
Abstract
Objectives:
Cytologically indeterminate thyroid nodules (Bethesda class III or IV) carry a 10–40% risk of malignancy. Diagnostic lobectomies are frequently performed but negative surgeries incur unnecessary costs on the healthcare system, potential complications, and negative impacts on quality of life. Molecular tests (MTs) have been developed to reduce unnecessary surgeries. However, well-validated, high-performance MTs are often expensive, and their cost-effectiveness has not been studied in the Asian population. This study evaluates the rate of unnecessary surgery in the setting without MT (our current practice) and the cost-effectiveness of introducing a commercially available MT for the management of cytologically indeterminate thyroid nodules in a modernized city in Asia.
Methods:
Management decisions and outcomes of consecutive Bethesda III or IV thyroid nodules in a tertiary endocrine surgery center in Hong Kong were evaluated. Costs of health service provided by the public health system, which covers >90% of healthcare service in the city, were retrieved. A decision tree model was developed to compare the cost-effectiveness in avoiding unnecessary surgeries of current practice versus routine MT from a public healthcare provider’s perspective. In our current practice, MT was not available, and patients with indeterminate nodules received either upfront lobectomy, repeat fine needle aspiration cytology (FNAC), or active surveillance.
Results:
Over a 4-year period, 2157 FNACs were performed. After exclusion, 1957 FNACs were analyzed, and 18.6% were Bethesda III or IV. Thirty-six percent of these cytologically indeterminate nodules received upfront surgery, with 28% having malignancy in final pathology, that is, 72% of surgeries were unnecessary. Routine MT could reduce 82 unnecessary surgeries/year, 26% more than current practice. Routine MT resulted in an incremental cost-effectiveness ratio of Hong Kong dollar (HKD) 49,102 (US dollar [USD] 6314) per unnecessary surgery. Sensitivity analysis showed test cost of MT contributed significantly to incremental cost-effectiveness ratio. Lowering the commercial price of MT to below HKD 8044 (USD 1031) would render routine MT cost-saving.
Conclusion:
Currently, a high rate of unnecessary surgeries is being performed for cytologically indeterminate thyroid nodules. MT was more effective in reducing unnecessary surgeries than current practice, but at a higher cost. MT will become cost-saving if the test cost could be lowered.
Introduction
Thyroid nodules affect up to 65% of the general population. 1 Ultrasound (USG) is the initial investigation of choice and guides the decision of fine needle aspiration cytology (FNAC) in suspicious nodules. 2 In the Bethesda System for Reporting Thyroid Cytopathology, 3 classes III and IV are considered indeterminate in nature. The observed risk of malignancy of indeterminate nodules varies widely across institutions and ranges from 10% to 40%. 3 Indeterminate cytology presents a diagnostic challenge to clinicians and often leads to diagnostic lobectomies. In clinical practice, a significant proportion of these cytologically indeterminate nodules that received surgery were actually benign, meaning surgery was unnecessary. Unnecessary lobectomies may subject patients to surgical risks and create substantial emotional stress and anxiety to patients. They also contribute to significant costs to the healthcare system. The problem is expected to grow owing to the increasing rates of asymptomatic, incidental thyroid nodules being diagnosed from high-resolution imaging. 4,5
As a result, molecular tests (MTs) have been developed and widely used in Western countries to better predict the risk of malignancy in indeterminate nodules and guide decisions on surgery. MT was shown to improve the rate of malignancy in diagnostic lobectomies, or in other words, reduce unnecessary surgery. 6,7 ThyroSeq v3 is one commercially available MT that has been validated by a large number of studies. 8 –11 Previous studies from Western countries have shown ThyroSeq to be effective in reducing unnecessary surgeries, and also cost-effective in the overall management of indeterminate thyroid nodules. 12 –15
Despite the benefits of MT shown in studies from the Western countries, well-validated MTs are not widely available in Hong Kong, and the test costs are not covered by the public healthcare system. Furthermore, there have been no previous studies that investigated the effectiveness and cost-effectiveness of using MTs in an Asian population. Notably, it is known that in the Asian population, there is a trend to adopt a more conservative approach for indeterminate thyroid nodules, with a much lower rate of resection when compared to the Western countries (37.6% vs. 51.3%). 16 Cancer incidence also varied between population and institutions due to differences in screening thresholds and regional practices. 3,17 Differences in test cost, cancer detection rates, and choice of management for indeterminate thyroid nodules, that is, direct lobectomy, repeat FNAC, or active surveillance, exist in Asia and could significantly affect the rates of unnecessary surgery, hence the effectiveness and cost-effectiveness of using MT in the overall management of indeterminate thyroid nodules. Considering these limitations and knowledge gaps, we conduct the first cost-effectiveness study on the routine use of a high-performance MT—ThyroSeq V3 in an Asian population for the management of cytologically indeterminate thyroid nodules versus that of our current practice in which MT is not available, and patients are managed with either lobectomy, repeat FNAC, or surveillance.
Methods
This study followed the principles in the Declaration of Helsinki and was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (UW 24-436).
The study comprised two parts. In the first part, we evaluated the thyroid FNAC results and clinical outcomes of indeterminate Bethesda III and IV thyroid nodules from January 2018 to December 2021 at a tertiary endocrine surgery center in Hong Kong, during which MT was not available. Amongst these indeterminate nodules, the rates of surgery, repeat FNAC, or active surveillance were evaluated. The rate of malignancy among operated nodules was charted. Based on this information, probability rates were established for building the base case for cost-effectiveness analysis.
