et al. 12 Another study showed no change in mean FT4 concentration in a longitudinal follow-up period of 13 years (age at baseline around 45 years). 5 However, an increase in mean FT4 concentration varying from 0.26 pmol/L over 13 years and 4.5 pmol/L over 6.5 years of follow-up were reported as well at an older age (age at baseline around 70 years). 7,10
Indirect methods to establish RIs, i.e., methods using a large amount of existing historical laboratory data, can be seen as an excellent alternative for the determination of direct RIs in specific populations. 13 Indirect methods are able to determine RIs even in the presence of pathological data, as long as these do not exceed 20–40% of the total dataset. 14 Depending on the initial dataset, extensive exclusion criteria are not always necessary. To establish direct RIs in the older population, inclusion of healthy older adults is necessary. However, comorbidities and the use of interfering medication increase with aging and older adults are, therefore, less often suitable to serve as healthy volunteers for their age category. Furthermore, there may be ethical objections to include healthy children to determine direct RIs. Two previous studies showed that an indirect method can be reliably used for the determination of TSH and FT4 RIs. 11,12 Recently, we used an indirect method to establish RIs for TSH and FT4 using four frequently used immunoassay platforms (Roche, Abbott, Siemens, and Beckman Coulter), which confirmed the necessity of stratification based on age. 15 Therefore, the current study aimed to establish indirect TSH and FT4 age-specific RIs using those four frequently used immunoassay platforms in the same dataset as Dirks et al. 15
Materials and Methods
TSH and FT4 results
In this multicenter retrospective cross-sectional study, indirect RIs were established using historical data (2008–2022) from 13 Dutch laboratories including inpatients and outpatients from general practitioners and local hospitals. These laboratories covered most parts of the Netherlands (Atalmedial Diagnostic Centers, Amsterdam; Northwest Clinics, Alkmaar; St. Jansdal Hospital, Harderwijk; Meander Medical Center, Amersfoort; St. Antonius Hospital, Nieuwegein; Dicoon Gelderse Vallei Hospital, Ede; Treant Zorggroep, Hoogeveen; VieCuri Medical Center, Venlo; Eurofins Gelre, Apeldoorn; Saltro Diagnostic Center, Utrecht; Nij Smellinghe Hospital, Drachten; Diagnostiek voor U, Eindhoven; Stichting Certe Medische Diagnostiek en Advies, Groningen). Due to the retrospective design, the study was not subject to the Medical Research Involving Human Subjects Act because it does not impose any act or mode of behavior on the subjects. This was confirmed by the local institutional review board of St. Antonius Hospital. All data were distributed anonymously. TSH and FT4 concentrations were analyzed using the commonly used automated immunoassays Cobas and Modular (Roche Diagnostics, Vienna, Austria), Architect (Abbott Diagnostics, Lake Forest, IL, USA), Unicel Dxl (Beckman Coulter Inc, Brea, CA, USA), and Centaur and Atellica (Siemens Diagnostics, Erlangen, Germany). Immunoassays showed stable RIs from 2008 to 202215. Only the Abbott FT4 RIs decreased between 2013 and 2015. Therefore, only results from 2015 to 2022 were included for this immunoassay. TPO-antibody status was not known. Several TSH and/or FT4 results per year are more likely to indicate thyroid pathology. Therefore, TSH and FT4 results were excluded in case of more than one measurement per calendar year per person to minimize thyroid pathology in the data. In addition, non-numerical results and results from patients older than 100 years were excluded. No other exclusions were made. TSH and FT4 concentrations are highly variable during the first weeks after birth, which has been established in previous literature. 1 We did not have sufficient retrospective data to draw conclusions for this group nor for the age category 1–2 years and, therefore, did not include children below the age of 2 years. Reflex-testing bias, meaning that FT4 may be more often pathological in response to an abnormal TSH result, was tested and was not present. This was reported in the paper of Dirks et al. 15 Indirect RIs established in age category 18–60 years (TSH) or 18–70 years (FT4) (hereafter called regular adult RIs) per immunoassay based on this dataset were reported in the article by Dirks et al. and more detailed information on the methodology can be found in that paper. 15
