
Abstract
Background:
In the era of molecular testing, thyroid nodules with indeterminate cytology are increasingly being managed nonoperatively. The false-negative rates of these molecular tests, and therefore missed malignancies, are not well defined in real-world clinical practice.
Methods:
This retrospective study of patients undergoing fine needle aspiration (FNA) biopsy at our health system between November 2017 and March 2022 included nodules with The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) III and IV cytology and negative, currently negative, or negative but limited ThyroSeq version 3 (TSv3) results. Surgical pathology of resected nodules, as well as details of ultrasound (US) surveillance practices, was recorded. A range of prevalence of malignancy (PoM) estimates were calculated based on all nodules (PoM low) and surgically resected nodules (PoM high).
Results:
The study cohort consisted of 556 nodules. TSv3 results were distributed as 443 (80%) negative, 85 (15%) currently negative, and 28 (5%) negative but limited. Overall, 75 nodules were resected: 54 nodules (9.7%) had immediate surgery, and 21 nodules (3.8%) had delayed surgery after surveillance imaging. Currently negative and negative but limited nodules were more likely to undergo immediate surgical resection compared with negative nodules (20%, 18%, and 7%, respectively, p < 0.001). The PoM in molecularly benign TBSRTC III and IV thyroid nodules ranged between 3% and 23% depending on the inclusion of all versus resected nodules. TBSRTC IV molecularly benign nodules had a higher PoM than TBSRTC III (PoM low 7.3% vs. 1.6%, p < 0.001; PoM high 48% vs. 13%, p = 0.0013). In the 90% of nodules that were managed nonoperatively, 63% had at least one surveillance US. Timing of initial surveillance US ranged from 3 to 60 months (median 13 months, interquartile [IQR] 11–19 months). Median follow-up duration was 25 months (IQR 17–34 months). Nodule growth occurred in 24% of nodules; only a minority (7%) underwent repeat FNA.
Conclusions:
Negative subtype of TSv3 should be considered in clinical management recommendations. For negative but limited samples, repeat FNA should be performed. Optimal surveillance strategy for nonresected negative and currently negative nodules remains unknown. Until further real-world data are available, surveillance ultrasonography is recommended for TSN and TSCN nodules, similar to the ATA guidelines for TBSRTC II nodules.
Introduction
Thyroid nodules are common, and ultrasound (US) characteristics are used to identify those nodules requiring fine needle aspiration (FNA) biopsy for further evaluation. In addition to reporting benign and malignant cytological diagnoses, the Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) includes the following two diagnostic categories that are indeterminate for malignancy: TBSRTC III (atypia of undetermined significance, AUS) and TBSRTC IV (follicular neoplasm or oncocytic follicular neoplasm, FN or OFN). The proportion of FNA specimens classified as TBSRTC III or IV ranges from 34%–65% and has increased over time, perhaps, in part, due to the implementation of the American College of Radiology Thyroid Imaging Reporting and Data Systems (TI-RADS) US criteria. 1 The average rates of malignancy (and ranges) of TBSRTC III and TBSRTC IV categories are reported to be 22% (13–30%) and 30% (23–34%), respectively. 2 Historically, before the availability of molecular testing, diagnostic lobectomy or total thyroidectomy was performed for lesions in these categories to differentiate malignant from benign nodules.
Molecular testing is becoming more of a norm and allows further risk stratification to inform treatment decisions in cytologically indeterminate nodules. One such test is the ThyroSeqv3 Genomic Classifier® (TSv3), which has been in clinical use since 2017. This test uses next-generation sequencing technology to analyze 112 genes over 5 classes of genetic alterations, including point mutations, insertions/deletions, gene fusions, copy number alterations, and abnormal gene expression. TSv3 reports results as negative (including additional subtypes of currently negative and negative but limited) or positive based on algorithmic analysis. 3 A currently negative TSv3 result indicates that the genomic classifier score was 1, signifying a molecular change associated with a low risk of malignancy (5–10%), rather than 0 for negative result. When presequencing steps result in low cellularity or the postsequencing analysis is inadequate due to the low expression of thyroid cell markers, TSv3 results are negative but low thyroid cell content or negative but limited, respectively. 4
In initial validation studies, where all patients underwent surgery regardless of TSv3 results, the false-negative rate was 3% in TBSRTC III or IV nodules. 4 This false-negative rate is similar to the reported 4% risk of malignancy in nodules diagnosed as benign (TBSRTC II) on FNA. 2 Therefore, it has been suggested that patients with indeterminate cytology and subsequent negative TSv3 molecular profile can be monitored with US surveillance rather than proceeding to surgery, similar to the recommendations for clinical management of TBSRTC II nodules. 5 Given the benign call rate of 61% in a TSv3 validation study, 4 surgery could be avoided for almost two-thirds of patients with TBSRTC III or IV cytological diagnoses on the basis of a negative molecular profile.