The second part of the study is a cost-effectiveness analysis from a public healthcare provider’s perspective in Hong Kong, where a decision tree representing the management strategies for a low-risk, cytologically indeterminate thyroid nodule was developed. The cost-effectiveness of routine MT versus current practice (no MT) in the management of Bethesda III or IV nodules was compared.
Evaluation of current practice of indeterminate thyroid nodules in the absence of MT
All FNACs performed by endocrine surgeons at our institution between January 2018 and December 2021 were evaluated. The FNACs were performed under ultrasound guidance and prepared with a standardized method using smears fixed in 95% alcohol and rinsed with 50:50 alcohol preparation, followed by cell block preparation, staining, and microscopic examination by a pathologist. Cytology findings were reported based on The Bethesda System for Reporting Thyroid Cytopathology 2017, which was the most updated version at the time. All cytology was interpreted and endorsed by the same team of cytopathologists at the same tertiary referral hospital. They are highly experienced in the regular reporting of thyroid cytopathology for at least 5 years and adhere to the Bethesda system in all reports. Nonthyroidal FNAC specimens and patients lost to follow-up were excluded. Indeterminate nodules were defined as Bethesda class III (atypia or follicular lesion of undetermined significance) and class IV nodules (follicular neoplasm, or suspicious for follicular neoplasm). Among indeterminate nodules, the clinical management and eventual outcomes were reviewed from the electronic health records to determine the rate of malignancy and the rate of unnecessary surgery in our locality. Unnecessary surgery was defined as surgery performed with a final benign surgical histopathology.
In our current practice, patients with Bethesda III nodules were counseled in detail on the probabilities of malignancy according to the Bethesda guidelines, 3 and offered the options of a diagnostic lobectomy or a repeat FNAC. Since MT is not available, it is not offered to our patients. For Bethesda IV nodules, patients were also counseled in detail on the probabilities of malignancy 3 and would be offered a diagnostic lobectomy. Repeating FNAC was not our usual practice for Bethesda IV nodules but may be performed upon request from patients after detailed discussion on the rare occasion. In any scenario when patients refuse surgery, a follow-up clinic visit and USG would be arranged every 6 months.
Cost-effectiveness analysis
Base case
The base case is a patient with a solitary thyroid nodule with the largest diameter >1 cm and <4 cm, with indeterminate FNAC cytology, defined as either Bethesda class III or IV, but otherwise low risk (Table 1). The nodule has no high-risk ultrasonographic features, for example, irregular borders, taller-than-wide, presence of punctate echogenicity, extrathyroidal extension, or suspicious enlarged cervical lymph nodes. 2,18 The patient has had no previous neck irradiation or any known genetic predisposition to thyroid cancer.
Base Case Characteristics
Performance of ThyroSeq v3
The MT utilized in this decision analysis was ThyroSeq v3. According to a previous prospective, multicenter, blinded study, ThyroSeq v3 has a positive predictive value (PPV) of 66% and negative predictive value (NPV) of 97% at a prevalence of 28%. 10 From the first part of our study, the local prevalence of malignancy amongst operated Bethesda III and IV nodules was found to be 28%. Since the positive and negative predictive values are directly related to the prevalence, at the same disease prevalence of 28%, we utilized a test PPV of 66% and NPV of 97% and calculated the empirical base case test sensitivity and specificity to be 91% and 86% respectively.
Decision tree model
The decision tree model developed for cost-effectiveness analysis is shown in Figure 1. An indeterminate Bethesda III/IV nodule would be approached with either the use of routine MT (MT arm) or without an MT as per the current practice at our institution (current practice arm). The cycle length was 1 year. For this study, the management and follow-up duration were set to be complete at 2 years for both arms.
