
Abstract
Background:
The international medullary thyroid carcinoma (MTC) grading system (IMTCGS) has been proposed as an independent tool to predict disease-specific survival (DSS), distant metastasis-free survival (DMFS), and locoregional recurrence-free survival (LRFS). We aimed to evaluate the performance of IMTCGS in our series of sporadic MTCs and to compare its predictive power with conventional prognostic factors.
Methods:
In a retrospective cohort study, we evaluated data from 314 patients with sporadic MTC, all managed at the Pisa University Hospital. We divided patients according to the extent of the disease at diagnosis into localized (183/314, 58.3%) (confined to the thyroid), regional (100/314, 31.8%) (limited to the neck, involving surrounding thyroid tissues and/or regional lymph nodes), and distant (31/314, 9.9%) (distant metastases) disease. Data about somatic mutations were available in 212/314 (67.5%) patients. Expert pathologists differentiated high- and low-grade tumors.
Results:
According to the IMTCGS, 115/314 (36.6%) had high- and 199/314 (63.4%) patients had low-grade tumors. Patients with high-grade tumors showed higher preoperative calcitonin levels compared with low-grade (542 vs. 76 pg/mL, p < 0.01) as well as larger tumor size (2.3 vs. 1.1 cm, p < 0.01) and more frequent multifocality (22.6 vs. 12.1%, p = 0.01), minimal extrathyroidal extension (30.4 vs. 9.5%, p < 0.01), and lymph node metastases (63.5 vs. 27.6%, p < 0.01). Overall, patients with high-grade showed lower DSS, LRFS, and DMFS (p < 0.01). Grouping the whole cohort according to different disease extent at diagnosis, only in the case of localized disease, patients with high-grade tumors had significantly lower LRFS compared with low-grade. Similarly, in the other subgroups, we did not identify any difference in DSS, LRFS, and DMFS. Moreover, in the case of RET aggressive mutations, no differences in DSS, LRFS, and DMFS were observed between high- and low-grade tumors.
Conclusions:
We confirmed the usefulness of IMTCGS in predicting DSS, LRFS, and DMFS. However, it finds the best utility in patients with a lower risk of recurrence and mortality, identifying those rare cases with more aggressive clinical behavior. Conversely, when laterocervical lymph nodes (N1), distant metastasis (M1), or RET mutations, particularly M918T or indels, are already present at diagnosis, the role of IMTCGS in predicting DSS, DMFS, and LRFS becomes less relevant.
Introduction
Medullary thyroid carcinoma (MTC) is a neuroendocrine tumor, arising from thyroid C cells producing calcitonin (Ct). It can occur sporadically or be inherited as part of multiple endocrine neoplasia type 2 syndrome (MEN2), in case of germline RET mutation. In sporadic cases, somatic RET mutations are present in about 50% of all cases and more than 85% of advanced ones. 1,2
In patients with MTC, disease-specific survival (DSS) is reported to be 89% and 81% at 5 and 10 years, respectively. 3 One of the main DSS determining factors is the disease extent at diagnosis. In patients with disease confined to the thyroid gland (localized disease), to the neck (i.e., tissues surrounding the thyroid gland and/or regional lymph nodes) (regional disease), and with distant metastases (metastatic disease), 10-years DSS is reported to be 95.6%, 75.5%, and 40%, respectively. 4 Moreover, patients with more advanced disease extent at diagnosis show worse local recurrence (LRFS) and distant metastasis-free survival (DMFS). 5,6
Beyond disease extent at diagnosis, also RET status in sporadic MTC cases is a recognized predictor of prognosis. 7,8 Particularly, the presence of RET M918T or indels mutations is associated with worse outcomes. 9,10
Very recently, a grading system based on histological features has been proposed to better characterize the prognosis of MTC patients at diagnosis. 11 A two-tiered international MTC grading system (IMTCGS) was built upon retrospective data collected in several centers, categorizing tumors as low- and high-grade. According to the IMTCGS, the authors defined high-grade tumors in case of the presence of at least one of the following criteria: mitotic index ≥ 5 per 2 mm2, Ki67 proliferative index ≥ 5%, or tumor necrosis. At variance, low-grade tumors were defined in the absence of all of them. IMTCGS was shown as a powerful predictor of adverse outcomes in patients with MTC, regardless of disease extent at diagnosis 11 and also RET status. 12 However, despite its role in predicting outcome of MTC is widely accepted, 13 –17 few data are available regarding its application in the management of sporadic MTC in clinical practice.