A prior study at our institution reported that of nodules with TBSRTC III or IV cytology diagnoses, 71% were TSv3 negative. 6 In this same study, TSv3-negative nodules were less likely to undergo surgical resection than TSv3-positive nodules (10% vs. 79%). 6 Additional data from a recent retrospective study showed that 90% of patients with TBSRTC III or IV cytology and negative TSv3 results were managed with surveillance. 7
Given the shift in clinical practice to deferring surgery for the majority of patients with TBSRTC III and IV molecularly benign nodules, insufficient numbers of patients undergo surgery to allow for meaningful calculations of true false-negative rates in postvalidation TSv3 use. Therefore, it is necessary to understand clinical follow-up and outcomes of indeterminate thyroid nodules with a negative molecular profile. This study aims to assess the prevalence of malignancy (PoM) in thyroid nodules with TBSRTC III and IV cytology undergoing contemporary real-world management and to describe the observed clinical surveillance practices within our health system.
Materials and Methods
Study population
Thyroid nodules with TBSRTC III and IV cytology and negative, currently negative, or negative but limited TSv3 results from November 2017 to March 2022 were assessed for inclusion in this retrospective study. At our institution, the approximate rates of TBSRTC III and IV cytological diagnoses are 25% and 19%, respectively. The clinical pathway for nodule evaluation includes reflexive molecular testing on nodules with TBSRTC III and IV cytology.
Exclusion criteria included age younger than 18 years, no diagnostic US at the University of Pennsylvania Health System (UPHS), US-guided FNA not performed at the UPHS, prior molecular testing of the same nodule, prior thyroid malignancy, or FNA of nonthyroidal neck mass or thyroid bed lesion (Fig. 1). This study was deemed exempt by the Institutional Review Board at the Perelman School of Medicine, University of Pennsylvania under Exempt Category 4 (IRB: DIJFGCT).
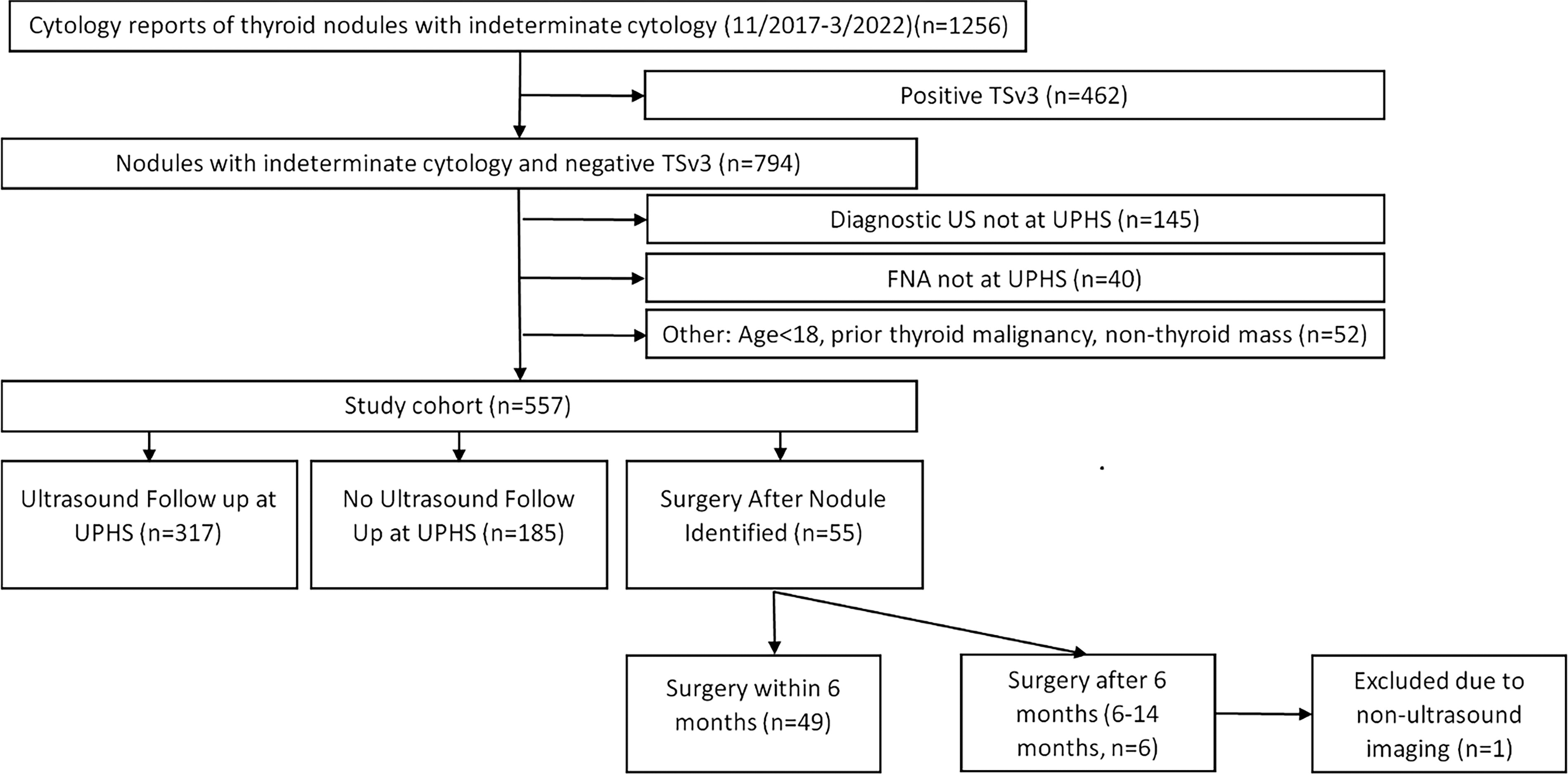
Participant flow diagram. Abbreviations: TSv3, ThyroSeqv3; US, ultrasound; FNA, fine needle aspiration; UPHS, University of Pennsylvania Health System.
Study design
For each nodule, data were abstracted from cytopathology reports to determine TBSRTC diagnosis and TSv3 result. Molecularly benign results included three negative subtypes of TSv3 and were categorized as “Negative,” “Currently Negative,” and “Negative but Limited” (TSN, TSCN, and TSNBL, respectively). The TSNBL categorization included both “Negative but Limited” and “Negative but Low Thyroid Cell Content.”
Additional data obtained from imaging reports determined index nodule size and sonographic imaging classification by TI-RADS at the time of initial FNA and at follow-up US examinations. Nodule growth was defined as >50% change in volume. 8
