
Abstract
Introduction:
Concerns have been raised that glucagon-like peptide 1 receptor agonists (GLP1-RAs) may increase the risk of thyroid cancer, but evidence remains conflicting. We therefore investigated if GLP1-RA use, compared with use of dipeptidyl peptidase-4 inhibitors (DPP-4is), was associated with thyroid cancer risk in patients with type 2 diabetes.
Methods:
This multisite cohort study with subsequent meta-analysis included six population-based databases from Canada (Ontario), Denmark, Norway, South Korea, Sweden, and Taiwan. Study populations comprised patients with type 2 diabetes between 2007 and 2023. Cox regression models estimated hazard ratios (HR) and 95% confidence intervals (CIs) for thyroid cancer among GLP1-RA users compared with DPP-4is. Models were weighted using standardized mortality ratio weights generated from time-specific propensity scores. Site-specific HRs were pooled using a fixed-effects model.
Results:
We identified 98,147 users of GLP1-RA and 2,488,303 users of DPP-4i, with the median follow-up among users of GLP1-RA ranging from 1.8 to 3.0 years. Overall, use of GLP1-RA relative to use of DPP-4i was not associated with an increased risk of thyroid cancer (pooled weighted HR 0.81, CI 0.59–1.12). Similarly, we observed no increased risk in thyroid cancer with increasing cumulative dose of GLP1-RA among GLP1-RA ever-users. Subgroup analysis of types of thyroid cancer was not possible. Results remained consistent across a range of supplementary analyses.
Discussion:
In this large multisite study, utilizing data from six population-based databases, we found no evidence that GLP1-RA use is associated with an increased risk of thyroid cancer with follow-up ranging from 1.8 to 3.0 years, providing some reassurance to patients and clinicians about the short-term safety of these drugs. Nevertheless, evidence was insufficient to rule out excess risk with long-term use, due to the short follow-up.
Introduction
Glucagon-like peptide 1 receptor agonists (GLP1-RAs) are a class of incretin-based glucose-lowering medications, 1 commonly used treatments for type 2 diabetes due to their favorable cardiovascular, weight and blood glucose outcomes. 2,3 Recently, two GLP1-RAs (liraglutide and semaglutide) have been shown to be highly effective in the management of obesity. 4,5 However, concerns have been raised that GLP1-RAs may increase the risk of thyroid cancer. 6
The hypothesis that GLP1-RAs may increase the risk of thyroid cancer is biologically plausible. Glucagon-like peptide 1 receptors are more prominently expressed in papillary thyroid cancer cells than in normal thyroid cells.,7,8 Furthermore, preclinical studies have demonstrated an excess in C-cell thyroid malignancies in rodents. 9,10 However, the relevance to humans is undetermined. 9,11 Several observational studies have evaluated this association, reporting conflicting findings. A recent study reported that GLP1-RA users were at increased risk of thyroid cancer (hazard ratio [HR] 1.46, 95% confidence interval [CI] 1.23–1.74) compared with nonusers. 6 However, the association between GLP1-RA and thyroid cancer at low levels of exposure (≤1 year use) indicates the potential for residual confounding. Other observational studies have reported null associations with GLP1-RA and thyroid cancer risk. 12,13 Further, in long-term evaluations of randomized trial participants, there was no indication of increase in biomarkers for thyroid cancer or thyroid cancer among GLP1-RA users. 14,15 In contrast, meta-analyses of randomized trials report elevated odds ratios for thyroid cancer with GLP1-RA. 16 –19
In light of the conflicting evidence and owing to increasing trends in GLP1-RA use, 20 we aimed to evaluate if GLP1-RAs used to treat type 2 diabetes are associated with an increased risk of thyroid cancer across six international sites, with a specific focus on cumulative dose.
Methods
Data sources
This international cohort study utilized a common protocol approach to examine the risk of thyroid cancer with GLP1-RA use utilizing databases from Canada, Denmark, Norway, South Korea, Sweden, and Taiwan. We included data between 2019 and 2022 in Canada, 2007 and 2023 in Denmark, 2009 and 2022 in Norway, 2010 and 2022 in South Korea, 2010 and 2022 in Sweden, and 2014 and 2020 in Taiwan. Supplementary Table S1 in Supplementary Data provides further details on data sources.