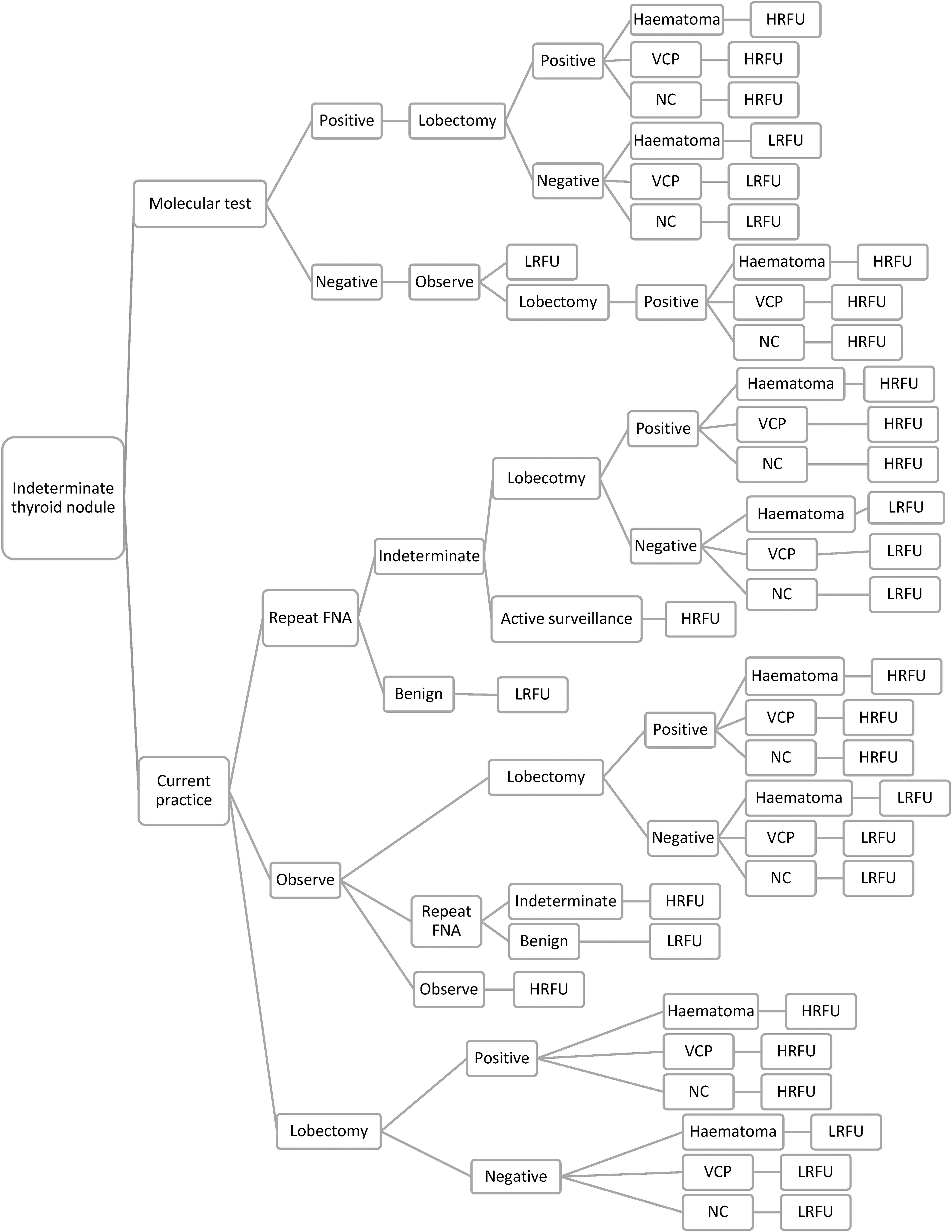
Decision tree denoting the management strategy of a patient with an indeterminate thyroid nodule. LRFU, low-risk follow-up; HRFU, high-risk follow-up; NC, no complications; VCP, vocal cord palsy.
Patients in the MT arm would either receive a diagnostic lobectomy if test-positive or continue to be observed and followed up yearly if test-negative (low-risk follow-up). It was assumed that the small percentage of false negative nodules (cancers missed by MT) would show progression within 2 years of clinical follow-up and hence being picked up and managed with lobectomy.
Patient in the current practice arm would either undergo a diagnostic lobectomy, repeat FNAC, or active surveillance. A repeat FNAC showing benign cytology would be observed (low-risk follow-up); a repeat FNAC showing malignancy would receive surgery; a repeat FNAC showing indeterminate cytology would either receive surgery or active surveillance (high-risk follow-up). Patients who opted for active surveillance would be followed up every half-yearly with ultrasound, clinical consultation, and repeat FNAC when indicated (high-risk follow-up) and managed with surgery if indicated. The decision for surgery would be an informed and joint decision between the doctor and the patient after a detailed discussion.
Patients who received lobectomy will be managed according to the final pathological diagnosis; benign lesions would be followed up yearly (low-risk follow-up), while malignant lesions would be followed up every half-yearly (high-risk follow-up). Potential surgical complications of postoperative hematoma requiring evacuation, and vocal cord palsy, were also included in the decision tree, as they were the major complications from lobectomy that would translate to extra costs.
Probability and cost estimation
Transition probabilities and costs for health states used in this cost-effectiveness analysis based on the first part of the study and literature are summarized in Table 2. Since the public healthcare system in Hong Kong covers >90% of health services in the city, cost-effectiveness analysis was performed from a local public healthcare provider’s perspective, that is, all healthcare costs related to indeterminate thyroid nodules would be funded by the government. Costs were calculated in Hong Kong dollars (HKD) (conversion to US dollars [USD] with a factor of 7.8) through a microcosting methodology, whereby each monetized unit costs for each resource consumed during the evaluation and management of an indeterminate thyroid nodule were captured. Data on unit costs were collected from the 2019 Hong Kong Special Administrative Region Government Gazette and Hospital Authority Ordinance. Unit costs utilized for analysis are summarized in Table 3. The total costs incorporated in each management option (MT vs. current practice) were calculated from the cost-effectiveness model as denoted by the decision tree (Fig. 1) based on the relative probabilities (Table 2) of each management option and subsequent events. In short, the costs of the current practice arm would follow the three management options—repeat FNAC, observation, and lobectomy. The total cost of the repeat FNAC option follows the decision iterated above regarding results of benign, indeterminate, and malignancy. The same applies to the observation option, where follow-up frequencies and costs depend on high- and low-risk situations. The total cost of lobectomy included costs of preoperative laryngoscopy, the operation itself and costs of managing complications, pathology review of specimen, and 2 days of hospitalization, whereas follow-up costs included specialist outpatient follow-up visits, where each patient would receive a bedside ultrasonography of the neck. The total cost of the MT arm included the test cost, the cost of subsequent lobectomy if tested true positive and related costs from complications and follow-up as mentioned above; costs of follow-up if tested true negative; and costs if tested false negative and patient requiring lobectomy when disease progression is noted in follow-up visits.
