
Abstract
Background:
The necessity of prophylactic central lymph node dissection (p-CLND) in patients with clinically node-negative papillary thyroid carcinoma (PTC) is unclear. The present study evaluated the central lymph node (LN) metastases status in patients with clinically node-negative PTC on both preoperative thyroid ultrasonography (USG) and neck computed tomography (CT) who underwent p-CLND.
Methods:
This retrospective cohort study included 3002 clinically node-negative patients diagnosed with PTC who had undergone thyroidectomy with p-CLND from January 2000 to September 2022. Clinically node-negative was defined as the absence of suspicious metastatic LNs on preoperative USG and neck CT. Low-risk central LN metastases were defined as LN metastases <2 mm in size with metastatic LNs ≤5. The median follow-up duration was 4.52 (interquartile range [IQR]: 1.6–7.5) years.
Results:
Of the 3002 patients, 1194 (39.7%) had central LN metastases, whereas 1808 (60.3%) did not. The 1194 patients with central LN metastases included 507 (16.9%) with intermediate-risk metastases and 610 (20.3%) with low-risk LN metastases, with a total of 2428 (80.5%) patients having low-risk LN metastases or no central LN metastases. High-risk metastases were observed in only 77 (2.5%) patients. Of the 584 patients with intermediate-/high-risk metastases, 577 (98.8%) had central LN metastases <1 cm in size, whereas only 7 (1.2%) had central LN metastases ≥1 cm. The disease recurrence rates for the no LN metastases, low-risk LN metastases, and intermediate-/high-risk LN metastases groups were 0.4%, 1.1%, and 1.9%, respectively (p = 0.012). Factors independently associated with intermediate-/high-risk central LN metastases included age <55 years (odds ratio [OR] = 2.29), male sex (OR = 2.33), tumor size >1 cm on USG (OR = 1.94), and the presence of extrathyroidal extension on CT scans (OR = 1.53), with p < 0.001 for all factors.
Conclusions:
Most LNs confirmed after CLND in cN0 PTC patients assessed by USG and CT were either metastasis-free or classified as low-risk metastatic LNs. Furthermore, the majority of metastatic LNs were small in size, typically measuring <1 cm. p-CLND may be unnecessary if preoperative thyroid USG and neck CT show no evidence of central neck LN metastaes.
Introduction
Over the past few decades, the incidence of thyroid cancer has continued to rise, with papillary thyroid carcinoma (PTC) being the most common subtype. PTC typically metastasizes through lymph nodes (LNs), with the cervical LNs being the most frequent site of recurrence after initial treatment. 1,2 Accurately determining the presence of LN metastasis before thyroidectomy is therefore crucial, not only for deciding the extent of surgery but also for avoiding unnecessary central neck LN dissection.
The necessity of p-CLND in clinically node-negative (N0) thyroid cancer patients remains unclear. Advocates claim that CLND could reduce potential locoregional recurrence because central LN metastasis is common in patients with very small PTCs. 3 –5 By contrast, opponents argue that CLND cannot reduce rates of local recurrence and death but can increase risks of complications, such as permanent hypocalcemia and recurrent laryngeal nerve injury. 6,7 In addition, thyroid ultrasonography (USG) and neck computed tomography (CT) have been reported to be sufficiently sensitive to detect metastatic cervical LNs. 8 –10 Furthermore, micrometastases (very small-sized metastatic foci) are common in p-CLND specimens, but their clinical meaning is unclear.
Current guidelines recommend thyroid USG as the primary and fundamental tool for diagnosing cervical LN metastases in patients with thyroid cancer. 11 More recently, however, the combination of thyroid USG and neck CT has been reported to be more sensitive than thyroid USG alone. 8,9 Furthermore, neck CT has been shown accurate in assessing cervical LN metastases, especially in areas challenging to evaluate by USG, such as the retropharyngeal and superior mediastinal areas. 10,12 For these reasons, along with the advantage it provides surgeons in accurately understanding patients’ anatomical structures preoperatively, an increasing trend in the use of preoperative neck CT in PTC patients can be reasonably anticipated.
The necessity of p-CLND is unclear in patients with PTC who have no evidence of central neck LN metastasis on both thyroid USG and neck CT. The present study therefore evaluated central LN metastases in patients who underwent p-CLND with no evidence of cervical LN metastases on both preoperative thyroid USG and neck CT.