Study cohorts
Within each database, we conducted a cohort study where patients initiating GLP1-RAs were compared with patients initiating dipeptidyl peptidase 4 inhibitors (DPP-4is). Patients initiating these drugs were eligible for inclusion if they were aged 40 years or older (≥66 years and ≥60 years in Canada and Sweden, respectively), filled a prescription for metformin in the year prior to cohort entry and had a minimum of 5 years of medical information in their respective data source (minimum 1 year in Canada and Norway) to serve as minimum wash out period to ensure that patients had not used either drug class at any time before cohort entry. DPP-4is were chosen as the main active comparator as they are a clinically relevant alternative to GLP1-RAs. 2,21
Cohort entry was defined as the date of dispensing of a first prescription of either GLP1-RA or DPP-4i, with follow-up beginning 1 year after cohort entry to allow for a latency time window and to reduce reverse causality and detection bias. 22 We excluded patients with a history of cancer (except nonmelanoma skin cancer) partly to ensure that the cancer of interest was not an incorrectly diagnosed primary tumor or metastasis from an earlier tumor and partly because cancer treatments may increase the risk of subsequent cancers. We also excluded patients with a history of multiple endocrine neoplasia (not available in Norway), therapeutic radiation (not available in Norway or Sweden), those previously treated with radioiodine, or those who initiated a GLP1-RA and DPP-4i on the same day (to prevent misclassification bias). Finally, as the main analysis utilized an active comparator new user design, those prescribed either one of the study drugs of interest at any time before cohort entry were excluded. In Canada, the active comparator new user design could not be implemented, therefore, Canada only contributed to supplementary analysis 8 (see below). For definitions, see Supplementary Table S2 in Supplementary Data.
All patients were followed starting 1 year after cohort entry and followed until a first-ever diagnosis of thyroid cancer, death from any cause, emigration, 10 years after treatment initiation, or the end of the study period, whichever occurred first. We chose an intention-to-treat approach whereby patients were considered continuously exposed to their cohort entry drug until the end of follow-up, irrespective of treatment switching or discontinuation. Ethical review or approval for the use of each data source followed local governing bodies in each country. For further information on site-specific ethical review, see Supplementary Data.
Outcome definition
The primary outcome was incident thyroid cancer diagnosis. In Canada, Denmark, Norway, and Sweden, incident thyroid cancer was identified from their respective Cancer Registries. In addition, thyroid cancer diagnoses were identified from inpatient and outpatient records from the Patient Registries during 2023 in Denmark and during 2022 in Sweden (where cancer registry data was not yet available). In South Korea and Taiwan, incident thyroid cancer diagnoses were defined from either an inpatient or outpatient diagnosis during the follow-up period. See Supplementary Table S2 in Supplementary Data for definitions.
Confounder adjustment
We considered the following potential confounders, all measured on or before cohort entry: age, sex, diabetic nephropathy, diabetic retinopathy, diabetic neuropathy, peripheral arterial disease, chronic kidney disease, heart failure, myocardial infarction, ischemic heart disease, cerebrovascular disease, overweight or obesity, goiter (not available in Norway), hypothyroidism, hyperthyroidism (not available in Norway), thyroiditis (not available in Norway), pregnancy (not available in Norway), duration of treated diabetes, Charlson comorbidity index, income and education level (only available in Norway), markers of smoking, markers of alcoholism, and prescriptions for insulin, other glucose-lowering drugs, thyroid hormones, antithyroid medications (not available in Norway), lipid modifying drugs, antihypertensives, and antiplatelets (for definitions, see Supplementary Table S3 in Supplementary Data).
Statistical analysis
We used calendar time-specific (one-year intervals) propensity scores to reweigh our study population and account for differences in the baseline characteristics between GLP1-RA and DPP-4i cohorts. 23,24 Propensity scores were estimated using multivariable logistic regression as the predicted probability of receiving a GLP1-RA versus a DPP-4i conditional on the covariates listed above. Calendar-time-specific propensity scores were selected to account for the temporal changes in utilization patterns for glucose-lowering medications and changes in thyroid cancer incidence during the study period. 20,23 –26 Following propensity score estimation, individuals were weighted on the propensity score using standardized mortality ratio (SMR) weights. 27 Covariate balance was both assessed prior to and postweighting using standardized mean differences with differences less than 0.10 indicating good balance. 28
Using a Cox proportional hazards model, we calculated a weighted HR with 95% CI (robust variance estimator) to assess the association between GLP1-RA use (relative to DPP-4i use) and thyroid cancer. For the cumulative dose analysis, follow-up time was split into either 60-day (Norway), 90-day (Denmark), or 180-day (Sweden) time periods and the cumulative defined daily dose for GLP1-RA in each time period was calculated. Poisson regression was used to estimate adjusted rate ratios. In the cumulative dose analysis, we adjusted for a restricted number of covariates, including age, sex, calendar time, obesity (Norway only) and markers of diabetic severity (diabetic nephropathy [Norway only], insulin and other glucose-lowering drugs; for definitions, see Supplementary Table S3). Further elaboration of our analytical approach is provided in Supplementary Data.