If patients underwent surgery, pathology reports and reason for surgery were reviewed. Surgery was defined as immediate if patients underwent surgery after initial US and FNA without subsequent surveillance imaging. Surgery was defined as delayed if a follow-up US was performed. Surgical pathology was classified as malignant if the index nodule corresponding to the FNA site displayed malignant pathology. Incidental malignancies elsewhere in the thyroid gland were not considered malignant for the purposes of this study. Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) was categorized as malignant. If patients underwent repeat FNA, cytology, repeat molecular testing, and reason for repeat FNA were assessed.
Study outcomes and statistical analyses
Patient demographics (age, sex, ethnicity), median nodule size, baseline sonographic classification, and molecular testing results were reported by cytology diagnosis (Table 1). The primary outcome was PoM based on surgical pathology (Table 4). Since the majority of TBSRTC III and IV nodules with benign molecular profile no longer undergo surgery, a true negative-predictive value (NPV) cannot be reported. Instead, PoM estimates were calculated based on methodology reported in Valderrabano et al. 9 The low estimate of PoM is calculated using all nodules (n = 556) as the denominator and considers nonoperatively managed nodules to be benign. The high estimate of PoM is based upon only those nodules that were surgically resected (n = 75). The true PoM, which is equivalent to the false-negative rate, must lie between these estimates. Statistical analyses were performed using chi-squared, Fisher’s exact, and Moods median tests as appropriate with p values less than 0.05 considered statistically significant.
Baseline Characteristics of Patients with Thyroid Nodules with the Bethesda System for Reporting Thyroid Cytopathology III or IV and ThyroSeq v3-Negative Molecular Profile
No parameters significantly differ between TBSRTC III versus IV cohorts.
TBSRTC, The Bethesda System for Reporting Thyroid Cytopathology; TSv3, ThyroSeq v3; AUS, atypia of uncertain significance; FN, follicular neoplasm; OFN, oncocytic follicular neoplasm; HUP, Hospital of the University of Pennsylvania; PPMC, Penn Presbyterian Medical Center; TI-RADS, Thyroid Imaging Reporting and Data Systems.
Results
Of the 557 nodules meeting inclusion criteria of TBSRTC III or IV cytology and negative TSv3 result, 1 was excluded due to non-US imaging surveillance. The final study cohort included 556 nodules in 526 patients.
Baseline demographic characteristics of patients were similar among TBSRTC III and IV nodules (Table 1). The median age was 61.8 years (interquartile range [IQR] 50.3–70.1 years), 77% of patients were female, median nodule size was 3.3 cm3 (IQR 1.3–8.1 cm3), and the median largest dimension of the nodules was 2.5 cm (IQR 1.7–3.0 cm). There was no significant association between cytology result and baseline TI-RADS US category (p = 0.43), or TSv3 negative subtype result (p = 0.44).
