
Abstract
Introduction:
The increasing incidence of differentiated thyroid carcinoma (DTC) in children and adolescents has become a growing concern. This study provides the first extensive assessment of incidence patterns and temporal trends of pediatric DTC in Germany, using the best available data from the German Malignant Endocrine Tumor (MET) Registry and the German Childhood Cancer Registry (GCCR) covering a period of 25 years.
Patients and Methods:
We conducted a register-based incidence and time series analysis, identifying all children and adolescents diagnosed with DTC at ages 0–17 years between 1997 and 2021 in Germany, as recorded in the German MET Registry and/or the GCCR. Age-specific and age-standardized incidence rates (ASR) over time, average annual percentage changes (AAPC), and cross-tabulations were used to evaluate incidence and temporal patterns.
Results:
We identified 469 DTC cases, including 85.7% papillary thyroid cancer and 9.4% follicular thyroid cancer. The average ASR for the period 1997–2021 was 1.16 per million, with higher rates in females compared with males (1.64 vs. 0.72 per million, respectively). Incidence rates increased with increasing age. The overall ASR increased from 0.84 per million in 1997–2001 to 1.48 per million in 2017–2021, with an AAPC of 3.46% [confidence interval or CI: 2.12–4.83]. The increase was most pronounced in adolescents aged 15–17 years (AAPC: 6.79% [CI: 4.43–9.19]). The proportion of incidentalomas rose from 5% in 1997–2001 to 26% in 2017–2021, yet we observed no marked shift in tumor size between symptomatic and incidental cases.
Conclusions:
Our study revealed a significant increase in pediatric DTC incidence in Germany, most pronounced among adolescents. The observation of an increasing incidence mirrors global trends and presents a complex public health challenge. While improved detection likely contributes to this trend, the stable tumor size distribution suggests that other factors are also in play. The rising detection of incidentalomas suggests enhanced diagnostic practices unrelated to symptoms of thyroid neoplasia. These findings highlight the need to carefully evaluate diagnostic and screening practices in pediatric populations.
Introduction
The increasing incidence of differentiated thyroid carcinoma (DTC) in children and adolescents has become a growing concern. While relatively rare, with reported incidence rates of 1–3 per million children and adolescents, 1 DTC represents the most common endocrine malignancy in this age group, accounting for 0.5–1.5% of all pediatric cancers. 2,3 Several recent international publications indicate a significant increase in DTC incidence, 4 –10 eliciting a comprehensive assessment of DTC epidemiology, etiological factors, and implications for public health and clinical practice.
The upward trend in pediatric thyroid cancer incidence, including both differentiated and medullary thyroid carcinoma (MTC), has been documented across regions worldwide. In the United States, Siegel et al. 11 reported an average annual percentage change (AAPC) of 4.2% from 2003 to 2019 among 0–19-year-olds. Similarly, Lee et al. 12 observed an AAPC of 4.0% in South Korea from 2004 to 2016, with a notable female predominance. In Europe, Loizou et al. 13 reported a significant increase in Cyprus, with an average increase of 7.6% annually. Similar trends have been also observed in Canada, 14 South America, 14,15 Asia 14 (excluding Kuwait, Philippines, and Thailand), Oceania, 14 and various European countries, 6,7,14 particularly following the Fukushima and Chornobyl nuclear accidents.
The underlying causes of the rising incidence of pediatric DTC are speculative and likely multifaceted. The etiology of thyroid cancer remains overall poorly understood. However, several established risk factors have been identified, each potentially contributing to this upward trend. These include (1) childhood exposure to ionizing radiation, 16 –19 including nuclear accidents and associated early detection programs; (2) genetic predispositions, such as DICER1 syndrome 20 and PTEN hamartoma tumor syndrome 21 ; and (3) environmental influences, including iodine deficiency or excess. 22,23 However, also advancements in diagnostic techniques, including high-resolution ultrasound and fine-needle aspiration cytology, may have contributed to the observed rise in incidence. 24 Moreover, improvements in reporting and registration, heightened awareness among health care providers and the public, and better access to health care services have likely contributed to increased case identification. 9
Understanding DTC trends in children and adolescents is crucial for several reasons: Pediatric DTCs often display distinct biological behaviors compared with adult patients, necessitating age-specific research. Given the young age at diagnosis, pediatric patients with DTC face potential long-term effects of both the disease and its treatment. The increasing detection of incidental thyroid nodules raises questions about potential overdiagnosis and subsequent overtreatment in a vulnerable population.
Here, we present the first comprehensive assessment and critical appraisal of incidence patterns and temporal trends of pediatric DTC in Germany, utilizing the best available data from the German Malignant Endocrine Tumor (MET) Registry and the German Childhood Cancer Registry (GCCR). Specifically, our objectives were to:
Present incidence pattern and temporal trends in DTC incidence among children and adolescents in Germany from 1997 to 2021. Identify demographic and clinical characteristics associated with increased DTC incidence in this population.