Statistics
Results from the different immunoanalyzers per manufacturer were combined, analyzed, and presented per manufacturer. To assess indirect RIs, TSH and FT4 concentrations were described by age groups and sex. Age groups were established from 2 to 18 years by categories of 2 years and in adults by a category of 18–20 years followed by categories per decade between 20 and 100 years. TSH RIs were determined using Truncated-Minimum-Chi-Square (TMC; TMC Software Manual, version 13, revision 2022-11-15) and FT4 RIs were determined using refineR (R package refineR version 1.6.0). A recent study showed that TMC and refineR were the best suitable indirect methods for TSH and FT4 RI determination, respectively. 14 TSH generally has a heavily skewed distribution, whereas FT4 is approximately normally distributed, making TMC and refineR the most appropriate indirect methods. A combination of Excel and R Statistical Software v. 4.2.1 (Foundation for Statistical Computing, Vienna, Austria) was used to perform exclusion steps and statistical analyses. A minimum sample size of 300 samples per category was used. Indirect age-specific RIs were compared with the regular adult (indirect) RIs using equivalence limits (ELs). 16 In short, ELs are determined by the permissible measurement uncertainty at the two limits of the RI. It is based on the permissible analytical standard deviation derived from the empirical biological variation (calculated from the RI). Age-specific RIs with reference limits that surpassed ELs corresponding to the regular adult reference limits were considered statistically different, meaning an age-specific RI was appropriate. Further details regarding the establishment and comparison of indirect RIs can be found in the study by Dirks et al. 15
Reclassification in diagnosis of thyroid disease
We assessed whether the diagnoses of (subclinical) hypothyroidism and hyperthyroidism changed when applying sex- and age-specific RIs in adults. We included all measurements, and in contrast with the dataset described above, we also included samples with more than one measurement per year per person, of which only the first measurement was used. These samples may indicate thyroid pathology and could be useful for this purpose. To illustrate the impact of using age-specific RIs, we reclassified thyroid status of all Roche data, which was the largest dataset and deemed suitable for this proof-of-principle analysis. To reclassify (subclinical) hypothyroidism based on age-specific RIs, the percentages of these thyroidal illnesses with the regular adult indirect RIs were calculated and were compared with the percentages obtained with age- and sex-specific RIs. A TSH above the upper reference limit (URL) and FT4 within the RI were classified as subclinical hypothyroidism, while a TSH below the lower reference limit (LRL) and FT4 within the RI were assessed as subclinical hyperthyroidism. A TSH above the URL and FT4 below the LRL were classified as overt hypothyroidism and vice versa was classified as overt hyperthyroidism.
Results
The pattern of all TSH and FT4 immunoassay results with age is described in the next paragraphs, while absolute TSH and FT4 concentrations of all immunoassays can be found in Supplementary Tables S1, S2, S3, S4, S5 and S6. In total, we included 7.6 million TSH and 2.2 million FT4 requests. The indirect methods provided an estimated pathological fraction, based on the distribution of the analyte, which remained below 20%.
Pediatric age-specific RIs
TSH
Figure 1A shows, for all four immunoassays, age-specific TSH RIs (n = 412.837) for girls and boys separate and combined. From the age of 2 to 12, the URLs and LRLs of TSH were significantly higher compared to ELs corresponding to the regular adult reference limits. However, beyond the age of 12 years, the URLs and LRLs started to decrease and aligned with the regular adult levels somewhere between 14 and 18 years. In boys, TSH URLs started at a higher concentration at the age of 2 years than in girls. These URLs decreased and were comparable between boys and girls around 8 to 10 years.