Prevalence of malignancy
Of the 556 nodules included in the analysis, TSv3 negative results were distributed as 443 TSN (80%), 85 TSCN (15%), and 28 TSNBL (5%). During the entire study period, 75 nodules underwent surgical resection, classified as either immediate (54 nodules) or delayed (21 nodules) (Fig. 2). Considering all surgically resected nodules, 58 (77%) were benign, 15 (20%) were malignant, and 2 (3%) were NIFTP (Table 2). In patients with benign surgical pathology, over half (55%) demonstrated follicular nodular disease. There was no relationship between cytology diagnosis, for example, TBSRTC III versus IV, and whether nodules were hyperplastic or adenomas (p = 0.20). The American Thyroid Association (ATA) risk of recurrence 8 was low in the 15 nodules with malignant surgical pathology (Table 3).
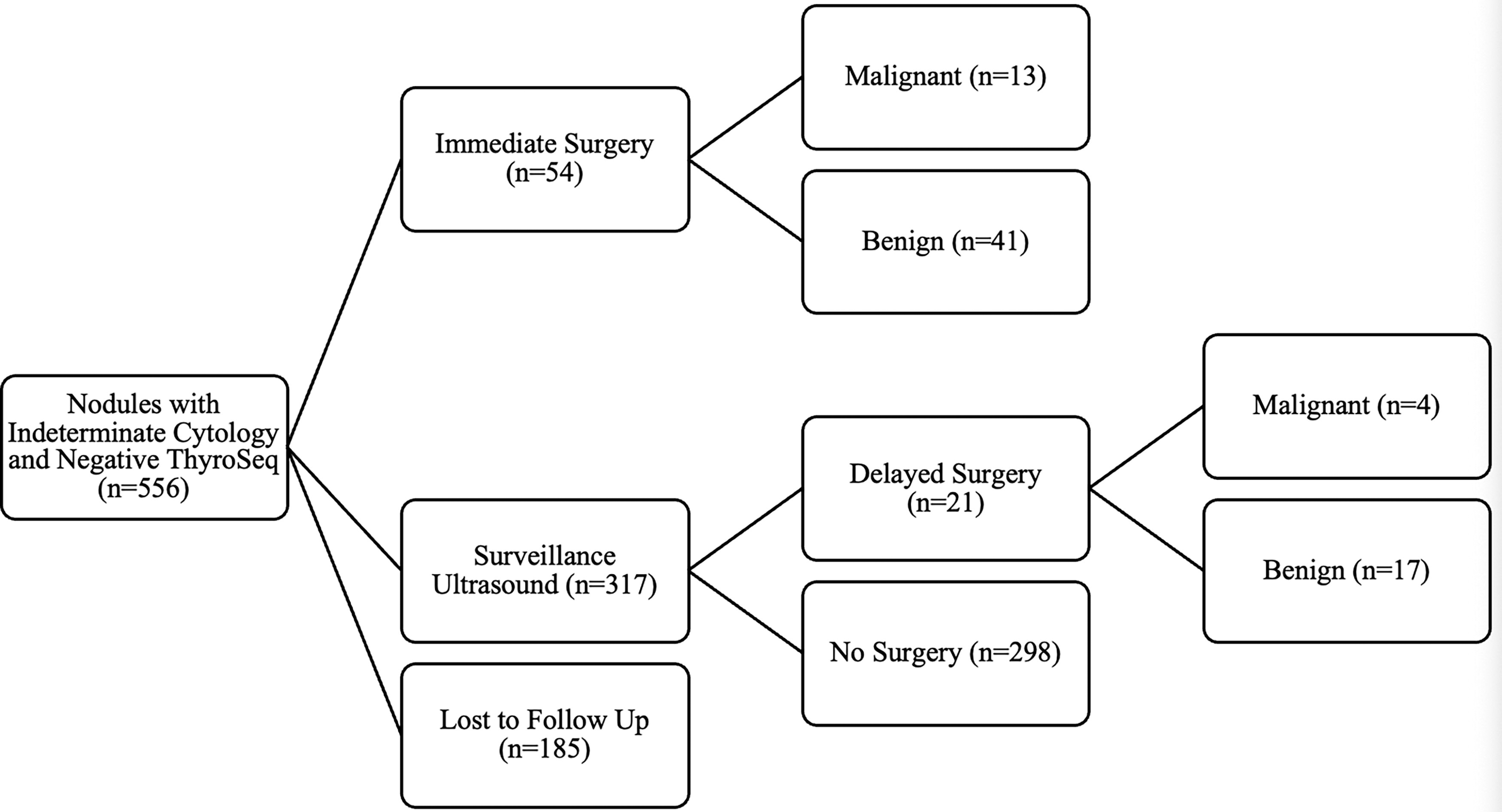
Flow diagram of management of nodules with indeterminate cytology and negative TSv3. Malignant classification includes two noninvasive follicular thyroid neoplasm with papillary like nuclear feature (NIFTP) nodules. TSv3, ThyroSeqv3.