Supplementary analyses
We performed the following supplementary analyses: (1) examined associations for thyroid cancer with GLP1-RA use within subgroups defined by sex and age (<70 years vs. ≥70 years); (2) changed the active comparator treatment to initiators of other glucose-lowering therapies including (a) sodium-glucose cotransporter 2 inhibitors (SGLT2i) and/or (b) sulfonylureas (SUs); (3) excluded patients with a history of thyroid-related disorders at baseline to reduce the risk of confounding (Norway excluded); (4) restricted GLP1-RA users to liraglutide only, that is, the earlier GLP1-RA with longer follow-up available (South Korea and Taiwan excluded); (5) examined associated for thyroid cancer by histological type of thyroid cancer (medullary vs. nonmedullary); (6) used a broader outcome definition by including both malignant and in situ thyroid cancer (South Korea and Norway excluded); (7) excluded patients using insulin at baseline to create a more homogenous study population (Taiwan excluded); (8) allowed GLP1-RA users with prior DPP-4i use to enter the GLP1-RA cohort to utilize the full study population (excluded in the main analysis); and (9) used an SMR weighted piece-wise exponential model to estimate time specific cumulative rate at 5 years and 10 years for risk of thyroid cancer among GLP1-RA users (South Korea and Taiwan excluded). Definitions are provided in Supplementary Table S4 in Supplementary Data.
Pooling site-specific estimates
HRs were pooled using a Mantel–Haenszel fixed-effects model. 29 A random-effects model was used with the Hartung–Knapp–Sidik–Jonkman estimator as a further analysis. 30 Heterogeneity was assessed using the I 2 statistic. 31
Study transparency 32
This study is registered in the Real-World Evidence Registry (https://osf.io/rk3uj/) including the initial protocol (using the HARPER template 33 ) and subsequent amendments. The analytical code for this study is available at https://gitlab.sdu.dk/pharmacoepi/glp1-thyroid. The procedures for accessing the databases utilized in the study can be found in Supplementary Data. The article is aligned with guidance from the reporting of studies conducted using observational routinely collected health data for pharmacoepidemiology 34 and the Strengthening the reporting of observational studies in epidemiology (STROBE) statements 35 (see Supplementary Table S5 in Supplementary Data for STROBE checklist).
Results
For the main analysis, 98,147 and 2,488,303 patients newly treated with GLP1-RA and DPP-4i, respectively, met the study inclusion criteria (database-specific flow charts are presented in Supplementary Figs. S1, S2, S3, S4 and S5 in Supplementary Data). Database-specific GLP1-RA cohorts ranged from 4141 individuals in Taiwan to 45,534 individuals in Denmark and DPP-4i cohorts ranged from 65,757 individuals in Norway to 1,763,176 individuals in South Korea (Supplementary Figs. S1, S2, S3, S4 and S5 in Supplementary Data). After pooling, the GLP1-RA cohorts generated 67 incident thyroid cancer events during 362,436 person-years of follow-up. In the DPP-4i cohorts, there were 6209 incident thyroid cancer events during 10,551,547 person-years of follow-up. The median follow-up across the GLP1-RA cohorts ranged from 1.8 to 3.0 years. The median follow-up across DPP-4i cohorts ranged from 2.8 to 6.8 years.
Before weighting, exposure groups were generally comparable, although, GLP1-RA users had a longer duration of treated diabetes than DPP-4i users, were more likely to use insulin, were less likely to use other classes of glucose-lowering medications, and were less likely to have a diagnosis of chronic kidney disease (Table 1). After weighting, all covariates were well balanced between exposure groups with the standardized differences <0.10 (database-specific standardized differences are presented in Supplementary Tables S6, S7, S8, S9 and S10 in Supplementary Data) (Table 1).
Pooled a Baseline Characteristics of Glucagon-Like Peptide 1 Receptor Agonists and Dipeptidyl Peptidase 4 Inhibitors
Before weighting: counts (percentages) unless otherwise stated; after weighting: counts, rounded to the nearest whole number (percentages), unless otherwise stated.
Pseudopopulation created by applying standardized mortality ratio weights from calendar time-specific propensity scores.
DPP-4is, dipeptidyl peptidase 4 inhibitors; GLP1-RA, glucagon-like peptide 1 receptor agonists; SD, standard deviation.
Compared with DPP-4i users, GLP1-RA users were not associated with an increased risk of thyroid cancer (pooled weighted HR 0.81, 95% CI 0.59–1.12) (Table 2). A total of 155,903 individuals contributed to the cumulative dose analysis (76,518 from Denmark, 38,444 from Norway and 40,941 from Sweden). When evaluating thyroid cancer risk among GLP1-RA ever-users as a function of amount filled, we found no trend in risk with increasing cumulative dose (Fig. 1). Site-specific results are shown in Supplementary Figure S6 in Supplementary Data. Due to small numbers, this analysis was not completed in Canada, South Korea, and Taiwan. Overall, in the main analysis, results were consistent across all sites, with weighted HR estimates ranging from 0.44 (95% CI 0.18–1.07) in Sweden to 1.54 (95% CI 0.75–3.15) in Norway (Table 2).