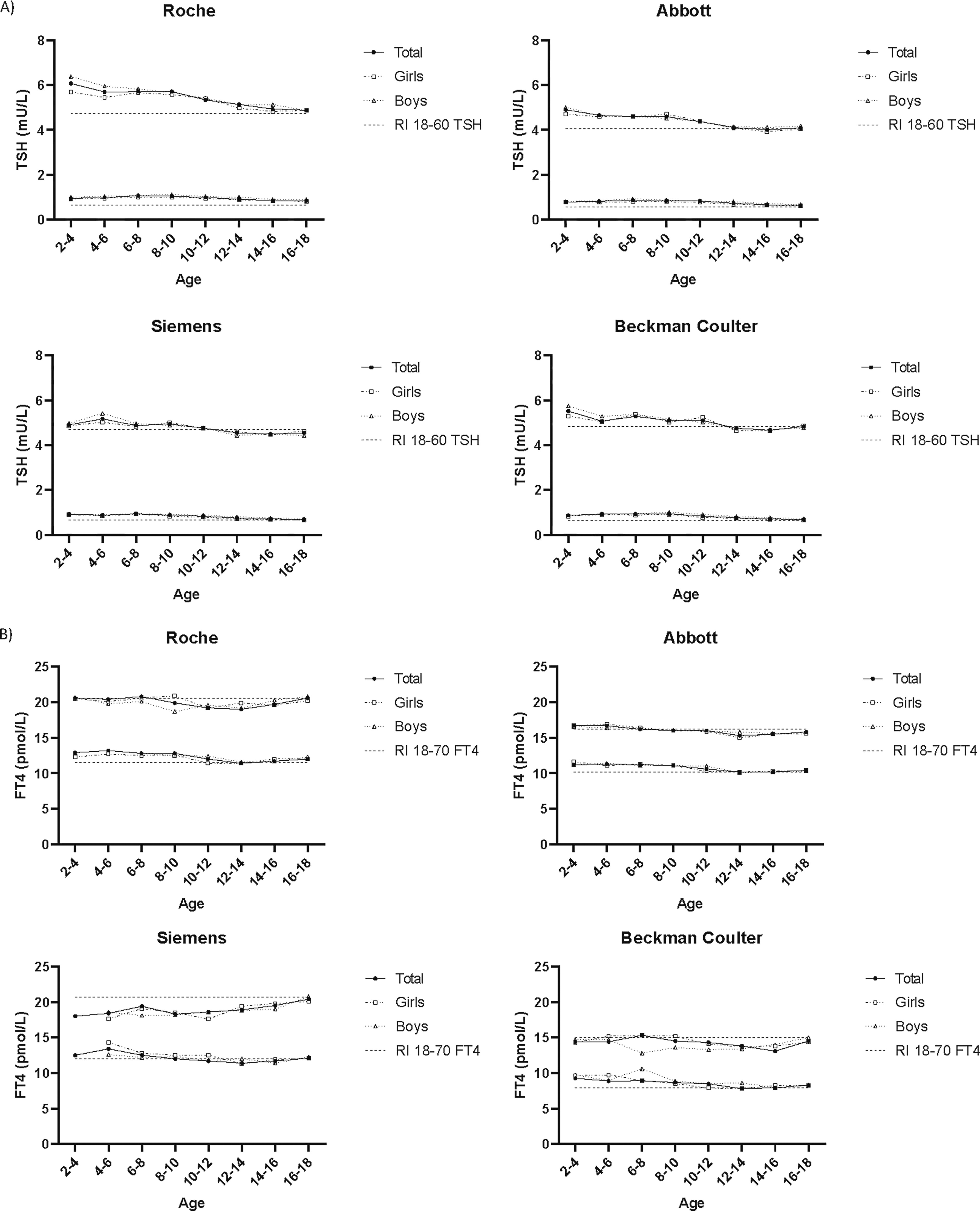
Pediatric age-specific reference limits (LRL and URL, lower and upper continuous lines) of the indirect RIs for girls and boys together and separately. (
FT4
Pediatric FT4 age-specific RIs (n = 112.189) are depicted in Figure 1B. For most methods, the FT4 URLs are stable during childhood, with a slight decrease between age 12 and 14 years. Only Siemens showed a continuously increasing FT4 URL up to adult levels around 16 to 18 years. FT4 LRLs were significantly higher up to the age of 10 years compared with adult levels and decreased after age 10 years to adult LRLs in all immunoassays. No substantial differences were seen between boys and girls.
Adult age-specific RIs
TSH
Age-specific TSH RIs (n = 7.2 million) in adulthood are depicted in Figure 2A. A statistically significant increase in TSH URLs from around the age of 60 was seen in all immunoassays, while the LRLs remained stable until the age of 80. This tendency was seen in both men and women, where in women the significant increase in TSH URLs already started earlier, around the age of 50 years. The LRLs slightly decreased above 80 years for Abbott and Beckman Coulter and above the age of 90 years for Roche and Siemens.