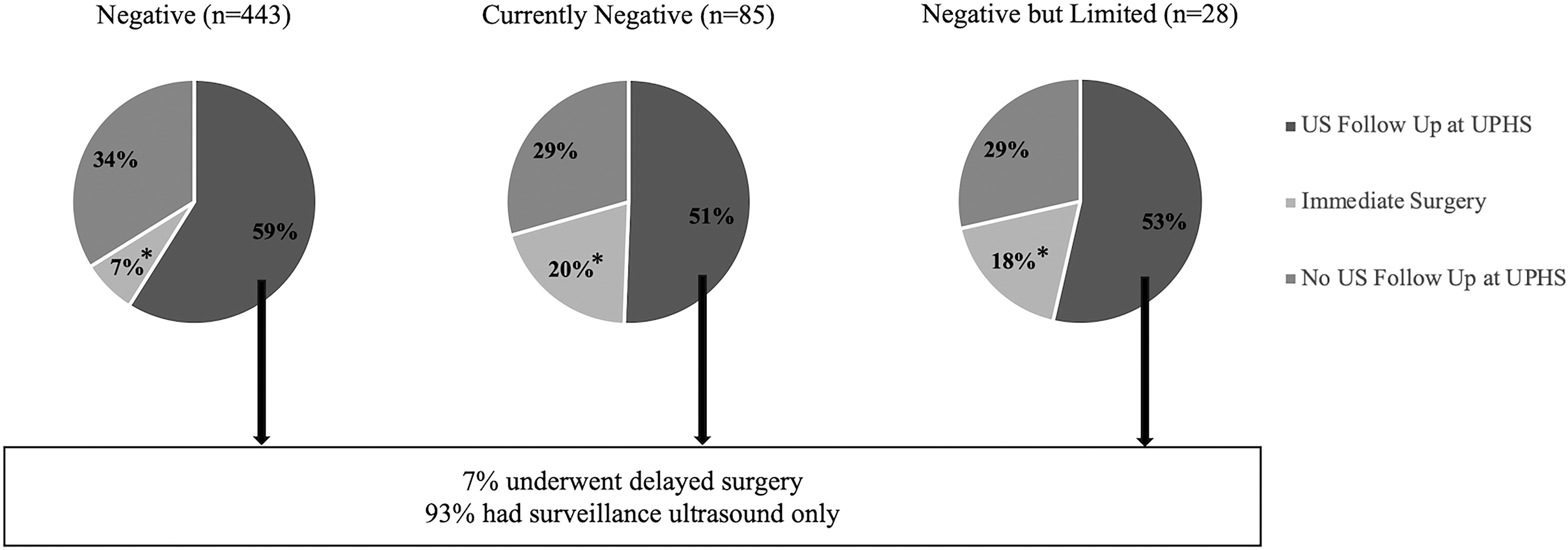
Clinical management based on TSv3 negative subtype result. *A p value of < 0.001 for rates of immediate resection among the TSv3 negative subtypes. TSv3, ThyroSeqv3; US, ultrasound; UPHS, University of Pennsylvania Health System.
Histopathologic Diagnosis of the Bethesda System for Reporting Thyroid Cytopathology III or IV Nodules by ThyroSeq v3 Negative Subtype
See Table 3 for ATA risk of recurrence.
ATA, American Thyroid Association; TBSRTC, the Bethesda System for Reporting Thyroid Cytopathology; TSv3, ThyroSeq v3; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; PTC, papillary thyroid cancer; FTC, follicular thyroid cancer.
Malignant Surgical Pathology
TSv3, ThyroSeqv3; FNA, fine needle aspiration; NA, not applicable; ATA, American Thyroid Association; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; FTC, follicular thyroid cancer; PTC, pPapillary thyroid cancer; AUS, atypia of uncertain significance; FN, follicular neoplasm; OFN, oncocytic follicular neoplasm; CNA, copy number alteration.