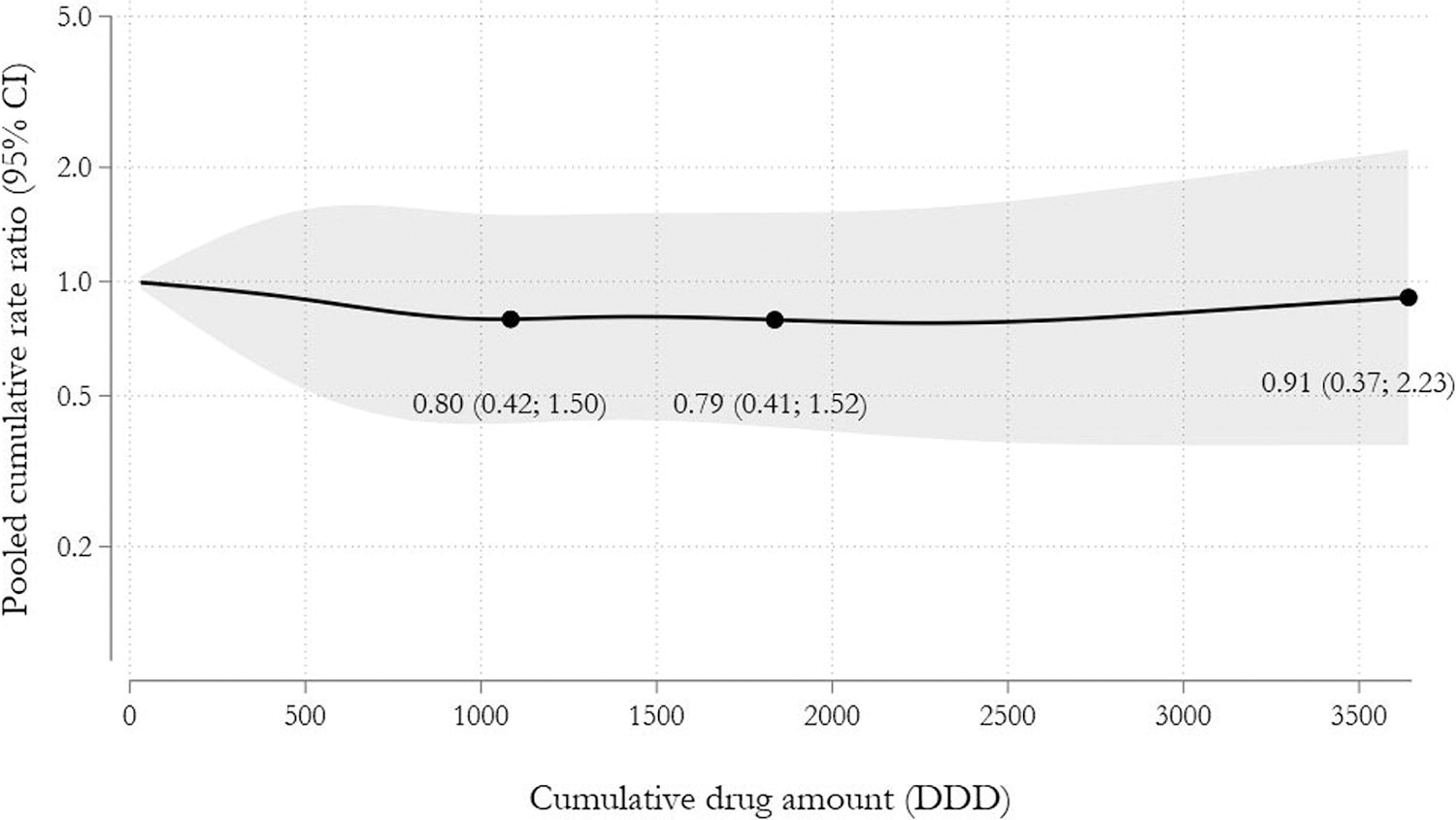
Pooled rate ratio of thyroid cancer as function of the cumulative amount of GLP1-RA filled (measured in DDDs) modeled using restricted cubic splines among GLP1-RA ever users. DDD, daily defined dose; GLP1-RA, glucagon-like peptide 1 receptor agonists.