Probability Values for Decision Tree Analysis
Steward, et al. Performance of a Multigene Genomic Classifier in Thyroid Nodules with Indeterminate Cytology, a Prospective Blinded Multicenter Study. JAMA Oncology. 2019; 5 (2):204–212.
Local data from Queen Mary Hospital, Hong Kong.
Surgical Outcomes Monitoring and Improvement Programme (SOMIP) Report, vol 15, July 2022-June 2023, Hong Kong Hospital Authority.
FNAC, fine needle aspiration cytology.
Health Cost Calculation
HKD, Hong Kong dollar; USD, US dollar.
Cost-effectiveness analysis
Cost-effectiveness analysis was performed with the decision tree model utilizing fixed base case parameters as listed in Table 1, with microsimulation of 10,000 patients over a 2-year time horizon. A 2-year time horizon was chosen to examine the early impacts of MT on costs and unnecessary surgery reduction. Mean costs and transition values for each management strategy were determined. Model development and statistical analysis were executed and analyzed with Amua v0.3.0, 2020, and RStudio version 2023.12.1 + 402. The unit of benefit was the percentage of unnecessary surgeries avoided. Unnecessary surgery for indeterminate thyroid nodules was defined as surgery performed with a benign final histopathology. The primary outcome was the incremental cost-effectiveness ratio (ICER), calculated by:
Sensitivity analysis
Monte Carlo probabilistic sensitivity analysis was executed with 10,000 simulations to derive 95% uncertainty intervals. One-way sensitivity analysis was performed on all probabilities and costs to determine the contribution of each variable to the unit of benefit. Threshold cost analysis and cost-effectiveness acceptability analyses were carried out to determine the contribution of the MT cost in affecting the total cost of each of the specific management strategies, that is, MT or current practice.
Results
Current practice trends and FNAC results
A total of 2175 FNACs were performed by our endocrine surgery unit between January 2018 and December 2021. After the exclusion of 30 nonthyroidal FNACs, and 188 that were lost to follow-up, 1957 thyroid FNACs were reviewed. There were 365 (18.6%) nodules having a Bethesda III or IV cytology. Table 4 shows the baseline characteristics of the Bethesda III and IV nodules. The median age was 62 (51–71), the majority were found in female patients (80%). The median largest diameter was 2 cm (1.4–3 cm), and none of the nodules were <1 cm. Bethesda III nodules accounted for the majority of indeterminate nodules (91.2%). The majority of nodules were either ACR TIRADS 2 3 (29.2%) or 4 (29.7%) on USG. There were TIRADS 1 and 2 nodules that were biopsied due to initial plans for thermal ablation, large size (≥3cm), or patient request. Table 5 describes the management of these indeterminate nodules: 36% of these patients with indeterminate Bethesda III or IV nodules opted for surgery, while 42% of them opted for repeat FNAC, and 22% opted to observe the lesion on ultrasound (Table 5). Out of the Bethesda III and IV nodules with upfront lobectomy performed, only 28% of them were malignant on final histopathology (Table 6). In the case that FNAC was repeated, 29% of the nodules were reclassified as benign, while 27% were still indeterminate on the second FNAC. Of the 174 patients who eventually received surgery in the cohort, the overall pathological malignancy rate was 28%, meaning that the rate of unnecessary surgery (benign pathology but received surgery) was 72% in our locality.
Characteristics of the 365 Thyroid Nodules with Indeterminate Cytology (Bethesda III or IV) That Were Analyzed
American College of Radiologist Thyroid Imaging Reporting and Data System.
Initial Management of Bethesda III and IV Thyroid Nodules
Rate of Malignancy After Upfront Lobectomy by Bethesda Class
Cost-effectiveness analysis
Based on the decision tree model representing 2 years of management strategy for cytologically indeterminate thyroid nodules in our locality (Fig. 1) and utilizing the prevalence and probabilities of different clinical scenarios from our cohort, the current practice (no MT) resulted in a mean cost of HKD 33,539 (USD 4313) and 0.64 mean effectiveness per unnecessary surgery avoided (Table 7). On the other hand, routine MT resulted in a higher mean effectiveness of 0.90 at a mean cost of HKD 46,066 (USD 5906). Routine MT resulted in an incremental effectiveness of 0.26 over current practice in avoiding unnecessary surgery (26% more unnecessary surgeries avoided). If we assume all patients diagnosed with indeterminate thyroid nodules over the study period received routine MT, MT could have reduced 82 unnecessary surgeries per year, versus 58 per year by current practice. All in all, routine MT incurred a higher cost but was more effective in reducing unnecessary surgeries. Calculated from the base case, the ICER of MT was HKD 49,102 (USD 6314) per unnecessary surgery avoided.
Cost-Effectiveness Analysis Based on Base Case
ICER, incremental cost-effectiveness ratio.