This study aimed to evaluate in a large monocentric series of sporadic MTCs the performance of the international grading system and its clinical usefulness according to different disease extents at diagnosis and RET status.
Methods
Patients
We retrospectively evaluated 314 consecutive patients with sporadic MTC, registered in a prospectively maintained database who performed surgical treatment at the Endocrine Surgery Unit between 2000 and 2018 and followed at the Endocrine Unit, before and after surgery, at the Pisa University Hospital, Italy. The data lock of the study was January 2024. All cases were confirmed to be sporadic MTC since in our institution germline RET mutation analysis is performed as standard of care in all patients with confirmed histology of MTC.
Patients were subgrouped based on disease extent at diagnosis. The study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the local Ethical Committee (CEAVNO-Comitato-Etico-Area-Vasta-Nord-Ovest) (prot. number 14387 and 57877). In addition, all patients gave their informed consent for the use of their data for scientific purposes as required by the University Hospital’s policy.
Serum Ct assay
Serum Ct was measured in our laboratory in all patients at each clinical evaluation. Throughout the study period (2000–2024), we utilized three different assays. From January 2000 to September 2013, an immunoradiometric assay was employed (IRMA) (ELSA-hCt, CIS, Gif-Sur-Yvette, France) with an analytical sensitivity of 2 pg/mL and reference values up to 10 pg/mL for both sexes. From September 2013 to December 2020, we used a chemiluminescent immunometric assay (CLIA) (Immulite, Siemens Healthcare Diagnostic Products Ltd., Lianberis, Gwynedd LL55 4EL, UK), with an analytical sensitivity of 2 pg/mL and reference values up to 18.2 pg/mL for males and 11.5 pg/mL for females. Finally, from January 2021 up to the study data lock, we used an ultrasensitive CLIA assay (Calcitonin II-Gen, DiaSorin LIAISON) with an analytical sensitivity of 1 pg/mL and normal reference values, after accurate comparison with the previous assay, adjusted to 18.2 pg/mL for males and 11.5 pg/mL for females.
Histology
The histological diagnosis of MTC was made on hematoxylin and eosin sections from formalin-fixed paraffin-embedded blocks by two expert pathologists, blinded to clinical data, according to the histopathological criteria proposed by the World Health Organization (WHO). 18 Moreover, according to the IMTCGS criteria recently endorsed by the last edition of WHO, 19 each tumor was defined as either low- or high-grade. Different grading scores between the two pathologists were observed in <10% of the cases, and a consensus was achieved in all cases after discussion. The mitotic count and Ki67 proliferative index were evaluated using the same methods proposed for other neuroendocrine tumors. 19 Both indexes were measured using the “hot-spot” method: the same area of the neoplasia with the highest proliferative activity or the highest mitotic count was chosen for the evaluation. Mitotic count was assessed per 2 mm2 spot and the Ki67 proliferative index was evaluated manually in at least 500 tumor cells per tumor.
In this study, only tumor necrosis was considered, discriminating this from other forms of necrosis, such as necrotic hemorrhagic events or infarct-like features, frequently associated with preoperative procedures (e.g., fine-needle aspiration). Tumor necrosis typically manifests as karyorrhectic nuclear debris and degenerating cytoplasm in variable amounts (Supplementary Fig. S1). For each tumor, the American Joint Committee on Cancer Staging 8th edition was applied. 20 In the case of multifocality, the tumor with the highest size was considered.
Somatic genetic mutations
Data regarding somatic mutations of the tumors was already available in 212/314 (67.5%) patients. Next-generation sequencing molecular profiling of tumoral tissue using a thyroid-specific custom panel that includes the whole coding region of the RET and hot-spot portions of the other 16 genes was performed as previously described. 2 Cases harboring RET somatic mutations were validated by Sanger sequencing, while the others were classified as “RET negative.”
Statistical analysis
Data are shown as median values and interquartile ranges (IQRs). The statistical analysis was performed using IBM SPSS Statistics for Windows (Version 25.0, IBM Corp., Armonk, NY, USA). The statistical tests employed included the Mann–Whitney U test, Pearson’s chi-squared test (with Yates correction if required), as well as Cox regression univariate and multivariable analysis. The multivariable Cox regression model was performed including as variables IMTCGS and extent of disease (first analysis) and IMTCGS and RET status (second analysis). To construct structural detection rate curves and perform the log-rank and Breslow test, we used Kaplan–Meier analysis. A p value of < 0.05 was considered statistically significant.