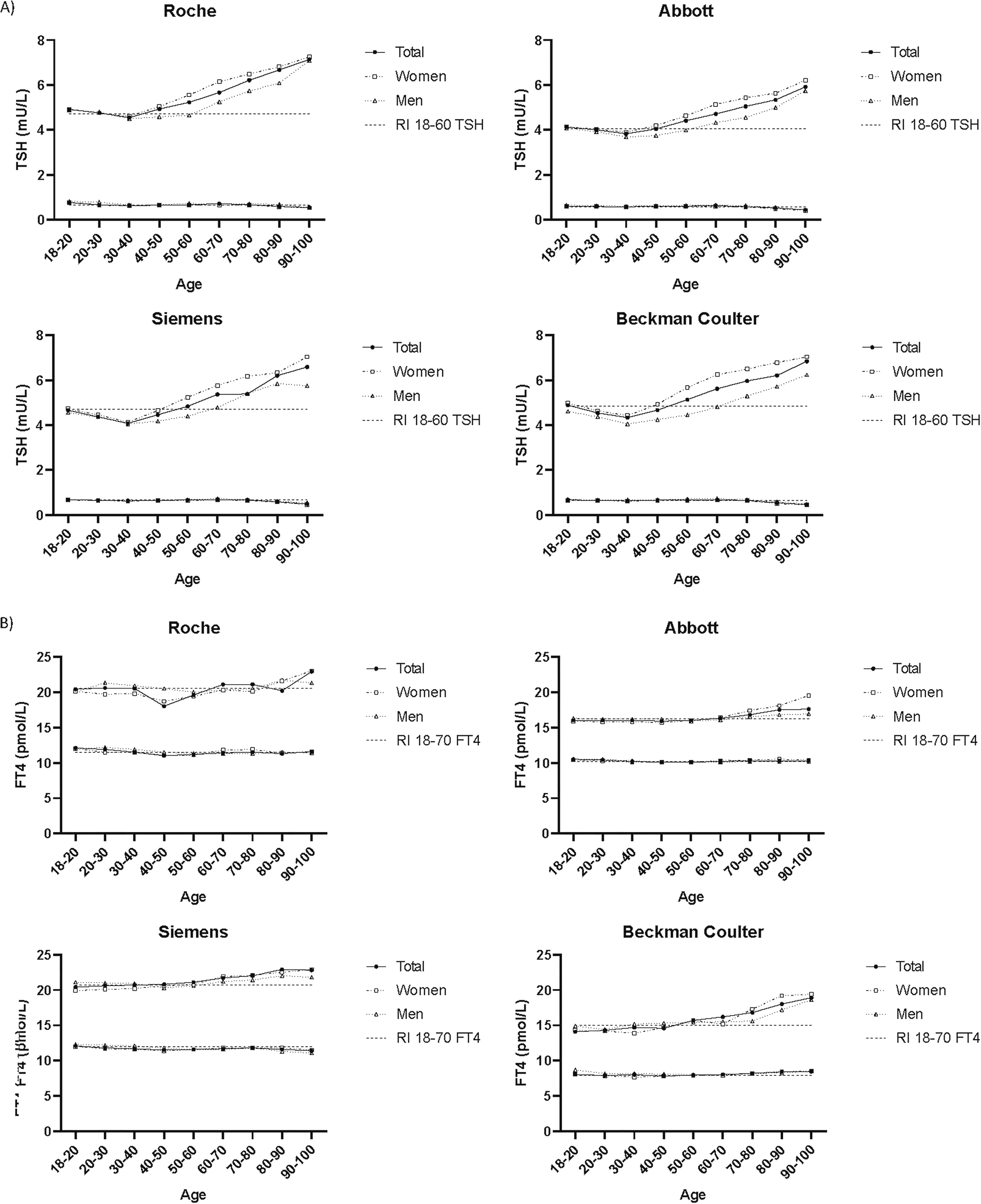
Adult age-specific reference limits (LRL and URL, lower and upper continuous lines) of the indirect RIs for women and men together and separately. (
FT4
Figure 2B shows age-specific FT4 RIs (n = 2.1 million) in adulthood. FT4 URLs increased from age 70 years onward. A dip in FT4 URLs was found at age 40–50 years for the Roche immunoassay, although this was not observed for the other immunoassays. In men, FT4 URLs increased less compared with women, which was similar for all immunoassays. The FT4 LRLs remained stable for all immunoassays in both women and men.