Hazard Ratios for the Association Between Glucagon-Like Peptide 1 Receptor Agonists and Dipeptidyl Peptidase 4 Inhibitors and Thyroid Cancer Incidence by Individual Site and Pooled Using Fixed-Effect Models
Pooled using a fixed-effects model; I 2 = 0%. Pooling with a random-effects model generated hazard ratio 0.83, CI 0.55–1.27.
DPP-4is, dipeptidyl peptidase 4 inhibitors; GLP1-RA, glucagon-like peptide 1 receptor agonists.
The supplementary analyses are summarized in Figure 2. There was no effect-measure modification by age or type of GLP1-RA. We observed no changes in thyroid cancer risk among male GLP1-RA users but observed a decreased risk of thyroid cancer among female GLP-RA users. When analysis was stratified by subtype of thyroid cancer no effect modification was observed for non medullary thyroid cancer. Analysis restricting to medullary thyroid cancer was not possible due to low number of outcomes. Results were consistent with the main analysis when the primary analysis was repeated to include both in situ and malignant cancer outcomes (weighted HR 0.73, 95% CI 0.47–1.13), removing insulin users at baseline (weighted HR 1.02, 95% CI 0.64–1.63), restricting to individuals with no history of thyroid disorders at baseline (weighted HR 0.80, 95% CI 0.55–1.16), permitting prior DPP-4i use among GLP1-RA users (weighted HR 1.08, 95% CI 0.76–1.53), and changing the comparator to SGLT2i (weighted HR 1.08, 95% CI 0.83–1.40). Changing the comparator to SUs, GLP1-RAs users had a significant elevation in risk of thyroid cancer (weighted HR 1.80, 95% CI 1.28–2.52). Database-specific flow-charts for each supplementary analyses, if relevant, are presented in Supplementary Figures S7, S8, S9, S10, S11, S12, S13, S14, S15, S16, S17, S18, S19, S20, S21, S22, S23, S24, S25, S26, S27, S28, S29 and S30 in Supplementary Data and database-specific results for each supplementary analyses are presented in Supplementary Tables S11, S12, S13, S14, S15, S16, S17 and S18 in Supplementary Data. Finally, when modelling time since initiation using restricted cubic splines, there was no evidence of an increase in thyroid cancer among GLP1-RA users with the cumulative rate ratio of 0.59 (95% CI 0.32–1.09) after 5 years and 1.00 (95% CI 0.61–1.65) after 10 years (Supplementary Fig. S31 in Supplementary Data).
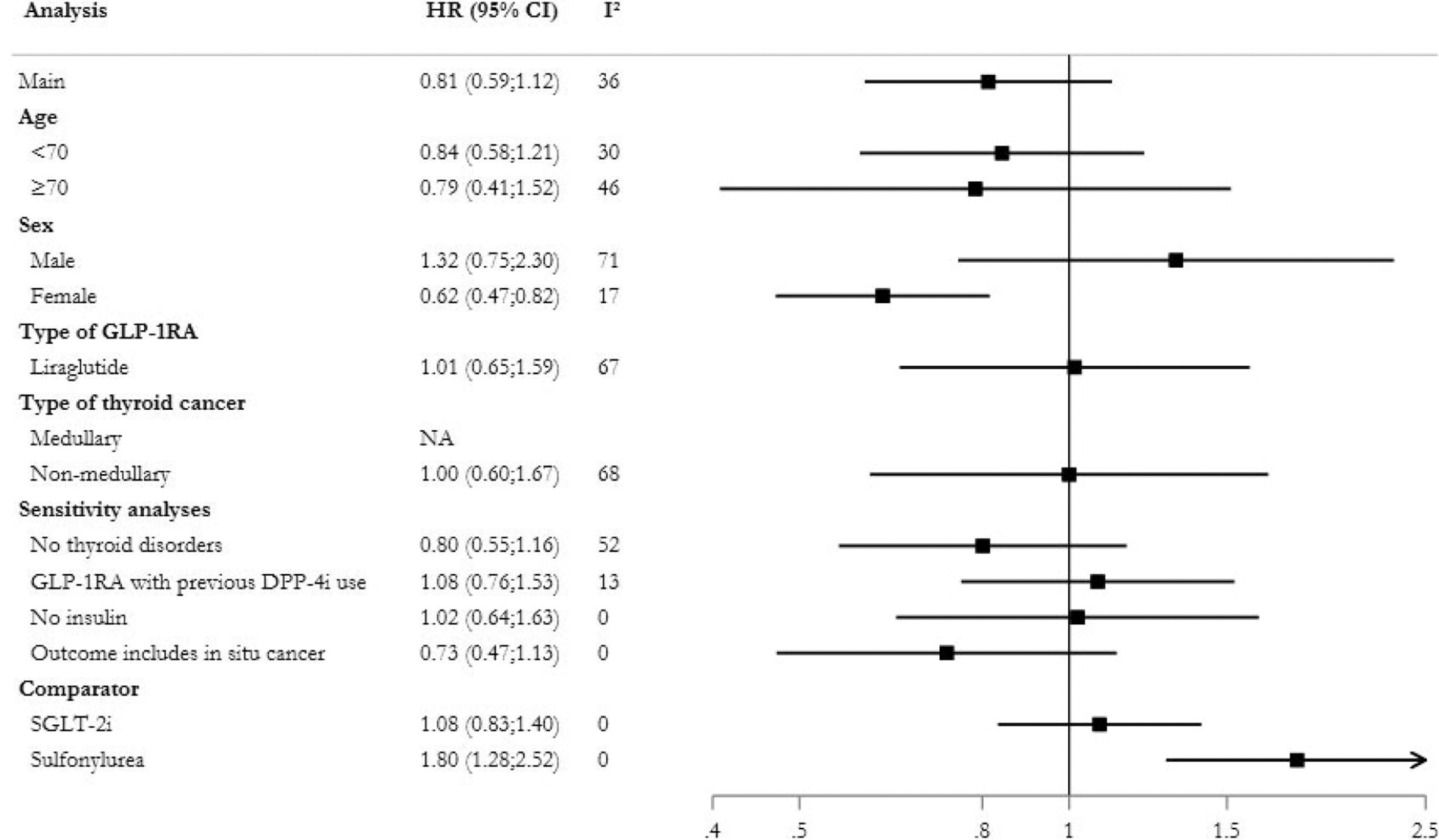
Forest plot summarizing the results of the pooled primary and supplementary analyses, with HRs and 95% CIs for the association between the use of GLP1-RAs vs. DPP-4is. CI, confidence interval; DPP-4is, dipeptidyl peptidase 4 inhibitors; GLP1-RA, glucagon-like peptide 1 receptor agonists; HR, hazard ratio; SGLT-2i: sodium-glucose cotransporter 2 inhibitor.
Discussion
In this large international cohort study, we observed that the use of GLP1-RA was not associated with an increased risk of thyroid cancer compared with DPP-4i use among patients with type 2 diabetes. Similarly, there was no observed risk of thyroid cancer associated with increasing cumulative dose of GLP1-RA use. The results generally remained consistent across supplementary analyses that addressed different sources of bias.