Results
In Table 1 epidemiological, biochemical, pathological, and outcome data of the patients included in the study group were reported. A total of 181 patients (57.4%) were female and the median age at diagnosis was 54 years (IQR 44–64, range 16–87).
Epidemiological, Biochemical, Pathological, and Clinical Data of the Whole Study Group (n = 314) and Divided According to the International Medullary Thyroid Cancer Grading System in Patients with Low-(n = 199) and High-Grade (n = 115) Tumors
Bold data represents the statistically significance results.
IQR, interquartile range; mETE, minimal extrathyroidal extension; AJCC, American Joint Committee on Cancer; IMTCGS, international medullary thyroid cancer grading system; MTC, medullary thyroid cancer.
Median tumor diameter was 1.5 cm and multifocality and minimal extrathyroidal extension (mETE) were detected in 50/314 (15.9%) and 54/314 (17.2%) cases, respectively. Lymph node metastases were observed in 129/314 (41.1%) cases. When dividing N1 according to the site involved, 59/129 (45.7%) were defined as N1a, 10/129 (7.8%) N1b alone, and 60/129 (46.5%) N1a+N1b. At diagnosis, 31/314 patients (9.9%) had distant metastases. Localized, regional, and metastatic disease was present in 183 (58.3%), 100 (31.8%), and 31 (9.9%) patients at diagnosis, respectively. According to the IMTCGS criteria, we observed low-grade and high-grade tumors in 199/314 (63.4%) and 115/314 (36.6%) patients, respectively.
Biochemical and histological features of MTC patients according to IMTCGS
Patients with high-grade tumors showed higher preoperative median serum Ct levels compared with low-grade (median 542 [IQR 141–1880, range 5–40871] vs. 76 pg/mL [IQR 28.8–295, range 5–84600], p < 0.001).
Regarding histological features, patients with high-grade tumors more frequently showed aggressive histological features: larger tumors, multifocality, mETE, and lymph node metastases (Table 1). Particularly, laterocervical metastatic lymph nodes were more commonly observed in high-grade (48/115, 41.7%) compared with low-grade tumors (22/199, 11.1%) (p < 0.001). Likewise, at diagnosis, patients having high-grade tumors more frequently showed distant metastases, compared with low-grade (20.9% vs. 3.5%, p < 0.001).
DSS according to disease extent at diagnosis and IMTCGS
During a median follow-up time of 115 months (IQR 67–165, range 4–255), 28/314 (8.9%) patients died of MTC. As shown in Table 2, patients with regional (hazard ratio [HR] 15.8) and distant metastatic (HR 163.2) disease showed significantly lower DSS compared with localized disease. Moreover, lower DSS was experienced by patients with high-grade tumors (HR 7.3) compared with low-grade.
Univariate and Multivariate Cox Regression Analysis Evaluating Disease Extent at Diagnosis and International Medullary Thyroid Cancer Grading System Impact on Disease-Specific Survival, Distant Metastasis-Free Survival, and Locoregional Recurrence-Free Survival
Bold data represents the statistically significance results.
HR, hazard ratio; DSS, disease specific-survival; LRFS, local recurrence free-survival; DMFS, distant metastasis free-survival; CI; confidence intervals.
LRFS and DMFS according to disease extent at diagnosis and IMTCGS
To evaluate LRFS and DMFS, we excluded patients with known distant metastases at diagnosis (n = 31; 9.9%). In the remaining (n = 283; 90.1%), during a median follow-up time of 79 months (IQR 35–131, 3–248), 23/283 patients (8.1%) showed recurrences only in the neck (i.e., lymph nodes or local recurrences), 7/283 (2.5%) only in distant sites, and 11/283 (3.9%) in both. Regional disease (HR 35.1 and 15.3) and high-grade (HR 4.8 and 5.8) were associated with both lower LRFS and DMFS (Table 2).
Clinical application of IMTCGS according to disease extent at diagnosis
Disease-specific survival
Multivariable analysis showed that only regional and distant metastatic disease persisted as an independent predictive factor for worse DSS (Table 2). To confirm this result, we stratified patients according to disease extent at diagnosis. In the case of localized disease, patients with high-grade tumors showed lower, but not significant, DSS compared with low-grade (Fig. 1A, p = 0.054). Otherwise, in the case of regional and distant metastatic disease, DSS did not differ between patients with high- and low-grade tumors (Fig. 1B and C).