Finally, we sought to compare incidence trends in Germany with those observed in other countries to contextualize our findings within a global framework.
Patients and Methods
Design and study population
We conducted a register-based incidence and time series analysis, pooling data from the German MET Registry and the GCCR. The study population comprised all children diagnosed with a primary DTC (including subsequent primary neoplasms [SPNs]) at ages 0–17 years between 1997 and 2021, residing in Germany at time of diagnosis and registered at the MET Registry and/or GCCR. SPNs were defined as any new primary DTCs occurring in a child or adolescent (at ages 0–17 years) with any previous cancer diagnosis, regardless of the time between those two diagnoses.
The MET Registry was approved by the ethics committees of the University of Luebeck (Institutional Review Board [IRB] 97125) and the Otto-von-Guericke-University Magdeburg (IRB 174/12 and 52/22), Germany. The MET Registry and the GCCR are operating based on written informed consent of the patients and/or their legal guardians. No additional ethics approval and consent were required for this study. The research was carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments including humans.
Data and data sources
The MET Registry, maintained by the German Society of Pediatric Oncology and Hematology (GPOH), collects prospectively detailed clinical, pathological, and follow-up data on patients aged 0–17 years. Collected information encompasses demographic information (age, sex), clinical presentation, diagnostic modalities, histopathological findings, therapeutic interventions, and outcomes; relevant data were extracted from medical records.
The GCCR is an epidemiological cancer registry, monitoring incident cases of pediatric malignancies and nonmalignant intracranial and intraspinal tumors in Germany since 1980, with national coverage in former Western Germany and full nationwide coverage since 1991 (after the German reunification). 25 Until 2009, cancers diagnosed at ages 0–14 years were registered; thereafter, registration was expanded to include children aged 0–17 years at diagnosis. Contrary to the MET Registry, the GCCR does not register extended clinical information. Registration is based on voluntary reporting by all pediatric hematology–oncology units and written informed consent of the respective caregivers and patients. During the initial buildup phase in the early 1980s, the GCCR quickly established a close and well-functioning network with treating hospitals and the GPOH and thereby reached high reporting completeness levels of above 95% for all pediatric cancers combined (diagnosed at ages 0–14 years). 26
Diagnostic criteria and tumor classification
We defined DTC according to the World Health Organization classification of tumors of endocrine organs applicable at the time of diagnosis. Tumor staging followed the American Joint Committee on Cancer/tumor node metastasis system in use at the time of diagnosis. 27
At the GCCR, cancer diagnoses are coded according to the International Classification of Childhood Cancer–Third Edition (ICCC-3). 28
The Yellow Booklet Program in Germany
In Germany, the Yellow Booklet Program was developed in the 1970s as a national preventive health initiative for children and adolescents. It provides a structured series of medical checkups (U-/J-Untersuchungen) aimed at early detection of diseases and developmental disorders. For pediatric thyroid cancer, the program facilitates the identification of thyroid nodules, which are then further investigated, potentially improving early detection rates of pediatric DTC. The program continues to be a cornerstone of preventive care and remains in operation, helping clinicians track health outcomes and intervene early where necessary.
Analytical sample
All diagnosis registered at the GCCR and classified to ICCC-3 group XI(b) with a morphology code compatible to DTC (8260/3, 8330/3, 8331/3, 8340/3, and 8341/3) were extracted to be eligible for the analytical sample set.
Information on DTC cases in the MET and GCC registries was compared, and discordant diagnostic information (incompatible morphology codes) was eliminated using an a priori developed decision matrix. Given that the GCCR covered only cancer diagnoses in children aged 0–14 years before 2009, data for patients aged 15–17 years diagnosed during 1997–2008 were solely available from the MET Registry.
Statistical analysis
We calculated age-specific and age-standardized incidence rates (ASR) for the entire study period (1997–2021) and by five-year diagnostic periods. The ASRs were calculated through direct age-standardization using the Segi 1960 World Standard Population 29 and expressed per million children and adolescents. Annual population estimates by age and sex were obtained from the German Federal Statistical Office. 30
We stratified analyses by DTC type (papillary thyroid cancer [PTC] and follicular thyroid cancer [FTC]), sex (female and male), and age at diagnosis (0–9, 10–14, and 15–17 years). For the graphical representation of incidence trends over time, a locally estimated scatterplot smoothing with linear interpolation was applied to the ASRs or else age-specific incidence rates by calendar year. To evaluate the direction and magnitude of incidence trends over time, we used Joinpoint regression. 31 Herewith, we estimated the AAPC and corresponding confidence intervals (CI) in incidence rates for 1997–2021.