Sensitivity analysis
Tornado plot (Fig. 2) shows how different variables contribute to the cost-effectiveness model on one-way sensitivity analysis, with the range of the parameters modified for sensitivity analysis summarized. Test cost, disease prevalence (PV), and rate of repeat FNAC (rFNA) were the three variables that contributed to the ICER of using MT. Supplementary Figure S1a–d further shows how each of these variables may affect the cost, effectiveness of avoiding unnecessary surgery, and ICER of MT over current practice respectively. The total cost of routine MT reduces with a reduction in test cost (Supplementary Fig. S1a). At a test cost of HKD 8044 (USD 1031), routine MT becomes cost-neutral when compared to the current treatment arm (Supplementary Fig. S1a). Routine MT becomes cost-saving if the test cost is lower than HKD 8044 (USD 1031). The effectiveness of avoiding unnecessary surgery increases with increased disease prevalence (Supplementary Fig. S1b). ICER increases when test cost, PV, or rate of rFNA increases (Supplementary Fig. S1c). An overall downward trend of ICER of MT was seen with longer-term follow-up for 10 years (Supplementary Fig. S1c). The higher the upfront surgery rate, the lower the ICER, and vice versa. At an upfront surgery rate of ∼68%, MTs would become cost-neutral as current practice (Supplementary Fig. S1d).
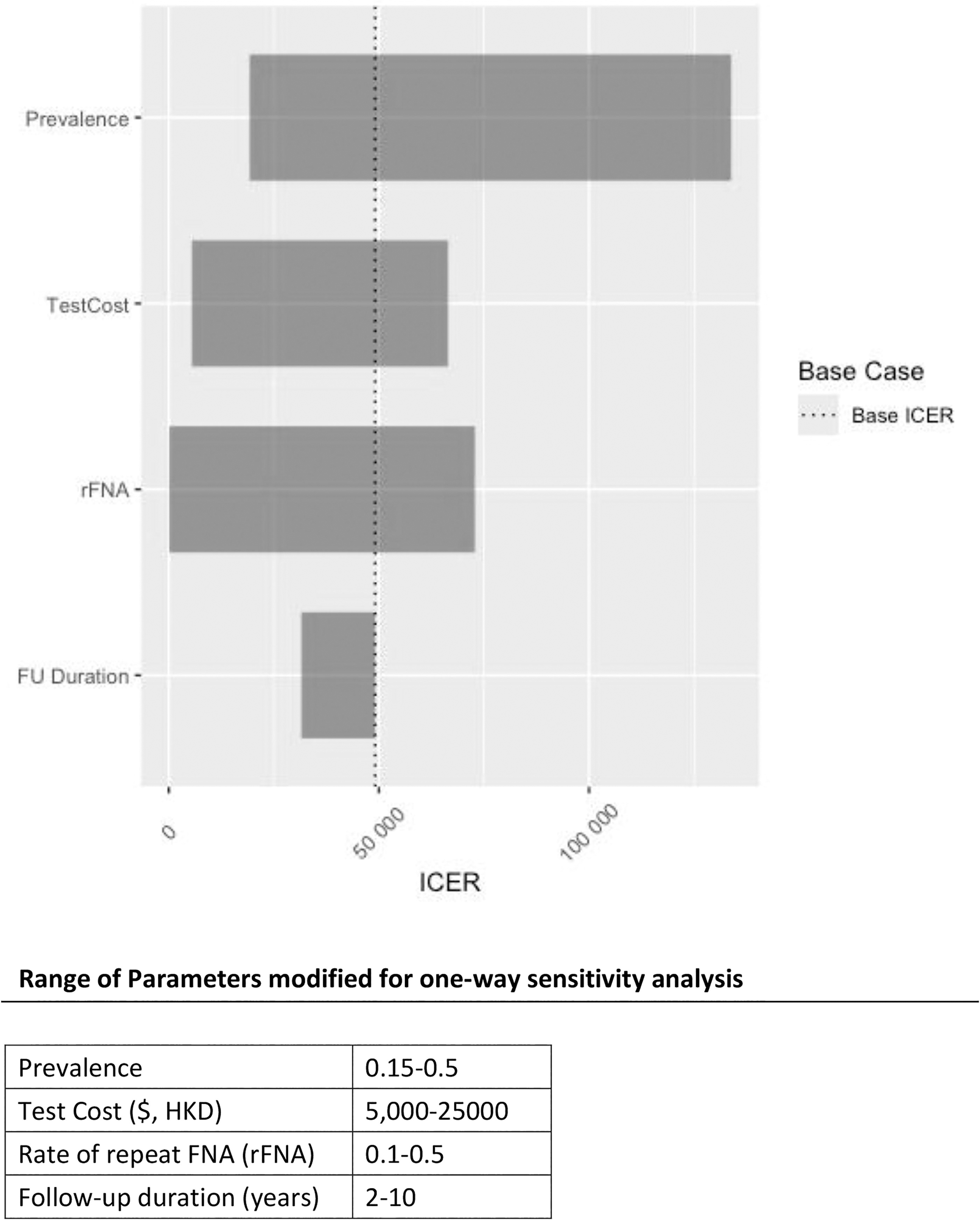
Tornado plot showing how different variables contribute to incremental cost-effectiveness ratio (ICER) on one-way sensitivity analysis. Molecular test cost, cancer prevalence, and rate of repeat FNA (rFNA) were the three major variables that contributed to ICER of using MT; follow-up (FU) duration had less bearing on ICER. The range of parameters varied is shown in the table.