In contrast to the findings in this study, meta-analyses of randomized trials have reported elevated risk estimates; however, the risk estimates were highly imprecise. 16 –19 Randomized trials are not designed to assess cancer as an outcome, with the included randomized trials reflecting post hoc analysis of safety events. Due to the low incidence of thyroid cancer and the short follow-up time of randomized trials, even large trials would not be sufficiently powered to detect outcomes such as thyroid cancer. Some observational studies also reported elevated estimates. A generally well-designed study reported an increase in risk in thyroid cancer among GLP1-RA users (HR 1.46, 95% CI 1.23–1.74) when compared with use of other glucose-lowering agents. 6 Similar results were also obtained when use of other glucose-lowering agents were used as comparators in a cohort study utilizing two U.S. databases. 36 Using “other glucose-lowering agents” as comparators has the potential to introduce heterogeneity into the cohort as exposure groups may be misaligned in important baseline characteristics, potentially introducing bias.
Our findings are consistent with recently published observational research that used robust methodologies such as the active comparator new-user design. A Scandinavian study that utilized DPP-4i as the active comparator reported an HR of 0.93 (95% CI 0.66–1.31) and an HR of 1.16 (95% CI 0.65–2.05) when SGLT2is were used as the active comparator. 13 Similarly, a South Korean study that utilized SGLT2i as the active comparator, demonstrated that GLP1-RAs were not associated with increased risk of thyroid cancer (HR 0.98, 95% CI 0.62–1.53). 12 Our study supports this growing evidence based on the short-term safety of GLP1-RA in relation to thyroid cancer risk.
Supplementary analyses generally remained consistent with the main analysis. However, in females we observed a significantly lower risk for thyroid cancer among GLP1-RA users compared with DPP-4i. Although a higher risk of thyroid cancer among female GLP1-RA users has previously been observed, overall, evidence is lacking and additional studies are required investigate this association. 6 Furthermore, we observed an elevated risk of thyroid cancer when the comparator was changed to SUs (HR 1.80, 95%CI 1.28–2.52). Clinicians may be less likely to prescribe SU’s to individuals who are overweight or obese due to the propensity for weight gain with these drugs and may prefer alternatives such as GLP1-RAs, which have beneficial weight loss effects. Although we tried to adjust for obesity, it is likely that many individuals were misclassified as not having obesity as obesity was not well captured and recorded, as we relied on a diagnosis of obesity to capture obesity, and we had no information on weight. Therefore, individuals with overweight or obesity are likely more prevalent in the GLP1-RA cohort compared with the SU cohort. Prior research has found a positive association between weight and thyroid cancer risk. 37 Therefore, as obesity is a risk factor for thyroid cancer, the imbalance in unmeasured obesity among the GLP1-RA cohort potentially could introduce bias that would drive the estimate towards increased risk.