Based on clinical data from the MET Registry, distributions of DTC detection methods (symptomatic tumor vs. incidentaloma) and tumor size (0 to ≤1, >1 to <2, ≥2 to 4, and >4 cm) by diagnosis period were calculated.
Analyses were performed using SAS Software 9.46 32 and Joinpoint Regression Program, version 4.9.1.0, National Cancer Institute. 31
Results
Our analytical dataset comprised 469 diagnoses of DTC, of which five diagnoses were only registered at the MET Registry and 53 diagnoses only at GCCR. Overall, 88 (18.8%) were SPNs. PTCs comprised 85.7%, while FTC comprised 9.4% of all DTCs. Females were more frequently diagnosed than males (68.9% vs. 31.1%). Children diagnosed at ages 10–14 years accounted for 53.3% and adolescents aged 15–17 years accounted for 30.7% of the total diagnoses (Table 1). The average ASR of DTCs overall for the study period (1997–2021) was 1.16 per million. We observed an ASR more than twice as high in females compared with males (1.64 vs. 0.72 per million) and an age-specific incidence rate six times higher in 10–14-year-olds and 15–17-year-olds compared with younger children (2.44 and 2.24 vs. 0.40 per million) (Table 1).
Number of Newly Diagnosed Children as Well as Age-Standardized and Age-Specific Incidence Rates with Corresponding Confidence Intervals of Differentiated Thyroid Cancer in Children Aged 0–17 Years in Germany (1997–2021)
Refers to the proportion of the column.
Including differentiated thyroid cancer, dedifferentiated thyroid cancer, poorly differentiated thyroid cancer, not otherwise specified thyroid cancer, not shown due to small numbers.
ASR, age-standardized incidence rate; CI, confidence interval; DTC, differentiated thyroid cancer; FTC, follicular thyroid cancer; N, number; PTC, papillary thyroid cancer; SPN, subsequent primary neoplasm.
The time trend analysis revealed a moderately increasing trend across all (sub-)groups. The ASR for DTC overall among 0–17-year-olds increased from 0.84 per million during 1997–2001 to 1.48 per million in most recent years (2017–2021) (Table 1, Fig. 1A), resulting in an average annual increase of 3.46% [CI: 2.12–4.83] (Table 2).

Age-standardized incidence rates (ASRs) per million children and adolescents with confidence intervals for differentiated thyroid cancer in children diagnosed
Average Annual Percentage Changes and Corresponding Confidence Intervals of Age-Standardized and Age-Specific Incidence Rates of Differentiated Thyroid Cancer in Children Aged 0–17 Years by Subtype, Sex, and Age at Diagnosis (1997–2021)
Including differentiated thyroid cancer, dedifferentiated thyroid cancer, poorly differentiated thyroid cancer, not otherwise specified thyroid cancer.
Until 2009, the GCCR registered only cancer diagnoses in children aged 0–14 years, the respective AAPC should be interpreted with caution.
AAPC, average annual percentage changes; GCCR, German Childhood Cancer Registry; n.a., not applicable.
Consistent with the overall pattern, the ASR of the most common DTC type, PTC, increased by an average of 3.51% [CI: 1.86–5.19] per year, from 0.67 to 1.24 per million (Tables 1 and 2). The increasing trend was evident among both males and females (Table 1, Fig. 2). Results of the Joinpoint regression analysis revealed that the increase was somewhat stronger among males compared with females (AAPC: 4.61% [CI: 2.06–7.21] vs. AAPC: 2.96% [CI: 1.16–4.79]) (Table 2). Visual inspection of the incidence for children diagnosed at ages 0–14 years indicated a less pronounced increase than for older adolescents (Fig. 1B). This indication was confirmed by the formal time trend analysis, revealing an average annual increase of ASRs among 15–17-year-olds of 6.79% [CI: 4.43–9.19], compared with 2.34% [CI: 0.26–4.46] among the children aged 10–14 years (Table 2, Fig. 3). In contrast, the incidence rate for the age group 0–9 years ranged between 0.31 and 0.48 per million without any noticeable temporal pattern during 1997–2021 (Table 1, Fig. 3). Age-specific trends by sex showed, that whereas the incidence rates in under 10-year-olds (surrogate for before puberty) were similar for boys and girls, incidence rates among 10–14-year-olds (as surrogate for during/after puberty) where notably higher in girls than in boys (Fig. 4).