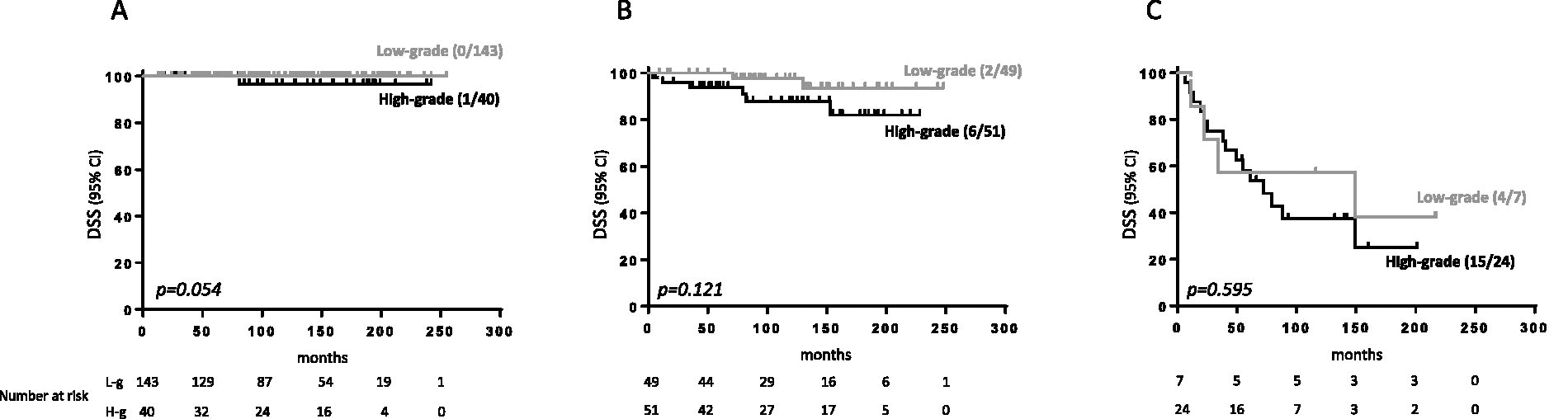
Disease-specific survival (DSS) in patients with low-(gray line) and high-grade (black line) tumors in localized (intrathyroidal, panel
Locoregional and distant metastasis recurrence-free survival
After excluding patients with distant metastases at diagnosis (n = 31, 9.9%) at multivariable analysis, both high-grade and regional diseases resulted in independent predictive factors for worse LRFS and DMFS (Table 2). When dividing patients according to the IMTCGS, in the case of localized disease, patients with high-grade tumors showed lower LRFS compared with low-grade (Fig. 2A, p = 0.01). Conversely, among patients with regional disease, no differences in LRFS were detected between high- and low-grade (Fig. 2B). Likewise, when evaluating DMFS, no difference was observed between patients with high- and low-grade tumors both in localized and regional disease (Fig. 2C and D).
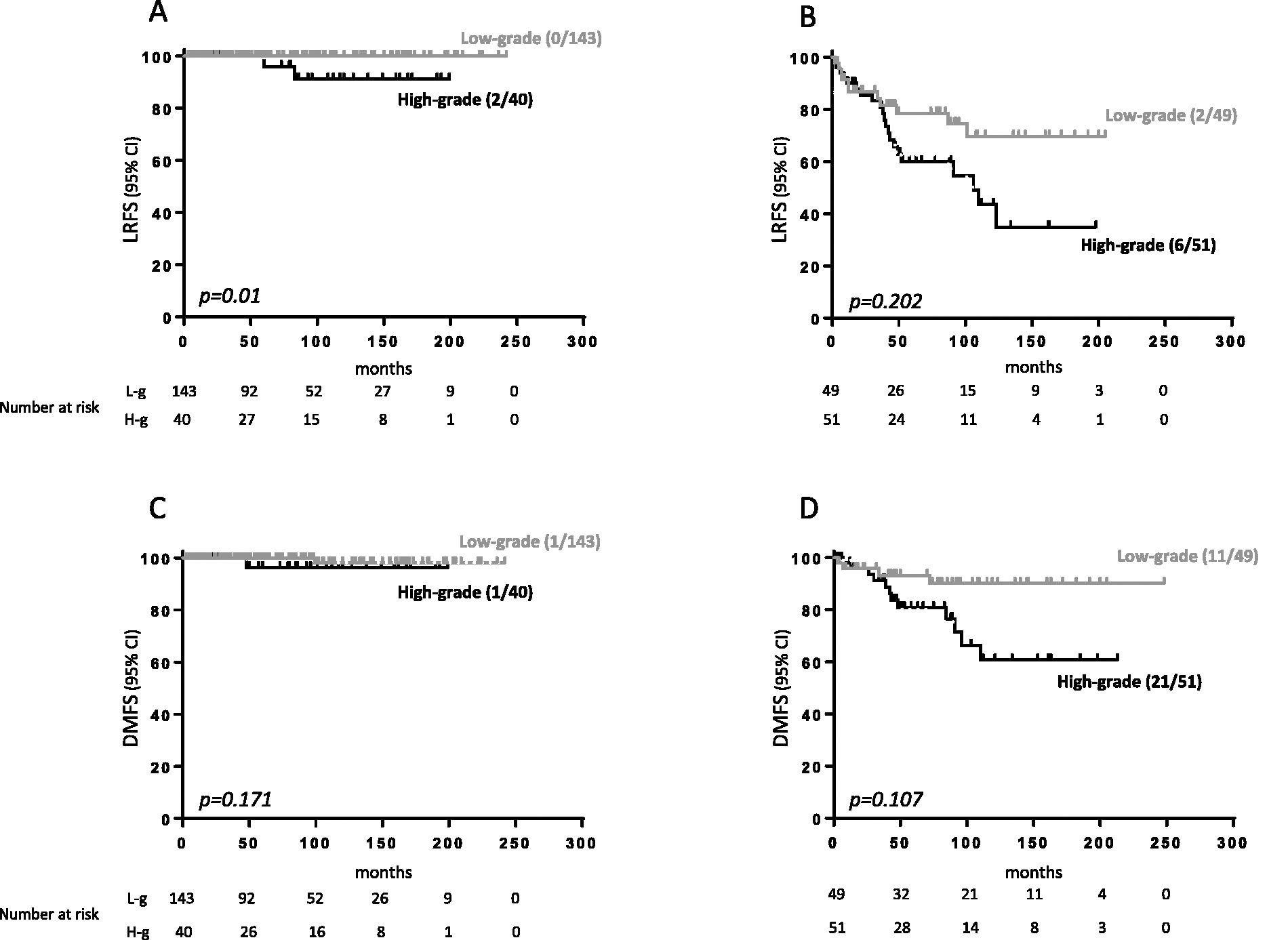
Local recurrence (LRFS) in patients with low-(gray line) and high-grade tumors (black line) in localized (panel
RET somatic mutation and IMTCGS
In 212/314 patients (67.5%), the data about somatic mutations were already available and being performed for other reasons. RET mutations were the most detected (116/212, 54.7%), while 96/212 (45.3%) cases were RET negative, of which 11 (12.9%) carried RAS mutations. Patients carrying RET