Reclassification in diagnosis of thyroid disease
Figure 3 shows the percentage of (subclinical) hypothyroidism diagnoses in women and men when either regular adult or our defined sex- and age-specific indirect RIs from the Roche dataset were used. In total, results from 194.856 women and 85.215 men were used. Results showed a decrease in subclinical hypothyroidism from 13.1% to 8.6% in women between age 50 and 60 years and from 22.7% to 8.1% in the age category of 90–100 years (in men 10.9% to 7.7% in age category 60 to 70 years and 27.4% to 9.6% in age category 90 to 100 years). Diagnoses of overt hypothyroidism decreased from 3.0% to 2.2% and from 2.8% to 2.3% in the same age categories in women (in men 1.7% to 1.4% and 4.0% to 2.9% in the same age categories). Results for (subclinical) hyperthyroidism did not show a clear decreasing or increasing pattern and can be found in Supplementary Figure S1.

Percentage of (subclinical) hypothyroidism in (
Discussion
This study showed that TSH and FT4 RIs are age-specific. Pediatric TSH RIs are generally wider than adult TSH RIs. Above the age of 50–60 years, TSH URLs increase considerably with age in both men and women. FT4 RIs display a similar, though moderate trend with aging. On the other hand, FT4 RIs in childhood are somewhat narrower; before the age of 10 years, the LRLs are slightly higher and after the age of 10 years, the URLs are a bit lower. Implementation of adult age-specific RIs for TSH in clinical practice remains a debated topic. However, our results indicate that age-specific RIs, especially for TSH, are clinically significant.
Pediatric age-specific RIs
Our data showed wider TSH RIs before the age of 12 years for all immunoassays, while FT4 RIs were more narrow. Multiple studies assessed TSH RIs during childhood and found decreasing TSH RIs in line with our results, irrespective of the immunoassay used. 2,17 –24 Hall et al. (Architect, Abbott) used a large prospective database (CALIPER database) with up to 1500 test results per analyte and used age categories of 6 months with which our results could best be compared. 19 We replicated the decreasing pattern of the TSH URLs described in the study of Hall et al., although a larger decrease was found by Hall. Our TSH LRLs gradually declined during childhood, while a temporary increase in LRLs followed by a decline was found in the study of Hall. Another comprehensive study considered all papers published until 2017 that established TSH RIs in childhood and showed a larger variation of TSH LRLs in the age category of 5–10 years compared with 1–5 years, which decreased in the age category of 10–20 years. 25 The TSH URLs decreased in the age category of 5–10 years and the variation increased again in the age category of 10–20 years. This variation together with a consistent decrease in TSH RIs highlights the importance of assay and population-specific RIs.
Our results showed stable FT4 URLs throughout childhood with a slight dip between ages 12 and 14 years. Previous literature confirmed stable FT4 URLs, 2,18,21,22,26 with a dip between ages 10 and 15 years in the study of Surup et al., 20 while a gradual decrease (1–2 pmol/L) toward adolescence was found by several studies as well. 17,19,23 Only the FT4 URL from Siemens showed a surprising increase in our study. Because changes in RI patterns are not expected to be assay-dependent, it is most likely due to the smaller number of Siemens FT4 requests we used for the indirect RI establishment. Slight sex-differences in FT4 URLs were seen at ages 8–10 years (Roche) and 6–8 years (Beckman Coulter), emphasizing a dip for boys. We were unable to provide a conclusive explanation. FT4 LRLs were comparable with adult RIs from the age of approximately 10 years onward. Several studies reported a gradual decrease in LRLs, 18 –21,23 while stable LRLs were found as well. 17,22,24,26 The study of Önsesveren et al. assessing many papers until 2017 showed a gradual decrease in FT4 LRLs and URLs during childhood. 25
Pediatric RIs are commonly used in most laboratories and also provided by several manufacturers. According to the ENDO-ERN network consensus statement, TSH and FT4 age-specific RIs should be used in the follow-up of children with congenital hypothyroidism. 27 However, so far no consensus has been reported regarding predetermined age categories. For example, the package insert of Roche advises to use three specific age categories below one year, and subsequently age categories 1 to 6, 6 to 11, and 11 to 20 years for TSH and FT4. It is well known that age-specific RIs below the age of 1 year are necessary for clinical diagnostics. 1 Our indirect RIs showed that age-dependency played an important role in childhood TSH and FT4 RIs as well and for this reason, we underscore the use of age-specific RIs in children between 1 and 18 years old. However, it is difficult to uniformly establish RIs for the appropriate age categories. Most studies showed that the TSH URLs gradually decline during childhood and demonstrate the benefit of using multiple age-specific RIs in childhood. Our indirect RIs showed that pediatric FT4 RIs may be necessary as well but necessitate fewer age categories than TSH and can be aligned with adult RIs from the age of approximately 16 years.