For all TSv3 negative subtypes, the lowest estimated PoM was 3% and differed among the subtypes (2%, 7%, and 7% in TSN, TSCN, and TSNBL, respectively, p = 0.02). The highest estimated PoM was 23% and did not differ by negative subtype (18%, 30%, and 33% in TSN, TSCN, and TSNBL, respectively, p = 0.46) (Table 4). Although TSv3 negative subtype distribution did not differ between TBSRTC III and IV nodules, both low and high PoMs were significantly higher in molecularly benign TBSRTC IV versus III nodules (PoM low 7.3% vs. 1.6%, p < 0.001; PoM high 48% vs. 13%, p = 0.0013). We also examined potential differences between different cytological subtypes. When TBSRTC III nodules were analyzed as AUS with nuclear atypia versus AUS due to other features, neither the TSv3 negative subtype distribution nor the PoM differed (PoM low 1.4% vs. 2.3%, p = 0.48; PoM high 10.8% vs. 17.6%, p = 0.49). In addition, there was no difference in PoM of oncocytic nodules (AUS oncocytic and OFN) compared with nononcocytic nodules (AUS due to other features and FN).
Prevalence of Malignancy Including All Resected Nodules
Rates of surgical resection were significantly higher in currently negative and negative but limited subtype results compared with negative, p < 0.005.
p < 0.05.
p NS.
TSv3, ThyroSeqv3; PoM, prevalence of malignancy.
TI-RADS classification did not influence PoM, with all malignancies being classified as TR3 or TR4 on initial ultrasonography. Furthermore, size ≥4 cm did not impact PoM.
Observed clinical management
Of the 556 nodules included in the analysis, 54 (9.7%) underwent immediate surgery, 317 (57%) were initially managed nonoperatively with US surveillance at UPHS, and 185 (33.3%) had no US follow up within our health system.
Immediate surgical resection rates were higher for nodules with TSCN and TSNBL results (20% and 18%, respectively) compared with those with TSN subtype (7%, p < 0.001, Fig. 3). Patients undergoing immediate surgery were more likely to be younger (median age 56.6 vs. 62.3, p = 0.02) and nodules were likely to be larger (median volume 5.8 vs. 3.1 cm3, p = 0.02, median largest dimension 3.1 vs. 2.3 cm, p = 0.009). TI-RADS classifications and cytology diagnoses did not differ between nodules undergoing immediate resection versus observation (Supplementary Table S1). Reasons for immediate surgery were varied and included a second nodule requiring surgery (n = 8; 7 TSv3 positive, 1 TBSRTC V), indications for parathyroidectomy or other neck surgery (n = 7), patient preference (n = 27), clinician preference (n = 6), and other (n = 6). Reasons for clinician preference included nodule size (n = 3) and rapid development of a nodule in a young patient (n = 1); rationale for the clinician’s surgical recommendation was not ascertainable in two cases. Other reasons for immediate surgery included hyperfunctioning nodules (n = 3), concurrent surgery for breast cancer metastatic to supraclavicular lymph nodes, a positive TSv3 result from repeat FNA on a TSNBL sample, and a concurrent contralateral lymph node biopsy showing thyroid cancer.
Of patients who did not undergo immediate surgery, 63% (317/502) had at least one surveillance US within our health system, with a median follow-up of 25 months (IQR 17–34 months]. Female patients (66% vs. 54% male) and those followed by an endocrinologist (73% vs. 38% no endocrinologist) were more likely to have surveillance sonography. The likelihood of having a follow-up US did not otherwise differ based upon patient age, TI-RADS classification, nodule size, TBSRTC III versus IV, or TSv3negative subtype (Supplementary Table S2).
When performed, the number of surveillance US examinations varied between 1 and 6. Time to first surveillance US showed a wide range between 3 and 60 months (median 13 months, IQR 11–19 months). Median follow-up duration was 25 months (IQR 17–34 months). Neither TBSRTC diagnosis (p = 0.93), III versus IV, nor TI-RADS classification (p = 0.60) impacted interval to first US. Growth, defined by the ATA definition of 50% increase in volume, was documented in 76 nodules (24%). Nodule growth was not associated with TSv3 negative subtype, TBSRTC diagnosis, TI-RADS classification, or nodule size.
During surveillance, 23 nodules (7%) underwent repeat FNA (Table 5). Although FNA was more likely to be repeated in nodules with sonographically documented growth rather than stability, only 14% (11/76) of growing nodules underwent repeat FNA versus 5% (12/243) of stable nodules (p < 0.01). Reasons for repeat biopsy were growth (11), change in TI-RADS category (2), and clinician preference (10).
Repeat Fine Needle Aspiration Results of Nodules with Negative Molecular Profile
TSv3, ThyroSeqv3; FNA, fine needle aspiration; AUS, atypia of undetermined significance; FN, follicular neoplasm; OFN, oncocytic follicular neoplasm; TI-RADS, Thyroid Imaging Reporting and Data Systems; CNA, copy number alterations.