Results from Monte Carlo probabilistic sensitivity analysis performed with 10,000 microsimulations are presented as a cost-effectiveness scatterplot in Figure 3. Each of the 10,000 trials represents a random sample of parameters from the probability and cost distributions and compares the MT arm with the current treatment arm as shown. The incremental cost and incremental effectiveness of probabilistic sensitivity analysis were recalculated as shown in Table 8. The resultant ICER on probabilistic sensitivity analysis was HKD 36,835 (USD 4722) per unnecessary surgery avoided. MT was superior in the incremental effectiveness gained; it was able to reduce unnecessary surgery by 27.6%.
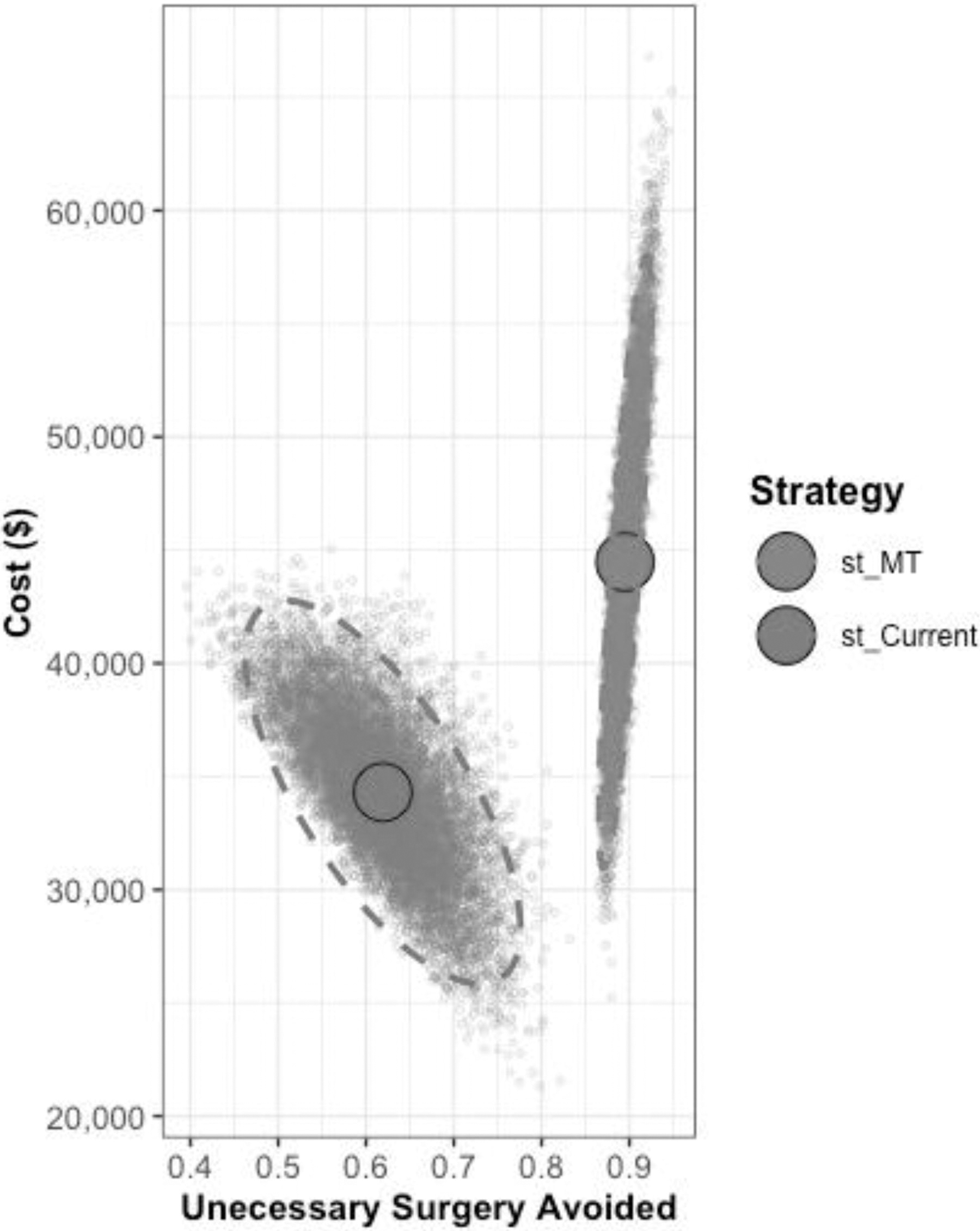
Probabilistic sensitivity analysis generated from 10,000 microsimulations. Costs expressed in Hong Kong dollars. Cluster on the left represents current practice strategy (st_Current); cluster on the right represents molecular test strategy (st_MT).
Incremental Cost-Effectiveness Ratio Calculated from Probabilistic Sensitivity Analysis
Supplementary Figure S2 shows the cost-effectiveness acceptability analysis that varies at different willingness-to-pay thresholds. Since the total cost of lobectomy was HKD 58,432 (USD 7941), if we assume that the government would be willing to pay at least the same amount for MT as for a lobectomy in order to avoid unnecessary surgery, routine MT (ICER HKD 49,102 [USD 6314]/unnecessary surgery avoided) would be cost-effective with close to 75% certainty.