Materials and Methods
Study design and population
This retrospective cohort study reviewed the medical records of 18,344 patients diagnosed with PTC who underwent thyroidectomy from January 2000 to September 2022 at a tertiary medical center (Asan Medical Center). Among these, 7601 patients who underwent both neck CT and thyroid USG, excluding those with only thyroid USG, were included. Subsequently, patients were excluded if they had clinically positive or indeterminate LNs in the central/lateral neck, did not undergo CLND, had abnormal thyroid function tests, or had missing data. Finally, the study cohort consisted of 3002 patients with clinically N0 PTC on thyroid USG and neck CT who underwent thyroidectomy with CLND (Fig. 1). This study was approved by the Institutional Review Board of Asan Medical Center (No. 2023-0006), which waived informed consent due to its retrospective nature.
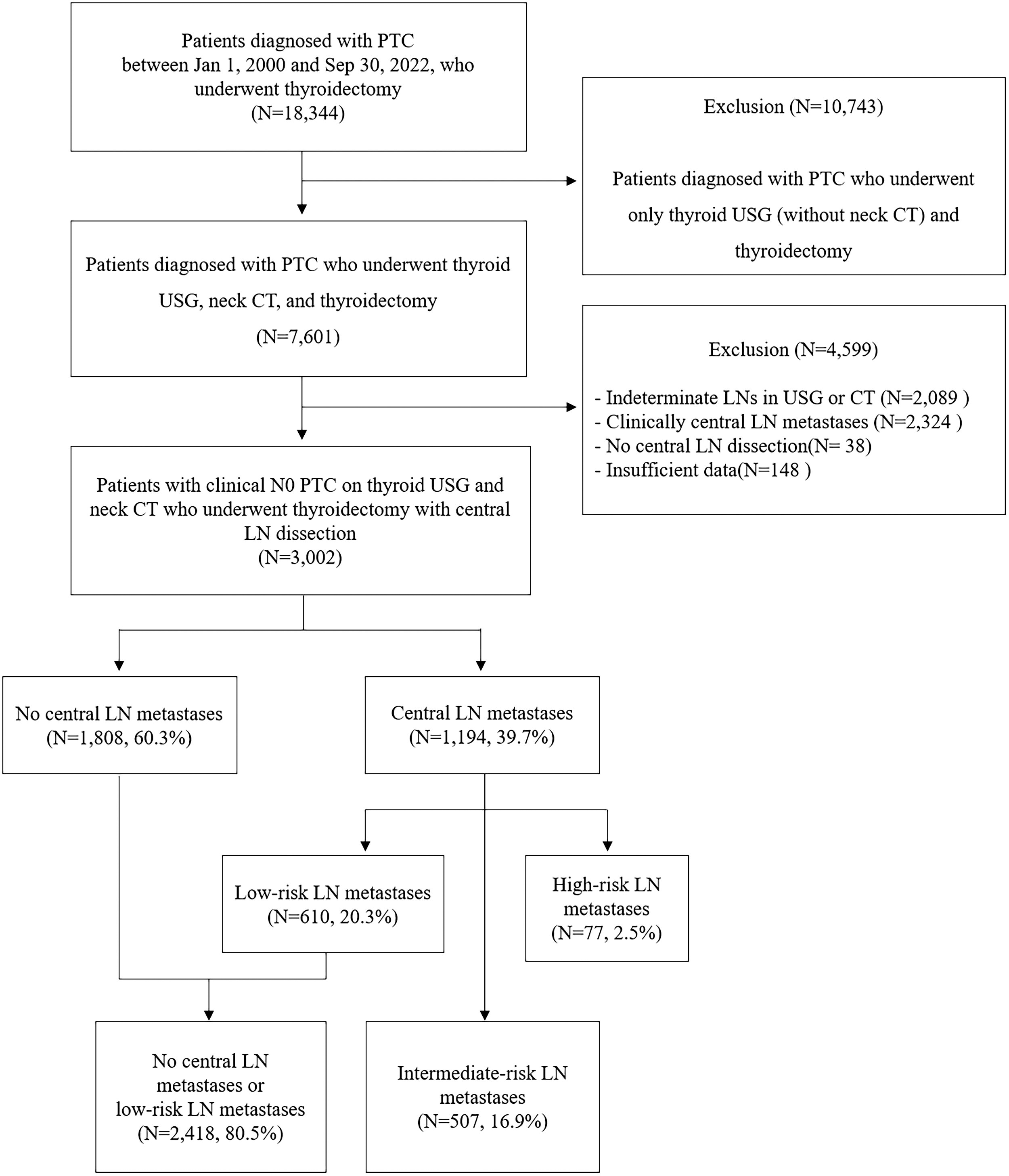
Study flowchart depicting the grouping of the patient population. CT, computed tomography; LN, lymph node; PTC, papillary thyroid carcinoma; USG, ultrasonography.