Our study has several strengths. First, to our knowledge, this is the largest study conducted in a diabetic population. Our multisite approach enabled us to utilize data from six different countries, increasing the generalizability of our results. Our standardized study design and analysis through implementation of a common protocol reduced heterogeneity. Second, we only considered new users of either GLP1-RAs or DPP-4is in the main analysis, thus eliminating the biases associated with inclusion of prevalent users. 38 Third, we used DPP-4i users as the active comparator as they are used at a similar stage of diabetes during the study period and were introduced around a similar time to GLP1-RAs, which likely reduced confounding by indication. 39 Finally, our results remained consistent across sites as well as across several supplementary analyses.
Our study has limitations. First, GLP1-RAs are relatively new drugs, limiting potential duration for follow-up. In our study, the median duration of follow-up for the GLP1-RA cohort ranged from 1.8 to 3.0 years and in the context of cancer latency this may be too short to investigate cancer risk. 40 However, the rationale of this current study was based on findings of an increased risk of thyroid cancer even at low levels of exposure, 6 therefore our study provides reassurance on the short-term thyroid cancer risk with GLP1-RA use. Second, due to the differences in availability of GLP1-RAs across different countries, subgroup analyses on individual agents were not permitted except for liraglutide. There may be differences in thyroid cancer risk within the class of GLP1-RAs and future work should endeavor to address this area. Third, residual confounding from unmeasured or unknown confounders (e.g., smoking, family history) as well as imperfectly captured confounders (e.g., obesity, ionizing radiation) is possible. As obesity increases the risk of thyroid cancer, this may have resulted in residual confounding. In an additional descriptive analysis of the AMORIS cohort 41 in Sweden, we found that GLP1-RA users tended to have slightly elevated body mass index (BMI) and HbA1c compared with DPP-4i users (see Supplementary Table S19 in Supplementary Data). We attempted to reduce the impact of confounding by indication using an active comparator and propensity score-weighted methods ensured balance in all measured baseline confounders. Exposure to GLP1-RAs resulted in a relatively low number of thyroid cancer events (n = 67), limiting statistical power. A considerable number of GLP1-RA users had prior DPP-4i use and were therefore excluded from the main analysis, reducing the size of the GLP1-RA cohort. An additional analysis was included to address this and reassuringly results were consistent with the main analysis. Finally, the risk of medullary thyroid cancer among GLP1-RA users could not be examined due to the low number of events.
In summary, the results of this large multinational cohort study and meta-analysis suggest that patients with type 2 diabetes newly treated with GLP1-RA were not at an increased risk of thyroid cancer compared with patients newly treated with DPP-4is. This study provides reassurance on the short-term safety of these drugs on thyroid cancer incidence, however, studies with longer follow-up are needed.
Footnotes
Acknowledgments
This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care. Parts of this material are based on data or information compiled and provided by the Canadian Institute for Health Information (CIHI). The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding, data sources, or CIHI. No endorsement is intended or should be inferred. The authors thank IQVIA Solutions Canada for use of their Drug Information File.