Repeat cytology results remained the same for the seven nodules with initial TBSRTC IV diagnoses (two FN and five OFN nodules). However, for 16 nodules with initial TBSRTC III diagnoses, repeat FNA cytology was TBSRTC II in 5 (31%), TBSRTC III in 8 (50%), and TBSRTC IV in 3 (19%). Repeat TSv3 testing was performed in 17 nodules with persistent TBSRTC III or IV cytology results and remained a negative subtype for 15 (88%) nodules. The TSv3 became positive in two nodules (one TSN and one TSNBL initial results). Repeat TSv3 on the first nodule, initially TSN with an EZH1 mutation, demonstrated mutations in both EZH1 and TP53 and was diagnosed as an oncocytic adenoma after resection. The second nodule, initially TSNBL was subsequently positive for CNA and was also resected, with histopathology of a minimally invasive oncocytic carcinoma. Five nodules had discordant repeat TSv3 results within the three negative subtypes: TSv3 became negative in three nodules, two initially TSNBL and one TSCN. For two nodules that were initially TSN, one was reported as TSCN and one was reported as TSNBL.
After surveillance US, delayed surgery occurred in 21 nodules. Delayed surgical resection rates did not differ based on the initial TSv3 negative subtype (p = 0.65) or nodule growth (p = 0.11). Thyroid cancer was diagnosed in 4 of the 21 nodules (19%), not significantly different from the cancer/NIFTP detection rates in those undergoing immediate surgery. Reasons for delayed surgery were need for parathyroidectomy or other neck surgery (n = 3), patient preference (n = 7), clinician preference (n = 8), and other (n = 3).
Discussion
Our single-institution study describes the observed PoM in thyroid nodules with TBSRTC III and IV diagnoses and TSv3 negative subtype results and the subsequent surveillance practices. Although the expected frequencies of TSv3 negative subtypes are not reported on its website (www.thyroseq.com), our distribution of TSv3 negative subtypes (TSN 80%, TSCN 15%, TSNBL 5%) is similar to that reported at the University of Pittsburgh, where the TSv3 test is performed (TSN 80%, TSCN 13%, TSNBL 7%). 10 Because most nodules with negative molecular results are not resected, the true false-negative rates and NPVs of molecular tests cannot be determined in a real-world study such as ours. Therefore, we calculated PoM using two scenarios. The low PoM estimate considers all nodules with a negative TSv3 results as benign, and the high PoM estimate only evaluates resected nodules. 9 The assumption is that the true PoM is in between these estimates. In this cohort, PoM for thyroid nodules with TBSRTC III or IV cytology and any TSv3 negative subtype was 23% for resected nodules and 3% for all nodules. TSCN and TSNBL nodules appeared to have a significantly higher PoM compared with TSN nodules when considering nonresected nodules as benign (p < 0.05). When estimating PoM based on resected nodules only, this difference is no longer significant, suggesting that higher rates of surgical resection of TSCN and TSNBL nodules account for this difference. The high PoM estimate of 23% is likely an overestimate, given the selection bias of nodules proceeding to surgery. Importantly, all of the resected thyroid cancers were classifiable as ATA low risk for structural recurrence.
To our knowledge, only one other study has examined risk of malignancy based on TSv3 negative subtypes. Notably, in this Canadian study, differences in rates of surgical resection based on TSv3 negative subtype were also reported with 1% (4/391) of TSN nodules undergoing surgical resection compared with 84% (38/35) of TSCN and 13% (4/32) of TSNBL nodules (p < 0.00001). 7 Estimated low and high PoMs for the entire study cohort were 4.4% and 46%. For each TSv3 negative subtype, the low and high PoMs were, respectively, 0.3% and 25% for TSN, 38% and 45% for TSCN, and 10% and 75% for TSNBL. 7 The extremely low rates of surgical resection in TSN and TSNBL nodules resulted in wide estimated ranges for PoM despite an overall low incidence of cancers. Our surgical resection rates were higher for TSN (11%) and TSNBL (21%) and lower for TSCN (21%) nodules, which likely accounts for observed differences in PoM.
Several studies of both TSv3 and Afirma Gene Sequence Classifier® (GSC) report NPVs assuming that all nonresected nodules are benign. 7,11 –13 In the current study, the low PoM of 3% for all TSv3 negative subtypes is similar to estimates in the initial validation studies and other TSv3 studies representing various clinical practice settings. 4,7,11 In addition, data from real-world studies of both TSv3 or GSC generally demonstrate a 7- to 10-fold difference between low and high PoM estimates, consistent with our findings. 11 –13
The current study’s finding of higher PoM in molecularly benign TBSRTC IV compared with TBSRTC III nodules has not been previously reported. This may be based upon the overall higher rates of malignancy in TBSRTC IV nodules, as reported in TBSRTC version 32 and other Western studies. 14,15 A recent multi-institutional study evaluating Afirma GSC reported a higher PoM in molecularly benign TBSRTC IV compared with TBSRTC III nodules in the two centers with higher baseline rates of malignancy for TBSRTC IV versus III, but this finding did not reach significance (p = 0.08). 12 In the current era of nonsurgical management for molecularly benign nodules, our institutional malignancy rates based upon TBSRTC III and IV cytological diagnosis alone cannot be calculated. It remains unclear whether nodules with a benign molecular profile should be followed differently based on an initial cytology result of TBSRTC IV versus III.