Preoperative USG
High-resolution USG using a linear-array broadband transducer captured gray-scale and color Doppler thyroid and neck images. Cervical LNs were categorized as suspicious, indeterminate, or benign based on ultrasonographic features. LNs were considered positive for metastasis if any displayed calcification, cystic changes, hyperechogenicity compared to adjacent muscles, or a peripheral chaotic Doppler pattern. Indeterminate LNs were defined as the loss of echogenic hilum and hilar vascularity. Imaging results were evaluated and USG-guided fine needle aspiration (FNA) was performed based on the criteria of the Korean Thyroid Image Reporting and Data System (K-TIRADS). 13
Preoperative neck CT
Neck CT was performed using 128-channel multidetector scanners. The protocol included unenhanced CT scanning from the skull base to the aortopulmonary window to detect calcifications in neck LNs. After contrast injection, arterial and delayed phase scans were performed at 25 and 70 seconds, with 0.6 mm collimation. Cervical LNs were classified as suspicious of metastasis, indeterminate, or probably benign based on their CT features. LN metastasis was suspected if LNs displayed calcification, cystic changes, strong enhancement without hilar vessel enhancement, or heterogeneous enhancement on CT. Indeterminate LNs were defined as the loss of hilar fat and vessel enhancement with no suspicious features. Imaging results were evaluated using K-TIRADS criteria. 13
Surgical strategy and postoperative pathology
All patients were preoperatively diagnosed with suspicious thyroid nodules through FNA or core needle biopsy (CNB), which were confirmed as PTC. Hemithyroidectomy removed one lobe with the isthmus and pyramidal lobe, while total thyroidectomy removed all thyroid tissue. CLND involved removing the pretracheal, paratracheal, and prelaryngeal LNs on the inner side of the internal carotid artery. CLND accompanying total thyroidectomy could be unilateral or bilateral, depending on the surgeon’s preference. The extent of surgery (total thyroidectomy or hemithyroidectomy) was based on the American Thyroid Association’s risk stratification criteria. 14
Postoperative pathological results were evaluated by an experienced pathologist. LN metastasis was defined as the confirmation of the spread of cancer cells from the thyroid gland to the regional LNs. LN metastases <2 mm were defined as micrometastases, whereas LN metastases ≥2 mm were defined as macrometastases. 15 Low-risk central LN metastasis was defined as having metastatic central LNs ≤5, with all metastatic LNs classified as micrometastases. Intermediate-risk LN metastasis was defined as either (1) 2 mm ≤ metastatic LNs < 3 cm, regardless of the number of metastatic LNs, or (2) metastatic LNs < 3 cm with metastatic central LNs >5. High-risk central LN metastasis was defined as having any metastatic central LNs ≥3 cm in size, regardless of the number of metastatic LNs. 14,16,17 Microscopic extrathyroidal extension (m-ETE) referred to tumor extension beyond the thyroid capsule into nearby soft tissue without invasion. Extranodal extension (ENE) refers to the migration of tumor cells beyond the LN capsule into adjacent perinodal tissue.
Outcomes and statistical analysis
In this study, clinically significant central LN metastases are defined as metastatic LNs categorized as intermediate or high risk by ATA guidelines, reflecting an increased risk of disease recurrence associated with central LN metastases. 14 Disease recurrence included metastasis in the central/lateral compartments or new metastatic lesions, but excluded recurrence in the remnant thyroid gland. Disease recurrence was confirmed cytologically or histologically based on suspicious USG or CT findings. Postoperative bleeding was defined as a hematoma at the surgical site requiring reoperation for bleeding control. Recurrent laryngeal nerve (RLN) injury was defined as the presence of voice changes confirmed by laryngoscopy. Transient hypoparathyroidism was defined as a postoperative serum intact-parathyroid hormone level below the normal range (10–57 pg/mL) accompanied by hypocalcemia (serum calcium <8.6 mg/dL), requiring calcium supplementation, and if the same condition persisted beyond 6 months after surgery, it was classified as permanent hypoparathyroidism.