To further examine the role of MT in other Asian countries, sensitivity analysis was carried out based on Japanese data. Japan was chosen because the information from available literature was most detailed for decision tree construction. The details of health costs and probability states, and the decision tree for Japan can be found in Supplementary Tables S2 and S3 19 –22 and Supplementary Figure S3. Consistently, in Japan where the surgery rate was low (34%), MT is still more effective than current practice in reducing unnecessary surgery (effectiveness 0.89 vs. 0.75), at a higher total cost and ICER (Supplementary Table S4).
To further examine how applying MT at different stages influences its effectiveness and ICER in reducing unnecessary surgery, a third strategy was tested: selective MT (Supplementary Fig. S4). In the selective MT approach, a routine repeat FNA is first performed. Patients with benign cytology from the repeat FNA are observed, while patients with persistently indeterminate cytology proceed to MT. The findings consistently show that the selective MT strategy is more effective (0.94) than current practice in reducing unnecessary surgery, although at a higher cost. The ICER of the selective MT strategy is HKD 19,418 (2489 USD), which is lower than that of the routine MT strategy.
Discussion
To the best of our knowledge, this is the first cost-effectiveness analysis in an Asian population on the use of a commercially available multigene MT for Bethesda III and IV indeterminate thyroid nodules. MT has been shown to be cost-effective in the overall management of indeterminate thyroid nodules, 12 –15 and negative MT can reduce the rate of surgery. 23 These findings were primarily based on results from North America, where commercially available MTs were developed and tested. A previous meta-analysis has shown significantly lower surgery rate for indeterminate thyroid nodules in the East (Asia, Middle East) when compared with the Western countries (USA, South America) (37.6% vs. 51.3%). 16 Focusing on Asian data versus North American data (Supplementary Table S1 19,24 –40 ), surgery rate for indeterminate nodules in Asian countries was consistently <40%, with a pooled rate of 24.2%; whereas for data from the USA (where commercial MTs were developed), surgery rates were mostly >50%, with a pooled rate of 52.4%. Lower surgery rates and different cancer prevalence 17 could affect unnecessary surgery rates, or downplay the role of MT, 17 rendering it necessary to carefully examine the effectiveness and cost-effectiveness of MTs in an Asian setting. Notably, the surgery rate for indeterminate thyroid nodules at our center (36%) was comparable to the rates in other Asian countries and lower than the Western countries. Nevertheless, our final rate of unnecessary surgery of 72% was still very high. This highlights the need for a better risk stratification tool, for example, routine use of MT. Despite already having a lower resection rate in our current practice, the use of MT could effectively reduce unnecessary surgery by 26% more than our current practice. Probabilistic sensitivity analysis yielded consistent results, showing MT is more effective than current practice in reducing unnecessary surgery at a wide range of simulations, but at a higher cost.
Routine MT was found to be more expensive than current practice in our study. Notably, the commercial price of MT was shown to greatly affect cost-effectiveness in a sensitivity analysis. From a public healthcare provider’s perspective, MT would become cost-neutral when its commercial price is lowered to HKD 8044 (USD 1031), that is, it could reduce unnecessary surgery by 26% without additional costs. If the commercial price could be further lowered, MT could theoretically reduce healthcare budgets, and at the same time benefit a vast number of patients. Unfortunately, current well-validated MTs were developed in the United States and require well-preserved FNAC specimens to be sent overseas for testing. Expectedly, significant costs are attributed to shipping and administration. Furthermore, these tests were not yet validated in an Asian population. To address these issues, it would be valuable if a local, high-quality MT tailored to Asian thyroid cancer genomics could be developed and made available at a lower price. Another important finding would be that the cost-effectiveness of MT increases with the rate of upfront surgery (Supplementary Fig. S1d). Without lowering the current MT price, MT is probably more likely to have lower ICERs in places with higher surgery rates (e.g., North America).
Interestingly, the application of MT at different stages in the management pathway influences the overall costs. In the third strategy tested—the selective MT strategy (Supplementary Fig. S4)—MT is performed only for patients with persistently indeterminate cytology after repeat FNA, MT is consistently more effective in reducing unnecessary surgery than current practice, albeit at a higher cost. The ICER for selective MT is lower than that for routine MT, because of the reduced number of patients requiring MT. Overall, while applying MT at different stages can reduce unnecessary surgeries, it does come at a higher cost.
MT could potentially allow for better risk stratification for patient selection for surgery and thus provide a more accurate and personalized treatment. This is important because thyroidectomy, although in general safe in expert hands, is not without risks and morbidities, for example, hematoma requiring evacuation, recurrent laryngeal nerve injury, wound infection, and scarring voice change, and hence quality of life impairment. 41 –43 These postoperative impacts can incur costs at both the personal and societal levels. We should note that these indirect costs were not accounted for in our study, and therefore, the incremental cost and ICER would probably be an overestimation.
To ensure an accurate reflection of our current practice, we rigorously reviewed the treatment choices, clinical outcomes, and malignancy rates of our patients with indeterminate cytology within our current practice (without MT). We utilized decision and outcome probabilities from our cohort in the decision tree to simulate a real-life clinical scenario. The other unique feature of our decision tree model was the inclusion of all management options following an indeterminate thyroid cytology result, that is, lobectomy, repeat FNAC, surveillance, or MT, as recommended by well-established guidelines and adopted in real-world practice. 17 Different from previous studies that omit the option of repeating FNAC, 9,10,19 we believe our approach could better simulate the real-world scenario faced by clinicians in their day-to-day practice.