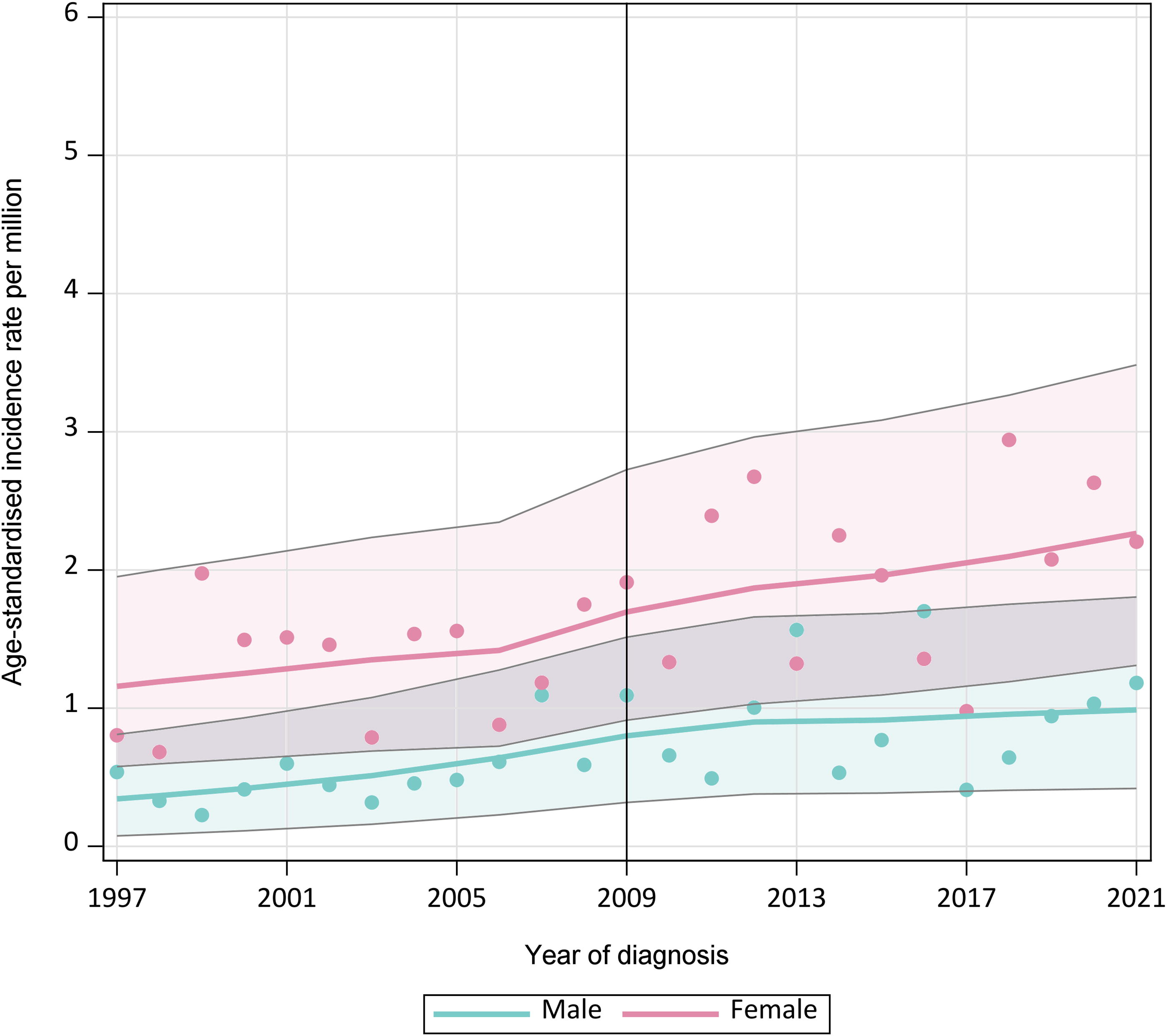
ASRs per million children and adolescents with confidence intervals for differentiated thyroid cancer in boys and girls diagnosed at ages 0–17 years in Germany (1997–2021). ASRs were directly age-standardized using Segi 1960 World Standard Population. LOESS with linear interpolation was applied to the ASRs by calendar year (1997–2021). Until 2009, the GCCR registered only cancer diagnoses in children aged 0–14 years. The reference line in 2009 indicates the time point when the GCCR expanded its registration to under 18-year-olds.