Overall, the reassuringly low false-negative rates reported in studies of real-world clinical practice based upon the low PoM estimate have decreased diagnostic surgical resection for molecularly benign nodules. 5 In the current study, 87% (481/556) of molecularly benign nodules were managed nonoperatively, similar to prior reports. 7 It is therefore crucial not only to understand the PoM in molecularly benign nodules, but also to delineate guidelines for clinical management of nodules that do not undergo surgical resection.
At present, there is no consensus regarding optimal surveillance strategies for cytologically indeterminate nodules with a benign molecular profile. In the current study, 63% of nonoperatively managed nodules underwent follow-up US, similar to a recent study from the Ohio State University where US surveillance was performed for 63% of TBSRTC III and IV GSC benign nodules. 13 Growth was documented in 24% of nodules in the current study during a median follow-up of 25 months, consistent with observed rates for GSC benign nodules (Ahmadi et al 20%, 12 Azaryan et al 25% 13 ) followed for similar time periods (Ahmadi et al 23 months, 12 Azaryan et al 34 months 13 ). Growth is less likely to be detected in studies with a shorter follow-up. 11 Since only a small number of growing nodules (14%) were resected, the current study is not powered to assess whether growth is a determinant of missed malignancy in molecularly benign nodules. This likely applies to other studies that have reported malignancy rates in surgically resected growing nodules with molecularly benign results. 12,13 In addition, in the current study as in other published observational reports, nodule growth does not generally lead to repeat FNA for this group of nodules (Azaryan et al repeat FNA in 14/30 [47%], 13 our data 11/76 [14%]).
Our data are also consistent with prior studies that repeat FNA renders a benign cytology diagnosis in 31% of nodules with initial TBSRTC III cytology. 16 For TBSRTC III nodules, repeat FNA is a valid option for patients especially when molecular testing is not available or not financially feasible. In addition, TSv3-negative results remained a negative subtype for 88% of nodules with repeat molecular testing. A low-risk cancer and a benign adenoma accounted for the pathology results in the two nodules where the repeat TSv3 became positive.
The limitations of this study include absence of surgical follow-up for all observed nodules, which is a universal limitation due to shifting clinical practice to observation rather than diagnostic surgical resection. Only surgeries and US follow-up within our health system were evaluated, and therefore, rates of surgical resection and US surveillance may be underreported if patients were managed at another institution. In addition, this study was conducted at a large academic center and variations in referral patterns possibly resulted in a higher PoM in our patient population.
In conclusion, the PoM in nodules with a negative molecular profile as assessed by TSv3 is between 3% and 23%. When malignancies were identified, all were ATA low risk. For TSv3 negative molecular testing results, we believe attention should be paid to the negative subtype. Our data suggest that repeat FNA should be considered for all TSNBL samples. Our study and others 7 have shown that TSCN nodules are more likely to be resected as per either patient or physician reasons, however, optimal surveillance for nonresected TSN and TSCN nodules remains unknown. Based on our institutional experience, we suggest implementation of surveillance US practices for TSN and TSCN nodules similar to the ATA guidelines for nodules with TSBRTC II cytological diagnoses. Repeat biopsy should be considered for change in sonographic features. Whether nodule growth alone should lead to repeat FNA is not known because growth has not been shown to be a reliable identifier of false-negative cytology for nodules with prior TSBRTC II diagnoses. 17 However, because of the higher PoM associated with TSCN versus TSN, repeat FNA may be considered if a TSCN nodule grows. Further research is needed to establish optimal surveillance intervals and duration of follow-up for molecularly benign nodules.
Footnotes
Acknowledgments
A portion of this research was previously presented as an oral presentation at the ATA annual conference held in Chicago, IL, in October 2024. The authors would like to acknowledge the work of Dr. Pablo Valderrabano and his mentor Dr. Bryan McIver for adapting POM calculations for the real-world assessment of molecular testing.
Authors’ Contributions
Conceptualization, methodology, data curation, formal analysis, and writing (original draft) by S.N. Methodology and writing (review and editing) by I.T.R. Conceptualization, data curation, and writing (review and editing) by Z.B. Conceptualization, methodology, formal analysis, writing (review and editing), and supervision by S.J.M.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2