mutated cancer had lower DSS (78.1% vs. 97.9%, p < 0.001), LRFS (72.9% vs. 90.6%, p = 0.006), and DMFS (82.1% vs. 96.9%, p = 0.002) compared with patients without RET mutation (Supplementary Fig. S2). Furthermore, those patients harboring cancer with somatic RETM918T and RET indels mutations had lower DSS (72.2% vs. 96.2%, p < 0.001), LRFS (61.1% vs. 89.9%, p < 0.001), and DMFS (74.1% vs. 96.9%, p < 0.001) compared with those carrying other somatic RET mutations.
Applying IMTCGS to patients in whom data about somatic mutations were available, 113/212 (53.3%) were low-grade and 99/212 (46.7%) were high-grade. Patients with high-grade (71/99, 71.7%) had more frequent RET mutated cancer compared with low-grade (45/113, 39.8%) (p < 0.001). Likewise, among RET somatic mutations, high-grade tumors (54/71, 76.1%) harbored more frequently RETM918T and RET indels compared with low-grade ones (25/45, 55.6%, p = 0.021).
Univariate and multivariable analyses showed that RET mutations and high-grade tumors were independent predictive factors for worse DSS, LRFS, and DMFS (Supplementary Table S1). We further categorized RET mutations into aggressive (i.e., RETM918T or RET indels) and other variants. Either aggressive RET mutations and high-grade tumors were independent predictive factors for worse DSS and LRFS or only aggressive RET mutations were predictive factors for worse DMFS (Table 3).