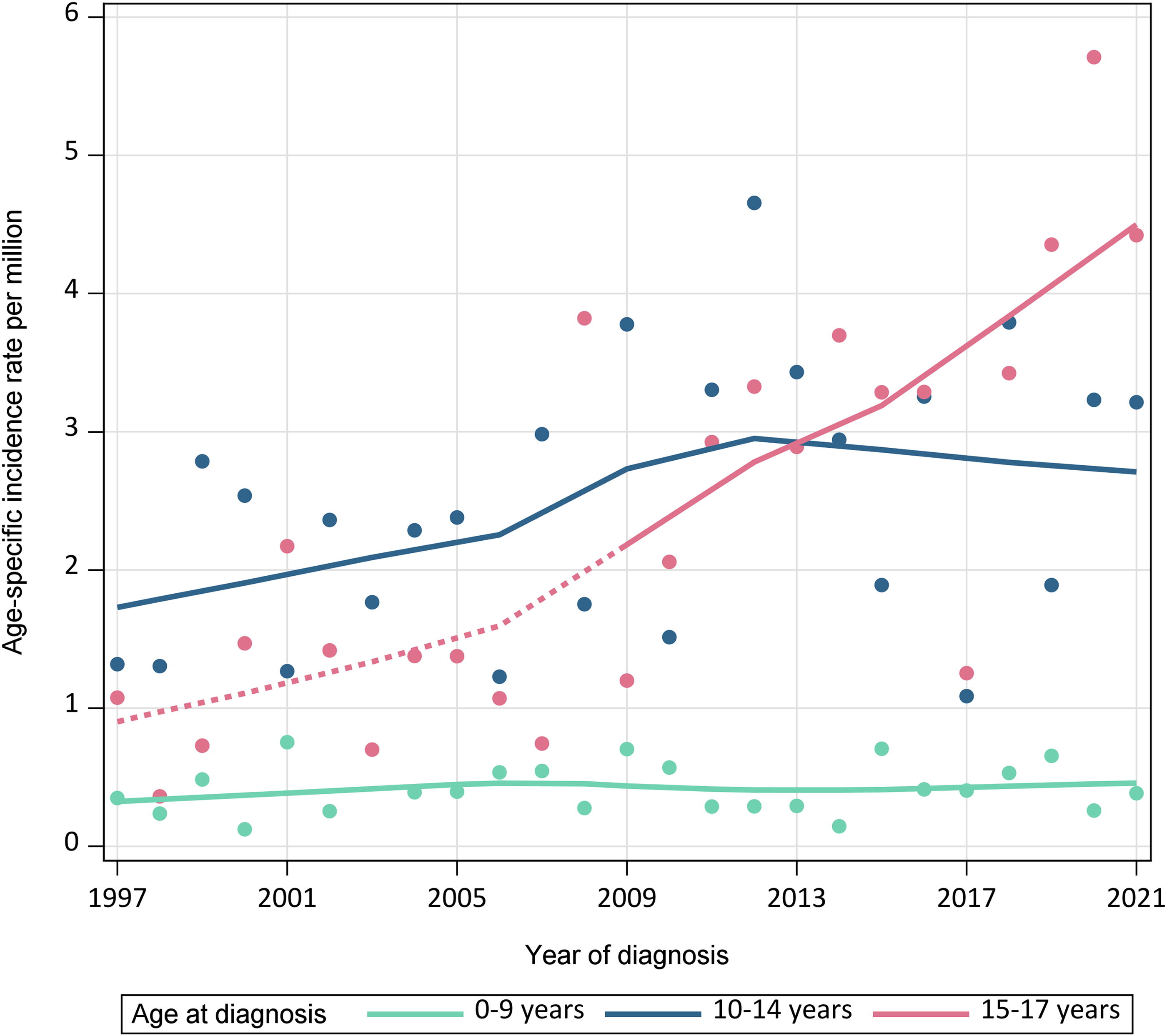
Age-specific incidence rates per million children and adolescents for differentiated thyroid cancer in children diagnosed at ages 0–9, 10–14, and 15–17 years in Germany (1997–2021). LOESS with linear interpolation was applied to the age-specific incidence rates by calendar year (1997–2021). Until 2009, the GCCR registered only cancer diagnoses in children aged 0–14 years. The dashed line reflects the period (1997–2008) when the incidence rates were solely based on data from the German Malignant Endocrine Tumor (MET) Registry.