Continuous variables were presented as median values (interquartile range) and analyzed using the Kruskal-Wallis H test. Categorical variables were presented as counts (%) and compared by Fisher’s exact or χ 2 tests. Univariate and multivariable logistic analyses identified factors significantly associated with central LN metastasis. Two-way interaction terms were included in the multivariable logistic regression to assess their effect on LN metastasis. Statistical reliability was ensured with an events-per-variable (EPV) ratio ≥20. Multicollinearity was evaluated using the variance inflation factor (VIF), with a threshold of 10. Model fit was assessed with the Hosmer-Lemeshow test, and subgroup event counts were reviewed for sufficient observations. All statistical analyses were performed using SPSS Statistics version 26 (IBM Corp., Armonk, NY), with p-values <0.05 considered statistically significant.
Results
Clinical characteristics of patients
Among 3002 patients who underwent thyroidectomy with CLND, 1194 (39.7%) were positive and 1808 (60.3%) negative for central neck LN metastases. The 1194 patients with central LN metastases included 610 (20.3%) with low-risk LN metastases, 507 patients (16.9%) with intermediate-risk LN metastases, and 77 patients (2.5%) with high-risk LN metastases. Among all 3002 patients, 2418 (80.5%) were negative for central LN metastases or had low-risk LN metastases (Fig. 1).
The preoperative clinical characteristics of patients by central LN metastases risk groups are shown in Table 1. The proportion of patients aged ≤55 years and males increased with higher LN metastasis risk, from the no LN metastasies group to the low-risk and intermediate-/high-risk groups (65.3% vs. 77.9% vs. 80.5% for age; 18.0% vs. 25.2% vs. 34.6% for male patients; p < 0.001). The median tumor size on USG was similar between the no LN metastases and low-risk LN metastases groups but was slightly larger in the intermediate-/high-risk LN metastases group (0.8 cm vs. 0.8 cm vs. 1.0 cm, p < 0.001). The proportion of patients with a tumor size >1cm on USG increased with the risk of LN metastases (27.8% vs. 32.8% vs. 44.2%, p < 0.001).
Preoperative Clinical Characteristics of Patients by Central LN Metastases Risk Groups
CT, computed tomography; ETE, extrathyroidal extension; IQR, interquartile range; LN, lymph node; TSH, thyroxine-stimulating hormone; USG, ultrasonography.
The total thyroidectomy rates were similar in the no LN metastases and low-risk LN metastases groups but higher in the intermediate-/high-risk LN metastases group (35.5% vs. 33.8% vs. 41.4%, p = 0.012). The proportion of patients with ETE on CT was also similar between the no LN metastases and low-risk LN metastases groups but was higher in the intermediate-/high-risk LN metastases group (21.7% vs. 19.3% vs. 31.2%, p < 0.001). There were no significant differences in median preoperative thyroxine-stimulating hormone concentrations, the proportion of patients with gross ETE on CT, the type of ETE on CT, or multifocality on USG.
The postoperative pathological characteristics of patients by central LN metastases risk groups are shown in Table 2. The classical PTC subtype was slightly more common in low- and intermediate-/high-risk LN metastases groups than in the no LN metastases group (88.9% vs. 93.4% vs. 94.1%, p < 0.001). Median pathological tumor size was similar across groups (1.0 cm vs. 1.1 cm vs. 1.2 cm, p < 0.001). The intermediate-/high-risk LN metastases group exhibited significantly higher values compared to the low-risk LN metastases group for median metastatic LN size (3.0 mm vs. 1.0 mm, p < 0.001), number of retrieved LNs (7.0 vs. 6.0, p < 0.001), number of metastatic LNs (3.0 vs. 1.0, p < 0.001), and LN ratio (0.4 vs. 0.2, p < 0.001). Among intermediate-/high-risk LN metastases patients, 13.2% had ENE, with a median size of 1.0 mm. All patients classified as having high-risk LN metastases were categorized as such solely due to the presence of ENE.
Postoperative Pathological Characteristics and Outcomes of Patients by Central LN Metastases Risk Groups
ENE, extranodal extension; PTC, papillary thyroid carcinoma; RAI, radioactive iodine; N/A, not applicable.
Radioactive iodine (RAI) therapy rates increased with higher LN metastasis risk (16.4% vs. 29.7% vs. 39.9%, p < 0.001), and the median treatment dose was higher in the low-risk and intermediate-/high-risk groups. The detailed protocol for RAI treatment is provided in Supplementary Table S1. Disease recurrence rates also increased with LN metastasis risk (0.4% vs. 1.1% vs. 1.9%, p = 0.012), with a median follow-up duration of 4.52 years (IQR: 1.6–7.5 years).