Univariate and Multivariate Cox Regression Analysis Evaluating RET Status (RETM918T/Indels Mutations, Other RET Mutations, Absence of RET Mutations) and International Medullary Thyroid Cancer Grading System
Bold data represents the statistically significance results.
Notably, in the presence of RETM918T or RET indels mutations, patients with high-grade tumors did not show lower DSS (p = 0.111, Fig. 3A), LRFS (p = 0.736, Fig. 3B), and DMFS (p = 0.586, Fig. 3C) compared with low-grade ones. Moreover, also when other RET somatic mutations were detected, patients with high-grade tumors showed a lower, but not significant (p = 0.06, Fig. 3D), DSS compared with low-grade ones, such as LRFS (p = 0.84, Fig. 3E) and DMFS (p = 0.21, Fig. 3F).
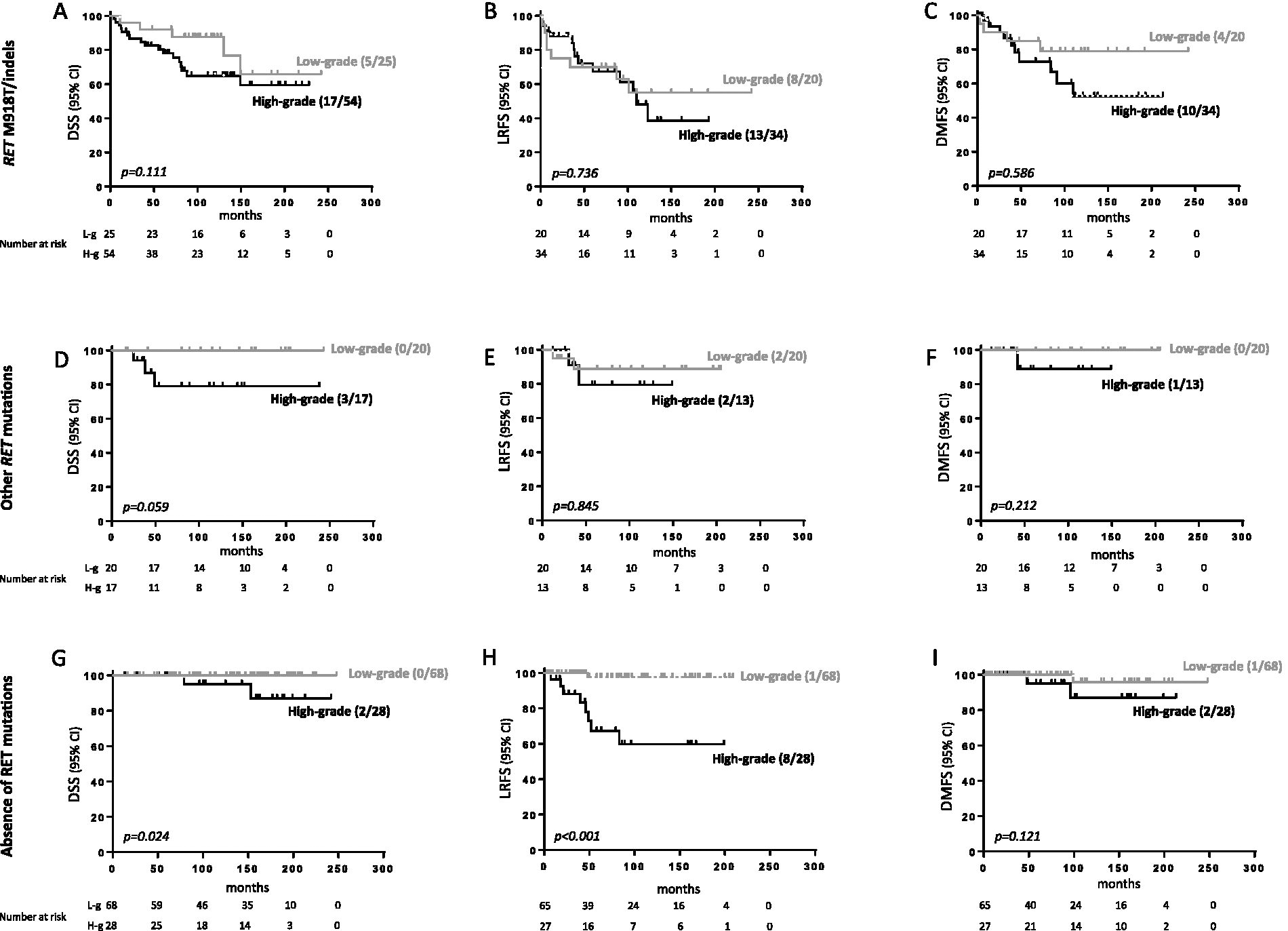
Disease specific-survival (DSS), local recurrence (LRFS), and distant metastasis free-survival (DMFS) in patients with low-(gray line) and high-grade tumors (black line) in the presence of RET M918T/indels mutations (panels
In the absence of any RET somatic mutations, patients with high-grade tumors showed lower DSS (p = 0.02, Fig. 3G) and LRFS (p < 0.001, Fig. 3H), but not DMFS (p = 0.12, Fig. 3I) compared with those with low-grade.