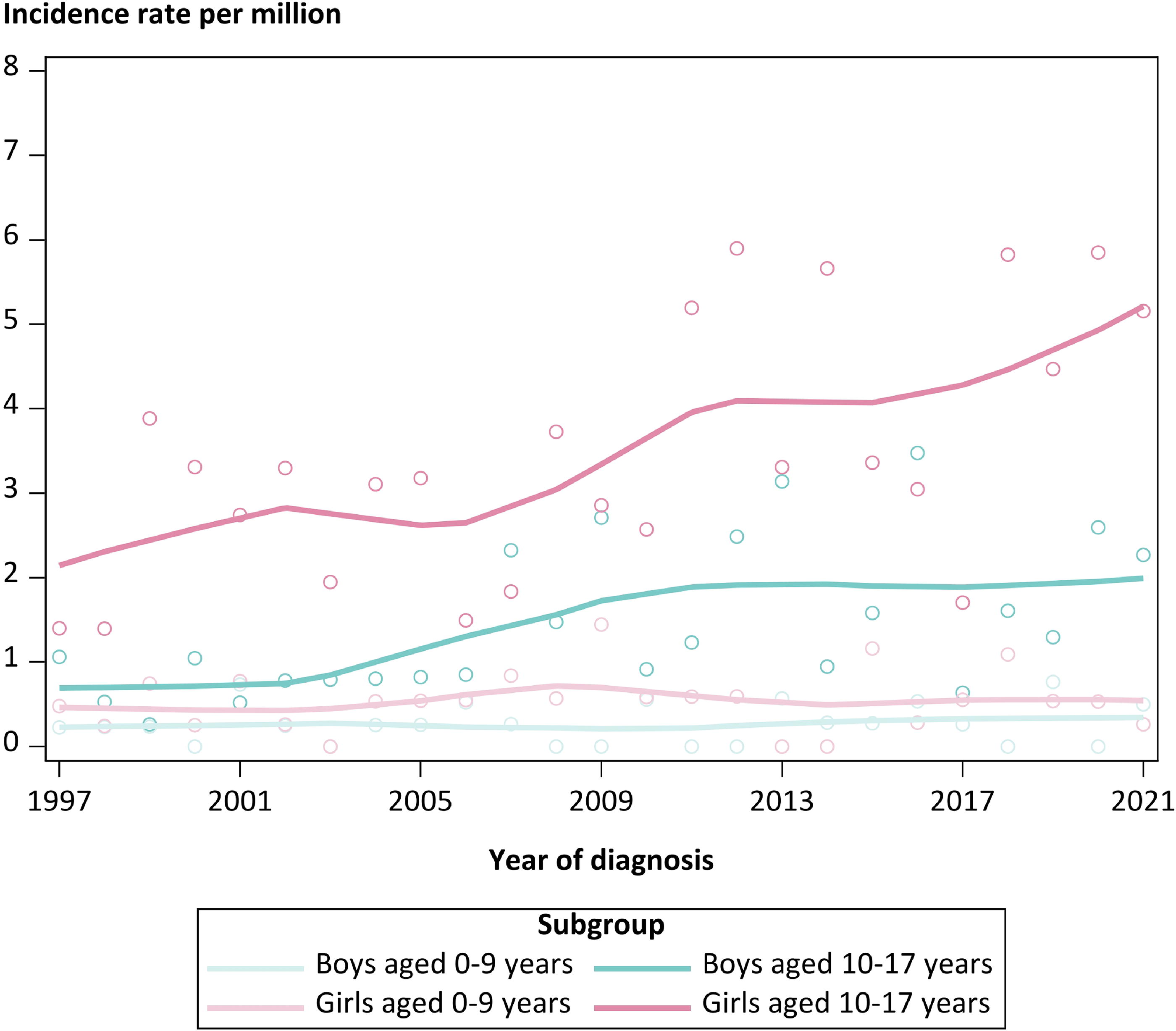
Age-specific incidence rates per million children and adolescents for differentiated thyroid cancer in boys and girls diagnosed at ages 0–9 and 10–14 years in Germany (1997–2021). LOESS with linear interpolation was applied to the age-specific incidence rates by calendar year (1997–2021).
In total, for 379 diagnoses (80.8%) information on tumor size was available in the MET Registry. Most of the patients were diagnosed with tumors sized 2–4 cm (N = 163; 34.8% of the total). There were no shifts in tumor size over time (Table 3).
Tumor Size and Occasion of Detection Among Children and Adolescents with a Differentiated Thyroid Cancer (DTC) Diagnosed at Ages 0–17 Years in Germany over Time
To protect personal integrity and in compliance with GDPR and the GCCR’s informed consent procedure, we do not provide the exact number of observations, but use “<5” to denote subgroups including less than five observed cases.
Refers to the proportion of the column.
For 350 patients (74.6%), information on the occasion of tumor detection was available. Almost half of the patients (46.5%) were diagnosed during an examination due to symptoms suggestive of a tumor, including a palpable neck mass, hoarseness, difficulty swallowing, neck pain, and swollen lymph nodes. While 32 patients (6.8%) were diagnosed during the national early detection program in pediatrics (“Yellow Booklet”), 33 –35 most asymptomatic cases (N = 100; 21.3%) were detected incidentally during other examinations (Table 3). The proportion of incidentalomas (diagnosed during examinations unrelated to suspected cancer) increased considerably over time, from 5% in 1997–2001 to 26% in 2017–2021 (Table 3).
For 329 patients with a DTC, information on both tumor size and tumor detection method was available (Table 4). Among incidentalomas, 22.7% were diagnosed at ≤1 cm; incidentalomas sized >1 to <2 cm and ≥2 to 4 cm accounted for 31.1% and 36.4%, respectively, while 6.1% were diagnosed with tumors larger than 4 cm (Table 4). Notably, the distribution of tumor size did not differ considerably between incidentalomas and symptomatic DTCs (for symptomatic DTC: 10.1%, 25.2%, 45.4%, and 11.9%, respectively) (Table 4).