Authors’ Contributions
S.M.B.: conceptualization (supporting); interpretation (equal); methodology (equal); project administration (supporting); writing—original draft (lead); writing—critical review and editing (equal). L.C.L.: conceptualization (supporting); interpretation (equal); methodology (equal); formal analysis (support); writing—critical review and editing (equal). J.H.A.: formal analysis (lead); interpretation (equal); software (lead); validation (lead); visualization (lead); writing—critical review and editing (equal). T.H.B.: clinical expertise (equal); interpretation (equal); critical writing—review and editing (equal). L.H.: clinical expertise (equal); interpretation (equal); writing—critical review and editing (equal). M.H.-C.H.: formal analysis (support); interpretation (equal); software (support); validation (supporting); writing—critical review and editing (equal). C.T.-T.S.: formal analysis (support); interpretation (equal); software (support); validation (supporting); writing—critical review and editing (equal). M.C.-Y.C.: interpretation (equal); writing—critical review and editing (equal). Z.C.-J.C.: interpretation (equal); writing—critical review and editing (equal). E.C.-C.L.: funding acquisition; resources (equal); interpretation (equal); writing—critical review and editing (equal). S.H.: formal analysis (support); interpretation (equal); software (support); validation (supporting); writing—critical review and editing (equal). C.C.: interpretation (equal); writing—critical review and editing (equal). T.G.: interpretation (equal); writing—critical review and editing (equal). T.A.: interpretation (equal); writing—critical review and editing (equal). A.E.: interpretation (equal); writing—critical review and editing (equal). Z.B.: interpretation (equal); writing—critical review and editing (equal). M.T.: resources (equal); interpretation (equal); writing—critical review and editing (equal). S.B.: formal analysis (support); interpretation (equal); software (support); validation (supporting); writing—critical review and editing (equal). E.-Y.C: formal analysis (support); interpretation (equal); software (support); validation (supporting); writing—critical review and editing (equal). J.-Y.S.: resources (equal); interpretation (equal); writing—critical review and editing (equal). K.M.: resources (equal); writing—critical review and editing (equal). M.T.: formal analysis (support); interpretation (equal); software (support); validation (supporting); writing—critical review and editing (equal). R.L.: resources (equal); interpretation (equal); writing—critical review and editing (equal). H.L.G.: resources (equal); interpretation (equal); writing—critical review and editing (equal). Ø.K.: formal analysis (support); resources (equal); interpretation (equal); software (support); validation (supporting); writing—critical review and editing (equal). B.H.: conceptualization (supporting); methodology (equal); interpretation (equal); writing—critical review and editing (equal). A.P.: conceptualization (lead); resources (equal); methodology (equal); interpretation (equal); project administration (lead); supervision (lead); writing—critical review and editing (equal).
Author Disclosure Statement
A.P. reports participation in research projects funded by Alcon, Almirall, Astellas, AstraZeneca, Boehringer-Ingelheim, Novo Nordisk, Servier, and LEO Pharma, all regulator-mandated phase IV studies, all with funds paid to the institution where he was employed (no personal fees) and with no relation to the work reported in this article. E.C.-C.L. reports research funding outside the submitted work from Amgen, Pfizer, Sanofi, Takeda, Roche, IQVIA, but the grants with no relation to the current work. L.C.L. reports participation in research projects funded by Menarini Pharmaceuticals and LEO Pharma, all with funds paid to the institution where he was employed (no personal fees) and with no relation to the current work. J.H.A. reports participation in research projects funded by Novo Nordisk but with no relation to the current work. L.H. reports receiving consultancy fees from Bracco Suisse, Berlin-Chemie, Horizon, IBSA, Lundbeck, and Novo Nordisk with no relation to the work reported in this article. J.-Y.S. received grants from the Ministry of Food and Drug Safety, the National Research Foundation of Korea, and Pharmaceutical Companies, including Pfizer, Celltrion, and SK bioscience. No other relationships or activities have influenced the submitted work. Ø.K. reports participation in research projects funded by Bristol Myers Squibb, Novo Nordisk, and LEO Pharma, all regulator-mandated phase IV studies, all with funds paid to the institution where he was employed (no personal fees) and with no relation to the work reported in this article. H.L.G. reports previous participation (before 2020) in research projects and clinical trials funded by Novo Nordisk, GSK, AstraZeneca, and Boheringer-Ingelheim, all paid to her previous institution Oslo University Hospital (no personal fees) and with no relation to the work reported in this article. R.L. reported receiving grants from Sanofi Aventis paid to his institution outside the submitted work; and receiving personal fees from Pfizer outside the submitted work. R.L. and M.T. are employed at the Swedish Medical Products Agency, Uppsala, Sweden. The views expressed in this article do not necessarily represent the views of this Government agency. Z.B. is a current employee of AstraZeneca but was not an employee of AstraZeneca during the completion of this study. This current work has no relation to his employment with AstraZeneca. A.E., B.H., C.C., C.T.-T.S., E.-Y.C., K.M., M.T., M.C.-Y.C., M.T., M.H.-C.H., S.M.B., S.B., S.H., T.G., T.A., T.H.B., and Z.C.-J.C. declare no conflict of interest.
Funding Information
M.H.-C.H., C.T.-T.S., M.C.-Y.C., Z.C.-J.C., and E.C.-C.L. were supported in part by the Taiwan National Science and Technology Council (112-2628-B-006-003, 113-2628-B-006-009) and the Taiwan National Health Research Institutes (NHRI-11A1-CG-CO-04-2225-1). S.B., E.-Y.C., and J.-Y.S. were supported by a grant (RS-2024-00393167) from the Ministry of Food and Drug Safety of South Korea in 2024-28. S.M.B., L.C.L., J.H.A., T.H.B., L.H., S.H., C.C., T.G., T.A., A.E., Z.B., M.T., K.M., M.T., R.L., H.L.G., O.K., B.H., and A.P. declare no funding support for this project.
Supplementary Material
Supplementary Data