Discussion
Since its definitive histological description in 1959, 21 differently from other neuroendocrine tumors, MTC lacked a widely accepted histological grading system. 22 However, very recently, in a multicentric study analyzing 327 patients, a two-tiered IMTCGS has been proposed. 11 IMTCGS defined two histological grades, low- and high-grade, according to mitotic count, presence or absence of necrosis, and Ki-67 rate. When applying IMTCGS in their series of MTC patients, the authors observed its ability to predict overall survival, DSS, LRFS, and DMFS. Moreover, thanks to its interobserver reproducibility, 23 other studies confirmed that patients with high-grade tumors showed a lower survival rate compared with those with low-grade. 13,14 Conversely, Vissio et al. 15 applied IMTCGS in an independent cohort of 111 MTC patients (68 sporadic and 43 familial cases) and did not observe any difference in the overall survival rate between patients with high- and low-grade tumors.
In the first part of our study, we applied IMTCGS in a cohort of 314 sporadic MTC patients all surgically treated and followed at the same institution. We found that patients with high-grade tumors showed a worse disease extent at diagnosis compared with low-grade ones, as well as other negative prognostic factors (e.g., higher T, N, and M stage, mETE, and multifocality) in line with previous studies. 11,13 Moreover, patients with high-grade tumors showed higher preoperative serum Ct levels compared with low-grade ones. However, the association between histological aggressiveness and IMTCGS raised the question if IMTCGS application could provide more information about prognosis overcoming disease extent at diagnosis.
In our series, we confirmed that patients with high-grade tumors showed lower DSS compared with low-grade ones as already demonstrated in several papers. 11,13 –16 However, when patients were stratified according to their disease extent at diagnosis (localized, regional, and distant metastatic disease), having high-grade tumors was significantly associated with lower DSS only in the case of localized disease. Conversely, when known predictive factors of aggressiveness (i.e., N1b or distant metastases) were already present at diagnosis, no statistically significant difference in DSS was observed according to the low or high grade. In line with our results, Torricelli et al. compared the prognostic performance of IMTCGS and SEER-based risk in 66 MTC cases and they observed that SEER-based risk was a stronger predictor of worse outcome, compared with IMTCGS. 17,24 On the contrary, Xu et al. showed that IMTCGS persisted as an independent predictor of DSS, DMFS, and LRFS. 11 However, the lower prevalence of high-grade tumors in their study (24.8% vs. 36.6%) compared with ours and the inclusion in our study of consecutive patients could, at least in part, explain this difference.
We found that patients with high-grade tumors showed lower DMFS and LRFS, as already observed. 11,13,15 Accordingly, Nigam et al. 16 reported that patients with high-grade tumors, although without distant metastasis at diagnosis, frequently showed structural disease at the end of a median follow-up time of 70 months in a cohort of 117 MTC patients. However, this association weakens in the presence of already-known predictive factors for disease recurrence. Particularly, in the case of serum Ct doubling time <2 years, six out of six patients with low-grade and 17 out of 20 of those with high-grade tumors showed structural disease during the follow-up. 16 Likewise, although we did not evaluate the serum Ct doubling time, we observed that in patients with known predictive factors of recurrence (i.e., N1a and/or N1b), IMTCGS lost its efficacy in predicting worse LRFS and DMFS. Conversely, patients with high-grade tumors showed lower LRFS compared with low-grade, but exclusively in case of localized disease.