Tumor Size in Relation to the Occasion of Tumor Detection for DTCs Diagnosed in Children Aged 0–17 Years in Germany (1997–2021)
Refers to the proportion of the column.
If a DTC was diagnosed during an examination due to symptoms of suspected cancer, it was labeled as “tumor-related”; incidentalomas usually are DTCs diagnosed by chance during any other medical examination, for example, by sonography.
Number of missing information of both tumor size and occasion of detection = 69.
Discussion
This nationwide, register-based study provides the first comprehensive assessment of incidence patterns and temporal trends of DTC among children and adolescents in Germany, covering a period of 25 years (1997–2021). Our findings showed an average ASR of 1.16 per million children and adolescents, with notable disparities between sexes and age groups. The AAPC of 3.5% in ASRs reflects the increase in incidence, from 0.84 per million in the late 1990s to 1.48 per million in recent years, highlighting a concerning upward trajectory. This trend is particularly pronounced in adolescents aged 15–17 years with an AAPC of 6.79%.
Our study specifically focuses on DTC, while most publications on pediatric thyroid cancer include both DTC and MTC. Notably, Lebbink et al. 36 reported divergent incidence trends for DTC and MTC among young Dutch patients (0–24 years) over a 30-year period.
Our results align with the global increase in thyroid cancer incidence, although some heterogeneous temporal patterns are observed across countries. 9,15,37 Studies from the United States (Siegel et al., 11 AAPC of 4.2%) and several European countries 7,9 reported similar upward trends, while others, such as the Netherlands 38 and Denmark, 39 have observed stable incidence rates over extended periods. These differences may be influenced by factors such as variations in screening practices; for instance, Germany’s “Yellow Booklet” early detection program differs from the more centralized approaches in the Netherlands and Denmark.
Countries like South Korea (AAPC of 4.0%) 12 and Japan 40 have experienced a more pronounced increase, partly due to heightened public awareness and extensive screening following nuclear events. Additional factors, such as iodine intake and disparities in health care practices across countries, particularly in imaging utilization, likely contribute to these trends; of note, Japan has the highest number of computed tomography scanners per capita worldwide. 41 Our study identified 32 cases through the “Yellow Booklet” program and another 100 cases incidentally detected during other radiological examinations. The relatively low number of cases identified through the “Yellow Booklet” program is not surprising, as it does not include routine ultrasound of the thyroid gland. This highlights the impact of health care access and diagnostic practices. 24
The quality and completeness of cancer registration systems also play a crucial role in capturing accurate incidence trends. Countries with robust, longstanding cancer registries, such as the Netherlands and Denmark, may provide more reliable long-term trend data, whereas increases in countries with less developed or recently established registries may reflect improvements in data collection and reporting over time rather than true changes in incidence.
Although our study indicates an upward trend in DTC incidence, several factors warrant careful consideration. The longstanding registration of DTC cases in both the MET and GCC registries supports the likelihood of a genuine increase. However, the GCCR started registration of patients aged 15–17 years only in 2009, which may have contributed the apparent rise in this age group. Furthermore, the increase in incidentalomas, from 5% in 1997–2011 to 26% in 2017–2021, likely reflects enhanced health care utilization and more frequent use of imaging. 24 Routine preventive health examinations in pediatrics in Germany (“Yellow Booklet” visits) 33 –35 such as the J1 (12–14 years) and J2 (16–17 years), include an assessment of the family history, thyroid hormone levels, and neck palpation. In cases of notable findings, ultrasound may also be conducted, thereby promoting early detection of asymptomatic tumors, similar to practices in South Korea. 12
Interestingly, our study found no difference in tumor size between incidentally detected cases and those diagnosed following symptoms, challenging the assumption that increased detection mainly captures smaller, asymptomatic tumors. However, the large proportion of missing data (30%) limits our ability to draw definitive conclusions. Of note, the slow-growing nature of DTC implies that some cases incidentally detected during childhood in recent years might have been diagnosed later in life in earlier decades.
The absence of a significant difference in tumor size at detection between incidental and symptomatic cases may further reflect limitations in the accuracy of the mode of detection data. Although the mode of detection was provided by the treating or notifying physicians and verified by registry staff where possible, the observed uniformity in tumor size is unexpected from a clinical perspective and suggests that reporting inaccuracies may exist.
Additionally, while no increase in tumors was observed among the youngest age group, this could be attributed to small sample sizes leading to a type II error, or it may indicate that there is no emerging risk factor specifically affecting this group, as an increase in incidence would likely be observed across all age groups if a new risk factor was present.