Among 584 patients with intermediate-/high-risk LN metastases, 85.2% had metastatic LNs <5mm in size, 98.8% had LNs <1cm, and only 1.2% had LNs ≥1 cm, with 85.0% of patients having a number of metastatic LNs ≤5 (Fig. 2).

Size and number distribution of intermediate-risk central LN metastases (N = 584).
Table 3 presents postoperative complications. A total of 310 patients (10.3%) experienced complications, including bleeding in 20 patients (0.7%), transient hypoparathyroidism in 249 patients (8.2%), permanent hypoparathyroidism in 22 patients (0.7%), and RLN injury in 19 patients (0.4%). There were no statistically significant differences in complication rates across the central LN metastasis risk groups.
Surgical Complications According to Central LN Metastases Risk Groups
RLN, recurrent laryngeal nerve.
Factors associated with metastatic central LNs
Multivariable logistic regression analysis showed that age <55 years (odds ratio [OR]: 1.90, 95% confidence interval [CI]: 1.53–2.36), male sex (OR: 1.52, CI: 1.22–1.90), tumor size >1 cm on USG (OR: 1.29, CI: 1.05–1.58) were independent factors associated with low-risk central LN metastasis (Table 4, a). Factors independently associated with intermediate-/high-risk central LN metastasis included age <55 years (OR: 2.29, CI: 1.81–2.89), male sex (OR: 2.33, CI: 1.88–2.89), tumor size >1 cm on USG (OR: 1.94, CI: 1.58–2.37), and ETE (CT) (OR: 1.53, CI: 1.23–1.91). To evaluate potential interaction effects, two-way interaction terms were included in the model. However, none of the interactions were statistically significant (Table 4, b). Factors independently associated with intermediate-/high-risk LN metastasis, with low-risk LN metastasis as the reference, showed similar results except for the factor of age <55 years (Table 4, c).
Univariate and Multivariable Logistic Regression Analysis of Factors Related to Central Neck LN Metastases
CI, confidence interval; OR, odds ratio.
Discussion
The necessity of p-CLND in clinically N0 PTC patients remains unclear. A systematic review and meta-analysis of 18,376 PTC patients reported lower locoregional recurrence rates in those who underwent p-CLND. 4 More recent studies, however, including a randomized controlled trial involving 60 PTC patients, have reported a lack of association between the performance of p-CLND and disease recurrence. 18 Furthermore, microscopic central neck metastases were found to have little clinical significance. For example, active surveillance has been shown feasible for biopsy-proven metastatic cervical LNs <2 mm over 6–12 months, suggesting small LN metastases rarely affect papillary thyroid microcarcinoma prognosis. 19 ,20 Furthermore, according to the 2015 ATA guidelines, the neck nodal size threshold for recommending surgical treatment of biopsy-proven neck nodes in a previously operated compartment was central neck nodes ≥8 mm and lateral neck nodes ≥10 mm. 14 In the present study, 16.9% of patients had intermediate-risk LN metastases, 2.5% of patients had high-risk LN metastases, whereas 80.6% did not have central LN metastases or exhibited low-risk LN metastases. Only seven (1.2%) patients had central LN metastases ≥1 cm. These findings provide further evidence that small-sized cervical metastatic LNs may have little clinical significance. Furthermore, p-CLND was associated with higher rates of complications, such as permanent hypocalcemia and recurrent laryngeal nerve injury. 6,21
The present study used both thyroid USG and neck CT scans as basic components of preoperative evaluation. This combination has been reported as more advantageous than USG alone for the detection of central neck LN metastasis in patients with PTC. 9,10,22 For example, a meta-analysis reported CT was more sensitive (39% vs. 28%) but less specific (87% vs. 95%) than USG for detecting central neck metastases. 22 Another study found CT more sensitive (26.5% vs. 17.8%) but less specific (84.3% vs. 98.4%) than USG, with the combination offering better sensitivity (32.4%) and negative predictive value (NPV, 63.6%) than either modality alone. 10 In the present study, 60.3% of patients with clinically N0 PTC by combined USG and CT were confirmed on final pathology to have no central neck LN metastases. Furthermore, among the initial cohort of 7601 patients in this study, all of whom underwent both thyroid USG and CT, 277 patients demonstrated either CT findings suggestive of central LN metastasis or suspicious central LN metastasis, while no corresponding findings were observed on USG. These findings suggest that the combination of USG and CT is more beneficial in detecting central neck LN metastases and in predicting the absence of these metastases than USG or CT alone, potentially allowing the omission of p-CLND.