RET mutations in sporadic MTC are frequently detected, particularly in advanced cases, 1 and currently, their detection is crucial for the use of highly selective RET inhibitors. 25,26 The question of whether RET mutations are more frequently detected in patients with high-grade tumors is of interest. In our series, RET somatic mutations were significantly more frequent in patients with high-grade tumors compared with low-grade ones. Accordingly, Xu et al., in a cohort of 250 patients with sporadic MTC, confirmed that RET somatic mutations were associated with high-grade according to IMTCGS. 12 Censi et al. reported similar findings in a series of 141 patients with sporadic MTC. 27 On the contrary, Torricelli et al. 17 did not observe any correlation between IMTCGS and somatic RET point mutations probably due to a lower number of analyzed patients (n = 66). Looking at the type of RET mutations, patients with high-grade tumors more frequently showed RETM918T and indels, which are recognized as the most aggressive RET mutations in sporadic cases. 10 Interestingly, when those RET mutations were detected, no significant differences were shown in DSS, LRFS, and DMFS between patients with high- and low-grade tumors. However, only in patients without any RET mutations, who have longer DSS and LRFS, IMTCGS was able to identify those few patients with worse prognoses.
When we designed the study, we decided to include only patients with sporadic MTC. The first and more relevant reason is the well-recognized different disease extent at diagnosis and management between sporadic and hereditary MTC cases, 28 and, for this reason, grouping sporadic and hereditary cases may induce a bias. However, we cannot exclude that IMTCGS may have the same clinical usefulness both in sporadic and in hereditary cases. In line with that, in a rather small cohort of MTC patients (n = 111), although they confirmed that patients with high-grade tumors had a shorter disease-free survival, Vissio et al. 15 did not observe different overall survival rates comparing patients with high- and low-grade tumors both in the whole cohort of patients (hereditary and sporadic) and when analyzed sporadic cases alone (n = 68).
We are aware that our study has several limitations, the main one being its retrospective nature. However, given the rarity of the disease, as demonstrated by the multicentric retrospective nature of the IMTCGS, conducting a prospective study with a large patient cohort and extended follow-up would have been challenging. Regarding RET somatic status, not available in all cases, it should be emphasized that this procedure is not included in the standard of care of patients with sporadic MTC, mainly if not advanced and not requiring systemic therapy. 25 However, the large number of patients having these data (about 70%) led to a reduction of potential biases. Another limitation of this study is that the generalizability of these results can be affected by the high expertise of the pathologists involved in the current study, highly skilled in thyroid cancer diagnosis, thus limiting the application of these data in centers with less experience. Nonetheless, it should be pointed out that MTC is a rare tumor and patients suffering from this rare disease should be mainly followed-up in referral centers. Conversely, several strengths should be highlighted. To the best of our knowledge, this is the single-center study with the highest number of patients included, all surgically treated and followed-up at the same institution with the same modalities over time for the duration of the study, with the longest follow-up and survival time compared with other studies. 11,13 –15 Moreover, all cases were revised by the same pathologists with high expertise in thyroid cancer fields.
In conclusion, in our large cohort of sporadic MTC patients, we confirmed the overall reproducibility of IMTCGS since patients with high-grade tumors had lower DSS, LRFS, and DMFS compared with low-grade. However, this was clinically relevant only in patients with an apparently lower risk of recurrence and mortality (i.e., lower stages at diagnosis or RET negative cases). Conversely, when laterocervical lymph nodes (N1), distant metastasis (M1), or RET mutations, particularly M918T or indels, were already present at diagnosis, the role of IMTCGS in predicting DSS, DMFS, and LRFS became less relevant.
It would be advisable that our results can be confirmed in further large multicentric series, including sporadic MTC, having a centralized pathological and molecular evaluation.
Footnotes
Acknowledgment
The authors acknowledge the European Network for Rare Adult Solid Cancers (EURACAN) for its support.
Authors’ Contributions
A.P., L.T., C.G., R.E., and A.M.: Conceived and designed the research. A.P., L.T., C.G., R.C., T.R., C.R., V.C., P.P., G.M., R.E., and A.M.: Analyzed and discussed the data. A.P. and A.M.: Prepared the figures. A.P., C.G., R.E., and A.M.: Prepared the article. R.E.: Critically reviewed the article during its preparation. All authors revised and approved the final version of the article.
Author Disclosure Statement
R.E. is a consultant for EISAI, Lilly, Ipsen, and Bayer. A.M. is a consultant for Lilly. The other authors have nothing to declare.
Funding Information
This study has been supported by grants to R.E. from the Associazione Italiana per la Ricerca sul Cancro (AIRC, Investigator grant 2018, project code 21790).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1