Adult age-specific RIs
Our results showed that while the TSH LRLs remained stable in adulthood with age, or even slightly decreased, the TSH URLs increased significantly from age 60 years. Previous studies confirmed this finding, showing increased TSH URLs when using an indirect method 3,28 –30 or direct method to determine RIs. 4 –6,8,31 –33 Our study showed that TSH URLs increase already around the age of 50 years in women, whereas this is around age 60–70 years in men. The same pattern was found previously, 3,33,34 whereas three other studies could not find a sex difference in age-specific RIs. 4,6,8 We found that the URLs of FT4 slightly but significantly increased from age 70 years, which is in contrast with previous studies showing no effect of age at all. 30,32 –34 Using the Roche immunoassay, FT4 URL increased with almost 3 pmol/L from the age-interval 70–80 up to 90–100 in women. Furthermore, the increase in FT4 URLs we found was less obvious in men. The stable FT4 LRLs are in accordance with literature. 30,32,33
The cause of age dependency for TSH and FT4 RIs is still unknown. Previous studies showed that iodine status in childhood is correlated with thyroid function later in life. 35 Growing up in an iodine deplete area increased the risk of developing hyperthyroidism and an iodine excess increased the risk of hypothyroidism at older age. 36 This would argue for a pathophysiological process that does not match with adjusting RIs with age. On the other hand, previous studies showed a protective effect of increased TSH in adults above 80 years, 37 –39 which could be explained as a physiological response of the hypothalamus–pituitary–thyroid axis in aging. Supporting a physiological response, research in mice showed a decrease of liver deiodinase 1 and an induction of liver deiodinase 3 in normal aging mice, 40 resulting in decreased conversion of T4 into the active T3 and increased deactivation of T4 and T3, respectively. In combination with an increased TSH URL, this could support the hypothesis of decreased thyroid hormone metabolism during aging. Human data confirm higher reverse T3 concentrations with aging, indicating decreased deiodinase 1 and increased deiodinase 3 activity as well. 41
It has been shown that the incidence of subclinical hypothyroidism increases with age, with 10% prevalence in patients aged 80 years and older. 42 Although the current adult hypothyroidism European Thyroid Association guideline recommends to only consider levothyroxine treatment in adults >70 years if TSH >10 mU/L and in case of clear symptoms of hypothyroidism or a high risk of vascular disease, 43 levothyroxine is still largely prescribed for older adults with subclinical hypothyroidism without meeting these criteria. 44,45 As a result, levothyroxine can be discontinued in almost a third of its users without consequences for TSH and FT4 results, which was predominantly the case in patients who were diagnosed with subclinical hypothyroidism. 46 Furthermore, prospective randomized clinical trials showed no benefit of levothyroxine treatment for subclinical hypothyroidism in patients above 65 years. 47,48 Even more so, a slightly increased TSH may be advantageous in older adults above 80 years old, emphasizing treating subclinical hypothyroidism is not beneficial in this group at all. 37,38,49 Therefore, to further avoid subclinical thyroid disease to become a “laboratory induced condition,” it has been advocated to increase TSH URLs in older adults. 50,51 Applying age-specific TSH RIs in adulthood could reduce these clinically insignificant biochemical diagnoses of subclinical hypothyroidism in older adults. The study of Kahapola-Arachchige et al. evaluated this hypothesis and found a TSH URL increase from 3.75 mU/L at age 35–40 to 5.0 mU/L at age 85–90 (Centaur, Siemens) but was deemed to be irrelevant because only a maximum of 2% of participants aged <90 years would receive a reclassified outcome of thyroid status based on their age-specific RIs. 8 By contrast, our study showed a substantial decrease of diagnoses of subclinical hypothyroidism in women and men aged between 50 and 100 years using age-specific RIs. Diagnoses of overt hypothyroidism decreased as well, although to a lesser extent. We do not have a clear explanation for this contrasting observation compared with the study of Kahapola-Arachchige et al. Nevertheless, based on our results, we can conclude that implementing age-specific RIs in women >50 years and in men >60 years would lead to fewer diagnoses of (subclinical) hypothyroidism and less unnecessary levothyroxine prescriptions.