A randomized controlled trial evaluating the benefits of p-CLND in 60 patients with USG-determined clinically N0 PTC found no significant differences in oncologic outcomes between groups that did and did not undergo CLND. 18 An analysis in 295 patients with USG-determined clinically N0 low-risk differentiated thyroid carcinoma found that central neck dissection did not affect the rates of complete remission or tumor progression. 23 Furthermore, a study of 11,569 patients with cN0 PTC found that p-CLND did not significantly reduce locoregional recurrence rates, but increased the incidence of hypoparathyroidism. 21 In these studies, oncologic outcomes were similar between patients with and without CLND, and CLND did not reduce locoregional recurrence. The patients included in these studies were primarily preoperatively assessed using USG. In the present study, all patients were preoperatively assessed using a combination of USG and neck CT. p-CLND was performed in all clinically N0 patients, and the majority of these patients either had no central LN metastases or exhibited low-risk LN metastases. Considering the benefits of combined CT/USG for detecting LN metastasis and the outcomes of prior studies using USG alone, omitting CLND would likely yield favorable outcomes. However, adding neck CT scans to USG in PTC patients has drawbacks, including higher costs, radiation exposure, and potential upstaging, which may lead to unnecessary total thyroidectomy or therapeutic LN dissection.
Although the median tumor size on preoperative USG and the median pathological lesion size after surgery showed statistically significant differences among the three groups, the differences in tumor size were relatively small and may have limited clinical impact. In contrast, a clinically significant difference was observed in the proportion of tumor size >1cm on preoperative USG across the three groups, with the highest proportion notably in the intermediate-/high-risk LN metastases group. This finding suggests that tumor size >1cm on USG may be more closely associated with the risk of central LN metastasis.
A systematic review found that factors associated with central neck LN metastasis in patients with cN0 PTC included age <45 years, male sex, tumor size >1 cm, ETE, capsular invasion, and lymphovascular invasion. 24 In addition, a study of 39,562 patients found that age <45 years, male sex, and tumor size >1 cm were risk factors associated with central LN metastasis. 25 Similar results were observed in the present study, with age <55 years, male sex, and tumor size >1 cm on USG, and the presence of ETE on CT being factors independently associated with intermediate-/high-risk LN metastases, without significant interaction among these factors. While these factors may serve as useful indicators for performing p-CLND, we cannot recommend routine p-CLND in these patients. The difference in local recurrence between p-CLND and non-p-CLND is minimal, 6,7 and the retrospective nature of this study necessitates cautious interpretation of the results. Further studies are required to validate these findings.
This study had several limitations, including its retrospective, non-randomized, single-center design, which may introduce selection bias. Additionally, disease recurrence rates were not directly compared between groups of patients with cN0 PTC who did and did not undergo CLND based on neck CT and USG findings. However, this study had a notable strength in examining the characteristics of LN metastasis following central neck LN dissection in a relatively large cohort of patients with cN0 PTC. Another limitation was the potential variability in neck CT protocols, which likely differ from those in other institutions. This study did not analyze the cost-effectiveness of routinely adding neck CT to preoperative patient evaluation.
In conclusion, most LNs confirmed after central neck LN dissection in cN0 PTC patients assessed by USG and CT were either metastasis-free or low-risk metastatic LNs. The majority of metastatic LNs were small, typically measuring <1 cm. These findings suggest that p-CLND may be unnecessary in patients with no evidence of central neck LN metastasis on both thyroid USG and neck CT.
Footnotes
Authors’ Contributions
B.-C.K.: Writing—original draft (lead), formal analysis (lead). S.J.P., D.K., W.W.K., Y.-M.L., and T.-Y.S.: Conceptualization (supporting). W.G.K., W.B.K., J.H.B., J.H.L., Y.J.C., and D.E.S.: Conceptualization (supporting), methodology (supporting), writing—review and editing (equal). K.-W.C.: Conceptualization (lead), methodology (lead), writing—original draft (supporting), writing—review and editing (equal).
Author Disclosure Statement
None of the authors has anything to disclose.
Funding Information
None of the authors has any funding information to declare.
Supplementary Material
Supplementary Table S1