These findings emphasize the need to evaluate diagnostic and screening practices carefully, balancing the benefits of early detection with the risks of overdiagnosis and overtreatment, especially in pediatric populations for whom long-term consequences of treatment are considerable. 9
The increase in DTC incidence among adolescents aged 15–17 years, with an AAPC of 6.79%, is substantially higher than the 2.34% observed in the 10–14-year age group. This age-specific trend, which aligns with findings from other countries, 9,42 may suggest a role of pubertal hormones in the pathogenesis of DTC, predominantly affecting girls. However, the rise in adolescent incidence may also, at least to some extent, be a result of the expansion of the GCCR and inclusion of 15–17-year-olds in 2009, as outlined above. The observed sex disparity, with females having an ASR more than twice that of males, aligns with global observations 9,42 and suggests hormonal or genetic factors in the development of DTC.
Additionally, it is well established that nutritional iodine supply plays a critical role in the development of goiter and thyroid nodules, including DTC. According to data from the German Health Interview and Examination Survey for Children and Adolescents (KIGGS) surveys, the iodine status of children and adolescents in Germany has worsened significantly in recent years. The surveys revealed a considerable decline in iodine levels from 2009–2012 to 2014–2017, with up to 44% of children and adolescents experiencing mild iodine deficiency. 43 –45 Although no more recent data are available from the Robert Koch Institute (Germany’s federal government agency and research institute responsible for disease control and prevention), it is assumed that iodine deficiency in Germany continues to worsen. This trend could contribute to an increased incidence of thyroid abnormalities, including DTC, and highlights the importance of monitoring iodine intake as part of public health efforts.
Collectively, these factors highlight the complex interplay between genuine risk factors and enhanced surveillance in shaping the observed incidence trends of pediatric DTC. Although our study cannot directly assess the impact of specific environmental factors, environmental influences, such as ionizing radiation exposure, endocrine disruptors, and the rising prevalence of obesity among children and adolescents, may also contribute to the rising risk of DTC. 46 –48 Additionally, genetic susceptibility plays a critical role, with recent studies identifying germline variants that may predispose children to DTC. 49 –51 The interplay between genetic susceptibility and environmental exposures in pediatric populations requires further investigation.
The rising incidence of pediatric DTC has significant implications for health care systems and policy. Enhanced surveillance and early detection strategies must be balanced against the risks of overdiagnosis and overtreatment. 9 Guidelines for the management of thyroid nodules in children and adolescents should be regularly updated to reflect the evolving understanding of pediatric DTC’s natural history.
Future research should focus on long-term prospective studies of incidentally detected thyroid nodules, investigate the impact of obesity and metabolic factors on DTC risk, and evaluate potential environmental risk factors in pediatric populations.
The primary strength of our study lies in its comprehensive nationwide coverage and long study period of 25 years, providing robust data on DTC incidence trends in Germany. Additionally, Germany’s universal health care system, irrespective of socioeconomic status, and a sizeable population of approximately 13.5 million children aged 0–17 years allowed for analyses with mostly high statistical power.
However, the following limitations must be considered, including potential changes in reporting practices over time, limited information on incidental findings, and a significant proportion of missing data on clinical information, which could introduce systematic bias. Additionally, the GCCR only began collecting data for patients aged 15 and older from 2009, potentially affecting observed trends in this age group.
Conclusion
The increasing incidence of DTC in children and adolescents in Germany mirrors global trends and presents a complex public health challenge. While improved detection likely contributes to this trend, the stable tumor size distribution suggests that other factors are also in play. A multidisciplinary approach combining epidemiology, genetics, and environmental science is essential to enhance our understanding and develop effective prevention and intervention strategies. As we continue to unravel the complexities of pediatric DTC, it is crucial to balance the benefits of early detection with the potential harms of overdiagnosis, ensuring optimal outcomes for this vulnerable population.
Footnotes
Acknowledgment
The authors are grateful to the GPOH and the pediatric hematology–oncology units for their data contributions to the German Childhood Cancer Registry.
Authors’ Contributions
Mi.Ku.: Conceptualization, resources, writing-original draft, writing-review and editing, supervision, project administration, and funding acquisition. M.W.: Conceptualization, methodology, formal analysis, writing-original draft, writing-review and editing, and visualization. Ma.Ku.: Investigation, data curation, and writing-review and editing. C.T.: Data curation and writing-review and editing. C.R.: Methodology, resources, writing-review and editing. A.R.: Conceptualization, investigation, resources, writing-review and editing, and funding acquisition. F.E.: Conceptualization, methodology, resources, writing-original draft, writing-review and editing, supervision, and project administration.
Data Availability Statement
Under the permission that national data protection requirements are fully met, access to aggregated data may be made available upon reasonable request. All data access requests should be directed to the corresponding author.
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial, personal, or financial relationships with other people or organizations that could be construed as a potential conflict of interest.
Funding Information
The German MET studies were funded by