Strengths and limitations
The major strength of this study is the use of a large retrospective dataset from diverse regions across the Netherlands to determine TSH and FT4 RIs in child- and adulthood using four frequently used immunoassays. This dataset was sufficiently large to reliably establish TSH and FT4 RIs per 2 years in childhood and per decade in adulthood. This is an advantage compared with previous studies using less age categories, enabling to better assess the influence of age. A limitation of this design is that we did not have access to additional patient characteristics (e.g., body mass index, smoking status, ethnicity, pregnancy) that may influence TSH and FT4 concentrations. It is known that factors such as ethnicity or TPO-antibody status may influence TSH and FT4 concentrations. 52 Although ideally, we would assess the influence of these factors, it also reflects clinical laboratory practice, particularly in primary care, where RIs are used without taking most of these factors into account. Moreover, not all age-specific RIs were established with a sample size larger than 5000. The study of Ammer et al. described that this sample size would, in combination with a pathological fraction ≤20%, result in superior RIs compared with the direct method. However, also a smaller sample size still leads to precise results when maintaining a similar pathological fraction. 14 Although the pathological fraction of our dataset cannot be calculated exactly, the indirect methods do provide an estimated pathological fraction, based on the distribution of the analyte, which remained well below 20%. With that we are fairly confident that the pathological fraction never exceeded 20% of the total dataset. Therefore, we feel assured that our age-specific RIs can be reliably interpreted. In addition, our analysis exclusively incorporated laboratory results within the Netherlands, which may have limited generalizability of the RIs. Nevertheless, the data used from 13 Dutch laboratories provided a good representation of the Dutch population and may also be applied to countries with similar demographic compositions. Furthermore, we assessed RIs from the four most frequently used immunoassays in the Netherlands.
Conclusion
Based on the establishment of our indirect RIs, we would encourage using age-specific RIs for TSH and FT4 in childhood and TSH in older age. Data are less uniform regarding FT4 age-specific RIs in adults and more research should be performed before implementing this. Furthermore, using age-specific adult RIs for TSH (and FT4) is likely to have an impact on diagnosing (subclinical) hypothyroidism and, thus, treatment decisions. Therefore, its implementation in clinical practice is recommended.
Footnotes
Acknowledgments
Results related to this manuscript have been presented by Heleen Jansen as Rapid Communication at the European Congress of Endocrinology (Stockholm, 11–14 May 2024).
Author Contribution Statement
H.I.J.: Conceptualization, Methodology, Investigation, Writing—original draft, Writing—review and editing, Visualization. N.F.D.: Conceptualization, Methodology, Formal analysis, Investigation, Writing—review & editing. J.J.H.: Writing—review and editing. E.T.B.: Investigation, Writing—review and editing. J.W.B.: Investigation, Writing—review and editing. M.M.B.: Investigation, Writing—review and editing. A.Y.D.: Investigation, Writing—review and editing. I.M.D.: Investigation, Writing—review & editing. S.C.E.: Investigation, Writing—review and editing. P.E.: Investigation, Writing—review and editing. J.G.: Investigation, Writing—review and editing. M.J.W.J.: Investigation, Writing—review and editing. S.K.: Investigation, Writing—review and editing. W.H.A.K.-J.: Investigation, Writing—review and editing. A.K.: Investigation, Writing—review and editing. E.M.: Investigation, Writing—review and editing. A.W.: Investigation, Writing—review and editing. A.S.P.V.T.: Writing—review and editing. M.D.H.: Writing—review and editing. E.B.: Writing—review and editing. A.B.: Writing—review and editing. A.C.H.: Conceptualization, Methodology, Supervision, Writing—review and editing. W.P.J.D.E.: Conceptualization, Methodology, Supervision, Writing—review and editing.
Author Disclosure Statement
All authors declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6