It is important to note that the ATA guidelines did not recommend repeat FNAC for Bethesda IV nodules. This was also the case in our practice, where repeat FNAC was not the primary recommendation for our patients with Bethesda IV nodules. However, among the patients with a Bethesda IV nodule who refused surgery, a small subset of patients (9%) would request for and later receive, a repeat FNAC after detailed discussion and informed consent. To reflect the real-life pragmatic scenario, we still included the arm of repeat FNAC for Bethesda IV nodules in our decision tree, albeit this being an option having a low probability state.
Nevertheless, the results of this study have to be interpreted with the following limitations in mind. First, while ThyroSeq v3 has been well-validated in the Western countries, its performance has not yet been validated in an Asian population. Whether its notable effectiveness can be replicated in Asia remains unclear. We evaluated the influence of the performance of ThyroSeqV3 on the ICER by varying cancer prevalence, which affects both the positive and negative predictive values. However, the effect of different intrinsic sensitivity and specificity on ICER was not evaluated, as this would require an evaluation of another MT and is beyond the scope of this study. Furthermore, potential biases may exist regarding the reported test accuracy and performance of MTs. Second, our study is designed and contextualized to the Hong Kong healthcare system. Given that healthcare costs vary amongst countries, we remain cautious with generalizability. Therefore, a sensitivity analysis was carried out to examine the cost-effectiveness of MT in Japan. The results were consistent, in which MT has a higher effectiveness in reducing unnecessary surgery, despite the low surgery rate (34%) in Japan, at a higher cost and ICER. However, we acknowledge that this sensitivity analysis was largely limited by data availability and quality, including the rates of repeating FNA, and rate of surgery following initial observation, the baseline characteristics and size of nodules, and local healthcare costs. Consequently, we developed a simplified decision tree with the omission of the repeat FNA arm. This may have contributed to a lower overall surgery rate, and together with a lower total cost of lobectomy, may explain the higher ICER in Japan. Dedicated studies would be needed to fully ascertain the cost-effectiveness of MT in other Asian countries. Third, our model did not address indirect costs associated with lobectomy, which may lead to the underestimation of lobectomy costs, and hence an overestimation of ICER. Sociopsychological costs such as patients’ emotional stress, economical or productivity loss from being away from work as a result of committing to surgery, and money spent on care outside of the medical setting were not accounted for. This may result in an overestimation of the incremental cost (HKD 12,527 [USD 1606]) and ICER of MT. Additionally, the impact on quality of life as a result of a change in clinical decision due to MT was not addressed in this study. Currently, there is a lack of literature addressing the differences in quality-adjusted life years between patients with indeterminate thyroid nodules who did or did not receive MT. Future data on this matter will enable a cost-utility analysis of using MT. Moreover, since the primary aim of our study was to evaluate the early cost impact of MT as a diagnostic adjunct, we employed a 2-year time horizon for cost analysis. Although extending the follow-up duration to 10 years reduced the ICER of MT in sensitivity analysis, there is currently no consensus on the recommended long-term follow-up for MT-negative patients. Accurate simulation of the long-term cost-effectiveness of MT will require more future literature support. For instance, annual follow-up beyond 5 years for MT-negative patients may be excessive and spuriously inflate cost estimations on MT. Uncertainties also exist for the long-term follow-up frequencies for the patients who were purely observed in the current practice arm. Fourth, it is assumed that all MT-negative patients would not choose to undergo surgery in the current study. Deviation from this assumption in the real world would affect the cost-effectiveness of MT. However, we believe such deviation would likely be minimal in an otherwise low-risk nodule as defined in the base case. Actual deviation could only be assessed if routine MT is made available in our locality in the future. Last, the base case represents a simplified clinical situation where a single, small- to moderate-sized indeterminate thyroid nodule is the only clinical concern. There are real-life situations that are not adequately represented by the base case. For example, patients may have other indications for surgery, such as significant compressive symptoms from a retrosternal goiter, or concomitant thyroid cancer in the same lobe. Moreover, occult papillary microcarcinoma may sometimes be found in the same thyroid lobe when surgery was performed.
Conclusion
Thyroid nodules with indeterminate cytology were common. Despite a more selective approach for surgery in our locality and Asia, there was still a concerningly high rate of unnecessary surgeries being performed for these nodules. Under this setting, a MT with good performance can potentially reduce the rate of unnecessary surgery, although at a higher cost. Lowering the test cost could potentially render routine MTs both cost-saving and beneficial to the public.
Footnotes
Authors’ Contributions
All authors approved the final version of the article and agreed to be accountable for all aspects of the work. M.H.M.F.: Conception, data collection, data analysis, and article writing. C.T.: Data collection, data analysis, and article writing. G.W.K.: Data analysis. T.H.C.: Data collection. Y.L.: Data collection. D.T.W.L.: Data collection. C.K.H.W.: Conception, article review, and editing. B.H.H.L.: Conception, article review, and editing.
Data Availability
Datasets generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Author Disclosure Statement
The authors have no related conflicts of interest to declare.
Funding Information
The authors received no sponsorship. Equipment was provided by the authors’ institution.
Supplementary Material
Supplementary Data
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4